
Optimal Non-Pharmacological Interventions for Reducing Problematic Internet Use in Youth: A Systematic Review and Bayesian Network Meta-Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Methods
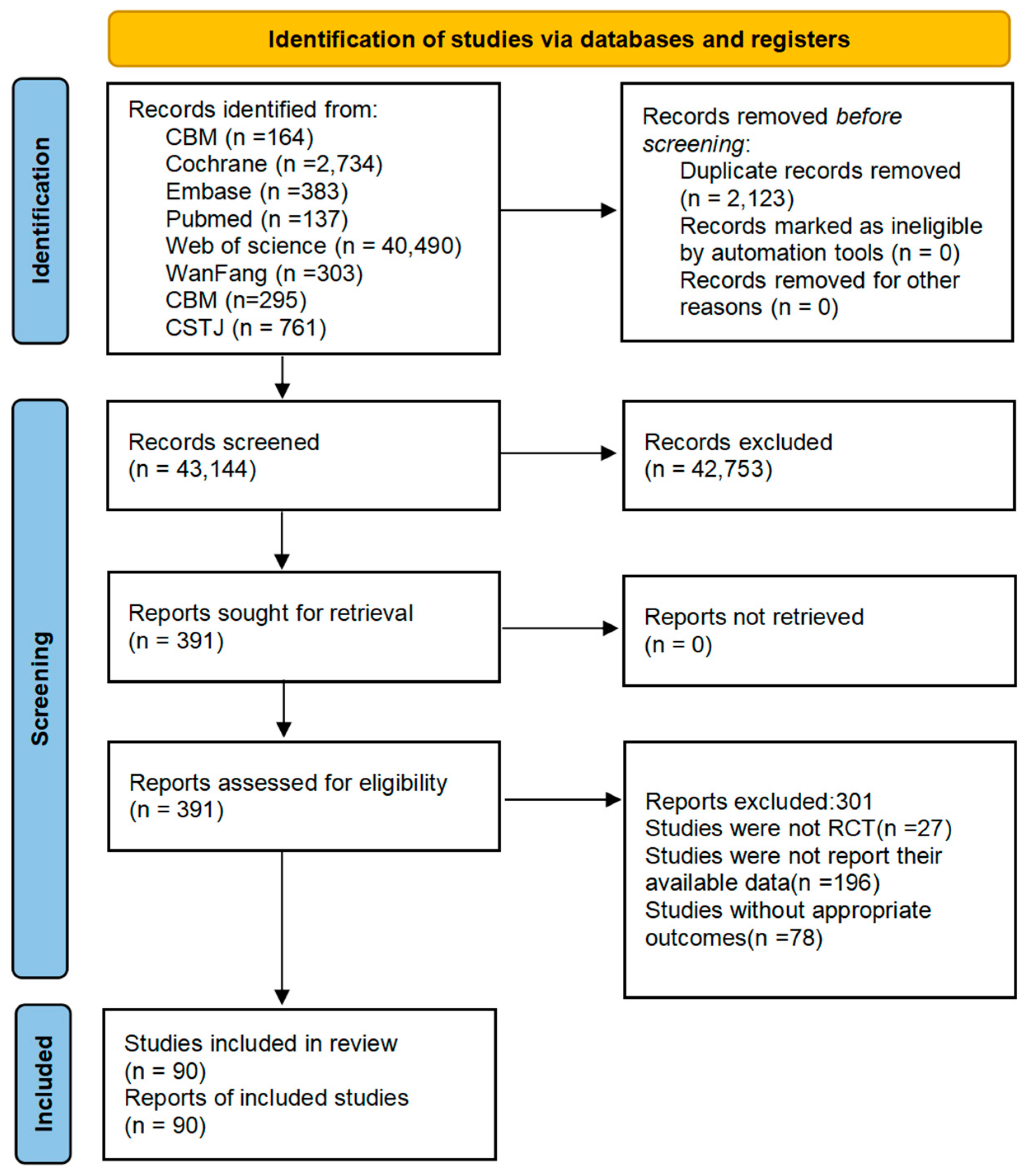
2.1. Literature Research
2.2. Inclusion and Exclusion Criteria
2.3. Outcome Measurement and Quality Appraisal
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics and ROB Quality of Included Studies
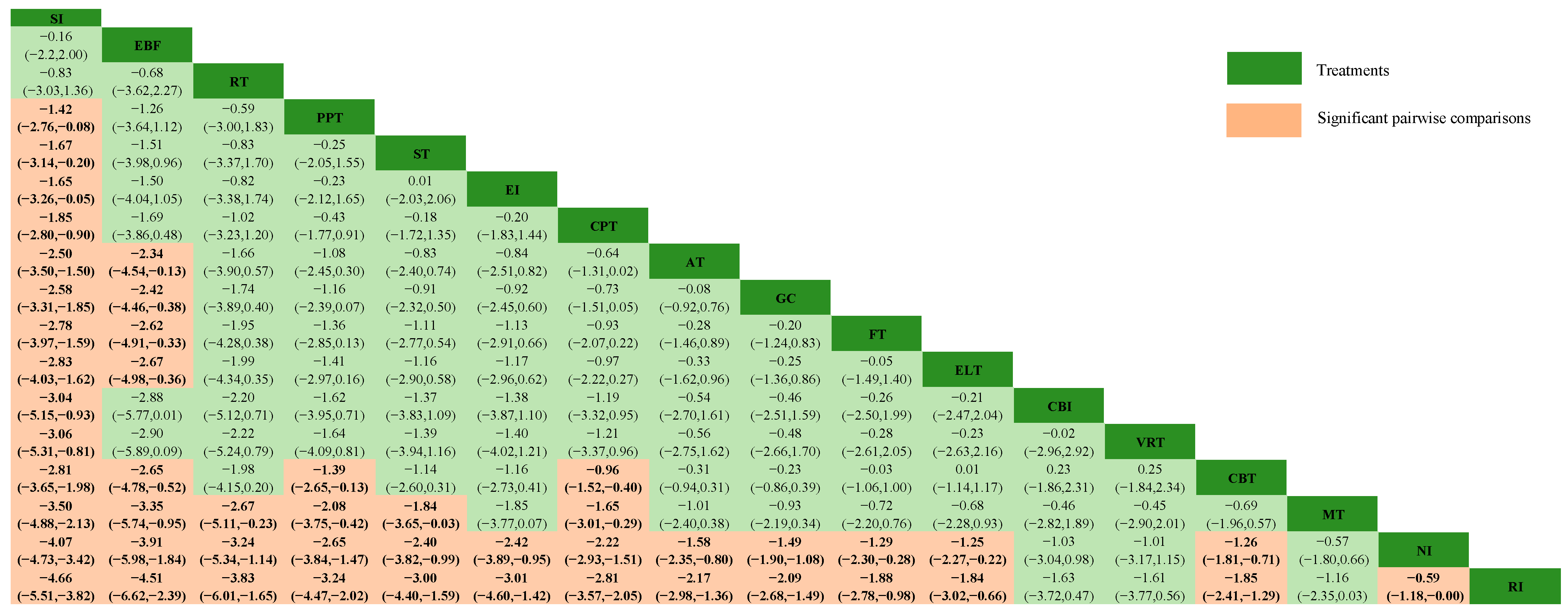
3.2. Results of the Pairwise and Network Meta-Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adalıer, A., & Balkan, E. (2012). The relationship between internet addiction and psychological symptoms. International Journal of Global Education (IJGE), 1(2), 45–48. [Google Scholar]
- Altman, D. G., & Bland, J. M. (1996). Statistics notes: Detecting skewness from summary information. BMJ, 313(7066), 1200. [Google Scholar] [CrossRef]
- Banerjee, S., Hellier, J., Dewey, M., Romeo, R., Ballard, C., Baldwin, R., Bentham, P., Fox, C., Holmes, C., Katona, C., Knapp, M., Lawton, C., Lindesay, J., Livingston, G., McCrae, N., Moniz-Cook, E., Murray, J., Nurock, S., Orrell, M., & Burns, A. (2011). Sertraline or mirtazapine for depression in dementia (HTA-SADD): A randomised, multicentre, double-blind, placebo-controlled trial. Lancet, 378(9789), 403–411. [Google Scholar] [CrossRef]
- Bastioli, G., Arnold, J. C., Mancini, M., Mar, A. C., Gamallo-Lana, B., Saadipour, K., Chao, M. V., & Rice, M. E. (2022). Voluntary exercise boosts striatal dopamine release: Evidence for the necessary and sufficient role of BDNF. Journal of Neuroscience, 42(23), 4725–4736. [Google Scholar] [CrossRef] [PubMed]
- Burton, J. K., Craig, L. E., Yong, S. Q., Siddiqi, N., Teale, E. A., Woodhouse, R., Barugh, A. J., Shepherd, A. M., Brunton, A., Freeman, S. C., Sutton, A. J., & Quinn, T. J. (2021). Non-pharmacological interventions for preventing delirium in hospitalised non-ICU patients. Cochrane Database of Systematic Reviews, 11(11), CD013307. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J., Cumpston, M., Li, T., Page, M. J., & Welch, V. (2019). Cochrane handbook for systematic reviews of interventions. Wiley. [Google Scholar]
- Dai, Y. K., Wu, Y. B., Li, R. L., Chen, W. J., Tang, C. Z., Lu, L. M., & Hu, L. (2020). Efficacy and safety of non-pharmacological interventions for irritable bowel syndrome in adults. World Journal of Gastroenterology, 26(41), 6488–6509. [Google Scholar] [CrossRef] [PubMed]
- De Crescenzo, F., D’Alò, G. L., Ostinelli, E. G., Ciabattini, M., Di Franco, V., Watanabe, N., Kurtulmus, A., Tomlinson, A., Mitrova, Z., Foti, F., Del Giovane, C., Quested, D. J., Cowen, P. J., Barbui, C., Amato, L., Efthimiou, O., & Cipriani, A. (2022). Comparative effects of pharmacological interventions for the acute and long-term management of insomnia disorder in adults: A systematic review and network meta-analysis. Lancet, 400(10347), 170–184. [Google Scholar] [CrossRef]
- Follmann, D., Elliott, P., Suh, I., & Cutler, J. (1992). Variance imputation for overviews of clinical trials with continuous response. Journal of Clinical Epidemiology, 45(7), 769–773. [Google Scholar] [CrossRef]
- Hedges, L. V. (1984). Advances in statistical methods for meta-analysis. New Directions for Program Evaluation, 24, 25–42. [Google Scholar] [CrossRef]
- Hutton, B., Salanti, G., Caldwell, D. M., Chaimani, A., Schmid, C. H., Cameron, C., Ioannidis, J. P. A., Straus, S., Thorlund, K., Jansen, J. P., Mulrow, C., Catalá-López, F., Gøtzsche, P. C., Dickersin, K., Boutron, I., Altman, D. G., & Moher, D. (2015). The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Annals of Internal Medicine, 162(11), 777–784. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y. -S., Liu, T. -H., Qin, D., Wang, Z. -P., He, X. -Y., & Chen, Y. -N. (2024). Effects of non-pharmacological interventions on youth with internet addiction: A systematic review and meta-analysis of randomized controlled trials. Frontiers in Psychiatry, 14, 1327200. [Google Scholar] [CrossRef] [PubMed]
- Kim, J. E., Son, J. W., Choi, W. H., Kim, Y. R., Oh, J. H., Lee, S., & Kim, J. K. (2014). Neural responses to various rewards and feedback in the brains of adolescent Internet addicts detected by functional magnetic resonance imaging. Psychiatry and Clinical Neurosciences, 68(6), 463–470. [Google Scholar] [CrossRef]
- King, D. L., Delfabbro, P. H., Potenza, M. N., Demetrovics, Z., Billieux, J., & Brand, M. (2018). Internet gaming disorder should qualify as a mental disorder. Australian & New Zealand Journal of Psychiatry, 52(7), 615–617. [Google Scholar]
- Lizarte Simón, E. J., Khaled Gijón, M., Galván Malagón, M. C., & Gijón Puerta, J. (2024). Challenge-obstacle stressors and cyberloafing among higher vocational education students: The moderating role of smartphone addiction and Maladaptive. Frontiers in Psychology, 15, 1358634. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Blasco, R., Robres, A. Q., & Sánchez, A. S. (2022). Internet addiction in young adults: A meta-analysis and systematic review. Computers in Human Behavior, 130, 107201. [Google Scholar] [CrossRef]
- Lu, G., & Ades, A. E. (2004). Combination of direct and indirect evidence in mixed treatment comparisons. Statistics in Medicine, 23(20), 3105–3124. [Google Scholar] [CrossRef] [PubMed]
- Lu, J. -X., Zhai, Y. -J., Chen, J., Zhang, Q. -H., Chen, T. -Z., Lu, C. -L., Jiang, Z. -L., Guo, L., & Zheng, H. (2023). Network analysis of internet addiction and sleep disturbance symptoms. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 125, 110737. [Google Scholar] [CrossRef] [PubMed]
- Melsen, W. G., Bootsma, M. C., Rovers, M. M., & Bonten, M. J. (2014). The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clinical Microbiology and Infection, 20(2), 123–129. [Google Scholar] [CrossRef] [PubMed]
- Meng, S. -Q., Cheng, J. -L., Li, Y. -Y., Yang, X. -Q., Zheng, J. -W., Chang, X. -W., Shi, Y., Chen, Y., Lu, L., Sun, Y., Bao, Y. -P., & Shi, J. (2022). Global prevalence of digital addiction in general population: A systematic review and meta-analysis. Clinical Psychology Review, 92, 102128. [Google Scholar] [CrossRef] [PubMed]
- Nakshine, V. S., Thute, P., Khatib, M. N., & Sarkar, B. (2022). Increased screen time as a cause of declining physical, psychological health, and sleep patterns: A literary review. Cureus, 14(10), e30051. [Google Scholar] [CrossRef]
- Nam, B., Bae, S., Kim, S. M., Hong, J. S., & Han, D. H. (2017). Comparing the effects of bupropion and escitalopram on excessive internet game play in patients with major depressive disorder. Clinical Psychopharmacology and Neuroscience, 15(4), 361–368. [Google Scholar] [CrossRef] [PubMed]
- Poon, K. -T. (2018). Unpacking the mechanisms underlying the relation between ostracism and internet addiction. Psychiatry Research, 270, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Rücker, G., & Schwarzer, G. (2015). Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Medical Research Methodology, 15, 58. [Google Scholar] [CrossRef] [PubMed]
- Salanti, G. (2012). Indirect and mixed-treatment comparison, network, or multiple-treatments meta-analysis: Many names, many benefits, many concerns for the next generation evidence synthesis tool. Research Synthesis Methods, 3(2), 80–97. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y., Cao, X., Tan, T., Shan, C., Wang, Y., Pan, J., He, H., & Yuan, T. F. (2016). 10-Hz repetitive transcranial magnetic stimulation of the left dorsolateral prefrontal cortex reduces heroin cue craving in long-term addicts. Biological Psychiatry, 80(3), e13–e14. [Google Scholar] [CrossRef]
- Sterne, J. A., & Egger, M. (2001). Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. Journal of Clinical Epidemiology, 54(10), 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Stevens, M. W. R., King, D. L., Dorstyn, D., & Delfabbro, P. H. (2019). Cognitive-behavioral therapy for Internet gaming disorder: A systematic review and meta-analysis. Clinical Psychology & Psychotherapy, 26(2), 191–203. [Google Scholar] [CrossRef]
- Strafella, A. P., Paus, T., Barrett, J., & Dagher, A. (2001). Repetitive transcranial magnetic stimulation of the human prefrontal cortex induces dopamine release in the caudate nucleus. Journal of Neuroscience, 21(15), Rc157. [Google Scholar] [CrossRef] [PubMed]
- Thorlund, K., & Mills, E. J. (2012). Sample size and power considerations in network meta-analysis. Systematic Reviews, 1, 41. [Google Scholar] [CrossRef] [PubMed]
- Wu, J., Du, Z. -Z., Tan, Y., & Zhou, Z. -L. (2019). The relative validity of exercise prescription: Net work meta-analysis of 4 measures in the intervention of adolescent internet addiction. Sports & Science, 40(5), 97–106+112. [Google Scholar] [CrossRef]
- Wu, J., Zhan, H., Du, Z. -Z., & Wu, W. -J. (2018). Meta analysis for exercise prescription interferes with the effect of adolescent internet addiction disorder. Sports & Science, 39(3), 46–54. [Google Scholar] [CrossRef]
- Yang, C. -Y., & Zeng, G. -F. (2017). The effect of tai chi exercise on college students’ internet addiction. Chinese Journal of School Health, 38(2), 292–294. [Google Scholar] [CrossRef]
- Young, K. S. (1996). Psychology of computer use: XL. Addictive use of the Internet: A case that breaks the stereotype. Psychological Reports, 79(3), 899–902. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X., Zhang, J., Zhang, K., Ren, J., Lu, X., Wang, T., Yang, H., Guo, H., Yuan, G., Zhu, Z., Hao, J., Sun, Y., Su, P., Yang, L., & Zhang, Z. (2022). Effects of different interventions on internet addiction: A meta-analysis of random controlled trials. Journal of Affective Disorders, 313, 56–71. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y., Liang, W., Yang, S., Dai, P., Shen, L., & Wang, C. (2013). Repetitive transcranial magnetic stimulation for hallucination in schizophrenia spectrum disorders A meta-analysis. Neural Regeneration Research, 8(28), 2666–2676. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y., Chen, H., Li, J., Mei, X., & Wang, W. (2023). Effects of different interventions on internet addiction: A systematic review and network meta-analysis. BMC Psychiatry, 23(1), 921. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, J.-J.; He, X.-Y.; Guo, Z. Optimal Non-Pharmacological Interventions for Reducing Problematic Internet Use in Youth: A Systematic Review and Bayesian Network Meta-Analysis. Behav. Sci. 2025, 15, 98. https://doi.org/10.3390/bs15010098
Tian J-J, He X-Y, Guo Z. Optimal Non-Pharmacological Interventions for Reducing Problematic Internet Use in Youth: A Systematic Review and Bayesian Network Meta-Analysis. Behavioral Sciences. 2025; 15(1):98. https://doi.org/10.3390/bs15010098
Chicago/Turabian StyleTian, Jing-Jing, Xiao-Ya He, and Zhen Guo. 2025. "Optimal Non-Pharmacological Interventions for Reducing Problematic Internet Use in Youth: A Systematic Review and Bayesian Network Meta-Analysis" Behavioral Sciences 15, no. 1: 98. https://doi.org/10.3390/bs15010098
APA StyleTian, J.-J., He, X.-Y., & Guo, Z. (2025). Optimal Non-Pharmacological Interventions for Reducing Problematic Internet Use in Youth: A Systematic Review and Bayesian Network Meta-Analysis. Behavioral Sciences, 15(1), 98. https://doi.org/10.3390/bs15010098