
Mindful Eating and Its Relationship with Obesity, Eating Habits, and Emotional Distress in Mexican College Students


 , ,
, ,  and
and 
Abstract
1. Introduction
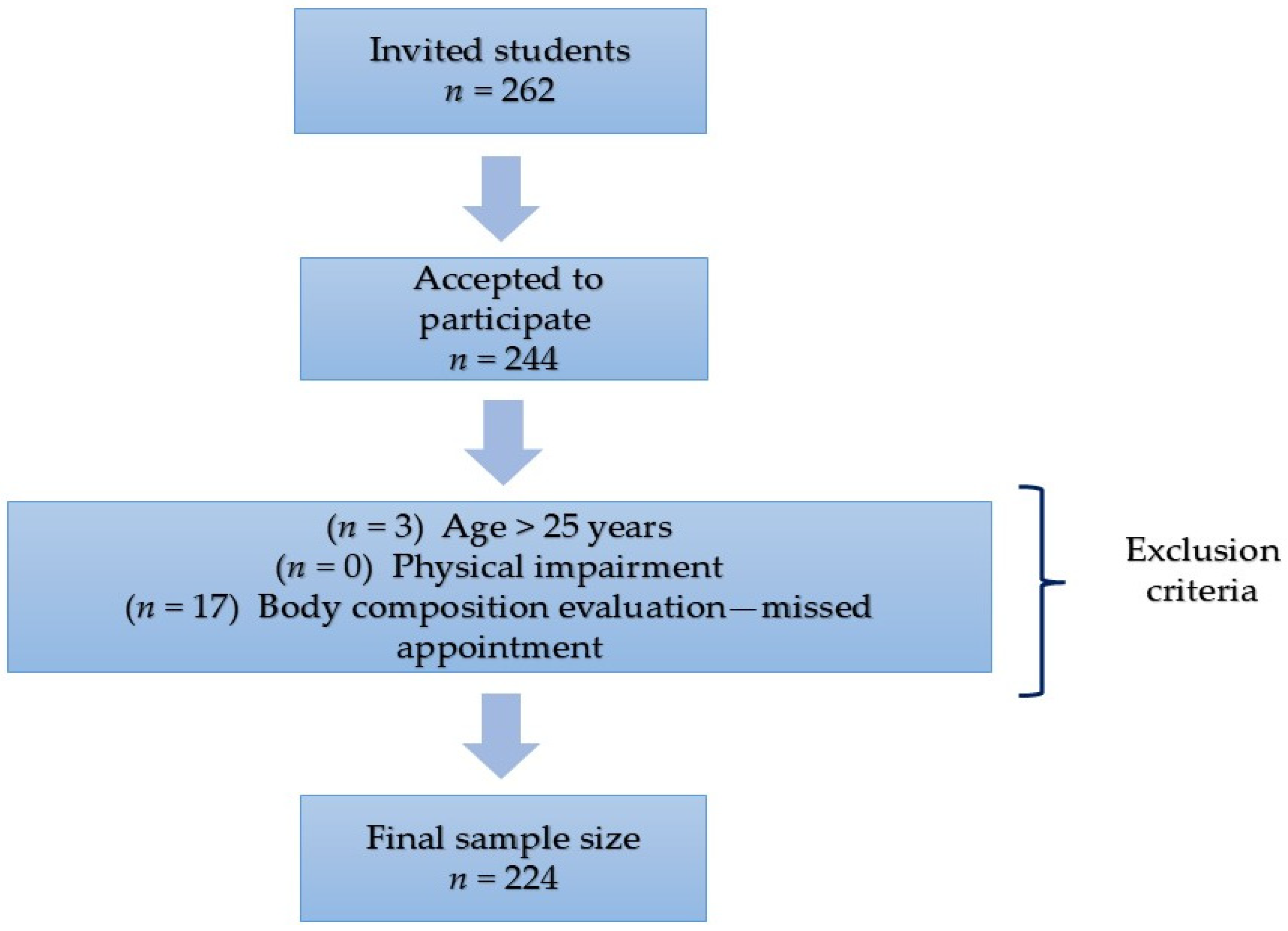
2. Materials and Methods
2.1. Anthropometric Measurements
2.2. Mindful Eating Instrument
2.3. Food Frequency Questionnaire
2.4. Depression, Anxiety, and Stress Scale (DASS-21)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ME | Mindful Eating |
| BMI | Body Mass Index |
| ME-11 | Mindful Eating Questionnaire, 11 items |
| ME-8 | Mindful Eating Questionnaire, 8 items |
| EE | Emotional Eating |
References
- Alvarenga, M. S., Scagliusi, F. B., & Philippi, S. T. (2010). Development and validity of the disordered eating attitude scale (DEAS). Perceptual and Motor Skills, 110(2), 379–395. [Google Scholar] [CrossRef]
- Antony, M., Bieling, P., Cox, B., Enns, M., & Swinson, R. (1998). Psychometric properties of the 42-item and 21-item versions of the depression anxiety stress scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181. [Google Scholar] [CrossRef]
- Antúnez, Z., & Vinet, E. (2012). Escalas de Depresión, Ansiedad y Estrés (DASS-21): Validación de la versión abreviada en estudiantes universitarios chilenos. Terapia Psicologica, 30, 49–55. [Google Scholar] [CrossRef]
- Aucoin, M., LaChance, L., Naidoo, U., Remy, D., Shekdar, T., Sayar, N., & Cooley, K. (2021). Diet and anxiety: A scoping review. Nutrients, 13(12), 4418. [Google Scholar] [CrossRef] [PubMed]
- Baer, R. (2019). Assessment of mindfulness by self-report. Current Opinion in Psychology, 28, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Beccia, A. L., Dunlap, C., Hanes, D. A., Courneene, B. J., & Zwickey, H. L. (2018). Mindfulness-based eating disorder prevention programs: A systematic review and meta-analysis. Mental Health & Prevention, 9, 1–12. [Google Scholar] [CrossRef]
- Beshara, M., Hutchinson, A. D., & Wilson, C. (2013). Does mindfulness matter? Everyday mindfulness, mindful eating and self-reported serving size of energy dense foods among a sample of South Australian adults. Appetite, 67, 25–29. [Google Scholar] [CrossRef]
- Bishop, S., Lau, M., Shapiro, S., Carlson, L., Anderson, N., Carmody, J., & Devins, G. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11, 230–241. [Google Scholar] [CrossRef]
- Brown, K., Ryan, R., & Creswell, J. (2007). Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18(4), 211–237. [Google Scholar] [CrossRef]
- Brown, T., Chorpita, B., Korotitsch, W., & Barlow, D. (1997). Psychometric properties of the depression anxiety stress scales (DASS) in clinical samples. Behaviour Research and Therapy, 35(1), 79–89. [Google Scholar] [CrossRef]
- Campos-Nonato, I., Galván-Valencia, O., Hernández-Barrera, L., Oviedo-Solís, C., & Barquera, S. (2023). Prevalencia de obesidad y factores de riesgo asociados en adultos mexicanos: Resultados de la Ensanut 2022. Salud Pública de México, 65(1), S238–S247. [Google Scholar] [CrossRef] [PubMed]
- Celik-Erden, S., Karakus-Yilmaz, B., Kozaci, N., Uygur, A. B., Yigit, Y., Karakus, K., Aydin, I. E., Ersahin, T., & Ersahin, D. A. (2023). The relationship between depression, anxiety, and stress levels and eating behavior in emergency service workers. Cureus, 15(2), e35504. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Rodríguez, J., González-Vázquez, R., Reyes-Castillo, P., Mayorga-Reyes, L., Nájera-Medina, O., & Ramos-Ibáñez, N. (2019). Dietary intake and body composition associated with metabolic syndrome in university students. Mexican Journal of Eating Disorders, 10(1), 42–52. [Google Scholar] [CrossRef]
- Dakanalis, A., Mentzelou, M., Papadopoulou, S. K., Papandreou, D., Spanoudaki, M., Vasios, G. K., Pavlidou, E., Mantzorou, M., & Giaginis, C. (2023). The association of emotional eating with overweight/obesity, depression, anxiety/stress, and dietary patterns: A review of the current clinical evidence. Nutrients, 15(5), 1173. [Google Scholar] [CrossRef]
- Demirbas, N., Kutlu, R., & Kurnaz, A. (2021). The relationship between mindful eating and body mass index and body compositions in adults. Annals of Nutrition and Metabolism, 77(5), 262–270. [Google Scholar] [CrossRef] [PubMed]
- Denova-Gutiérrez, E., Ramírez-Silva, I., Rodríguez-Ramírez, S., JiménezAguilar, A., Shamah-Levy, T., & Rivera-Dommarco, J. A. (2016). Validity of a food frequency questionnaire to assess food intake in Mexican adolescent and adult population. Salud Pública de Mexico, 58(6), 617–628. [Google Scholar] [CrossRef]
- Dogan, B. G., & Tengilimoglu-Metin, M. M. (2023). Does mindful eating affect the diet quality of adults? Nutrition, 110, 112010. [Google Scholar] [CrossRef]
- Durán, S., Crovetto, M., Espinoza, V., Mena, F., Oñate, G., Fernández, M., Coñuecar, S., Guerra, A., & Valladares, M. (2017). Caracterización del estado nutricional, hábitos alimentarios y estilos de vida de estudiantes universitarios chilenos: Estudio multicéntrico. Revista Medica de Chile, 145(11), 1403–1411. [Google Scholar] [CrossRef]
- Fernández-Carrasco, M. P., & López-Ortiz, M. M. (2019). Relation between eating habits and risk of developing diabetes in Mexican university students. Nutrición Clínica y Dietetica Hospitalaria, 39(4), 32–40. [Google Scholar] [CrossRef]
- Framson, C., Kristal, A. R., Schenk, J., Littman, A., Zeliadt, S., & Benitez, D. (2009). Development and validation of the Mindful Eating Questionnaire. Journal of American Dietetic Association, 109(8), 1439–1444. [Google Scholar] [CrossRef]
- Fulton, S., Décatirie-Spain, L., Fioramonto, X., Guiard, B., & Nakajima, S. (2021). The menace of obesity to depression and anxiety prevalence. Trends in Endocrinology & Metabolism, 33(1), 18–35. [Google Scholar] [CrossRef]
- Gallagher, D., Heymsfield, S. B., Heo, M., Jebb, S. A., Murgatroyd, P. R., & Sakamoto, Y. (2000). Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. The American Journal of Clinical Nutrition, 72(3), 694–701. [Google Scholar] [CrossRef]
- Gaona-Pineda, E. B., Rodríguez-Ramírez, S., Medina-Zacarías, M. C., Valenzuela-Bravo, D. G., Martínez-Tapia, B., & Arango-Angarita, A. (2023). Consumidores de grupos de alimentos en población mexicana. Ensanut Continua 2020–2022. Salud Pública de México, 65(Suppl. S1), S248–S258. [Google Scholar] [CrossRef] [PubMed]
- Giannopoulou, I., Kotopoulea-Nikolaidi, M., Daskou, S., Martyn, K., & Patel, A. (2020). Mindfulness in eating is inversely related to binge eating and mood disturbances in university students in health-related disciplines. Nutrients, 12(2), 396. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K. M., Gallo, L. C., & Afari, N. (2015). Mindfulness-based interventions for binge eating: A systematic review and meta-analysis. Journal of Behavioral Medicine, 38(2), 348–362. [Google Scholar] [CrossRef]
- Gradidge, P. J. L., & Cohen, E. (2018). Body mass index and associated lifestyle and eating behaviours of female students at a South African University. South African Journal of Clinical Nutrition, 31(4), 89–91. [Google Scholar] [CrossRef]
- Gurrola, G., Balcazar, P., Bonilla, M., & Virseda, J. (2006). Estructura factorial y consistencia interna de la escala de depresión ansiedad y estrés (DASS-21) en una muestra no clínica. Psicología y Ciencia Social, 8(2), 3–7. [Google Scholar]
- Hilger-Kolb, J., Loerbroks, A., & Diehl, K. (2017). Eating behaviour of university students in Germany: Dietary intake, barriers to healthy eating and changes in eating behaviour since the time of matriculation. Appetite, 109, 100–107. [Google Scholar] [CrossRef]
- Hill, D., Conner, M., Clancy, F., Moss, R., Wilding, S., & Bristow, M. (2022). Stress and eating behaviours in healthy adults: A systematic review and meta-analysis. Health Psychology Review, 16(2), 280–304. [Google Scholar] [CrossRef]
- Hinton, E. C., Beesley, V., Leary, S. D., & Ferriday, D. (2024). Associations between body mass index and episodic memory for recent eating, mindful eating, and cognitive distraction: A cross-sectional study. Obesity Science & Practice, 10(1), e728. [Google Scholar] [CrossRef]
- Hsu, T., & Forestell, C. A. (2021). Mindfulness, depression, and emotional eating: The moderating role of nonjudging of inner experience. Appetite, 160, 105089. [Google Scholar] [CrossRef]
- Jordan, C. H., Wang, W., Donatoni, L., & Meier, B. P. (2014). Mindful eating: Trait and state mindfulness predict healthier eating behavior. Personality and Individual Differences, 68, 107–111. [Google Scholar] [CrossRef]
- Keyte, R., Egan, H., & Mantzios, M. (2020). How does mindful eating without non-judgement, mindfulness and self-compassion relate to motivations to eat palatable foods in a student population? Nutrition and Health, 26(1), 27–34. [Google Scholar] [CrossRef]
- Kheniser, K., Saxon, D. R., & Kashyap, S. R. (2021). Long-term weight loss strategies for obesity. The Journal of Clinical Endocrinology & Metabolism, 106(7), 1854–1866. [Google Scholar] [CrossRef]
- Kim, K. S., Oh, H. J., Choi, Y. J., Huh, B. W., Kim, S. K., & Park, S. W. (2016). Reappraisal of waist circumference cutoff value according to general obesity. Nutrition & Metabolism, 13(1), 26. [Google Scholar] [CrossRef]
- Konttinen, H., van Strien, T., Männistö, S., Jousilahti, P., & Haukkala, A. (2019). Depression, emotional eating and long-term weight changes: A population-based prospective study. International Journal of Behavioral Nutrition and Physical Activity, 16(1), 28. [Google Scholar] [CrossRef]
- Kyle, U. G., Bosaeus, I., De Lorenzo, A. D., Deurenberg, P., Elia, M., Gómez, J. M., & Pichard, C. (2004). Bioelectrical impedance analysis—Part I: Review of principles and methods. Clinical Nutrition, 23(5), 1226–1243. [Google Scholar] [CrossRef]
- Lazarevich, I., Irigoyen-Camacho, M. E., Velazquez-Alva, M. C., Lara-Flores, N., Nájera-Medina, O., & Zepeda-Zepeda, M. A. (2018). Depression and food consumption in Mexican college students. Nutricion Hospitalaria, 35(3), 252–257. [Google Scholar] [CrossRef]
- Lingvay, I., Cohen, R. V., le Roux, C. W., & Sumothran, P. (2024). Obesity in adults. The Lancet, 404(10456), 972–987. [Google Scholar] [CrossRef]
- Lorenzini, R., Betancur-Ancona, D. A., Chel-Guerrero, L. A., Segura-Campos, M. R., & Castellanos-Ruelas, A. F. (2015). Estado nutricional en relación con el estilo de vida de estudiantes universitarios mexicanos. Nutricion Hospitalaria, 32(1), 94–100. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P., & Lovibond, S. (1995). The structure of negative emotional states: Comparison of the tDepression, Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335–343. [Google Scholar] [CrossRef]
- López-Nieves, G., Sosa-Cordobés, E., Garrido-Fernández, A., Travé-González, G., & García-Padilla, F. M. (2019). Hábitos, preferencias y habilidades culinarias de estudiantes de primer curso de la Universidad de Huelva. Enfermería Global, 18(3), 127–156. [Google Scholar] [CrossRef]
- Lyzwinski, L. N., Caffery, L., Bambling, M., & Edirippulige, S. (2018). A systematic review of electronic mindfulness-based therapeutic interventions for weight, weight-related behaviors, and psychological stress. Telemedicine and e-Health, 24(3), 173–184. [Google Scholar] [CrossRef] [PubMed]
- Mantzios, M., Egan, H., Bahia, H., Hussain, M., & Keyte, R. (2018a). How does grazing relate to body mass index, self-compassion, mindfulness and mindful eating in a student population? Health Psychology Open, 5(1), 2055102918762701. [Google Scholar] [CrossRef] [PubMed]
- Mantzios, M., Egan, H., Hussain, M., Keyte, R., & Bahia, H. (2018b). Mindfulness, self-compassion, and mindful eating in relation to fat and sugar consumption: An exploratory investigation. Eating and Weight Disorders-Studies of Anorexia, Bulimia and Obesity, 23(6), 833–840. [Google Scholar] [CrossRef]
- Mantzios, M., & Wilson, C. (2015). Mindfulness, eating behaviors, and obesity: A review and reflection on current findings. Current Obesity Report, 4(1), 141–146. [Google Scholar] [CrossRef]
- Mason, E., Epel, S., Aschbacher, K., Lustig, H., Acree, M., & Daubenmier, J. (2016). Reduced reward-driven eating accounts for the impact of a mindfulness-based diet and exercise intervention on weight loss: Data from the SHINE randomized controlled trial. Appetite, 100, 86–93. [Google Scholar] [CrossRef]
- Mercado, D., Robinson, L., Gordon, G., Werthmann, J., Campbell, I. C., & Schmidt, U. (2021). The outcomes of mindfulness-based interventions for obesity and binge eating disorder: A meta-analysis of randomized controlled trials. Appetite, 166, 105464. [Google Scholar] [CrossRef]
- Metin, Z. E., Bayrak, N., Celik, O. M., & Akkoca, M. (2024). The relationship between emotional eating, mindful eating, and depression in young adults. Food Science & Nutrition, 13(1), e4028. [Google Scholar] [CrossRef]
- Moor, K. R., Scott, A. J., & McIntosh, W. D. (2013). Mindful eating and its relationship to body mass index and physical activity among university students. Mindfulness, 4, 269–274. [Google Scholar] [CrossRef]
- Muñoz-Rodríguez, J. R., Luna-Castro, J., Ballesteros-Yáñez, I., Pérez-Ortiz, J. M., Gómez-Romero, F. J., & Redondo-Calvo, F. J. (2021). Influence of biomedical education on health and eating habits of university students in Spain. Nutrition, 86, 111181. [Google Scholar] [CrossRef] [PubMed]
- Olatona, F. A., Onabanjo, O. O., Ugbaja, R. N., Nnoaham, K. E., & Adelejan, D. A. (2018). Dietary habits and metabolic risk factors for non-communicable diseases in a university undergraduate population. Journal of Health, Population and Nutrition, 37(21), 21. [Google Scholar] [CrossRef]
- Olvera-Ruvalcaba, A. J., Gómez-Peresmitre, G., & Velasco-Rojano, E. (2019). Construction and validation of a mindful eating scale: A first approximation in the Mexican population. Mexican Journal of Eating Disorders, 10(2), 163–172. [Google Scholar] [CrossRef]
- Omage, K., & Omuemu, V. O. (2018). Assessment of dietary pattern and nutritional status of undergraduate students in a private university in southern Nigeria. Food Science & Nutrition, 6(7), 1890–1897. [Google Scholar] [CrossRef]
- Özkan, N., & Bilici, S. (2021). Are anthropometric measurements an indicator of intuitive and mindful eating? Eating and Weight Disorders. EWD, 26(2), 639–648. [Google Scholar] [CrossRef]
- Paolassini-Guesnier, P., Van Beekum, M., Kesse-Guyot, E., Baudry, J., Bernard-Srour, B., Bellicha, A., & Péneau, S. (2025). Mindful eating is associated with a better diet quality in the NutriNet-Santé study. Appetite, 206, 107797. [Google Scholar] [CrossRef]
- Pepe, R. B., Coelho, G. S. M. A., Miguel, F. D. S., Gualassi, A. C., Sarvas, M. M., Cercato, C., & de Melo, M. E. (2023). Mindful eating for weight loss in women with obesity: A randomized controlled trial. British Journal of Nutrition, 130(5), 911–920. [Google Scholar] [CrossRef]
- Pintado-Cucarella, S., & Rodriguez-Salgado, P. (2016). Mindful eating and its relationship with body mass index, binge eating, anxiety, and negative affect. Journal of Behavior, Health & Social Issues, 8, 19–24. [Google Scholar] [CrossRef]
- Ruiz-Fuentes, S., & Llorca, G. (2016). Mindful eating and eating styles in disorders of eating behavior. Agora de Salut, 3(36), 339–345. [Google Scholar] [CrossRef]
- Sala, M., Ram, S. S., Vanzhula, I. A., & Levinson, C. A. (2020). Mindfulness and eating disorder psychopathology: A meta-analysis. Eating Disorders, 53(6), 834–851. [Google Scholar] [CrossRef]
- Sala, M., Vanzhula, I., Roos, C. R., & Levinson, C. A. (2022). Mindfulness and eating disorders: A network analysis. Behavior Therapy, 5(2), 224–239. [Google Scholar] [CrossRef] [PubMed]
- Shamah-Levy, T., Romero-Martínez, M., Barrientos-Gutiérrez, T., Cuevas-Nasu, L., Bautista-Arredondo, S., Colchero, M. A., & Rivera-Dommarco, J. (2022). Encuesta nacional de salud y nutrición 2021 sobre COVID-19. Instituto Nacional de Salud Pública. Available online: https://www.insp.mx/resources/images/stories/2022/docs/220801_Ensa21_digital_29julio.pdf (accessed on 10 January 2025).
- Tanofsky-Kraff, M., & Yanovski, S. Z. (2004). Eating disorder or disordered eating? Non-normative eating patterns in obese individuals. Obesity Research, 12(9), 1361–1366. [Google Scholar] [CrossRef]
- Tapper, K. (2022). Mindful eating: What we know so far. Nutrition Bulletin, 47(2), 168–185. [Google Scholar] [CrossRef] [PubMed]
- Turgon, R., Ruffault, A., Juneau, C., Blatier, C., & Shankland, R. (2019). Eating disorder treatment: Systematic review and meta-analysis of the efficacy of mindfulness-based programs. Mindfulness, 10, 2225–2244. [Google Scholar] [CrossRef]
- Vittengl, J. R. (2018). Mediation of the bidirectional relations between obesity and depression among women. Psychiatry Research, 264, 254–259. [Google Scholar] [CrossRef]
- Warren, M., Smith, N., & Ashwell, M. (2017). A structured literature review on the role of mindfulness, mindful eating and intuitive eating in changing eating behaviours: Effectiveness and associated potential mechanisms. Nutrition Research Reviews, 30(2), 272–283. [Google Scholar] [CrossRef] [PubMed]
- Winkens, L. H. H., Elstgeest, L. E. M., van Strien, T., Penninx, B. W. J. H., Visser, M., & Brouwer, I. A. (2020). Does food intake mediate the association between mindful eating and change in depressive symptoms? Public Health Nutrition, 23(9), 1532–1542. [Google Scholar] [CrossRef]
- Winkens, L. H. H., van Strien, T., Brouwer, I. A., Penninx, B. W. J. H., Visser, M., & Lähteenmäki, L. (2018). Associations of mindful eating domains with depressive symptoms and depression in three European countries. Journal of Affective Disorders, 1(228), 26–32. [Google Scholar] [CrossRef]
- World Health Organization (WHO). (2000). Physical status: The use of and interpretation of anthropometry, report of a WHO expert committee. WHO technical report series 894. Available online: https://apps.who.int/iris/handle/10665/37003 (accessed on 15 January 2025).
- World Health Organization (WHO). (2024). Obesity and overweight. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 29 November 2024).

{kind=link}
| Variable | Mean (± SD) or n (%) |
|---|---|
| Age (years) | 21.95 ± 2.16 |
| Sex | |
| Female | 173 (77.23) |
| Male | 51 (22.77) |
| Body Mass Index (kg/m2) | |
| (mean ± SD) | 24.21 ± 3.88 |
| Normal (≥18.5 and <25) | 138 (61.61) |
| Overweight/obesity (≥25) | 86 (38.39) |
| Waist Circumference (cm) (cutoff values females ≥80, males ≥90) | |
| Normal | 148 (66.07) |
| High | 76 (33.93) |
| Body Fat (%) (cutoff values females ≥ 33, males ≥ 20) | |
| Normal | 108 (48.21) |
| High | 116 (51.79) |
| Mindful Eating Score (ME-11) (mean ± SD) | 26.71 ± 8.62 |
| Mindful Eating Score (excluding emotional eating items, ME-8) (mean ± SD) | 19.85 ± 7.03 |
| Emotional Distress (DASS-21) 1 (mean ± SD) | |
| Depression score | 16.27 ± 4.59 |
| Anxiety score | 17.65 ± 4.66 |
| Stress score | 14.21 ± 3.82 |
| Food Consumption | |
| Sweetened Beverages | |
| ≥2 times per week | 98 (43.75) |
| <2 times per week | 126 (56.25) |
| Sweetened Dairy Drinks | |
| ≥2 times per week | 61 (27.23) |
| <2 times per week | 163 (72.77) |
| Fried Foods | |
| ≥1 time per week | 173 (77.23) |
| <1 time per week | 51 (22.77) |
| Sweets and Desserts | |
| ≥1 time per week | 168 (75.00) |
| <1 time per week | 56 (25.00) |
| Sweetened Cereals | |
| ≥1 time per week | 60 (26.79) |
| <1 time per week | 164 (73.21) |
| Fast Food | |
| ≥1 time per week | 138 (61.61) |
| <1 time per week | 86 (38.39) |
| Mexican Snacks | |
| ≥1 time per week | 149 (66.52) |
| <1 time per week | 75 (33.48) |
| Processed Meat | |
| ≥1 time per week | 148 (66.07) |
| <1 time per week | 76 (33.93) |
| Alcohol | |
| ≥2 times per week | 80 (35.71) |
| <2 times per week | 144 (64.29) |
| (a) ME-11 | |||
| Outcome Variable | OR (95% CI) 1 | p | |
| Body Mass Index 3 | |||
| Mindful eating score (ME-11) 2 | 1.08 (1.04–1.12) | <0.001 | |
| Waist Circunference 4 | |||
| Mindful eating score (ME-11) 2 | 1.09 (1.04–1.13) | <0.001 | |
| Body Fat (%) 5 | |||
| Mindful eating score (ME-11) 2 | 1.06 (1.02–1.10) | <0.001 | |
| (b) ME-8 | |||
| Outcome Variable | OR (95% CI) 1 | p | |
| Body Mass Index 3 | |||
| Mindful eating score (ME-8) 2 | 1.10 (1.05–1.15) | <0.001 | |
| Waist Circunference 4 | |||
| Mindful eating score (ME-8) 2 | 1.11 (1.06–1.16) | <0.001 | |
| Body Fat (%) 5 | |||
| Mindful eating score (ME-8) 2 | 1.98 (1.03–1.13) | <0.001 | |
| (a) ME-11 | |||
| Outcome Variable | OR (95% CI) 1 | p | |
| Sweetened Beverages 3 | |||
| Mindful eating score (ME-11) 2 | 1.01 (0.98–1.05) | 0.468 | |
| Sweetened Dary Drinks 3 | |||
| Mindful eating score (ME-11) 2 | 1.02 (0.99–1.06) | 0.224 | |
| Fried Food 4 | |||
| Mindful eating score (ME-11) 2 | 1.06 (1.02–1.11) | 0.005 | |
| Sweets and Desserts 4 | |||
| Mindful eating score (ME-11) 2 | 1.07 (1.02–1.11) | 0.003 | |
| Sweetened Cereals 4 | |||
| Mindful eating score (ME-11) 2 | 1.01 (0.97–1.05) | 0.656 | |
| Fast Food 4 | |||
| Mindful eating score (ME-11) 2 | 1.05 (1.02–1.09) | 0.003 | |
| Mexican Snacks 4 | |||
| Mindful eating score (ME-11) 2 | 1.00 (0.97–1.04) | 0.867 | |
| Procesesed Meat 4 | |||
| Mindful eating score (ME-11) 2 | 1.00 (0.98–1.04) | 0.610 | |
| Alcohol 3 | |||
| Mindful eating score (ME-11) 2 | 1.03 (0.99–1.06) | 0.126 | |
| (b) ME-8 | |||
| Outcome Variable | OR (95% CI) 1 | p | |
| Sweetened Beverages 3 | |||
| Mindful eating score (ME-8) 2 | 1.01 (0.97–1.05) | 0.621 | |
| Sweetened Dary Drinks 3 | |||
| Mindful eating score (ME-8) 2 | 1.02 (0.97–1.06) | 0.457 | |
| Fried Food 4 | |||
| Mindful eating score (ME-8) 2 | 1.06 (1.01–1.11) | 0.024 | |
| Sweets and Desserts 4 | |||
| Mindful eating score (ME-8) 2 | 1.06 (1.01–1.12) | 0.026 | |
| Sweetened Cereals 4 | |||
| Mindful eating score (ME-8) 2 | 1.00 (0.96–1.05) | 0.974 | |
| Fast Food 4 | |||
| Mindful eating score (ME-8) 2 | 1.05 (1.01–1.10) | 0.020 | |
| Mexican Snacks 4 | |||
| Mindful eating score (ME-8) 2 | 1.00 (0.96–1.04) | 0.897 | |
| Procesesed Meat 4 | |||
| Mindful eating score (ME-8) 2 | 1.00 (0.97–1.04) | 0.938 | |
| Alcohol 3 | |||
| Mindful eating score (ME-11) 2 | 1.02 (0.98–1.06) | 0.429 | |
| (a) ME-11 | |||
| Mindful Eating, Including All Items of the Questionnaire (ME-11) 2 Outcome Variable | Predictor Variables | OR (95% CI) | p |
| Low Score (Tertile 1, reference) | |||
| Medium Score (Tertile 2) | Depression Score | 1.04 (0.97–1.12) | 0.253 |
| Age | 1.04 (0.94–1.15) | 0.466 | |
| Sex (Female = 1) | 1.51 (0.74–3.09) | 0.253 | |
| High Score (Tertile 3) | Depression Score | 1.14 (1.05–1.24) | <0.001 |
| Age | 1.03 (0.92–1.14) | 0.642 | |
| Sex (Female = 1) | 5.91 (2.22–15.73) | <0.001 | |
| Medium Score (Tertile 2) | Anxiety Score | 1.06 (0.99–1.14) | 0.112 |
| Age | 1.04 (0.94–1.16) | 0.425 | |
| Sex (Female = 1) | 1.49 (0.73–3.05) | 0.273 | |
| High Score (Tertile 3) | Anxiety Score | 1.19 (1.09–1.29) | <0.001 |
| Age | 1.04 (0.93–1.16) | 0.488 | |
| Sex (Female = 1) | 5.89 (2.17–15.97) | <0.001 | |
| Medium Score (Tertile 2) | Stress Score | 1.06 (0.98–1.16) | 0.150 |
| Age | 1.04 (0.94–1.15) | 0.473 | |
| Sex (Female = 1) | 1.44 (0.71–2.95) | 0.315 | |
| High Score (Tertile 3) | Stress Score | 1.15 (1.05–1.27) | 0.003 |
| Age | 1.03 (0.92–1.14) | 0.631 | |
| Sex (Female = 1) | 5.24 (1.98–13.86) | <0.001 | |
| (b) ME-8 | |||
| Mindful Eating Score, Excluding Emotional Eating Items of the Questionnaire (ME-8) 2 Outcome Variable | Predictor Variable | OR (95% CI) | p |
| Low Score (Tertile 1, reference) | |||
| Medium Score (Tertile 2) | Depression Score | 1.06 (0.99–1.14) | 0.078 |
| Age | 1.07 (0.96–1.19) | 0.241 | |
| Sex (Female = 1) | 2.51 (1.21–5.22) | 0.014 | |
| High Score (Tertile 3) | Depression Score | 1.11 (1.02–1.20) | 0.011 |
| Age | 1.04 (0.93–1.17) | 0.490 | |
| Sex (Female = 1) | 5.90 (2.24–15.54) | <0.001 | |
| Medium Score (Tertile 2) | Anxiety Score | 1.08 (1.01–1.16) | 0.026 |
| Age | 1.07 (0.96–1.20) | 0.207 | |
| Sex (Female = 1) | 2.45 (1.18–5.12) | 0.017 | |
| High Score (Tertile 3) | Anxiety Score | 1.13 (1.05–1.23) | 0.002 |
| Age | 1.05 (0.93–1.18) | 0.404 | |
| Sex (Female = 1) | 5.74 (2.17–15.22) | <0.001 | |
| Medium Score (Tertile 2) | Stress Score | 1.10 (1.01–1.20) | 0.031 |
| Age | 1.07 (0.96–1.19) | 0.243 | |
| Sex (Female = 1) | 2.35 (1.13–4.90) | 0.023 | |
| High Score (Tertile 3) | Stress Score | 1.12 (1.02–1.23) | 0.017 |
| Age | 1.04 (0.93–1.17) | 0.494 | |
| Sex (Female = 1) | 5.40 (2.24–15.54) | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lazarevich, I.; Irigoyen-Camacho, M.E.; Radilla-Vázquez, C.C.; Gutiérrez-Tolentino, R.; Velazquez-Alva, M.C.; Zepeda-Zepeda, M.A. Mindful Eating and Its Relationship with Obesity, Eating Habits, and Emotional Distress in Mexican College Students. Behav. Sci. 2025, 15, 669. https://doi.org/10.3390/bs15050669
Lazarevich I, Irigoyen-Camacho ME, Radilla-Vázquez CC, Gutiérrez-Tolentino R, Velazquez-Alva MC, Zepeda-Zepeda MA. Mindful Eating and Its Relationship with Obesity, Eating Habits, and Emotional Distress in Mexican College Students. Behavioral Sciences. 2025; 15(5):669. https://doi.org/10.3390/bs15050669
Chicago/Turabian StyleLazarevich, Irina, María Esther Irigoyen-Camacho, Claudia Cecilia Radilla-Vázquez, Rey Gutiérrez-Tolentino, Maria Consuelo Velazquez-Alva, and Marco Antonio Zepeda-Zepeda. 2025. "Mindful Eating and Its Relationship with Obesity, Eating Habits, and Emotional Distress in Mexican College Students" Behavioral Sciences 15, no. 5: 669. https://doi.org/10.3390/bs15050669
APA StyleLazarevich, I., Irigoyen-Camacho, M. E., Radilla-Vázquez, C. C., Gutiérrez-Tolentino, R., Velazquez-Alva, M. C., & Zepeda-Zepeda, M. A. (2025). Mindful Eating and Its Relationship with Obesity, Eating Habits, and Emotional Distress in Mexican College Students. Behavioral Sciences, 15(5), 669. https://doi.org/10.3390/bs15050669