Using Behavioural Skills Training with Healthcare Staff to Promote Greater Independence for People Living with Dementia: A Randomised Single-Case Experimental Design


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Setting
2.3. Experimental Design
2.4. Measurement
2.5. Procedure
2.5.1. Baseline
2.5.2. Intervention
2.5.3. Generalisation
2.5.4. Maintenance
2.5.5. Social Validity
2.6. Analytic Approach
3. Results
3.1. Visual Analysis
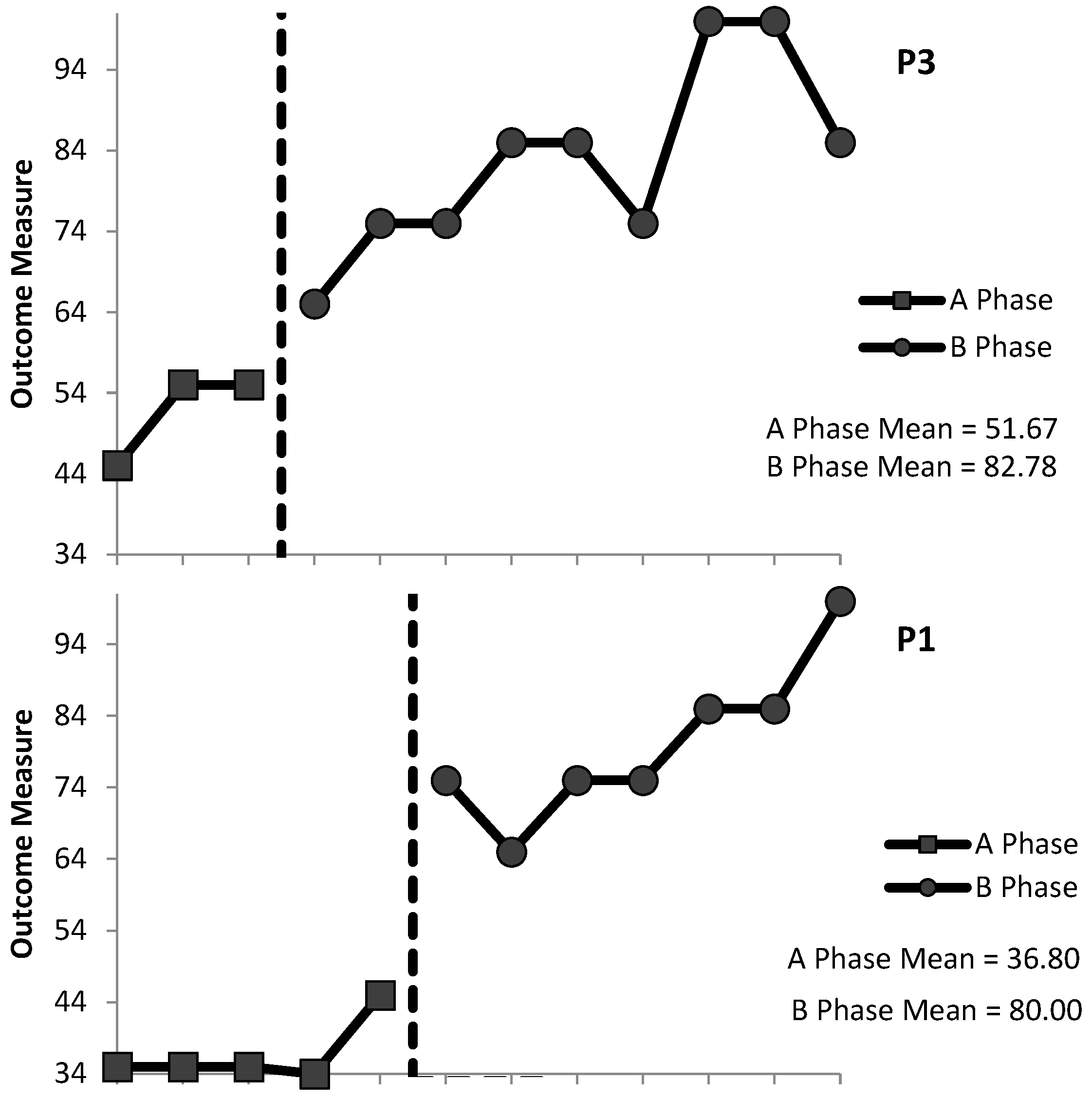
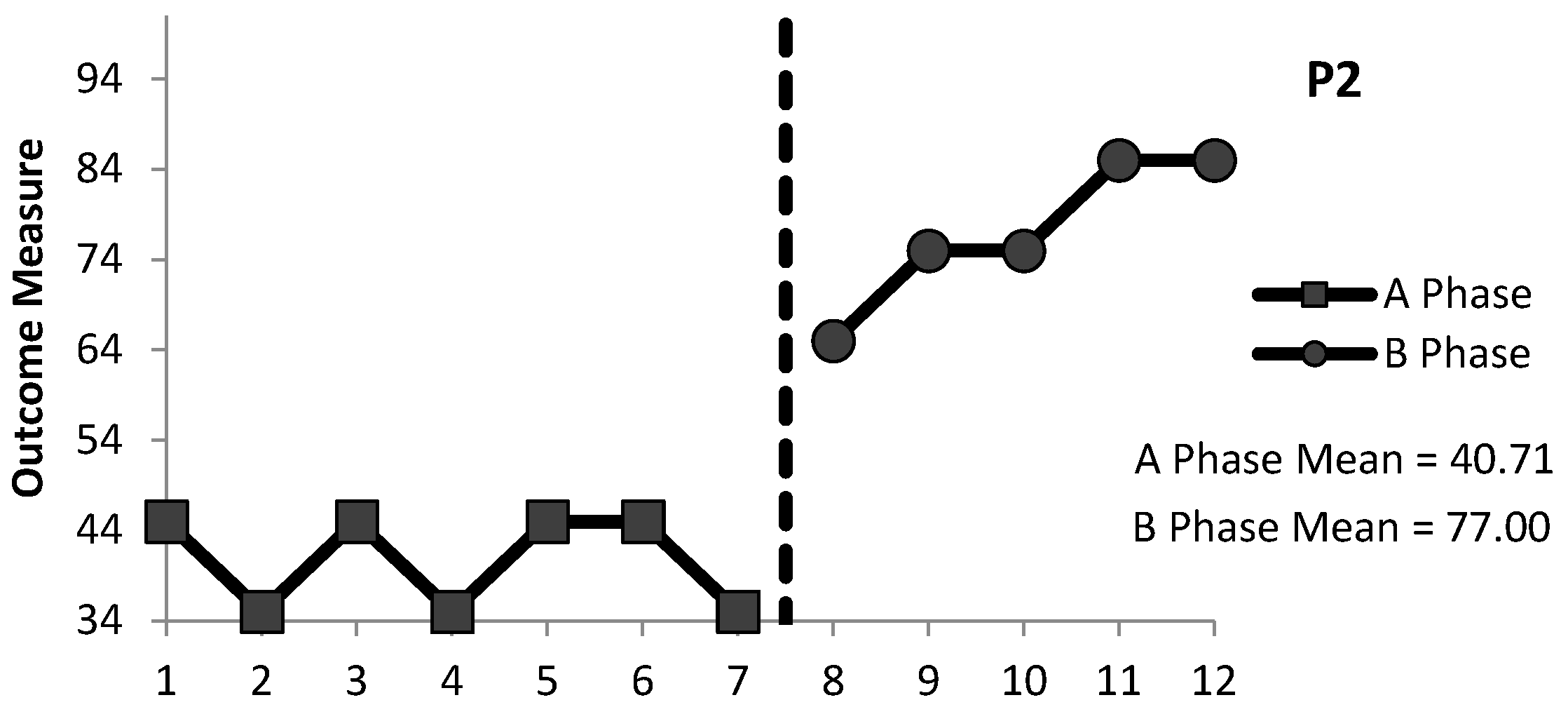
3.1.1. ADL1: Assistance to Stand
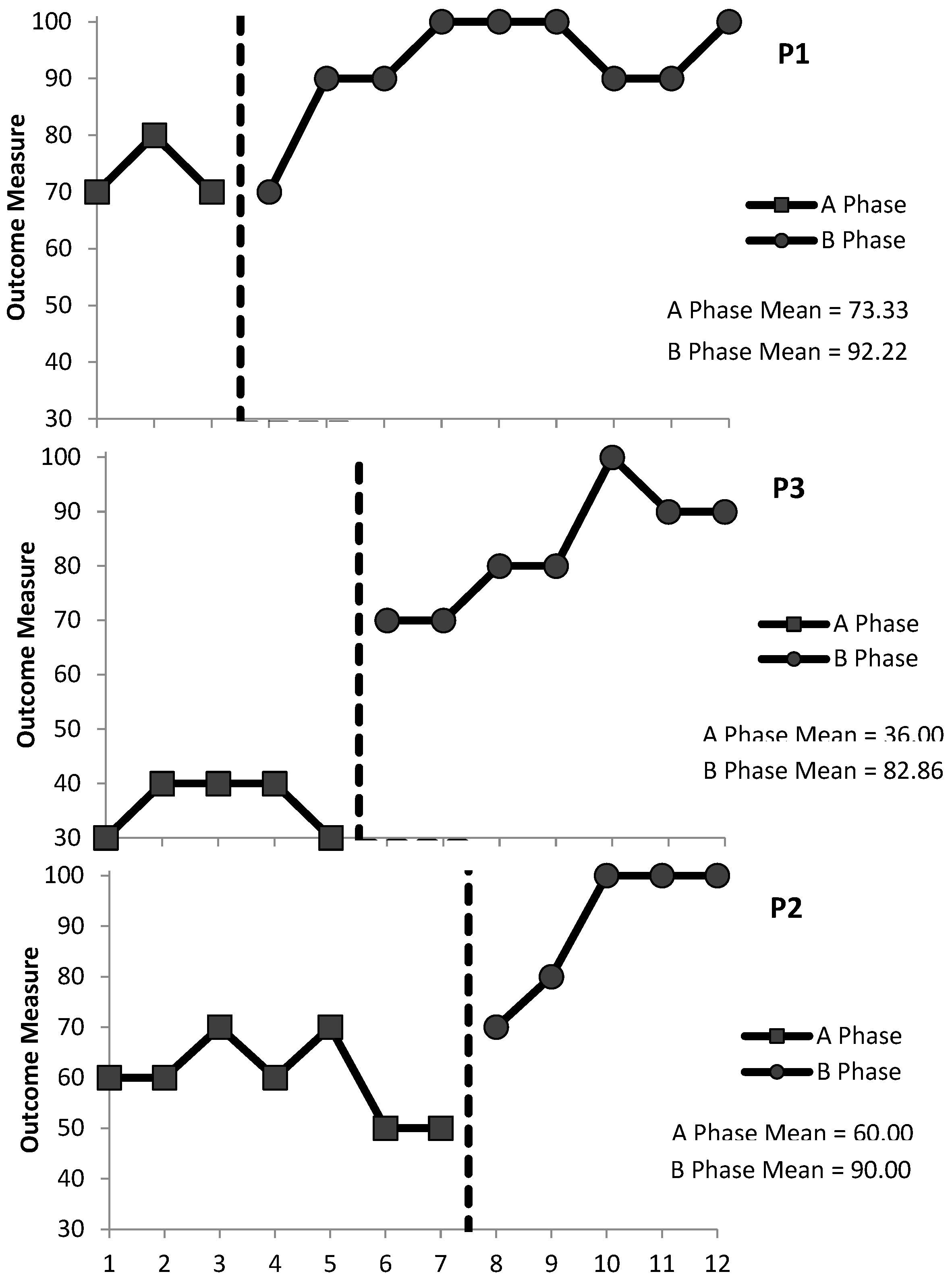
3.1.2. ADL2: Assistance with Drinking
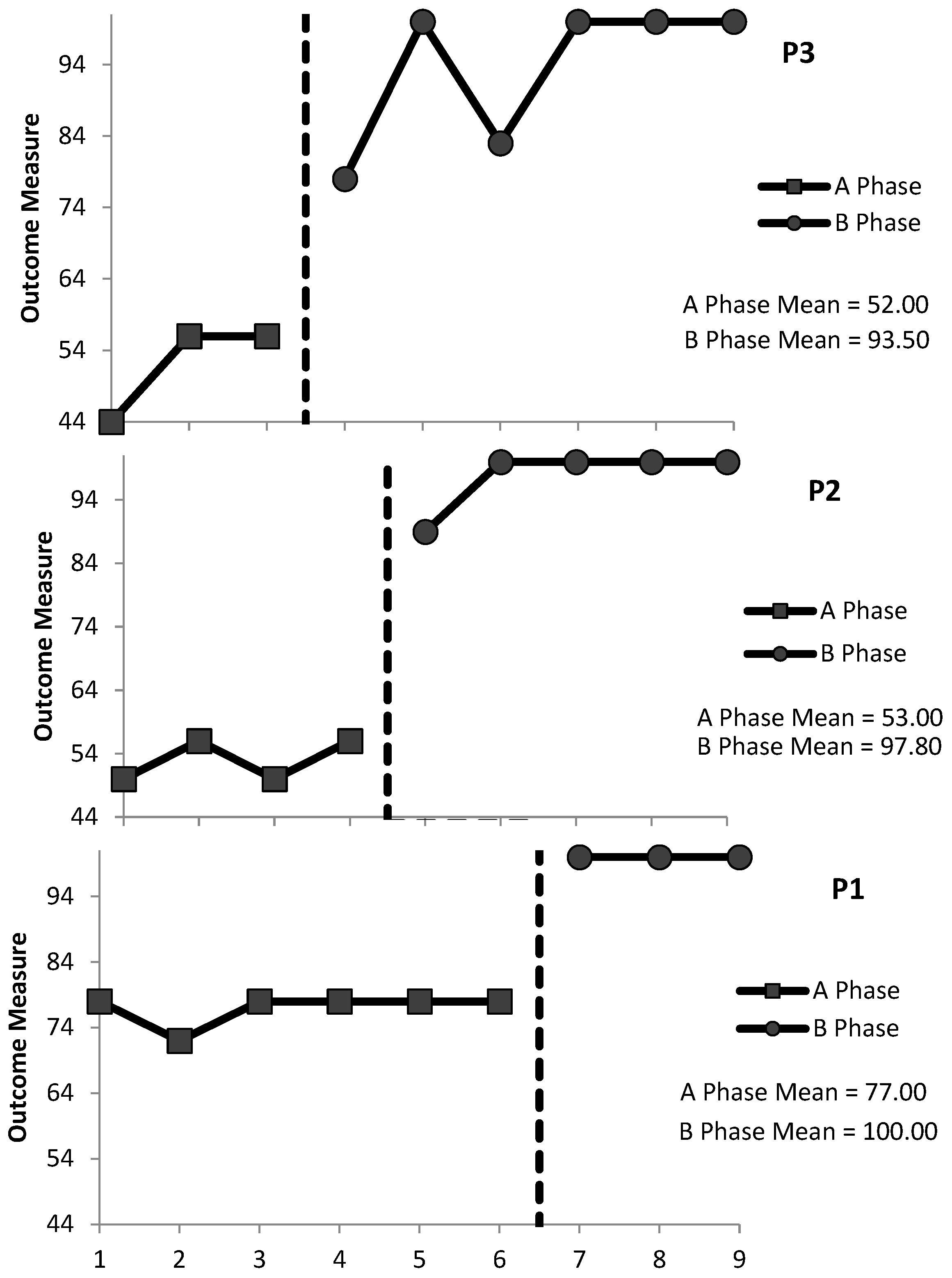
3.1.3. ADL3: Assistance to Brush Teeth
3.2. Statistical Analysis
3.3. Interobserver Agreement
3.4. Generalisation
3.5. Social Validity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PLwD | Person living with dementia |
| ADL | Activity of daily living |
| BST | Behavioural Skills Training |
| L-M | Least to most |
| WWC | What Works Clearing House |
| MBD | Multiple-baseline design |
| IV | Independent variable |
| DV | Dependent variable |
| UNCRPD | United Nations Convention on the Rights of People with Disabilities |
| SD | Discriminative stimulus |
| QoL | Quality of life |
| SCED | Single-case experimental design |
| SCRIBE | Single-Case Reporting Guideline in Behavioural Interventions |
| FETAC | Further Education and Training Awards Council |
| ExPRT | Excel Package of Randomization Tests |
| PND | Percentage of non-overlapping data |
| P1 | Participant 1 |
| P2 | Participant 2 |
| P3 | Participant 3 |
References
- Alaimo, C., Seiverling, L., Sarubbi, J., & Sturmey, P. (2018). The effects of a behavioral skills training and general-case training package on caregiver implementation of a food selectivity intervention. Behavioral Interventions, 33(1), 26–40. [Google Scholar] [CrossRef]
- Baker, J. C., Fairchild, K. M., & Seefeldt, D. A. (2015). Behavioral gerontology: Research and clinical considerations. In Clinical and organisational applications of applied behavior analysis (pp. 425–450). Elsevier. [Google Scholar] [CrossRef]
- Batsch, N., Mittler, P., & Kingston, D. (2017). Brief for Alzheimer associations: Access to the United Nations Convention on the rights of persons with disabilities by people living with dementia. Alzheimer’s Disease International & Dementia Alliance International. Available online: https://www.alzint.org/resource/access-to-united-nations-convention-on-the-rights-of-persons-with-disabilities-by-people-living-with-dementia-crpd/ (accessed on 24 June 2025).
- Brenske, S., Rudrud, E. H., Schulze, K. A., & Rapp, J. T. (2008). Increasing activity attendance and engagement in individuals with dementia using descriptive prompts. Journal of Applied Behavior Analysis, 41(2), 273–277. [Google Scholar] [CrossRef] [PubMed]
- Brown, R. T., Diaz-Ramirez, L. G., Boscardin, W. J., Lee, S. J., Williams, B. A., & Steinman, M. A. (2019). Association of functional impairment in middle age with hospitalization, nursing home admission, and death. JAMA Internal Medicine, 179(5), 668. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, A. J., Christenson, A., Houlihan, D., & Ostrom, C. (2011). The role of behavior analysis in the rehabilitation of persons with dementia. Behavior Therapy, 42, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, A. J., DeJager, B., Garcia, S., Houlihan, D., Sears, C., Fairchild, K., & Sattler, A. (2018). The relationship between instruction specificity and resistiveness to care during activities of daily living in persons with dementia. Clinical Nursing Studies, 6(4), 45. [Google Scholar] [CrossRef]
- Buchanan, J., Husfeldt, J., Berg, T., & Houlihan, D. (2008). Publication trends in behavioral gerontology in the past 25 years: Are the elderly still an understudied population in behavioral research? Behavioral Interventions, 23(1), 65–74. [Google Scholar] [CrossRef]
- Burgio, L. D., Engel, B. T., Hawkins, A., McCormick, K., Scheve, A., & Jones, L. T. (1990). A staff management system for maintaining improvements in continence with elderly nursing home residents. Journal of Applied Behavior Analysis, 23(1), 111–118. [Google Scholar] [CrossRef]
- Cipriani, G., Danti, S., Picchi, L., Nuti, A., & Fiorino, M. D. (2020). Daily functioning and dementia. Dementia & Neuropsychologia, 14(2), 93–102. [Google Scholar] [CrossRef]
- Clare, L., & Jones, R. S. (2008). Errorless learning in the rehabilitation of memory impairment: A critical review. Neuropsychology Review, 18(1), 1–23. [Google Scholar] [CrossRef]
- Courtemanche, A. B., Turner, L. B., Molteni, J. D., & Groskreutz, N. C. (2021). Scaling up behavioral skills training: Effectiveness of large-scale and multiskill trainings. Behavior Analysis in Practice, 14(1), 50. [Google Scholar] [CrossRef]
- Coyne, M. L., & Hoskins, L. (1997). Improving eating behaviors in dementia using behavioral strategies. Clinical Nursing Research, 6(3), 275–290. [Google Scholar] [CrossRef]
- Craig, A. R., & Fisher, W. W. (2019). Randomization tests as alternative analysis methods for behavior-analytic data. Journal of the Experimental Analysis of Behavior, 111(2), 309–328. [Google Scholar] [CrossRef]
- Dallery, J., & Raiff, B. R. (2014). Optimising behavioral health interventions with single-case designs: From development to dissemination. Translational Behavioral Medicine, 4(3), 290–303. [Google Scholar] [CrossRef] [PubMed]
- Engelman, K. K., Altus, D. E., & Mathews, R. M. (1999). Increasing engagement in daily activities by older adults with dementia. Journal of Applied Behavior Analysis, 32(1), 107–110. [Google Scholar] [CrossRef]
- Engelman, K. K., Altus, D. E., Mosier, M. C., & Mathews, R. M. (2003). Brief training to promote the use of less intrusive prompts by nursing assistants in a dementia care unit. Journal of Applied Behavior Analysis, 36(1), 129–132. [Google Scholar] [CrossRef] [PubMed]
- Erhard, P., Falcomata, T. S., Oshinski, M., & Sekula, A. (2022). The effects of multiple-exemplar training on generalization of social skills with adolescents and young adults with autism: A systematic review. Journal of Autism and Developmental Disorders, 11(1), 66–85. [Google Scholar] [CrossRef]
- Fisher, J. E., Drossel, C., Yury, C., & Cherup, S. (2007). A contextual model of restraint-free care for persons with dementia. In Functional analysis in clinical treatment (pp. 211–237). Elsevier. [Google Scholar] [CrossRef]
- Gafurov, B. S., & Levin, J. R. (2023). ExPRT (Excel Package of Randomization Tests): Statistical analyses of single-case intervention data (Version 4.3) [Computer software]. ExPRT website. Available online: http://ex-prt.weebly.com (accessed on 22 August 2024).
- Gitlin, L. N., Winter, L., Burke, J., Chernett, N., Dennis, M. P., & Hauck, W. W. (2008). Tailored activities to manage neuropsychiatric behaviors in persons with dementia and reduce caregiver burden: A randomised pilot study. The American Journal of Geriatric Psychiatry, 16(3), 229–239. [Google Scholar] [CrossRef]
- Gormley, L., Healy, O., O’Sullivan, B., O’Regan, D., Grey, I., & Bracken, M. (2019). The impact of behavioural skills training on the knowledge, skills and well-being of front line staff in the intellectual disability sector: A clustered randomised control trial. Journal of Intellectual Disability Research, 63(11), 1291–1304. [Google Scholar] [CrossRef]
- Han, A., Radel, J., McDowd, J. M., & Sabata, D. (2016). Perspectives of people with dementia about meaningful activities. American Journal of Alzheimer’s Disease & Other Dementias, 31(2), 115–123. [Google Scholar] [CrossRef]
- Han, S. S., White, K., & Cisek, E. (2022). A feasibility study of individuals living at home with alzheimer’s disease and related dementias: Utilisation of visual mapping assistive technology to enhance quality of life and reduce caregiver burden. Clinical Interventions in Aging, 17, 1885–1892. [Google Scholar] [CrossRef]
- Hartley, C., & Whiteley, H. A. (2024). Do multiple exemplars promote preschool children’s retention and generalisation of words learned from pictures? Cognitive Development, 70, 101459. [Google Scholar] [CrossRef]
- Health Information and Quality Authority. (2016). National standards for residential care settings for older people in Ireland. Available online: https://www.hiqa.ie/sites/default/files/2017-01/National-Standards-for-Older-People.pdf (accessed on 25 May 2023).
- Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The use of single-subject research to identify evidence-based practice in special educatio. Exceptional Children, 71(2), 165–179. [Google Scholar] [CrossRef]
- Howick, J., Chalmers, I., Glasziou, P., Greenhalgh, T., Heneghan, C., Liberati, A., Moschetti, I., Phillips, B., Thornton, H., Goddard, O., & Hodgkinson, M. (2011). The Oxford 2011 levels of evidence. Oxford Centre for Evidence-Based Medicine. Available online: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence (accessed on 12 June 2024).
- Hung, L., & Chaudhury, H. (2011). Exploring personhood in dining experiences of residents with dementia in long-term care facilities. Journal of Aging Studies, 25(1), 1–12. [Google Scholar] [CrossRef]
- Hwang, Y., Levin, J. R., & Johnson, E. W. (2016). Pictorial mnemonic-strategy interventions for children with special needs: Illustration of a multiply randomized single-case crossover design. Developmental Neurorehabilitation, 21(4), 223–237. [Google Scholar] [CrossRef] [PubMed]
- Josling, M. (2015). A review of behavioural gerontology and dementia related interventions. Studies in Arts and Humanities, 1(5), 39–51. [Google Scholar] [CrossRef]
- Kazdin, A. E. (1982). Single-case research designs: Methods for clinical and applied settings. Oxford University Press. [Google Scholar]
- Kelly, M. E., Lawlor, B. A., Coen, R. F., Robertson, I. H., & Brennan, S. (2019). Cognitive rehabilitation for early stage alzheimer’s disease: A pilot study with an irish population. Irish Journal of Psychological Medicine, 36(2), 105–119. [Google Scholar] [CrossRef]
- Kitwood, T. (1990). The dialectics of dementia: With particular reference to Alzheimer’s disease. Ageing & Society, 10(2), 177–196. [Google Scholar]
- Koehler, M. J., & Levin, J. R. (1998). Regulated randomization: A potentially sharper analytical tool for the multiple-baseline design. Psychological Methods, 3(2), 206–217. [Google Scholar] [CrossRef]
- Kratochwill, T. R., Hitchcock, J., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., & Shadish, W. R. (2010). Single-case designs technical documentation. Available online: https://ies.ed.gov/ncee/wwc/docs/referenceresources/wwc_scd.pdf (accessed on 4 November 2024).
- Kratochwill, T. R., Hitchcock, J. H., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., & Shadish, W. R. (2013). Single-case intervention research design standards. Remedial and Special Education, 34(1), 26–38. [Google Scholar] [CrossRef]
- Kratochwill, T. R., & Levin, J. R. (2010). Enhancing the scientific credibility of single-case intervention research: Randomization to the rescue. Psychological Methods, 15(2), 124–144. [Google Scholar] [CrossRef]
- Lancioni, G. E., Singh, N. N., O’reilly, M. F., Sigafoos, J., Bosco, A., Zonno, N., & Badagliacca, F. (2011). Persons with mild or moderate alzheimer’s disease learn to use urine alarms and prompts to avoid large urinary accidents. Research in Developmental Disabilities, 32, 1990–2004. [Google Scholar] [CrossRef] [PubMed]
- Lane, J. D., & Gast, D. L. (2014). Visual analysis in single case experimental design studies: Brief review and guidelines. Neuropsychological Rehabilitation, 24(3–4), 445–463. [Google Scholar] [CrossRef]
- Laver, K., Piersol, C. V., & Wiley, R. (2021). Optimising independence in activities of daily living. In Dementia rehabilitation: Evidence-based interventions and clinical recommendations (pp. 81–96). Elsevier. [Google Scholar] [CrossRef]
- Lerman, D. C., LeBlanc, L. A., & Valentino, A. L. (2015). Evidence-based application of staff and caregiver training procedures. In Clinical and organisational applications of applied behavior analysis (pp. 321–351). Elsevier. [Google Scholar] [CrossRef]
- Levin, J. R., Ferron, J. M., & Gafurov, B. S. (2018). Comparison of randomization-test procedures for single-case multiple-baseline designs. Developmental Neurorehabilitation, 21(5), 290–311. [Google Scholar] [CrossRef]
- Levin, J. R., & Kratochwill, T. R. (2021). Randomised single-case intervention designs and analyses for health sciences researchers: A versatile clinical trials companion. Therapeutic Innovation & Regulatory Science, 55, 755–764. [Google Scholar] [CrossRef]
- Levin, J. R., Kratochwill, T. R., & Ferron, J. M. (2019). Randomization procedures in single-case intervention research contexts: (Some of) “The rest of the story”. Journal of the Experimental Analysis of Behavior, 112(3), 334–348. [Google Scholar] [CrossRef]
- Libby, M., Weiss, J. S., Bancroft, S., & Ahearn, W. H. (2008). A comparison of most-to-least and least-to-most prompting on the acquisition of solitary play skills. Behavior Analysis in Practice, 1(1), 37–43. [Google Scholar] [CrossRef]
- Lichtenstein, M. J., Federspiel, C. F., & Schaffner, W. (1985). Factors associated with early demise in nursing home residents: A case control study. Journal of the American Geriatrics Society, 33(5), 315–319. [Google Scholar] [CrossRef] [PubMed]
- Manolov, R., & Moeyaert, M. (2017). How can single-case data be analysed? Software resources, tutorial, and reflections on analysis. Behavior Modification, 41(2), 179–228. [Google Scholar] [CrossRef] [PubMed]
- McCurry, S., & Drossel, C. (2011). Treating dementia in context: A step-by-step guide to working with individuals and families. American Psychological Association. [Google Scholar] [CrossRef]
- McGowan, B., Gibb, M., Cullen, K., & Craig, C. (2019). Non-cognitive symptoms of dementia (NCSD): Guidance on non-pharmacological interventions for healthcare and social care practitioners. Available online: https://dementia.ie/wp-content/uploads/2020/01/Non-cognitive_Symptoms_of_Dementia1.pdf (accessed on 9 May 2023).
- Millá N-Calenti, J. C., Tubío, J., Pita-Ferná Ndez, S., Gonzá Lez-Abraldes, I., Lorenzo, T., Ferná Ndez-Arruty, T., & Maseda, A. (2010). Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Archives of Gerontology and Geriatrics, 50, 306–310. [Google Scholar] [CrossRef]
- Miltenberger, R. G. (2016). Behavior modification: Principles and procedures. In Behavior modification: Principles and procedures (6th ed.). Cengage Learning. [Google Scholar]
- Mlinac, M. E., & Feng, M. C. (2016). Assessment of activities of daily living, self-care, and independence. Archives of Clinical Neuropsychology, 31(6), 506–516. [Google Scholar] [CrossRef]
- Moniz-Cook, E. D., Swift, K., James, I., Malouf, R., de Vugt, M., & Verhey, F. (2012). Functional analysis-based interventions for challenging behaviour in dementia. Cochrane Database of Systematic Reviews, 2012(2), CD006929. [Google Scholar] [CrossRef] [PubMed]
- Namazi, K. H., & Johnson, B. D. (1991). Environmental effects on incontinence problems in alzheimer’s disease patients. American Journal of Alzheimer’s Care and Related Disorders & Research, 6(6), 16–21. [Google Scholar] [CrossRef]
- Orth, J., Li, Y., Simning, A., & Temkin-Greener, H. (2019). Providing behavioral health services in nursing homes is difficult: Findings from a national survey. Journal of the American Geriatrics Society, 67(8), 1713–1717. [Google Scholar] [CrossRef] [PubMed]
- Ouslander, J. G. (1995). Predictors of successful prompted voiding among incontinent nursing home residents. JAMA: The Journal of the American Medical Association, 273(17), 1366. [Google Scholar] [CrossRef]
- Palmen, A., Didden, R., Korzilius, H., & Kannerhuis, L. (2010). Effectiveness of behavioral skills training on staff performance in a job training setting for high-functioning adolescents with autism spectrum disorders. Research in Autism Spectrum Disorders, 4, 731–740. [Google Scholar] [CrossRef]
- Parker, R. I., & Vannest, K. (2009). An improved effect size for single-case research: Nonoverlap of all pairs. Behavior Therapy, 40(4), 357–367. [Google Scholar] [CrossRef]
- Parsons, M. B., Rollyson, J. H., & Reid, D. H. (2012). Evidence-based staff training: A guide for practitioners. Behavior Analysis in Practicee, 5(2), 2–11. [Google Scholar] [CrossRef]
- Pierse, T., O’ Shea, E., & Carney, P. (2019). Estimates of the prevalence, incidence and severity of dementia in ireland. Irish Journal of Psychological Medicine, 36(2), 129–137. [Google Scholar] [CrossRef]
- Prizer, L. P., & Zimmerman, S. (2018). Progressive Support for activities of daily living for persons living with dementia. The Gerontologist, 58(Suppl. S1), S74–S87. [Google Scholar] [CrossRef]
- Reid, D. H., Parsons, M. B., & Green, C. W. (2021). The supervisor’s guidebook: Evidence-based strategies for promoting work quality and enjoyment among human service staff (2nd ed.). Charles C Thomas Pub Ltd. [Google Scholar]
- Rogers, J. C., Holm, M. B., Burgio, L. D., Hsu, C., Hardin, J. M., & Mcdowell, B. J. (2000). Excess disability during morning care in nursing home residents with dementia. International Psychogeriatrics, 12(2), 267–282. [Google Scholar] [CrossRef]
- Sarokoff, R. A., & Sturmey, P. (2004). The effects of behavioral skills training on staff implementation of discrete-trial teaching. Journal of Applied Behavior Analysis, 37(4), 535–538. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, M. R., Andzik, N. R., Kranak, M. P., Willke, C. P., Curiel, E. S. L., Hensley, L. E., & Neef, N. A. (2017). Improving pre-service teachers’ performance skills through behavioral skills training. Behaviour Skills Training, 10, 296–300. [Google Scholar] [CrossRef]
- Schmidt, A. L. (2016). Using behavior skills training to teach effective conversation skills to individuals with disabilities [Master’s thesis, Missouri State University]. Available online: https://bearworks.missouristate.edu/theses/3044 (accessed on 10 February 2023).
- Scruggs, T. E., & Mastropieri, M. A. (1998). Summarising single-subject research. Behavior Modification, 22(3), 221–242. [Google Scholar] [CrossRef] [PubMed]
- Shadish, W. R. (2014). Analysis and meta-analysis of single-case designs: An introduction. Journal of School Psychology, 52(2), 109–122. [Google Scholar] [CrossRef] [PubMed]
- Sherman, J., Richardson, J., & Vedora, J. (2021). The use of behavioral skills training to teach components of direct instruction. Behavior Analysis in Practice, 14, 1085–1091. [Google Scholar] [CrossRef]
- Skinner, B. F. (1983). Intellectual self-management in old age. American Psychologist, 38, 239–244. [Google Scholar] [CrossRef]
- Slane, M., & Lieberman-Betz, R. G. (2021). Using behavioral skills training to teach implementation of behavioral interventions to teachers and other professionals: A systematic review. Behavioral Interventions, 36(4), 984–1002. [Google Scholar] [CrossRef]
- Slocum, T. A., Pinkelman, S. E., Joslyn, P. R., & Nichols, B. (2022). Threats to internal validity in multiple-baseline design variations. Perspectives on Behavior Science, 45, 619–638. [Google Scholar] [CrossRef]
- Sturmey, P. (Ed.). (2020). Functional analysis in clinical treatment (2nd ed.). Academic Press. [Google Scholar]
- Tak, E., Kuiper, R., Chorus, A., & Hopman-Rock, M. (2015). Prevention of onset and progression of basic ADL disability by physical activity in community-dwelling older adults: A meta-analysis. Ageing Research Reviews, 24, 166–177. [Google Scholar] [CrossRef]
- Tanious, R., & Onghena, P. (2019). Randomized single-case experimental designs in healthcare research: What, why, and how? Healthcare, 7(4), 143. [Google Scholar] [CrossRef]
- Tate, R. L., Perdices, M., Rosenkoetter, U., Shadish, W., Vohra, S., Barlow, D. H., Horner, R., Kazdin, A., Kratochwill, T., Mcdonald, S., Sampson, M., Shamseer, L., Togher, L., Albin, R., Backman, C., Douglas, J., Evans, J. J., Gast, D., Manolov, R., … Barlow, D. H. (2016). The single-case reporting guideline in behavioural interventions (SCRIBE) 2016 statement. Physical Therapy, 96(7), 1. [Google Scholar] [CrossRef] [PubMed]
- Trahan, M. A., Fisher, A. B., & Hausman, N. L. (2011). Behavior-analytic research on dementia in older adults. Journal of Applied Behavior Analysis, 44, 687–691. [Google Scholar] [CrossRef]
- Trahan, M. A., Kuo, J., Carlson, M. C., & Gitlin, L. N. (2014). A systematic review of strategies to foster activity engagement in persons with dementia. Health Education & Behavior, 41(Suppl. S1), 70S–83S. [Google Scholar] [CrossRef]
- Wampold, B., & Worsham, N. (1986). Randomization tests for multiple-baseline designs. Behavioral Assessment, 8, 135–143. [Google Scholar]
- Wolery, M. (2013). A commentary: Single-case design technical document of the what works clearinghouse. Remedial and Special Education, 34(1), 39–43. [Google Scholar] [CrossRef]
- Wolery, M., Griffen, A. K., Jones Ault, M., Gast, D. L., & Munson Doyle, P. (1990). Comparison of constant time delay and the system of least prompts in teaching chained tasks. Education and Training in Mental Retardation, 25(3), 243–257. Available online: https://about.jstor.org/terms (accessed on 22 May 2025).
- World Health Organization. (2025). Dementia: Key facts. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 22 May 2025).
- Yates, L., Csipke, E., Moniz-Cook, E., Leung, P., Walton, H., Charlesworth, G., Spector, A., Hogervorst, E., Mountain, G., & Orrell, M. (2019). The development of the Promoting Independence in Dementia (PRIDE) intervention to enhance independence in dementia. Clinical Interventions in Aging, 14, 1615–1630. [Google Scholar] [CrossRef]
- Zanetti, O., Zanieri, G., Di Giovanni, G., De Vreese, L. P., Pezzini, A., Metitieri, T., & Trabucchi, M. (2001). Effectiveness of procedural memory stimulation in mild alzheimer’s disease patients: A controlled study. Neuropsychological Rehabilitation, 11(3–4), 263–272. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ADL1: Assistance to Stand | |||
| Participant | Baseline | Intervention | Design |
| 3 | 3 | 9 | AAABBBBBBBBB |
| 1 | 5 | 7 | AAAAABBBBBBB |
| 2 | 7 | 5 | AAAAAAABBBBB |
| ADL2: Assistance to Drink | |||
| Participant | Baseline | Intervention | Design |
| 1 | 3 | 9 | AAABBBBBBBBB |
| 3 | 5 | 7 | AAAAABBBBBBB |
| 2 | 7 | 5 | AAAAAAABBBBB |
| ADL3: Assistance to Brush Teeth | |||
| Participant | Baseline | Intervention | Design |
| 3 | 3 | 6 | AAABBBBBB |
| 2 | 4 | 5 | AAAABBBBB |
| 1 | 6 | 3 | AAAAAABBB |
| Percentage of Non-Overlapping Data | |||
|---|---|---|---|
| ADL1 | ADL2 | ADL3 | |
| Participant 1 | 100 | 88.8 | 100 |
| Participant 2 | 100 | 80 | 100 |
| Participant 3 | 100 | 100 | 100 |
| Overall PND | 100 | 89.6 | 100 |
| Effect Level 1 | Very effective | Very effective | Very effective |
| Social Validity Question | Staff Responses | |
|---|---|---|
| 1. | How do you feel participating in the behaviour skills training has impacted your interactions with individuals with dementia? | I can promote more independence when helping It was fine I feel like I can break small things down; I didn’t think about this before |
| 2. | Do you feel the skills you have learnt benefit individuals with dementia? Why? | Yes, they can do more than I thought Yes, made me think about my actions Yes, but it will take longer |
| 3. | Do you feel you can apply the skills you gained during the study to your work outside the activities of living that were directly taught? Where do you think this applies? | I will try Yes Yes, but it might take practice |
| 4. | Do you feel that this exercise increased your job satisfaction when working directly with individuals with dementia? | Yes Not really No |
| 5. | Would you participate in a similar type of training in the future? | Yes Probably not Not sure |
| 6. | Would you recommend this training to other healthcare staff members? Why? | Yes Yes, some staff need to slow down and give patients more time Yes, but being watched was strange |
| 7. | Do you feel more likely to promote independence within your work practice? Why? | Yes, more aware If I have time I will try |
| 8. | Is there anything that you would like to change if this was to become part of staff training | No No No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanniffy, J.; Kelly, M.E. Using Behavioural Skills Training with Healthcare Staff to Promote Greater Independence for People Living with Dementia: A Randomised Single-Case Experimental Design. Behav. Sci. 2025, 15, 870. https://doi.org/10.3390/bs15070870
Hanniffy J, Kelly ME. Using Behavioural Skills Training with Healthcare Staff to Promote Greater Independence for People Living with Dementia: A Randomised Single-Case Experimental Design. Behavioral Sciences. 2025; 15(7):870. https://doi.org/10.3390/bs15070870
Chicago/Turabian StyleHanniffy, Janette, and Michelle E. Kelly. 2025. "Using Behavioural Skills Training with Healthcare Staff to Promote Greater Independence for People Living with Dementia: A Randomised Single-Case Experimental Design" Behavioral Sciences 15, no. 7: 870. https://doi.org/10.3390/bs15070870
APA StyleHanniffy, J., & Kelly, M. E. (2025). Using Behavioural Skills Training with Healthcare Staff to Promote Greater Independence for People Living with Dementia: A Randomised Single-Case Experimental Design. Behavioral Sciences, 15(7), 870. https://doi.org/10.3390/bs15070870