
Best Practices for Teaching Psychotherapy to Medical Students: A Scoping Review

 ,
, 
Abstract
1. Introduction
1.1. Psychotherapy
1.2. Medical Education
1.3. Psychotherapy in Medical Education
1.4. Objectives of This Scoping Review
2. Materials and Methods
2.1. Search Strategies
2.2. Study Eligibility
2.3. Data Extraction
2.4. Quality Assessment
3. Results
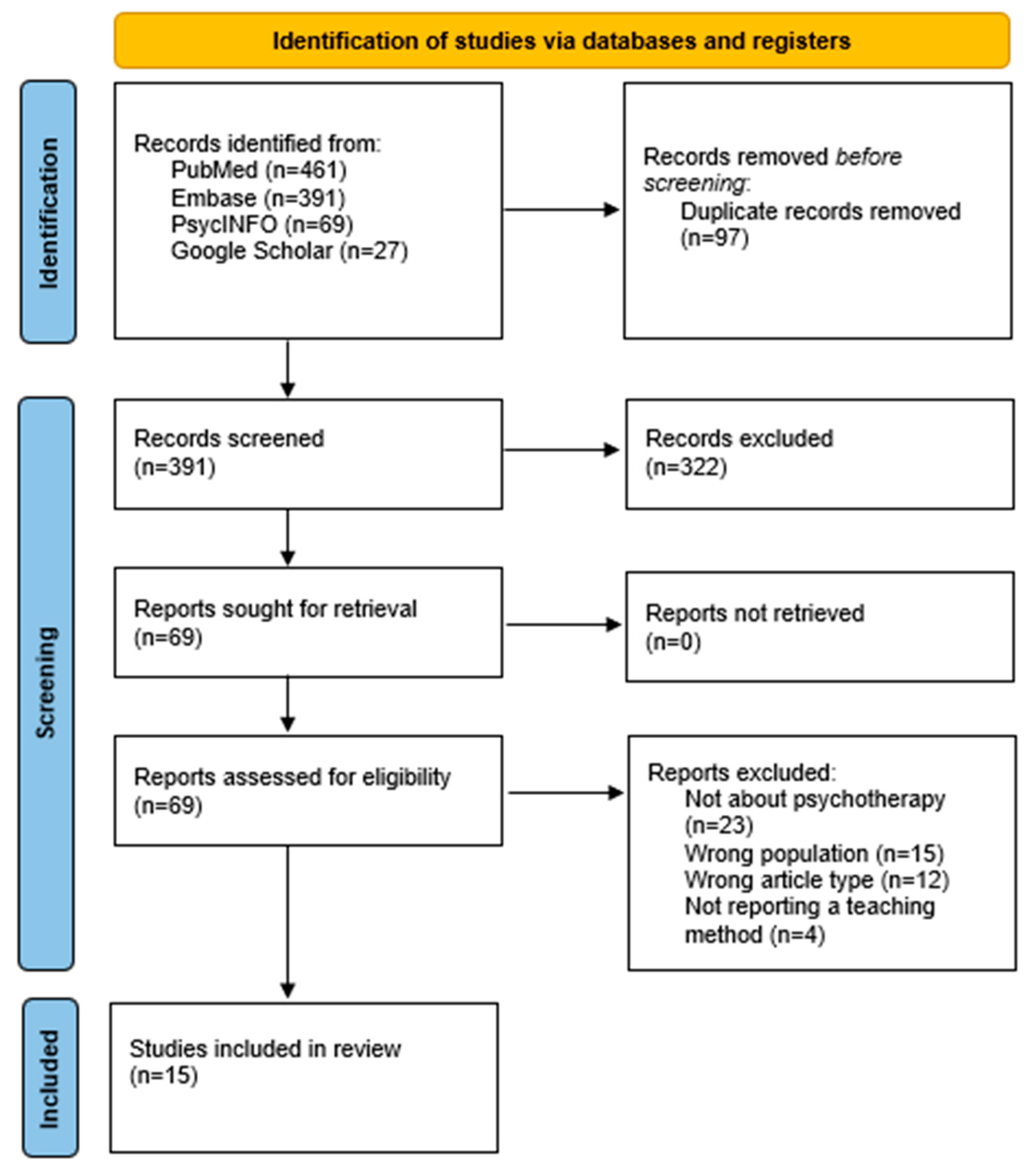
3.1. Description of Studies
3.2. Main Results
3.2.1. E-Learning
3.2.2. Role Play
3.2.3. Clinical Exposition
3.2.4. Multimodal
3.3. Quality Appraisal
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BEME | Best Evidence Medical Education |
| CBT | Cognitive–behavioral therapy |
| MD | Doctor of Medicine |
| MERSQI | Medical Education Research Study Quality Instrument |
| MI | Motivational interviewing |
| MITI | Motivational Interviewing Treatment Integrity |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews |
| SBIRT | Screening, Brief Intervention and Referral to Treatment |
References
- Bargh, J. A., & Morsella, E. (2008). The unconscious mind. Perspectives on Psychological Science, 3(1), 73–79. [Google Scholar] [CrossRef] [PubMed]
- Boivin, N., & Sakurai, S. (2024). 3-year medical education in North America: A student perspective. Medical Teacher, 46(6), 852–853. [Google Scholar] [CrossRef] [PubMed]
- Brent, D. A., & Kolko, D. J. (1998). Psychotherapy: Definitions, mechanisms of action and relationship to etiological models. Journal of Abnormal Child Psychology, 26(1), 17–25. [Google Scholar] [CrossRef]
- Buck, E., Billingsley, T., McKee, J., Richardson, G., & Geary, C. (2021). The physician healer track: Educating the hearts and the minds of future physicians. Medical Education Online, 26(1), 1844394. [Google Scholar] [CrossRef]
- Chéret, A., Durier, C., Noël, N., Bourdic, K., Legrand, C., D’Andréa, C., Hem, E., Goujard, C., Berthiaume, P., & Consoli, S. M. (2018). Motivational interviewing training for medical students: A pilot pre-post feasibility study. Patient Education and Counseling, 101(11), 1934–1941. [Google Scholar] [CrossRef] [PubMed]
- Cook, S. C., Schwartz, A. C., & Kaslow, N. J. (2017). Evidence-based psychotherapy: Advantages and challenges. Neurotherapeutics, 14(3), 537–545. [Google Scholar] [CrossRef] [PubMed]
- Craighead, W. E., & Craighead, L. W. (2001). The role of psychotherapy in treating psychiatric disorders. The Medical Clinics of North America, 85(3), 617–629. [Google Scholar] [CrossRef]
- Daeppen, J. B., Fortini, C., Bertholet, N., Bonvin, R., Berney, A., Michaud, P. A., Layat, C., & Gaume, J. (2012). Training medical students to conduct motivational interviewing: A randomized controlled trial. Patient Education and Counseling, 87(3), 313–318. [Google Scholar] [CrossRef]
- Daniel, D. G., Clopton, C. L., & Castelnuovo-Tedesco, P. (1990). How much psychiatry are medical students really learning?: A reappraisal after two decades. Academic Psychiatry, 14(1), 9–16. [Google Scholar] [CrossRef]
- Dobkin, P. L., & Hutchinson, T. A. (2013). Teaching mindfulness in medical school: Where are we now and where are we going? Medical Education, 47(8), 768–779. [Google Scholar] [CrossRef]
- Edwards, E. J., Arora, B., Green, P., Bannatyne, A. J., & Nielson, T. (2022). Teaching brief motivational interviewing to medical students using a pedagogical framework. Patient Education and Counseling, 105(7), 2315–2319. [Google Scholar] [CrossRef] [PubMed]
- Feller, S., Feller, L., Bhayat, A., Feller, G., Khammissa, R. A. G., & Vally, Z. I. (2023). Situational awareness in the context of clinical practice. Healthcare, 11(23), 3098. [Google Scholar] [CrossRef]
- Garcia-Huidobro, D., Fernandez, J., Espinosa, P., Lustig, N., Perez, I., & Letelier, L. M. (2024). Teaching therapy decision-making to medical students: A prospective mixed-methods evaluation of a curricular innovation. BMC Medical Education, 24(1), 1533. [Google Scholar] [CrossRef]
- Harden, R. M., Grant, J., Buckley, G., & Hart, I. R. (1999). BEME Guide No. 1: Best evidence medical education. Medical Teacher, 21(6), 553–562. [Google Scholar] [CrossRef] [PubMed]
- Jaros, S., & Beck Dallaghan, G. (2024). Medical education research study quality instrument: An objective instrument susceptible to subjectivity. Medical Education Online, 29(1), 2308359. [Google Scholar] [CrossRef]
- Kaltman, S., WinklerPrins, V., Serrano, A., & Talisman, N. (2015). Enhancing motivational interviewing training in a family medicine clerkship. Teaching and Learning in Medicine, 27(1), 80–84. [Google Scholar] [CrossRef] [PubMed]
- Kamenov, K., Twomey, C., Cabello, M., Prina, A. M., & Ayuso-Mateos, J. L. (2017). The efficacy of psychotherapy, pharmacotherapy and their combination on functioning and quality of life in depression: A meta-analysis. Psychological Medicine, 47(3), 414–425. [Google Scholar] [CrossRef]
- Karasu, T. B. (1977). Psychotherapies: An overview. American Journal of Psychiatry, 134(8), 851–863. [Google Scholar] [CrossRef]
- Keifenheim, K. E., Velten-Schurian, K., Fahse, B., Erschens, R., Loda, T., Wiesner, L., Zipfel, S., & Herrmann-Werner, A. (2019). “A change would do you good”: Training medical students in motivational interviewing using a blended-learning approach—A pilot evaluation. Patient Education and Counseling, 102(4), 663–669. [Google Scholar] [CrossRef]
- Kennedy, S. H., Lam, R. W., McIntyre, R. S., Tourjman, S. V., Bhat, V., Blier, P., Hasnain, M., Jollant, F., Levitt, A. J., MacQueen, G. M., McInerney, S. J., McIntosh, D., Milev, R. V., Müller, D. J., Parikh, S. V., Pearson, N. L., Ravindran, A. V., Uher, R., & CANMAT Depression Work Group. (2016). Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: Section 3. Pharmacological treatments. Canadian Journal of Psychiatry, 61(9), 540–560. [Google Scholar] [CrossRef]
- King, J., Hill, K., & Gleason, A. (2015). All the world’s a stage: Evaluating psychiatry role-play based learning for medical students. Australasian Psychiatry, 23(1), 76–79. [Google Scholar] [CrossRef] [PubMed]
- Leichsenring, F., Steinert, C., Rabung, S., & Ioannidis, J. P. A. (2022). The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: An umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry, 21(1), 133–145. [Google Scholar] [CrossRef]
- Marks, S. (2017). Psychotherapy in historical perspective. History of the Human Sciences, 30(2), 3–16. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, S. P., Hassed, C. S., & Gear, J. L. (2012). Medical and psychology students’ knowledge of and attitudes towards mindfulness as a clinical intervention. Explore, 8(6), 360–367. [Google Scholar] [CrossRef] [PubMed]
- McOwen, K. S., Whelan, A. J., & Farmakidis, A. L. (2020). Medical education in the United States and Canada, 2020. Academic Medicine, 95(9S), S2–S4. [Google Scholar] [CrossRef]
- Merlo, L. J., Dede, B. L., & Smith, K. B. (2022). Introduction to cognitive restructuring for medical students. MedEdPORTAL, 18, 11235. [Google Scholar] [CrossRef]
- Mikkonen, K., Helminen, E. E., Saarni, S. I., & Saarni, S. E. (2024). Learning outcomes of e-learning in psychotherapy training and comparison with conventional training methods: Systematic review. Journal of Medical Internet Research, 26, e54473. [Google Scholar] [CrossRef]
- Mintz, D. (2013). Teaching psychoanalytic concepts, skills and attitudes to medical students. Journal of the American Psychoanalytic Association, 61(4), 751–770. [Google Scholar] [CrossRef]
- Muzyk, A., Smothers, Z. P., Akrobetu, D., Veve, J. R., MacEachern, M., Tetrault, J. M., & Gruppen, L. (2019). Substance use disorder education in medical schools: A scoping review. Academic Medicine, 94(11), 1825–1834. [Google Scholar] [CrossRef]
- Neufeld, K. J., Alvanzo, A., King, V. L., Feldman, L., Hsu, J. H., Rastegar, D. A., Colbert, J. M., & MacKinnon, D. F. (2012). A collaborative approach to teaching medical students how to screen, intervene and treat substance use disorders. Substance Abuse, 33(3), 286–291. [Google Scholar] [CrossRef]
- Pei, T., Ding, Y., Tang, J., & Liao, Y. (2025). Evaluating the effectiveness of a multimodal psychotherapy training program for medical students in China: Protocol for a randomized controlled trial. JMIR Research Protocols, 14, e58037. [Google Scholar] [CrossRef]
- Selzer, R., Ellen, S., & Adler, R. (2015). Teaching psychological processes and psychotherapy to medical students. Australasian Psychiatry, 23(1), 69–71. [Google Scholar] [CrossRef] [PubMed]
- Solobutina, M. M., & Miyassarova, L. R. (2019). Dynamics of existential personality fulfillment in the course of psychotherapy. Behavioral Sciences, 10(1), 21. [Google Scholar] [CrossRef] [PubMed]
- Stoudemire, A. (1996). Psychiatry in medical practice: Implications for the education of primary care physicians in the era of managed care: Part 1. Psychosomatics, 37(6), 502–508. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., … Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMAScR): Checklist and explanation. Annals of Internal Medicine, 169, 467–473. [Google Scholar] [CrossRef]
- Truong, A., Wu, P., Diez-Barroso, R., & Coverdale, J. (2015). What is the efficacy of teaching psychotherapy to psychiatry residents and medical students? Academic Psychiatry, 39(5), 575–579. [Google Scholar] [CrossRef]

{kind=link}
| Authors Year | Title | Population | Type of Psychotherapy | Teaching Methods | Results |
|---|---|---|---|---|---|
| Buck et al. (2021) | The physician healer track: educating the hearts and the minds of future physicians | Medical students; n = 258 | Training in mindfulness, cognitive–behavioral therapy, nonviolent communication, motivational interviewing, spirituality in healthcare, wellness, equanimity and ‘being with suffering’ is reinforced across all 4 years. Community building and reflection are integral to the training both in the monthly sessions and the immersion courses. | The physician healer track—a 500-contact-hour curricula integrated over 4 years; monthly dinner meetings with faculty mentors; a two-month preceptorship in the first year; a one-month immersion course in MS4 and one elective. | Less than 1% attrition. In serial assessments, students report continued growth in personal development, professional development and the ability to empathize. Enrollment has grown from 26 students in the first year (11% of class) to a total of 258 students across our first 6 years (average of 20–26% of each class). |
| Chéret et al. (2018) | Motivational interviewing training for medical students: a pilot pre-post feasibility study | Medical students; n = 20 | Motivational interviewing. | Three four-hour sessions of MI training over one week; viewing and commenting on video clips; practical exercise; lectures and the distribution of memory aids; role playing. | Global scores from the MITI-3.1.1 code, including “MI-Spirit”, were attributed to the audiotaped interviews by two independent coders, who were blinded to the pre- or post-training status of the interview. Secondary outcomes were caregivers’ perception of students’ empathy (CARE questionnaire), students’ evaluation of self-efficacy to engage in a patient-centered relationship (SEPCQ score) and students’ satisfaction with their own performance (analog scale). MI-Spirit score increased significantly after training (p < 0.0001; effect size 1.5). Limited improvements in CARE score (p = 0.034; effect size 0.5) and one of the SEPCQ dimensions (sharing information and power with the patient; p = 0.047; effect size 0.5) were also noted. Students’ satisfaction score was unaffected (p = 0.69). These findings suggest that brief MI training can improve communication skills in medical students. |
| Daeppen et al. (2012) | Training medical students to conduct motivational interviewing: a randomized controlled trial | All students (n = 131) in year five of a six-year curriculum at Lausanne University Medical School in Switzerland were randomized into an experimental group (n = 66) or control group (n = 65) | Motivational interviewing. | Four-hour sessions of practical exercises and role playing. After training all students in basic communication skills in years two and three (control condition), an eight-hour MI training workshop was completed by students in the experimental group. One week after the training, students in both groups were invited to meet for 15 min with two standardized patients. | Motivational interviewing (MI) skills were coded by four blinded research assistants using the Motivational Interviewing Treatment Integrity (MITI) coding system, version 3.0. A superior performance was shown among trained versus control students, as demonstrated by higher mean values for empathy and MI spirit. Behavior- counts assessment demonstrated better performance in MI among trained versus control students regarding occurrences of MI-adherent behavior, MI nonadherent behavior, closed questions, open questions, simple reflections and complex reflections. In sum, an eight-hour training workshop was associated with improved MI performance, lending support for the implementation of MI training in medical schools. |
| Dobkin and Hutchinson (2013) | Teaching mindfulness in medical school: where are we now and where are we going? | Medical students (literature review on teaching mindfulness) | Mindfulness. | A wide range of formats are used in teaching mindfulness. These include simple lectures, 1-day workshops and 8–10 week programs in mindfulness-based stress; an 8-week course delivered in sessions of 2.5 h each week, with a silent retreat day; and lectures or workshops on mindfulness are interspersed throughout the 4-year curriculum. | Outcomes identified thus far include reductions in perceived stress, anxiety and symptoms of depression, as well as increases in mindfulness, empathy and self- compassion, as measured soon after the course. We have yet to learn if these changes are maintained over time. Moreover, we do not know how these impacts generalize to other aspects of the students’ lives and their work with peers, colleagues and patients. |
| Edwards et al. (2022) | Teaching brief motivational interviewing to medical students using a pedagogical framework | Pre-clinical medical students; n = 46 | Motivational interviewing. | Educational intervention premised on the Learn, See, Practice, Prove, Do, Maintain pedagogical framework, comprising 2 × 2 h lectures, a 2 h role play triad session and 3 × 2 h small-group simulated patient encounters supported by scaffolding strategies. | Students who received brief MI training improved in knowledge and confidence from baseline to post-training; gains remained at 3 months. Brief MI skills improved across the simulation sessions. |
| Kaltman et al. (2015) | Enhancing motivational interviewing training in a family medicine clerkship | 3rd year medical students; n = 16 | Motivational interviewing. | An online learning community for enhanced training in motivational interviewing was developed for 3rd-year medical students. The website included educational materials about motivational interviewing, as well as problematic health behaviors, a repository of exemplar videos and student videos with feedback and a discussion board. Student participants were given the opportunity to record an encounter with a patient and to receive feedback on their use of motivational interviewing from a faculty member. | Student volunteers in the Family Medicine Clerkship at Georgetown University School of Medicine were randomized to enhanced training, which included the online learning community or training as usual. Students in the enhanced training arm were rated as having significantly higher scores in motivational interviewing style in the observed structured clinical exam than training-as-usual students. |
| Keifenheim et al. (2019) | “A change would do you good”: Training medical students in Motivational Interviewing using a blended-learning approach—A pilot evaluation | A mandatory MI course was implemented for sixth-semester medical students | Motivational interviewing. | A mandatory MI course/e-learning/blended learning is defined as a combination of e-learning and classical teaching formats, such as lectures and small groups. | This pilot study suggests that basic MI skills can be successfully taught in a blended-learning teaching approach. Further research should investigate sustainability and transfer to clinical practice. |
| King et al. (2015) | All the world’s a stage: evaluating psychiatry role-play based learning for medical students | A total of 107 students from three clinical schools of the University of Melbourne | All types (communication skills). | Role play-based learning (RBL), as a vehicle for teaching psychiatry. | Respondents were overwhelmingly positive about the sessions, reporting benefits for learning, communication skills, insight and confidence in managing both assessment tasks and real patients. |
| McKenzie et al. (2012) | Medical and psychology students’ knowledge of and attitudes towards mindfulness as a clinical intervention | A total of 91 medical students from Monash University, 49 medical students from Deakin University and 31 psychology students from Deakin University | Mindfulness. | All types of teaching compared to no teaching. | Medical students with exposure to mindfulness in their course have a greater knowledge of it and are more likely to administer it or recommend it compared to medical students without exposure. Knowledge of mindfulness is positively correlated with students’ willingness to use or recommend it. The inclusion of mindfulness exposure in medical courses and possibly also in psychology courses may help mindfulness fulfill its clinical potential and increasingly benefit patients who are suffering from a range of clinical conditions. |
| Merlo et al. (2022) | Introduction to Cognitive Restructuring for Medical Students | A total of 139 first-year medical students and 152 second-year medical students | Cognitve–behavioral therapy. | A 90-min learning activity, which included a short videotaped lecture, clinical case vignette, small-group discussion and application exercise. | Immediately following the learning activity, students and faculty completed anonymous evaluations. For the first-year cohort, upwards of 80% of students and 100% of faculty respondents rated the session either good or excellent. For the second-year cohort, over 80% of students and over 90% of faculty rated the session as either good or excellent. Approximately 90% of first- and second-year medical students and 100% of faculty recommended offering the session to future students. Open-ended feedback from students was overwhelmingly positive. |
| Mintz (2013) | Teaching psychoanalytic concepts, skills and attitudes to medical students | Medical students | Psychodynamic. | Multimodal approaches. | The authors argue that teaching psychoanalytic concepts to medical students (such as empathy, transference and the doctor–patient relationship) remains valuable despite their decline in curricula. They suggest practical ways to integrate these ideas through lectures, clinical experiences and electives. While challenges like limited resources and student resistance exist, incorporating psychodynamic perspectives can enhance professionalism, improve patient care and support recruitment into psychiatry. |
| Muzyk et al. (2019) | Behavior change counseling of patients with substance use disorders by health professions students | A total of 78 students from medicine, nursing, pharmacy, social work and physician assistant programs completed the one-month course, with 53 of them counseling a patient | Motivational interviewing. | Each course included four in-person classes with a total of six hours of instructional time. Class topics focused on (1) developing empathy and examining personal bias; (2) the behavioral change counseling model and implications for its use in healthcare settings; and (3) the recognition, screening and treatment of SUDs. Following these class sessions, students had an opportunity to counsel a patient with an SUD in the clinical setting using behavioral change counseling and receive observation, assessment and feedback from a faculty member experienced in this technique. | Students’ BECCI-rated counseling skills indicated that they performed the recommended counseling practices and spoke for “less than half the time” or for “about half the time” when counseling. A total of 93% of SUD patients reported a willingness for follow-up care about their substance use after the student-led session. |
| Neufeld et al. (2012) | A collaborative approach to teaching medical students how to screen, intervene and treat substance use disorders | Second- year medical students; n = 118 | Motivational interviewing. | A collaborative 15-h course using the SBIRT (Screening, Brief Intervention and Referral to Treatment) model to teach second-year medical students about substance use disorders. The 15-h course (39 faculty teaching hours) arose from a collaboration between faculties in the Departments of Medicine and Psychiatry and included 5 h of direct patient interaction during clinical demonstrations and in small-group skills development. | The course significantly improved students’ knowledge, as shown by a marked increase in post-test scores. Key features included interactive patient sessions, small-group skills training and interdepartmental collaboration between psychiatry and internal medicine. The course was well received and demonstrated the feasibility and effectiveness of experiential, integrated teaching on addiction in medical education. |
| Selzer et al. (2015) | Teaching psychological processes and psychotherapy to medical students | Medical students | All types. | Having a familiar information scaffold, as well as associating the teaching with a patient, makes the learning memorable, personal and relevant. Demonstrating this eclecticism shows that we can be flexible and suit the theory and practice to patient needs, that is, avoiding blind allegiance to one theory or another. | Teaching psychotherapy and psychological processes to medical students need not be difficult. We have described some of the techniques we have used successfully. |
| Truong et al. (2015) | What Is the Efficacy of Teaching Psychotherapy to Psychiatry Residents and Medical Students? | Medical students and residents | All types. | Multimodal approaches. | There is a need for more systematic evaluations and publications relating to psychotherapy teaching practices for both medical students and residents. Researchers are encouraged to study educational approaches across these groups, while training and clerkship directors should be surveyed on their content, methods and outcomes. |
| Article | BEME Score (0–11) | BEME Rating |
|---|---|---|
| Buck et al. (2021) | 8 | Moderate |
| Chéret et al. (2018) | 7.5 | Moderate |
| Daeppen et al. (2012) | 7 | Moderate |
| Dobkin and Hutchinson (2013) | 6.5 | Low |
| Edwards et al. (2022) | 8.5 | Moderate |
| Kaltman et al. (2015) | 8 | Moderate |
| Keifenheim et al. (2019) | 9 | High |
| King et al. (2015) | 8 | Moderate |
| McKenzie et al. (2012) | 6 | Low |
| Merlo et al. (2022) | 9 | High |
| Mintz (2013) | 7.5 | Moderate |
| Muzyk et al. (2019) | 10 | High |
| Neufeld et al. (2012) | 9.5 | High |
| Selzer et al. (2015) | 8.5 | Moderate |
| Truong et al. (2015) | 10.5 | High |
| Article | Study Design (0–3) | Sampling (0–3) | Type of Data (0–3) | Validity (0–3) | Analysis (0–3) | Outcomes (0–3) | Total MERSQI (0–18) | MERSQI Rating |
|---|---|---|---|---|---|---|---|---|
| Edwards et al. (2022) | 2 | 2 | 2 | 1 | 2 | 2 | 11 | Low |
| Keifenheim et al. (2019) | 2 | 2 | 2 | 2 | 2 | 2 | 12 | Moderate |
| King et al. (2015) | 2 | 2 | 2 | 1 | 2 | 2 | 11 | Low |
| Muzyk et al. (2019) | 2 | 2 | 2 | 2 | 3 | 3 | 14 | Moderate |
| Neufeld et al. (2012) | 2 | 2 | 2 | 1 | 2 | 2 | 11 | Low |
| Truong et al. (2015) | 3 | 3 | 2 | 2 | 3 | 3 | 16 | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garon, M.-H.; Létourneau, G.; Caron, D.; Renaud-Cloutier, L.; Désilets, M.; Hudon, A. Best Practices for Teaching Psychotherapy to Medical Students: A Scoping Review. Behav. Sci. 2025, 15, 780. https://doi.org/10.3390/bs15060780
Garon M-H, Létourneau G, Caron D, Renaud-Cloutier L, Désilets M, Hudon A. Best Practices for Teaching Psychotherapy to Medical Students: A Scoping Review. Behavioral Sciences. 2025; 15(6):780. https://doi.org/10.3390/bs15060780
Chicago/Turabian StyleGaron, Marie-Hélène, Geneviève Létourneau, David Caron, Léa Renaud-Cloutier, Marie Désilets, and Alexandre Hudon. 2025. "Best Practices for Teaching Psychotherapy to Medical Students: A Scoping Review" Behavioral Sciences 15, no. 6: 780. https://doi.org/10.3390/bs15060780
APA StyleGaron, M.-H., Létourneau, G., Caron, D., Renaud-Cloutier, L., Désilets, M., & Hudon, A. (2025). Best Practices for Teaching Psychotherapy to Medical Students: A Scoping Review. Behavioral Sciences, 15(6), 780. https://doi.org/10.3390/bs15060780