
Ready for School: A Multi-Dimensional Approach to School Readiness Assessment in Hispanic Children from Puerto Rico

 ,
, 
 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment Procedures
2.3. Measures
2.3.1. Batería IV Woodcock-Muñoz: Pruebas de Aprovechamiento (Brief Academic Battery)
2.3.2. Home Observation Measurement of the Environment—Short Form (HOME-SF)
2.3.3. NIH Toolbox Early Childhood Cognition Battery (NIHTB-Cog)
2.3.4. NIH Toolbox Parent Proxy Emotion Battery (NIHTB-EM)
2.3.5. Ages and Stages Questionnaire, Third Edition (ASQ-3)
2.3.6. Ages and Stages Questionnaire: Social-Emotional, Second Edition (ASQ:SE-2)
2.3.7. Peabody Developmental Motor Scale, Second Edition (PDMS-2)
2.3.8. Instrument-Based Vision Screening
2.3.9. Audiological Evaluation
2.3.10. Pediatrician Assessment (POPZE Child Investigation Form; CIF)
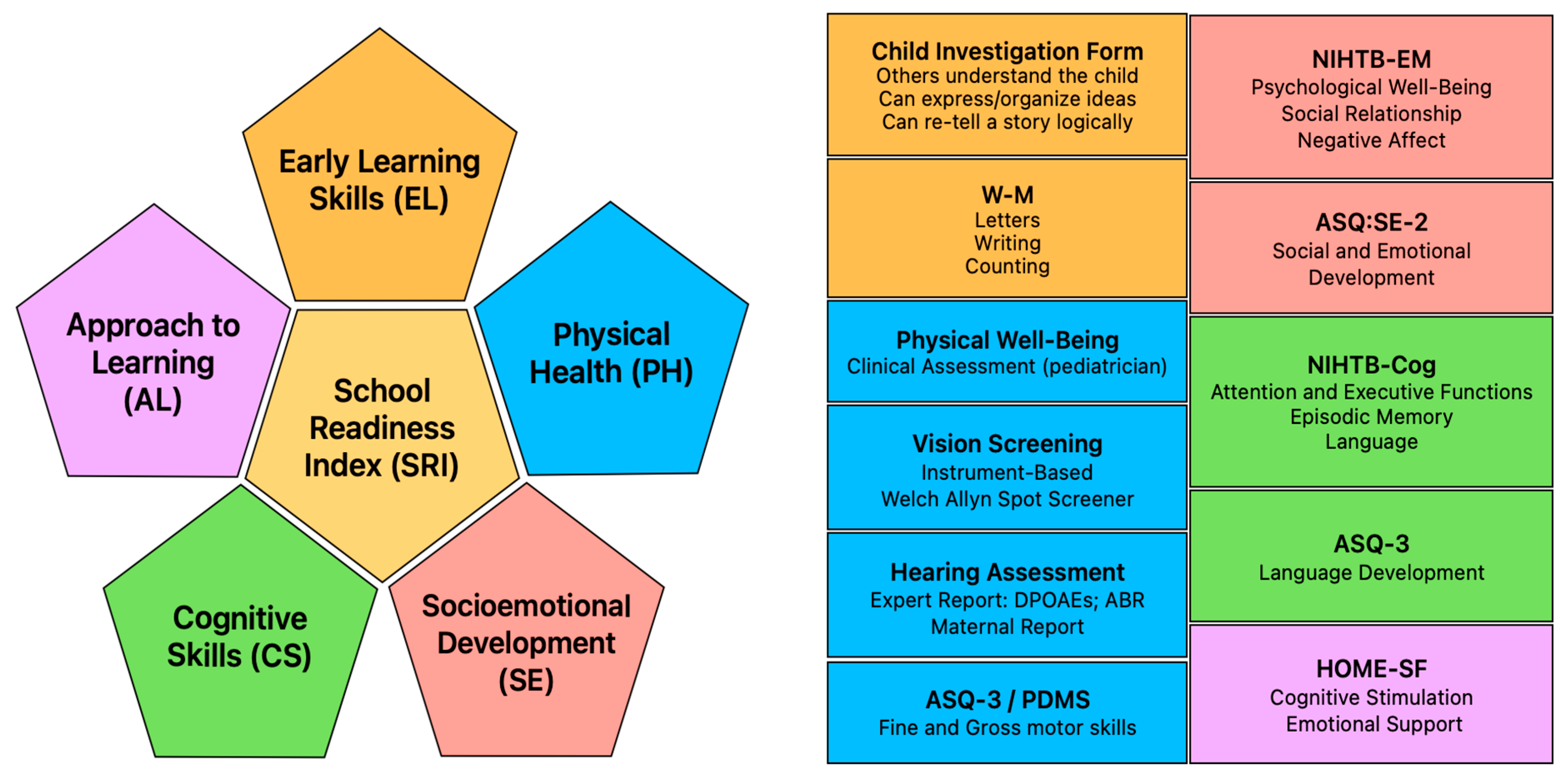
2.4. Defining the SRI
2.4.1. Scoring the SRI
Early Learning Skills (EL) Domain
Approach to Learning (AL) Domain
Cognitive Skills (CS) Domain
Socioemotional Development (SE) Domain
Physical Health (PH) Domain
2.4.2. Interpretation of the SRI
2.5. Data Analyses
3. Results
3.1. SRI Developmental Domains and Composite Scores
3.2. Relationships Among the SRI Composite Scores, Domains, and Determinants of Health
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alvarado-Domenech, L. I., Rivera-Amill, V., Appleton, A. A., Rosario-Villafañe, V., Repollet-Carrer, I., Borges-Rodríguez, M., Pérez-Rodríguez, N. M., Olivieri-Ramos, O., González, M., González-Montalvo, C., Muñiz-Forestier, W., Vargas-Lasalle, L., Pérez-Padilla, J., Paz-Bailey, G., & Rodríguez-Rabassa, M. (2022). Early childhood neurodevelopmental outcomes in children with prenatal zika virus exposure: A cohort study in Puerto Rico. The Journal of Pediatrics, 247, 38–45.e5. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Audiology. (2011). Childhood hearing screening. Clinical practice guidelines, issue. Available online: https://www.audiology.org/wp-content/uploads/2021/05/ChildhoodScreeningGuidelines.pdf_5399751c9ec216.42663963.pdf (accessed on 29 June 2024).
- Bauer, P. J., Dikmen, S. S., Heaton, R. K., Mungas, D., Slotkin, J., & Beaumont, J. L. (2013). III. NIH toolbox cognition battery (CB): Measuring episodic memory. Monographs of the Society for Research in Child Development, 78(4), 34–48. [Google Scholar] [CrossRef] [PubMed]
- Baxter. (n.d.). Welch Allyn spot vision screener. Available online: https://www.hillrom.com/en/products/spot-vision-screener/ (accessed on 12 September 2023).
- Bleil, M. E., Roisman, G. I., Hamilton, D. T., Magro, S. W., Appelhans, B. M., Gregorich, S. E., Booth-LaForce, C., & Pianta, R. C. (2024). Which aspects of education are health protective? A life course examination of early education and adulthood cardiometabolic health in the 30-year study of early child care and Youth Development (SECCYD). BMC Public Health, 24(1), 1092. [Google Scholar] [CrossRef]
- Bradley, R. H., & Caldwell, B. M. (1979). Home observation for measurement of the environment: A revision of the preschool scale. American Journal of Mental Deficiency, 84(3), 235–244. [Google Scholar]
- Brandlistuen, R. E., Flatø, M., Stoltenberg, C., Helland, S. S., & Wang, M. V. (2021). Gender gaps in preschool age: A study of behavior, neurodevelopment and pre-academic skills. Scandinavian Journal of Public Health, 49(5), 503–510. [Google Scholar] [CrossRef]
- Brumley, L. D., Brumley, B. P., & Jaffee, S. R. (2019). Comparing cumulative index and factor analytic approaches to measuring maltreatment in the national longitudinal study of adolescent to adult health. Child Abuse & Neglect, 87, 65–76. [Google Scholar] [CrossRef]
- Casaletto, K. B., Umlauf, A., Marquine, M., Beaumont, J. L., Mungas, D., Gershon, R., Slotkin, J., Akshoomoff, N., & Heaton, R. K. (2016). Demographically corrected normative standards for the Spanish language version of the NIH toolbox cognition battery. Journal of the International Neuropsychological Society, 22(3), 364–374. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. (2025). Child and teen BMI categories. U.S. Department of Health & Human Services. Available online: https://www.cdc.gov/bmi/child-teen-calculator/bmi-categories.html (accessed on 8 July 2025).
- Council on Communications and Media, Hill, D., Ameenuddin, N., Chassiakos, Y. R., Cross, C., Hutchinson, J., Levine, A., Boyd, R., Mendelson, R., Moreno, M., & Swanson, W. S. (2016). Media and young minds. Pediatrics, 138(5), e20162591. [Google Scholar] [CrossRef]
- Daily, S., Burkhauser, M., & Halle, T. (2010). A review of school readiness practices in the states: Early learning guidelines and assessments. Child Trends: Early Childhood Highlights, 1(3), 1–12. Available online: https://nces.ed.gov/programs/slds/pdf/10_III_IVb.pdf (accessed on 12 January 2024).
- Denboer, J. W., Nicholls, C., Corte, C., & Chestnut, K. (2014). National Institutes of Health toolbox cognition battery. Archives of Clinical Neuropsychology, 29(7), 692–694. [Google Scholar] [CrossRef]
- Donahue, S. P., & Nixon, C. N. (2016). Visual system assessment in infants, children, and young adults by pediatricians. Pediatrics, 137(1), 28–30. [Google Scholar] [CrossRef]
- Doyle, O., Harmon, C. P., Heckman, J. J., & Tremblay, R. E. (2009). Investing in early human development: Timing and economic efficiency. Economics & Human Biology, 7(1), 1–6. [Google Scholar] [CrossRef]
- Duncan, G. J., Dowsett, C. J., Claessens, A., Magnuson, K., Huston, A. C., Klebanov, P., Pagani, L. S., Feinstein, L., Engel, M., Brooks-Gunn, J., Sexton, H., Duckworth, K., & Japel, C. (2007). School readiness and later achievement. Developmental Psychology, 43(6), 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Entwisle, D. R., Alexander, K. L., & Olson, L. S. (2005). First grade and educational attainment by age 22: A new story. American Journal of Sociology, 110, 1458–1502. [Google Scholar] [CrossRef]
- Evans, G. W., Li, D., & Whipple, S. S. (2013). Cumulative risk and child development. Psychological Bulletin, 139(6), 1342–1396. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, C., Boers, E., & Pagani, L. S. (2020). Kindergarten readiness, later health, and social costs. Pediatrics, 146(6), e20200978. [Google Scholar] [CrossRef]
- Folio, M. R., & Fewell, R. R. (2000). PDMS-2: Peabody developmental motor scales (2nd ed.). ProEd. [Google Scholar]
- Fox, R. S., Manly, J. J., Slotkin, J., Devin Peipert, J., & Gershon, R. C. (2021). Reliability and validity of the Spanish-language version of the NIH toolbox. Assessment, 28(2), 457–471. [Google Scholar] [CrossRef]
- Garver, K. (2020). The “why” behind kindergarten entry assessments. NIEER Newsletter: National Institute for Early Education Research. [Google Scholar]
- Gershon, R. C., Slotkin, J., Manly, J. J., Blitz, D. L., Beaumont, J. L., Schnipke, D., Wallner-Allen, K., Golinkoff, R. M., Gleason, J. B., Hirsh-Pasek, K., Adams, M. J., & Weintraub, S. (2013). IV. NIH toolbox cognition battery (CB): Measuring language (vocabulary comprehension and reading decoding). Monographs of the Society for Research in Child Development, 78(4), 49–69. [Google Scholar] [CrossRef]
- Ghandour, R. M., Hirai, A. H., Moore, K. A., Paschall, K., LaForett, D. R., Reddington, E., & Kogan, M. D. (2024). School readiness among United States children: Results from the 2022 national survey of children’s health. Academic Pediatrics, 24(7), 1049–1061. [Google Scholar] [CrossRef]
- Ghandour, R. M., Hirai, A. H., Moore, K. A., Robinson, L. R., Kaminski, J. W., Murphy, K., Lu, M. C., & Kogan, M. D. (2021). Healthy and ready to learn: Prevalence and correlates of school readiness among United States preschoolers. Academic Pediatrics, 21(5), 818–829. [Google Scholar] [CrossRef]
- Gill, R., Karim, M. E., Puyat, J. H., Guhn, M., Janus, M., Gagné Petteni, M., Forer, B., & Gadermann, A. M. (2024). Childhood poverty and school readiness: Differences by poverty type and immigration background. SSM Population Health, 25, 101563. [Google Scholar] [CrossRef] [PubMed]
- Hair, N. L., Hanson, J. L., Wolfe, B. L., & Pollak, S. D. (2015). Association of child poverty, brain development, and academic achievement. JAMA Pediatrics, 169(9), 822–829. [Google Scholar] [CrossRef]
- Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O’Neal, L., McLeod, L., Delacqua, G., Delacqua, F., Kirby, J., & Duda, S. N. (2019). The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381. [Google Scholar] [CrossRef]
- Houtrow, A., Martin, A. J., Harris, D., Cejas, D., Hutson, R., Mazloomdoost, Y., & Agrawal, R. K. (2022). Health equity for children and youth with special health care needs: A vision for the future. Pediatrics, 149(Suppl. 7), e2021056150F. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C., Daly, I., Foley, S., White, N., & Devine, R. T. (2015). Measuring the foundations of school readiness: Introducing a new questionnaire for teachers—The brief early skills and support index (BESSI). British Journal of Educational Psychology, 85(3), 332–356. [Google Scholar] [CrossRef]
- Individuals with Disabilities Education Act. (2004). IDEA statue. Available online: https://uscode.house.gov/view.xhtml?path=/prelim@title20/chapter33&edition=prelim (accessed on 13 January 2024).
- Janus, M., & Offord, D. R. (2007). Development and psychometric properties of the early development instrument (EDI): A measure of children’s school readiness. Canadian Journal of Behavioural Science/Revue Canadienne des Sciences du Comportement, 39(1), 1–22. [Google Scholar] [CrossRef]
- Kaminski, J. W., Barrueco, S., Kelleher, K. J., Hoagwood, K., Edwards, A., & Fox, E. G. (2023). Vital signs for pediatric health: School readiness. NAM Perspectives. [Google Scholar] [CrossRef]
- MAICO. (n.d.-a). easyScreen: ABR + OAE combined in one hearing screening device. Available online: https://www.maico-diagnostics.com/products/oae-testing/easyscreen (accessed on 10 February 2024).
- MAICO. (n.d.-b). MA 25: A light and small portable audiometer for basic screening. Available online: https://www.maico-diagnostics.com/products/audiometers/ma-25 (accessed on 10 February 2024).
- Mott, F. L. (2004). The utility of the HOME-SF scale for child development research in a large national longitudinal survey: The national longitudinal survey of youth 1979 cohort. Parenting, 4(2–3), 259–270. [Google Scholar] [CrossRef]
- National Education Goals Panel. (1991). Striving for excellence: The national education goals. ERIC. [Google Scholar]
- Path Medical. (2022). Sntiero advanced: Quick start guide. Available online: https://www.pathme.de/download/quick-guides/EN/100800-18_Sentiero-Advanced-ASSR-Quick-Start-Guide_Rev2.pdf (accessed on 10 February 2024).
- Peterseim, M. M. W., Trivedi, R. H., Feldman, S., Husain, M., Walker, M., Wilson, M. E., & Wolf, B. J. (2020). Evaluation of the spot vision screener in school-aged children. Journal of Pediatric Ophthalmology & Strabismus, 57(3), 146–153. [Google Scholar] [CrossRef]
- Salsman, J. M., Butt, Z., Pilkonis, P. A., Cyranowski, J. M., Zill, N., Hendrie, H. C., Kupst, M. J., Kelly, M. A. R., Bode, R. K., Choi, S. W., Lai, J., Griffith, J. W., Stoney, C. M., Brouwers, P., Knox, S. S., & Cella, D. (2013). Emotion assessment using the NIH toolbox. Neurology, 80(11 Suppl. S3), S76–S86. [Google Scholar] [CrossRef]
- Shulman, K., Baicker, K., & Mayes, L. (2024). Reading for life-long health. Frontiers in Pediatrics, 12, 1401739. [Google Scholar] [CrossRef] [PubMed]
- Squires, J., Briker, D., & Twombly, E. (2002). The ages and stages questionnaires: Social-emotional (ASQ: SE) user’s guide. Paul H. [Google Scholar]
- Squires, J., Twombley, E., Bricker, D., & Potter, L. (2009). Ages and stages questionnaires (ASQ): A parent-completed child monitoring system (3rd ed.). Brookes. [Google Scholar]
- The Annie E. Casey Foundation. (2025). 2025 kids count data book: State trends in child well-being. Available online: https://cdn.prod.website-files.com/673540caa1e3cb96e03eb4b5/6849ad8abe10f62dada4f9d0_2025-Aecf-kidscountdatabook.pdf (accessed on 3 July 2025).
- Waldfogel, J., Kwon, S. J., Wang, Y., Washbrook, L., Casoni, V. P., Olczyk, M., Schneider, T., Panico, L., Solaz, A., Weinert, S., Volodina, A., de la Rie, S., Keizer, R., Nozaki, K., Yamashita, J., Kameyama, Y., & Akabayashi, H. (2023). Inequalities in resources for preschool-age children by parental education: Evidence from six advanced industrialized countries. European Journal of Population, 39(1), 37. [Google Scholar] [CrossRef] [PubMed]
- Wendling, B., Mather, N., & Schrank, F. (2019). Examiner’s manual. Bateria IV Woodcock Muñoz: Pruebas de aprovechamiento. Houghton Mifflin Harcourt. [Google Scholar]
- Widaman, K. F. (2023). Interrogating the validity of cumulative indices of environmental and genetic risk for negative developmental outcomes. Development and Psychopathology, 35(3), 1171–1187. [Google Scholar] [CrossRef] [PubMed]
- Williams, P. G., Lerner, M. A., Council on Early Childhood, Council on School Health, Sells, J., Alderman, S. L., Hashikawa, A., Mendelsohn, A., McFadden, T., Navsaria, D., Peacock, G., Scholer, S., Takagishi, J., Vanderbilt, D., De Pinto, C. L., Attisha, E., Beers, N., Gibson, E., Gorski, P., … Weiss-Harrison, A. (2019). School readiness. Pediatrics, 144(2), e20191766. [Google Scholar] [CrossRef]
- Woodcock, R., Alvarado, C., Shrank, F., McGrew, K., Mather, N., & Muñoz-Sandoval, A. (2019). Batería IV woodcock-muñoz. Houghton Mifflin Harcourt. [Google Scholar]
- Zelazo, P. D., Anderson, J. E., Richler, J., Wallner-Allen, K., Beaumont, J. L., & Weintraub, S. (2013). II. NIH toolbox cognition battery (CB): Measuring executive function and attention. Monographs of the Society for Research in Child Development, 78(4), 16–33. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Values | |
|---|---|---|
| n | % | |
| Participant sex | ||
| Male | 63 | 52.9 |
| Female | 56 | 47.1 |
| Special education program | ||
| Registered | 39 | 32.8 |
| Not registered | 80 | 67.2 |
| Annual household income | ||
| $14,999 or less | 61 | 51.3 |
| $15,000 or higher | 58 | 48.7 |
| Health insurance | ||
| Public | 88 | 73.9 |
| Private | 31 | 26.1 |
| Maternal civil status | ||
| Married or cohabitating | 89 | 74.8 |
| Other | 30 | 25.2 |
| Maternal education attainment | ||
| Certificate, high school or less | 51 | 42.9 |
| Associate degree or more | 68 | 57.1 |
| Maternal employment status | ||
| Employed | 59 | 49.6 |
| Unemployed | 60 | 50.4 |
| Model | Measure | Estimate | SE | 95% CI | p e | |
|---|---|---|---|---|---|---|
| LL | UL | |||||
| SLRM #1 | Intercept | 18.98 | 0.58 | 17.83 | 20.14 | <0.001 |
| Participant sex a | −1.89 | 0.80 | −3.48 | −0.30 | 0.02 | |
| SLRM #2 | Intercept | 17.09 | 0.62 | 15.87 | 18.31 | <0.001 |
| Maternal education b | 1.56 | 0.82 | −0.06 | 3.18 | 0.06 | |
| SLRM #3 | Intercept | 17.14 | 0.56 | 16.03 | 18.25 | <0.001 |
| Annual household income c | 1.73 | 0.81 | 0.13 | 3.32 | 0.03 | |
| SLRM #4 | Intercept | 14.98 | 0.63 | 13.73 | 16.23 | <0.001 |
| Registered in special education program d | 4.47 | 0.77 | 2.94 | 5.99 | <0.001 | |
| Measure | Estimate | SE | 95% CI | p d | |
|---|---|---|---|---|---|
| LL | UL | ||||
| Intercept | 15.13 | 0.85 | 13.46 | 16.81 | <0.001 |
| Participant sex a | −1.16 | 0.72 | −2.58 | 0.27 | 0.11 |
| Annual household income b | 1.34 | 0.71 | −0.08 | 2.75 | 0.06 |
| Registration in special education program c | 4.18 | 0.77 | 2.66 | 5.69 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Rabassa, M.; Muniz-Rodriguez, K.; Appleton, A.A.; Borges-Rodríguez, M.; Ruiz-Raíces, N.E.; Reyes-Santiago, F.J.; Olivieri-Ramos, O.; Alvarado-Domenech, L.I. Ready for School: A Multi-Dimensional Approach to School Readiness Assessment in Hispanic Children from Puerto Rico. Behav. Sci. 2025, 15, 957. https://doi.org/10.3390/bs15070957
Rodríguez-Rabassa M, Muniz-Rodriguez K, Appleton AA, Borges-Rodríguez M, Ruiz-Raíces NE, Reyes-Santiago FJ, Olivieri-Ramos O, Alvarado-Domenech LI. Ready for School: A Multi-Dimensional Approach to School Readiness Assessment in Hispanic Children from Puerto Rico. Behavioral Sciences. 2025; 15(7):957. https://doi.org/10.3390/bs15070957
Chicago/Turabian StyleRodríguez-Rabassa, Mary, Kamalich Muniz-Rodriguez, Allison A. Appleton, Marilyn Borges-Rodríguez, Nicole E. Ruiz-Raíces, Francisco J. Reyes-Santiago, Odette Olivieri-Ramos, and Luisa I. Alvarado-Domenech. 2025. "Ready for School: A Multi-Dimensional Approach to School Readiness Assessment in Hispanic Children from Puerto Rico" Behavioral Sciences 15, no. 7: 957. https://doi.org/10.3390/bs15070957
APA StyleRodríguez-Rabassa, M., Muniz-Rodriguez, K., Appleton, A. A., Borges-Rodríguez, M., Ruiz-Raíces, N. E., Reyes-Santiago, F. J., Olivieri-Ramos, O., & Alvarado-Domenech, L. I. (2025). Ready for School: A Multi-Dimensional Approach to School Readiness Assessment in Hispanic Children from Puerto Rico. Behavioral Sciences, 15(7), 957. https://doi.org/10.3390/bs15070957