
Psychometric Evaluation and Misophonic Experience in a Portuguese-Speaking Sample

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Measures
2.2.1. Selective Sound Sensitivity Syndrome Scale (S-Five) [20]
2.2.2. Translation Procedure
2.2.3. Other Measures
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. S-Five Statements
3.2.1. Statement Responses
3.2.2. Dimensionality and Measurement Invariance
3.2.3. Scores, Reliability, and Validity
3.3. S-Five Trigger Checklist
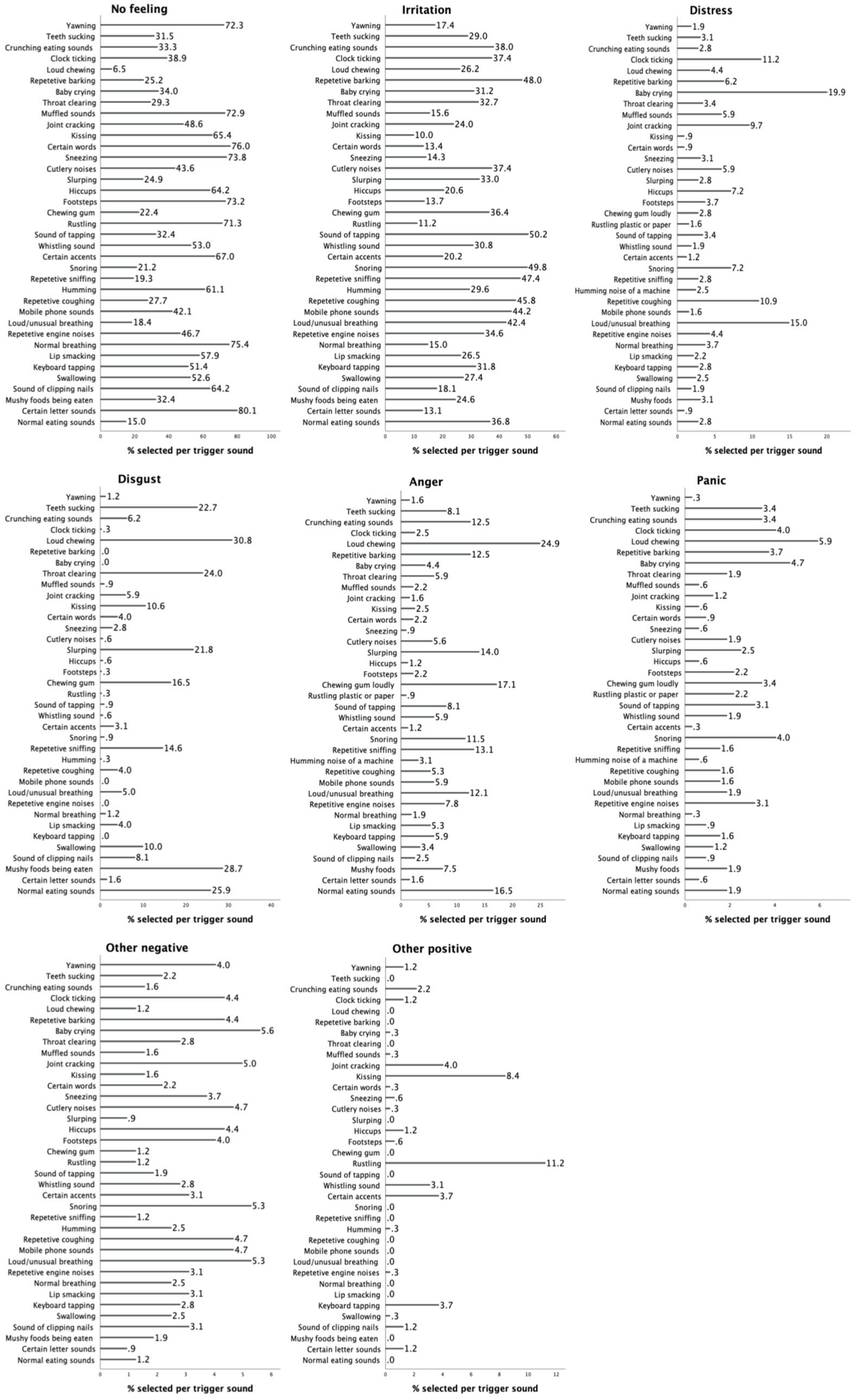
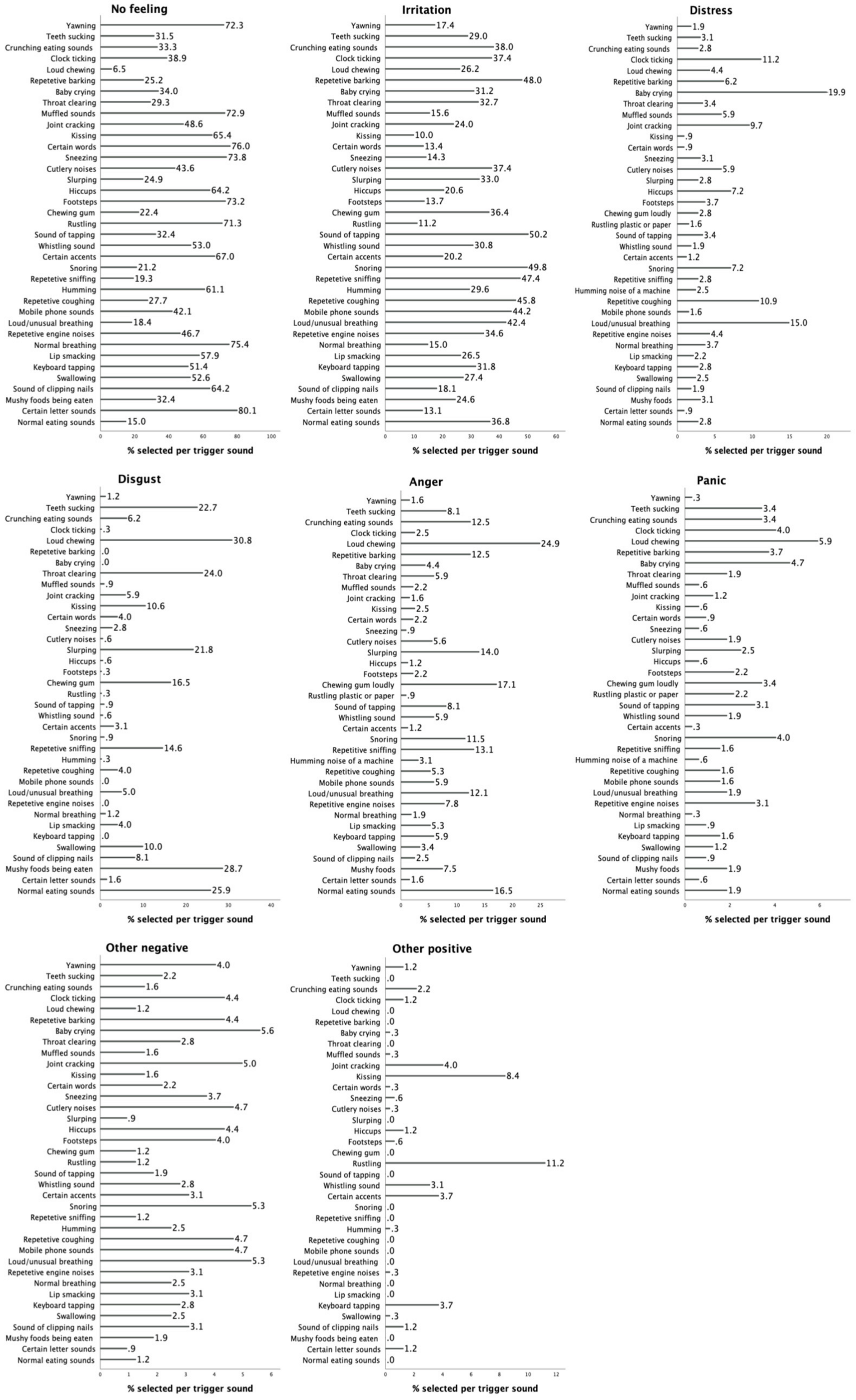
3.3.1. Reaction Counts
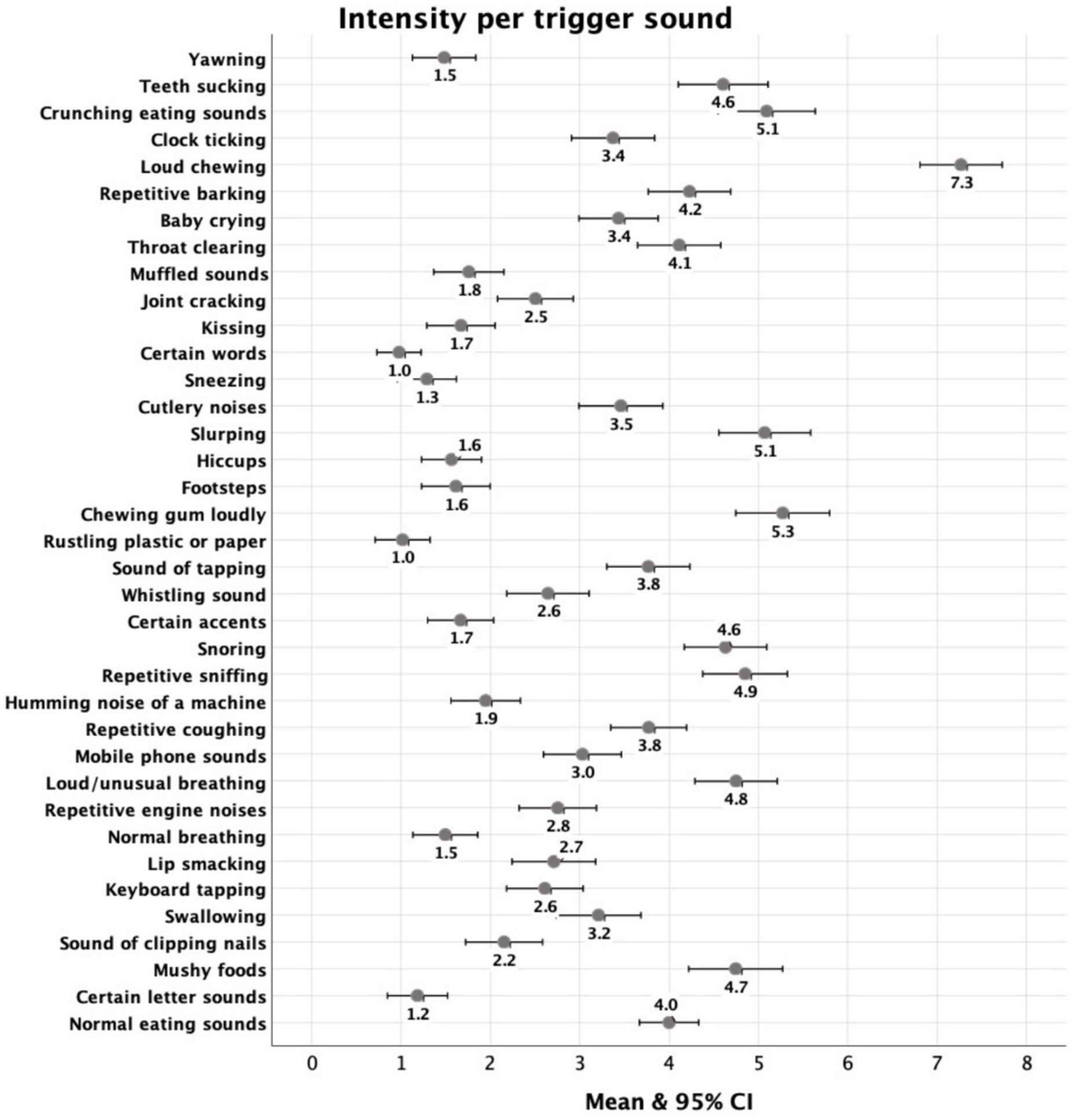
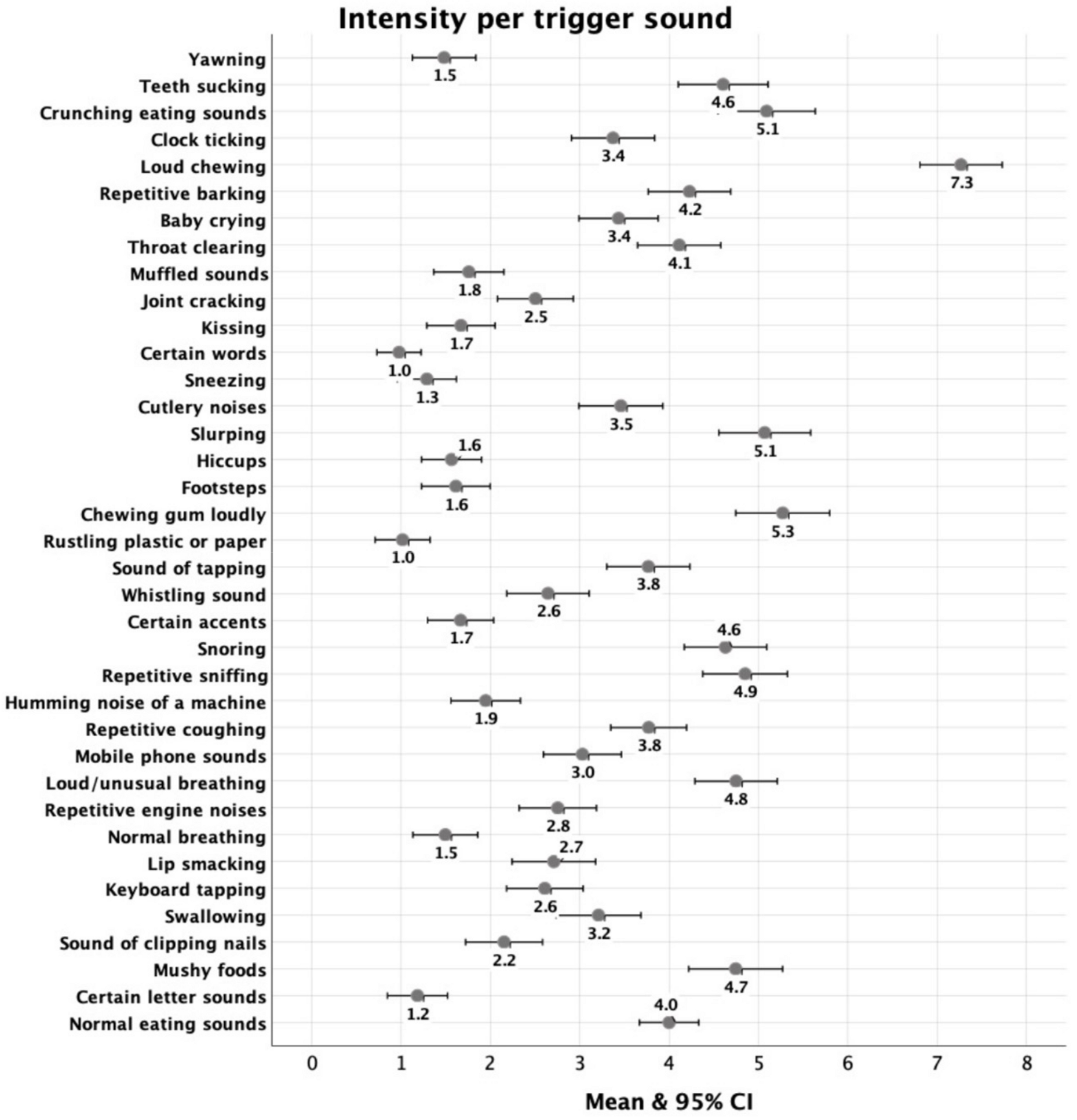
3.3.2. Intensity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- A.
- The S-Five scale
- B.
- The S-Five: Reactions (S-Five-R) *
- (i)
- Pensando nas últimas semanas, qual é a principal sensação que este som lhe causou? (por favor escolha a mais característica) Nenhum Sentimento, Irritação, Angustia, Repugnância, Raiva, Pânico, Outro Sentimento Negativo, Outro Sentimento Positivo
- (ii)
- Pensando nas ultimas semanas, por favor avalie a intensidade da sua reacção a este som quando feito por outra pessoua ou objecto (de 0: não me incomoda nada até 10: insuportavel/sofrimento)
- Emotional Reaction scores (ERS) para cada emoção: contar em todos os gatilhos as vezes que cada emoção foi selecionada no(s) item(ns) para criar um índice para cada emoção (por exemplo, ERS-Anger, assumindo valores entre 0 e 37). O índice fornece informações sobre reações emocionais específicas entre os participantes.
- Frequency/Intensity of Reactions Score (FIRS index): Adicione as respostas aos pontos (ii) em todos os gatilhos (intervalo de 0 a 370). O índice fornece informações combinadas sobre o número de sons de disparo e sua intensidade.
- Trigger Count (TC): Por favor, conte o número de respostas diferentes de zero para (ii). O índice assume valores entre 0 e 37 e fornece informações sobre o número de sons de disparo relatados por pessoa.
- Trigger Relative Intensity (TRE): Por favor, divida FIRS por TC para obter uma estimativa da intensidade das respostas de gatilho, em relação ao número de gatilhos relatados. O índice fornece informações sobre a intensidade da resposta aos gatilhos, independentemente de seu número.
References
- Ferrer-Torres, A.; Giménez-Llort, L. Misophonia: A Systematic Review of Current and Future Trends in This Emerging Clinical Field. Int. J. Environ. Res. Public Health 2022, 19, 6790. [Google Scholar] [CrossRef]
- Potgieter, I.; MacDonald, C.; Partridge, L.; Cima, R.; Sheldrake, J.; Hoare, D.J. Misophonia: A scoping review of research. J. Clin. Psychol. 2019, 75, 1203–1218. [Google Scholar] [CrossRef]
- Jastreboff, M.M.; Jastreboff, P.J. Components of decreased sound tolerance: Hyperacusis, misophonia, phonophobia. ITHS News Lett. 2001, 2, 5–7. [Google Scholar]
- Swedo, S.; Baguley, D.M.; Denys, D.; Dixon, L.J.; Erfanian, M.; Fioretti, A.; Jastreboff, P.J.; Kumar, S.; Rosenthal, Z.M.; Romke Rouw, R.; et al. A Consensus Definition of Misophonia: Using a Delphi Process to Reach Expert Agreement. medRxiv 2021. [Google Scholar] [CrossRef]
- Vitoratou, S.; Uglik-Marucha, N.; Hayes, C.; Erfanian, M.; Pearson, O.; Gregory, J. Item Response Theory Investigation of Misophonia Auditory Triggers. Audiology 2021, 11, 567–581. [Google Scholar] [CrossRef]
- Norris, J.E.; Kimball, S.H.; Nemri, D.C.; Ethridge, L.E. Toward a Multidimensional Understanding of Misophonia Using Cluster-Based Phenotyping. Front. Neurosci. 2022, 16, 832516. [Google Scholar] [CrossRef]
- Erfanian, M.; Kartsonaki, C.; Keshavarz, A. Misophonia and comorbid psychiatric symptoms: A preliminary study of clinical findings. Nord. J. Psychiatry 2019, 73, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Jager, I.; de Koning, P.; Bost, T.; Denys, D.; Vulink, N. Misophonia: Phenomenology, comorbidity and demographics in a large sample. PLoS ONE 2020, 15, e0231390. [Google Scholar] [CrossRef] [PubMed]
- Hansen, H.A.; Leber, A.B.; Saygin, Z.M. What sound sources trigger misophonia? Not just chewing and breathing. J. Clin. Psychol. 2021, 77, 2609–2625. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.S.; Lewin, A.B.; Murphy, T.K.; Storch, E.A. Misophonia: Incidence, Phenomenology, and Clinical Correlates in an Undergraduate Student Sample. J. Clin. Psychol. 2014, 70, 994–1007. [Google Scholar] [CrossRef] [PubMed]
- Larsen, E.-A.; Hovland, T.; Nielsen, G.E.; Larsen, L. Preliminary validation of the Norwegian version of misophonia questionnaire (MQ-NOR). Int. J. Audiol. 2022, 62, 1002–1007. [Google Scholar] [CrossRef]
- Vitoratou, S.; Hayes, C.; Uglik-Marucha, N.; Pearson, O.; Graham, T.; Gregory, J. Misophonia in the UK: Prevalence and norms from the S-Five in a UK representative sample. PLoS ONE 2023, 18, e0282777. [Google Scholar] [CrossRef]
- Kumar, S.; Tansley-Hancock, O.; Sedley, W.; Winston, J.S.; Callaghan, M.F.; Allen, M.; Cope, T.E.; Gander, P.E.; Bamiou, D.-E.; Griffiths, T.D. The Brain Basis for Misophonia. Curr. Biol. 2017, 27, 527–533. [Google Scholar] [CrossRef]
- Edelstein, M.; Brang, D.; Rouw, R.; Ramachandran, V.S. Misophonia: Physiological investigations and case descriptions. Front. Hum. Neurosci. 2013, 7, 296. [Google Scholar] [CrossRef]
- Swedo, S.E.; Baguley, D.M.; Denys, D.; Dixon, L.J.; Erfanian, M.; Fioretti, A.; Jastreboff, P.J.; Kumar, S.; Rosenthal, M.Z.; Rouw, R.; et al. Consensus Definition of Misophonia: A Delphi Study. Front. Neurosci. 2022, 16, 841816. [Google Scholar] [CrossRef]
- Siepsiak, M.; Vrana, S.R.; Rynkiewicz, A.; Rosenthal, M.Z.; Dragan, W. Does context matter in misophonia? A multi-method experimental investigation. Front. Neurosci. 2023, 16, 880853. [Google Scholar] [CrossRef]
- Schröder, A.; Vulink, N.; Denys, D. Misophonia: Diagnostic Criteria for a New Psychiatric Disorder. PLoS ONE 2013, 8, e54706. [Google Scholar] [CrossRef] [PubMed]
- Remmert, N.; Jebens, A.; Gruzman, R.; Gregory, J.; Vitoratou, S. A nomological network for misophonia in two German samples using the S-Five model for misophonia. Manuscript submitted in Advances in Understanding the Nature and Features of Misophonia. Front. Psychol. 2022, 13, 902807. [Google Scholar] [CrossRef] [PubMed]
- Rouw, R.; Erfanian, M. A Large-Scale Study of Misophonia. J. Clin. Psychol. 2018, 74, 453–479. [Google Scholar] [CrossRef] [PubMed]
- Vitoratou, S.; Uglik-Marucha, N.; Hayes, C.; Gregory, J. Listening to people with misophonia: Exploring the multiple dimensions of sound intolerance using a new psychometric tool, the S-Five, in a large sample of individuals identifying with the condition. Psych 2021, 3, 639–662. [Google Scholar] [CrossRef]
- Williams, Z.J.; Cascio, C.J.; Woynaroski, T.G. Psychometric validation of a brief self-report measure of misophonia symptoms and functional impairment: The duke-vanderbilt misophonia screening questionnaire. Front. Psychol. 2022, 13, 897901. [Google Scholar] [CrossRef] [PubMed]
- Vitoratou, S.; Wang, J.; Hayes, C.; Wang, Q.; Pentagiotissa, S.; Gregory, J. Evidence of cross-cultural consistency in a multidimensional model for the severity of misophonia and trigger burden: Psychometric conclusions emerging from the Mandarin version of the S-Five. Manuscript submitted in Advances in Understanding the Nature and Features of Misophonia. Front. Psychol. 2022, 13, 879881. [Google Scholar] [CrossRef]
- Cruz, M.; Assunção, S.; Simoes, J.A.; Santiago, L.; Cerejeira, J. Misophonia: The relation with depressive symptoms, coping mechanisms, and impact on daily life—observational study. In Proceedings of the 19th WPA World Congress of Psychiatry, Lisbon, Portugal, 21–24 August 2019. manuscript in preparation. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Monteiro, S.; Torres, A.; Pereira, A.; Albuquerque, E.; Morgadinho, R. Preliminary validation study of a Portuguese version of the patient health questionnaire (PHQ-9). Eur. Psychiatry 2013, 28, 1. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Gen. Psychiatry 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Sousa, T.V.; Viveiros, V.; Chai, M.V.; Vicente, F.L.; Jesus, G.; Carnot, M.J.; Gordo, A.C.; Ferreira, P.L. Reliability and validity of the Portuguese version of the Generalized Anxiety Disorder (GAD-7) scale. Health Qual. Life Outcomes 2015, 13, 50. [Google Scholar] [CrossRef]
- Taylor, S.; Zvolensky, M.J.; Cox, B.J.; Deacon, B.; Heimberg, R.G.; Ledley, D.R.; Abramowitz, J.S.; Holaway, R.M.; Sandin, B.; Stewart, S.H.; et al. Robust dimensions of anxiety sensitivity: Development and initial validation of the Anxiety Sensitivity Index-3. Psychol. Assess. 2007, 19, 176–188. [Google Scholar] [CrossRef]
- Ganho-Ávila, A.; Moura-Ramos, M.; Gonçalves Ó, F.; Almeida, J. Measuring vulnerability to anxiety: Factorial structure, reliability, validity, and discriminatory accuracy of the anxiety sensitivity index–3–PT. Meas. Eval. Couns. Dev. 2019, 52, 223–238. [Google Scholar] [CrossRef]
- Peterson, R.A.; Reiss, S. Anxiety Sensitivity Index Manual; International Diagnostic Systems: Worthington, OH, USA, 1992; Volume 2. [Google Scholar]
- Korkmaz, S.; Goksuluk, D.; Zararsiz, G. MVN: An R Package for Assessing Multivariate Normality. R J. 2014, 6, 151–162. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022. [Google Scholar]
- Mardia, K.V. Measures of multivariate skewness and kurtosis with applications. Biometrika 1970, 57, 519–530. [Google Scholar] [CrossRef]
- Henze, N.; Zirkler, B. A Class of Invariant Consistent Tests for Multivariate Normality. Commun. Stat. Theory Methods 1990, 19, 3595–3617. [Google Scholar] [CrossRef]
- Royston, P. Approximating the Shapiro-Wilk W test for non-normality. Stat. Comput. 1992, 2, 117–119. [Google Scholar] [CrossRef]
- Doornik, J.A.; Hansen, H. An Omnibus Test for Univariate and Multivariate Normality. Oxf. Bull. Econ. Stat. 2008, 70, 927–939. [Google Scholar] [CrossRef]
- Kyriazos, T.; Poga, M. Dealing with Multicollinearity in Factor Analysis: The Problem, Detections, and Solutions. Open J. Stat. 2023, 13, 404–424. [Google Scholar] [CrossRef]
- Vitoratou, S.; Uglik-Marucha, N.; Hayes, C.; Pickles, A. A Comprehensive Guide for Assessing Measurement Tool Quality: The Contemporary Psychometrics (ConPsy) Checklist. PsyArXiv 2023. in preparation. [Google Scholar] [CrossRef]
- Hoelter, J. The Analysis of Covariance Structures. Sociol. Methods Res. 1983, 11, 325–344. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M.R. Structural equation modelling: Guidelines for determining model fit. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Bentler, P.; Bonett, D. Significance tests and goodness of fit in the analysis of covariance structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Autom. Control. 1974, 19, 716–723. [Google Scholar] [CrossRef]
- Schwarz, G. Estimating the dimension of a model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Joreskog, K.; Goldberger, A. Estimation of a Model with Multiple Indicators and Multiple Causes of a Single Latent Variable. J. Am. Stat. Assoc. 1975, 70, 631–639. [Google Scholar]
- Muthén, B. A structural probit model with latent variables. J. Am. Stat. Assoc. 1979, 74, 807–811. [Google Scholar]
- Cronbach, L. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- McDonald, R.P. Test Theory: A Unified Treatment, 1st ed.; Psychology Press: New York, NY, USA, 1999. [Google Scholar]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 17; StataCorp LLC: College Station, TX, USA, 2021. [Google Scholar]
- Muthen, L.K.; Muthén, B. Mplus User’s Guide, 8th ed.; Muthén, B.O., Ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Spearman, C. The Proof and Measurement of Association between Two Things. Am. J. Psychol. 1904, 15, 72–101. [Google Scholar] [CrossRef]
- Quek, T.C.; Ho, C.S.; Choo, C.C.; Nguyen, L.H.; Tran, B.X.; Ho, R.C. Misophonia in Singaporean Psychiatric Patients: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1410. [Google Scholar] [CrossRef]
- Siepsiak, M.; Sliwerski, A.; Lukasz Dragan, W. Development and Psychometric Properties of MisoQuest-A New Self-Report Questionnaire for Misophonia. Int. J. Environ. Res. Public Health 2020, 17, 1797. [Google Scholar] [CrossRef]
- Zhou, X.; Wu, M.S.; Storch, E.A. Misophonia symptoms among Chinese university students: Incidence, associated impairment, and clinical correlates. J. Obsessive-Compulsive Relat. Disord. 2017, 14, 7–12. [Google Scholar] [CrossRef]
- Cusack, S.E.; Cash, T.V.; Vrana, S.R. An examination of the relationship between misophonia, anxiety sensitivity, and obsessive-compulsive symptoms. J. Obsessive-Compulsive Relat. Disord. 2018, 18, 67–72. [Google Scholar] [CrossRef]
- Dixon, L.J.; Witcraft, S.M.; Schadegg, M.J. COVID-19 anxiety and mental health among university students during the early phases of the U.S. pandemic. J. Am. Coll. Health 2021, 71, 1152–1160. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Vitoratou, S.; Uglik-Marucha, N.; Gregory, J. Emotion Processes Predicting Outbursts and Functional Impact in Misophonia. Front. Psychol. 2022, 13, 903142. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Statements | Factor Loading | ITC | AID |
|---|---|---|---|
| Externalising | |||
| I06 Others avoid making noises | 0.67 | 0.67 | 0.87 |
| I13 Others should not make sounds | 0.72 | 0.73 | 0.86 |
| I16 Others selfish | 0.81 | 0.71 | 0.86 |
| I21 Others’ bad manners | 0.74 | 0.70 | 0.86 |
| I25 Others disrespectful | 0.91 | 0.79 | 0.84 |
| Internalising | |||
| I05 Respect myself less | 0.68 | 0.64 | 0.91 |
| I08 Unlikeable person | 0.87 | 0.80 | 0.88 |
| I12 Angry person inside | 0.86 | 0.80 | 0.88 |
| I18 Bad person inside | 0.81 | 0.78 | 0.88 |
| I19 Dislike self | 0.83 | 0.79 | 0.88 |
| Impact | |||
| I01 Do not meet friends | 0.72 | 0.71 | 0.91 |
| I09 Eventually isolated | 0.93 | 0.84 | 0.88 |
| I14 Avoid places | 0.82 | 0.80 | 0.89 |
| I15 Cannot do everyday things | 0.87 | 0.80 | 0.89 |
| I20 Limited job opportunities | 0.74 | 0.74 | 0.90 |
| Outburst | |||
| I04 Verbally aggressive | 0.82 | 0.74 | 0.88 |
| I17 Physically aggressive | 0.80 | 0.78 | 0.87 |
| I22 Violence | 0.75 | 0.73 | 0.88 |
| I23 Shout at people | 0.80 | 0.75 | 0.88 |
| I24 Afraid of outburst | 0.81 | 0.74 | 0.88 |
| Threat | |||
| I02 Panic or explode | 0.89 | 0.87 | 0.94 |
| I03 Feel helpless | 0.87 | 0.84 | 0.94 |
| I07 Feel anxious | 0.90 | 0.88 | 0.94 |
| I10 Experience distress | 0.89 | 0.86 | 0.94 |
| I11 Feel trapped | 0.91 | 0.89 | 0.94 |
| Factor | Median (Q1, Q3) | Alpha | Correlation with Age (rho) | Gender Difference (Z) |
|---|---|---|---|---|
| Externalising | 26 (14, 39) | 0.88 | 0.06 | −0.91 |
| Internalising | 14 (1, 29) | 0.91 | −0.07 | 0.70 |
| Impact | 6 (0, 19) | 0.91 | 0.06 | 0.79 |
| Outburst | 11 (3, 24) | 0.90 | 0.02 | 0.97 |
| Threat | 26 (6, 41) | 0.95 | −0.08 | 2.13 * |
| Total | 91 (33, 140) | 0.96 | −0.01 | 0.80 |
| Externalising | Internalising | Impact | Threat | Outburst | Total Score | |
|---|---|---|---|---|---|---|
| S-Five (N = 491) | ||||||
| Externalising | - | |||||
| Internalising | 0.59 ** | - | ||||
| Impact | 0.59 ** | 0.75 ** | - | |||
| Threat | 0.64 ** | 0.80 ** | 0.81 ** | - | ||
| Outburst | 0.60 ** | 0.76 ** | 0.72 ** | 0.75 ** | - | |
| Total score | 0.79 ** | 0.89 ** | 0.87 ** | 0.92 ** | 0.87 ** | - |
| Misophonia Questionnaire (N = 185) | ||||||
| MSYS | 0.46 ** | 0.61 ** | 0.61 ** | 0.62 ** | 0.66 ** | 0.68 ** |
| MEBS | 0.60 ** | 0.74 ** | 0.75 ** | 0.84 ** | 0.79 ** | 0.86 ** |
| MSES | 0.53 ** | 0.66 ** | 0.66 ** | 0.73 ** | 0.68 ** | 0.74 ** |
| Total score | 0.58 ** | 0.73 ** | 0.74 ** | 0.80 ** | 0.79 ** | 0.84 ** |
| A-MISO-S (N = 214) | ||||||
| Total score | 0.56 ** | 0.73 ** | 0.72 ** | 0.79 ** | 0.65** | 0.81 ** |
| PHQ-9 (N = 440) | ||||||
| Total Score | 0.32 ** | 0.48 ** | 0.50 ** | 0.47 ** | 0.42 ** | 0.50 ** |
| GAD-7 (N = 442) | ||||||
| Total Score | 0.35 ** | 0.50 ** | 0.49 ** | 0.49 ** | 0.46 ** | 0.52 ** |
| ASI-3 (N = 216) | ||||||
| Total score | 0.23 ** | 0.31 ** | 0.31 ** | 0.35 ** | 0.30 ** | 0.35 ** |
| Physical Concerns | 0.17 * | 0.24 ** | 0.29 ** | 0.36 ** | 0.25 ** | 0.30 ** |
| Cognitive Concerns | 0.25 ** | 0.31 ** | 0.35 ** | 0.34 ** | 0.34 ** | 0.37 ** |
| Social Concerns | 0.17 * | 0.26 ** | 0.23 ** | 0.24 ** | 0.23 ** | 0.27 ** |
| N | Mean (SD) | Median (Q1–Q3) | Min–Max | |
|---|---|---|---|---|
| RC | ||||
| No feeling | 321 | 17.3 (7.4) | 17 (12–23) | 0–36 |
| Irritation | 321 | 10.8 (5.0) | 10 (7–14) | 0–27 |
| Distress | 321 | 1.7 (2.1) | 1 (0–2) | 0–12 |
| Disgust | 321 | 2.6 (2.6) | 2 (0–4) | 0–11 |
| Anger | 321 | 2.4 (3.4) | 1 (0–4) | 0–17 |
| Panic | 321 | 0.7 (1.7) | 0 (0–1) | 0–13 |
| TC | 200 | 20.8 (7.3) | 22 (15–26) | 4–37 |
| FIRS | 200 | 126 (70.0) | 128 (72.5–172.5) | 10–343 |
| SIRS | 200 | 5.7 (1.9) | 6.2 (4.4–7.1) | 1.2–9.3 |
| No Feeling | Irritation | Distress | Disgust | Anger | Panic | TC | FIRS | RIRS | |
|---|---|---|---|---|---|---|---|---|---|
| S-Five-T | |||||||||
| No feeling | - | ||||||||
| Irritation | −0.53 ** | - | |||||||
| Distress | −0.32 ** | −0.10 | - | ||||||
| Disgust | −0.30 ** | −0.13 * | 0.17 * | - | |||||
| Anger | −0.54 ** | 0.05 | 0.14 * | 0.03 | - | ||||
| Panic | −0.34 ** | −0.12 * | 0.19 ** | 0.10 | 0.35 ** | - | |||
| TC | −0.99 ** | 0.49 ** | 0.30 ** | 0.24 ** | 0.57 ** | 0.36 ** | - | ||
| FIRS | −0.85 ** | 0.35 ** | 0.23 ** | 0.18 * | 0.66 ** | 0.40 ** | 0.88 ** | - | |
| RIRS | −0.46 ** | 0.12 | 0.10 | 0.03 | 0.54 ** | 0.31 ** | 0.50 ** | 0.82 ** | - |
| S-Five | |||||||||
| Externalising | −0.47 ** | 0.11 | 0.11 | 0.25 ** | 0.49 ** | 0.24 ** | 0.43 ** | 0.57 ** | 0.55 ** |
| Internalising | −0.58 ** | 0.18 ** | 0.17 * | 0.12 * | 0.56 ** | 0.36 ** | 0.50 ** | 0.65 ** | 0.66 ** |
| Impact | −0.58 ** | 0.17 * | 0.23 ** | 0.12 * | 0.52 ** | 0.43 ** | 0.56 ** | 0.69 ** | 0.65 ** |
| Outburst | −0.54 ** | 0.23 ** | 0.16 * | 0.12 * | 0.57 ** | 0.32 ** | 0.47 ** | 0.64 ** | 0.66 ** |
| Threat | −0.56 ** | 0.16 * | 0.24 ** | 0.11 * | 0.59 ** | 0.43 ** | 0.56 ** | 0.71 ** | 0.70 ** |
| Total | −0.62 ** | 0.19 ** | 0.22 ** | 0.16 * | 0.65 ** | 0.42 ** | 0.60 ** | 0.78 ** | 0.77 ** |
| Age | −0.19 ** | 0.18 ** | 0.07 | 0.05 | −0.01 | −0.10 | 0.13 | 0.06 | −0.03 |
| Misophonia Questionnaire | |||||||||
| MSYS | −0.84 ** | 0.49 ** | 0.24 * | 0.16 | 0.55 ** | 0.23 * | 0.87 ** | 0.87 ** | 0.60 ** |
| MEBS | −0.55 ** | 0.24 * | 0.11 | 0.07 | 0.61 ** | 0.32 ** | 0.54 ** | 0.65 ** | 0.61 ** |
| MSES | −0.47 ** | 0.25 * | 0.22 * | 0.12 | 0.50 ** | 0.18 * | 0.43 ** | 0.50 ** | 0.50 ** |
| Total score | −0.75 ** | 0.39 ** | 0.20 * | 0.12 | 0.64 ** | 0.30 * | 0.78 ** | 0.84 ** | 0.68 ** |
| A-MISO-S Total | −0.61 ** | 0.22 * | 0.14 | 0.18 * | 0.56 ** | 0.39 ** | 0.59 ** | 0.72 ** | 0.65 ** |
| PHQ-9 Total | −0.44 ** | 0.17 * | 0.25 ** | 0.13 * | 0.24 ** | 0.29 ** | 0.46 ** | 0.41 ** | 0.22 * |
| GAD-7 Total | −0.45 ** | 0.14 * | 0.22 ** | 0.15 * | 0.28 ** | 0.33 ** | 0.50 ** | 0.49 ** | 0.32 ** |
| ASI-3 | |||||||||
| Total score | −0.27 ** | 0.02 | 0.16 * | 0.21 * | 0.21 * | 0.23 * | 0.28 * | 0.34 ** | 0.26 * |
| Physical Concerns | −0.16 * | 0.01 | 0.10 | 0.12 | 0.17 * | 0.17 * | 0.18 | 0.29 * | 0.28 * |
| Cognitive Concerns | −0.35 ** | 0.06 | 0.16 * | 0.19 * | 0.28 ** | 0.26 ** | 0.33 ** | 0.35 ** | 0.25 * |
| Social Concerns | −0.19 * | 0.01 | 0.15 | 0.20 * | 0.10 | 0.19 * | 0.23 * | 0.26 * | 0.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hayes, C.; Gregory, J.; Aziz, R.; Cerejeira, J.; Cruz, M.; Simões, J.A.; Vitoratou, S. Psychometric Evaluation and Misophonic Experience in a Portuguese-Speaking Sample. Behav. Sci. 2024, 14, 107. https://doi.org/10.3390/bs14020107
Hayes C, Gregory J, Aziz R, Cerejeira J, Cruz M, Simões JA, Vitoratou S. Psychometric Evaluation and Misophonic Experience in a Portuguese-Speaking Sample. Behavioral Sciences. 2024; 14(2):107. https://doi.org/10.3390/bs14020107
Chicago/Turabian StyleHayes, Chloe, Jane Gregory, Rahima Aziz, Joaquim Cerejeira, Marina Cruz, José Augusto Simões, and Silia Vitoratou. 2024. "Psychometric Evaluation and Misophonic Experience in a Portuguese-Speaking Sample" Behavioral Sciences 14, no. 2: 107. https://doi.org/10.3390/bs14020107
APA StyleHayes, C., Gregory, J., Aziz, R., Cerejeira, J., Cruz, M., Simões, J. A., & Vitoratou, S. (2024). Psychometric Evaluation and Misophonic Experience in a Portuguese-Speaking Sample. Behavioral Sciences, 14(2), 107. https://doi.org/10.3390/bs14020107