
The Impact of Different Types of Exercise on Executive Functions in Overweight/Obese Individuals: A Systematic Review and Network Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Registration
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection and Data Extraction
2.5. Quality Assessment
2.6. Data Synthesis and Statistical Analyses
3. Results
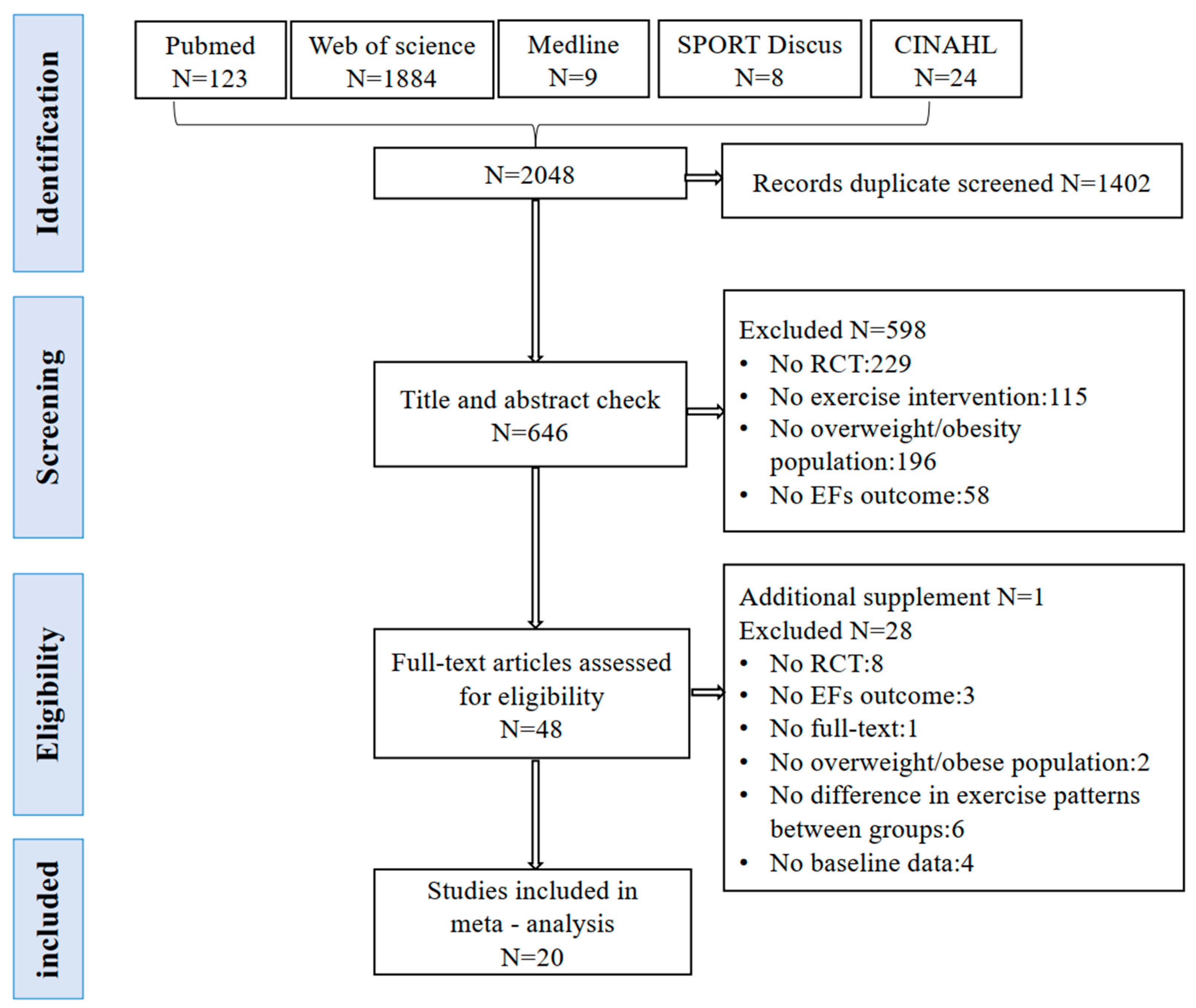
3.1. Study Selection
3.2. Study Characteristics
3.3. Network Meta-Analysis
3.3.1. Cognitive Function (CF)
3.3.2. Inhibitory Control
3.3.3. Academic Performance (AP)
3.3.4. Subgroup Analysis
4. Discussion
4.1. Exercise Effect on EFs
4.2. Age and Intervention Duration
4.3. Limitations and Implications for Future Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Klein, S.; Wadden, T.; Sugerman, H.J. AGA Technical Review on Obesity. Gastroenterology 2002, 123, 882–932. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253. [Google Scholar]
- Wood Alexander, M.; Wu, C.-Y.; Coughlan, G.T.; Puri, T.; Buckley, R.F.; Palta, P.; Swardfager, W.; Masellis, M.; Galea, L.A.M.; Einstein, G.; et al. Associations Between Age at Menopause, Vascular Risk, and 3-Year Cognitive Change in the Canadian Longitudinal Study on Aging. Neurology 2024, 102, e209298. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Chen, H.; Chang, Z.; Zhang, J.; Xie, D. Genetic Causal Role of Body Mass Index in Multiple Neurological Diseases. Sci. Rep. 2024, 14, 7256. [Google Scholar] [CrossRef] [PubMed]
- Muntaner-Mas, A.; Palou, P.; Vidal-Conti, J.; Esteban-Cornejo, I. A Mediation Analysis on the Relationship of Physical Fitness Components, Obesity, and Academic Performance in Children. J. Pediatr. 2018, 198, 90–97.e4. [Google Scholar] [CrossRef] [PubMed]
- Stuss, D.T. Cognitive Impairment. In Encyclopedia of the Neurological Sciences; Aminoff, M.J., Daroff, R.B., Eds.; Academic Press: New York, NY, USA, 2003; pp. 737–740. ISBN 978-0-12-226870-0. [Google Scholar]
- Dong, D.; Chen, X.; Li, W.; Gao, X.; Wang, Y.; Zhou, F.; Eickhoff, S.B.; Chen, H. Opposite Changes in Morphometric Similarity of Medial Reward and Lateral Non-Reward Orbitofrontal Cortex Circuits in Obesity. Neuroimage 2024, 290, 120574. [Google Scholar] [CrossRef] [PubMed]
- Benito-León, J.; Mitchell, A.J.; Hernández-Gallego, J.; Bermejo-Pareja, F. Obesity and Impaired Cognitive Functioning in the Elderly: A Population-Based Cross-Sectional Study (NEDICES). Eur. J. Neurol. 2013, 20, 899–906, e76–e77. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ji, W.; Jiang, F.; Wu, F.; Li, G.; Hu, Y.; Zhang, W.; Wang, J.; Fan, X.; Wei, X.; et al. Associations among Body Mass Index, Working Memory Performance, Gray Matter Volume, and Brain Activation in Healthy Children. Cereb. Cortex 2023, 33, 6335–6344. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Mora-Gonzalez, J.; Cadenas-Sanchez, C.; Esteban-Cornejo, I.; Migueles, J.H.; Solis-Urra, P.; Verdejo-Roman, J.; Rodriguez-Ayllon, M.; Molina-Garcia, P.; Ruiz, J.R.; et al. Effects of an Exercise Program on Brain Health Outcomes for Children With Overweight or Obesity The ActiveBrains Randomized Clinical Trial. Jama Netw. Open 2022, 5. [Google Scholar] [CrossRef]
- García-García, I.; Jurado, M.Á.; Garolera, M.; Marqués-Iturria, I.; Horstmann, A.; Segura, B.; Pueyo, R.; Sender-Palacios, M.J.; Vernet-Vernet, M.; Villringer, A.; et al. Functional Network Centrality in Obesity: A Resting-State and Task fMRI Study. Psychiatry Res. 2015, 233, 331–338. [Google Scholar] [CrossRef]
- Yang, Y.; Shields, G.S.; Guo, C.; Liu, Y. Executive Function Performance in Obesity and Overweight Individuals: A Meta-Analysis and Review. Neurosci. Biobehav. Rev. 2018, 84, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, F.; Perea, M.V.; Ladera, V.; Rosa, B.; García, R. Executive Functioning in Obese Individuals Waiting for Clinical Treatment. Psicothema 2017, 29, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.F.; Eichen, D.M.; Barch, D.M.; Wilfley, D.E. Executive Function in Childhood Obesity: Promising Intervention Strategies to Optimize Treatment Outcomes. Appetite 2018, 124, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children: A Systematic Review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [PubMed]
- Mora-Gonzalez, J.; Esteban-Cornejo, I.; Solis-Urra, P.; Rodriguez-Ayllon, M.; Cadenas-Sanchez, C.; Hillman, C.H.; Kramer, A.F.; Catena, A.; Ortega, F.B. The Effects of an Exercise Intervention on Neuroelectric Activity and Executive Function in Children with Overweight/Obesity: The ActiveBrains Randomized Controlled Trial. Scand. J. Med. Sci. Sports 2023, 34, e14486. [Google Scholar] [CrossRef]
- Oliveira, G.T.A.; Elsangedy, H.M.; Pereira, D.C.; de Melo Silva, R.; Faro, H.K.C.; Bortolotti, H.; Costa, E.C.; Fontes, E.B. Effects of 12 Weeks of High-Intensity Interval, Moderate-Intensity Continuous and Self-Selected Intensity Exercise Training Protocols on Cognitive Inhibitory Control in Overweight/Obese Adults: A Randomized Trial. Eur. J. Sport Sci. 2022, 22, 1724–1733. [Google Scholar] [CrossRef]
- Diamond, A. Executive Functions. Ann. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P.; Emerson, M.J.; Witzki, A.H.; Howerter, A.; Wager, T.D. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef]
- Xue, Y.; Yang, Y.; Huang, T. Effects of Chronic Exercise Interventions on Executive Function among Children and Adolescents: A Systematic Review with Meta-Analysis. Br. J. Sports Med. 2019, 53, 1397–1404. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.; Gilbert, S.; Serpell, L. Systematic Review: Are Overweight and Obese Individuals Impaired on Behavioural Tasks of Executive Functioning? Neuropsychol Rev. 2013, 23, 138–156. [Google Scholar] [CrossRef] [PubMed]
- Best, J.R.; Miller, P.H.; Naglieri, J.A. Relations between Executive Function and Academic Achievement from Ages 5 to 17 in a Large, Representative National Sample. Learn Individ. Differ. 2011, 21, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.A.; Feldman, J.F.; Jankowski, J.J. Modeling a Cascade of Effects: The Role of Speed and Executive Functioning in Preterm/Full-Term Differences in Academic Achievement. Dev. Sci. 2011, 14, 1161–1175. [Google Scholar] [CrossRef] [PubMed]
- Domal, S.V.; Chandrasekaran, B.; Palanisamy, H.P. Influence of Smartphone-Based Physical Activity Intervention on Executive Functions and Cardiometabolic Disease Risk in Obese Young Adults: A Pilot Randomised Controlled Trial. J. Diabetes Metab. Disord. 2023, 22, 619–628. [Google Scholar] [CrossRef]
- Zhang, L.; Chu, C.-H.; Liu, J.-H.; Chen, F.-T.; Nien, J.-T.; Zhou, C.; Chang, Y.-K. Acute Coordinative Exercise Ameliorates General and Food-Cue Related Cognitive Function in Obese Adolescents. J. Sports Sci. 2020, 38, 953–960. [Google Scholar] [CrossRef]
- Furlano, J.A.; Horst, B.R.; Petrella, R.J.; Shoemaker, J.K.; Nagamatsu, L.S. Changes in Cognition and Brain Function After 26 Weeks of Progressive Resistance Training in Older Adults at Risk for Diabetes: A Pilot Randomized Controlled Trial. Can. J. Diabetes 2023, 47, 250–256. [Google Scholar] [CrossRef] [PubMed]
- van Agtmaal, M.J.M.; Houben, A.J.H.M.; de Wit, V.; Henry, R.M.A.; Schaper, N.C.; Dagnelie, P.C.; van der Kallen, C.J.; Koster, A.; Sep, S.J.; Kroon, A.A.; et al. Prediabetes Is Associated With Structural Brain Abnormalities: The Maastricht Study. Diabetes Care 2018, 41, 2535–2543. [Google Scholar] [CrossRef]
- Baker, L.D.; Frank, L.L.; Foster-Schubert, K.; Green, P.S.; Wilkinson, C.W.; McTiernan, A.; Cholerton, B.A.; Plymate, S.R.; Fishel, M.A.; Watson, G.S.; et al. Aerobic Exercise Improves Cognition for Older Adults with Glucose Intolerance, a Risk Factor for Alzheimer’s Disease. J. Alzheimer’s Dis. 2010, 22, 569–579. [Google Scholar] [CrossRef]
- Ibañez, J.; Izquierdo, M.; Argüelles, I.; Forga, L.; Larrión, J.L.; García-Unciti, M.; Idoate, F.; Gorostiaga, E.M. Twice-Weekly Progressive Resistance Training Decreases Abdominal Fat and Improves Insulin Sensitivity in Older Men with Type 2 Diabetes. Diabetes Care 2005, 28, 662–667. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, P.; Boraxbekk, C.-J.; Wheeler, M.; Howard, B.; Dempsey, P.C.; Lambert, G.; Eikelis, N.; Larsen, R.; Sethi, P.; Occleston, J.; et al. Acute Effects of Breaking up Prolonged Sitting on Fatigue and Cognition: A Pilot Study. BMJ OPEN 2016, 6, 9630. [Google Scholar] [CrossRef] [PubMed]
- Lee, A. The Development of Network Meta-Analysis. J. R. Soc. Med. 2022, 115, 313–321. [Google Scholar] [CrossRef]
- Efthimiou, O.; Debray, T.P.A.; van Valkenhoef, G.; Trelle, S.; Panayidou, K.; Moons, K.G.M.; Reitsma, J.B.; Shang, A.; Salanti, G. GetReal in Network Meta-Analysis: A Review of the Methodology. Res. Synth. Methods 2016, 7, 236–263. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-C.; Kao, S.-C.; Pan, C.-C.; McCullick, B.; Fu, H.-L.; Wang, C.-H. Cognitively Engaging Movement Games Improve Interference Control and Academic Performance in Overweight Children: A Randomized Control Trial. Scand. J. Med. Sci. Sports 2023, 33, 521–534. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, D.; Liu, S.; Ren, F.-F.; Chi, L.; Xie, C. Effects of Acute High-Intensity Interval Exercise and High-Intensity Continuous Exercise on Inhibitory Function of Overweight and Obese Children. Int. J. Environ. Res. Public Health 2022, 19, 10401. [Google Scholar] [CrossRef] [PubMed]
- Zlibinaite, L.; Skurvydas, A.; Kilikeviciene, S.; Solianik, R. Two Months of Using Global Recommendations for Physical Activity Had No Impact on Cognitive or Motor Functions in Overweight and Obese Middle-Aged Women. J. Phys. Act. Health 2021, 18, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Žlibinaitė, L.; Solianik, R.; Vizbaraitė, D.; Mickevičienė, D.; Skurvydas, A. The Effect of Combined Aerobic Exercise and Calorie Restriction on Mood, Cognition, and Motor Behavior in Overweight and Obese Women. J. Phys. Act. Health 2020, 17, 204–210. [Google Scholar] [CrossRef]
- Inoue, D.S.; Monteiro, P.A.; Gerosa-Neto, J.; Santana, P.R.; Peres, F.P.; Edwards, K.M.; Lira, F.S. Acute Increases in Brain-Derived Neurotrophic Factor Following High or Moderate-Intensity Exercise Is Accompanied with Better Cognition Performance in Obese Adults. Sci. Rep. 2020, 10, 13493. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-R.; Tseng, C.-L.; Kuo, S.-Y.; Chang, Y.-K. Effects of a Physical Activity Intervention on Autonomic and Executive Functions in Obese Young Adolescents: A Randomized Controlled Trial. Health Psychol. 2016, 35, 1120–1125. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.J.; Blumenthal, J.A.; Babyak, M.A.; Craighead, L.; Welsh-Bohmer, K.A.; Browndyke, J.N.; Strauman, T.A.; Sherwood, A. Effects of the Dietary Approaches to Stop Hypertension Diet, Exercise, and Caloric Restriction on Neurocognition in Overweight Adults With High Blood Pressure. Hypertension 2010, 55, 1331-U85. [Google Scholar] [CrossRef]
- Dao, E.; Davis, J.C.; Sharma, D.; Chan, A.; Nagamatsu, L.S.; Liu-Ambrose, T. Change in Body Fat Mass Is Independently Associated with Executive Functions in Older Women: A Secondary Analysis of a 12-Month Randomized Controlled Trial. PLoS ONE 2013, 8, e52831. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.-T.; Chen, S.-R.; Chu, I.-H.; Liu, J.-H.; Chang, Y.-K. Multicomponent Exercise Intervention and Metacognition in Obese Preadolescents: A Randomized Controlled Study. J. Sport Exerc. Psychol. 2017, 39, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.L.; Tomporowski, P.D.; McDowell, J.E.; Austin, B.P.; Miller, P.H.; Yanasak, N.E.; Allison, J.D.; Naglieri, J.A. Exercise Improves Executive Function and Achievement and Alters Brain Activation in Overweight Children: A Randomized, Controlled Trial. Health Psychol. 2011, 30, 91–98. [Google Scholar] [CrossRef]
- Chou, C.-C.; Chen, K.-C.; Huang, M.-Y.; Tu, H.-Y.; Huang, C.-J. Can Movement Games Enhance Executive Function in Overweight Children? A Randomized Controlled Trial. J. Teach. Phys. Educ. 2020, 39, 527–535. [Google Scholar] [CrossRef]
- Allom, V.; Mullan, B.; Smith, E.; Hay, P.; Raman, J. Breaking Bad Habits by Improving Executive Function in Individuals with Obesity. BMC Public Health 2018, 18, 505. [Google Scholar] [CrossRef]
- Plaza-Florido, A.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Torres-Lopez, L.V.; Osuna-Prieto, F.J.; Gil-Cosano, J.J.; Radom-Aizik, S.; Labayen, I.; Ruiz, J.R.; Altmae, S.; et al. Gene-Exercise Interaction on Brain Health in Children with Overweight/Obesity: The ActiveBrains Randomized Controlled Trial. J. Appl. Physiol. 2023, 135, 775–785. [Google Scholar] [CrossRef] [PubMed]
- Quintero, A.P.; Johana Bonilla-Vargas, K.; Correa-Bautista, J.E.; Dominguez-Sanchez, M.A.; Triana-Reina, H.R.; Velasco-Orjuela, G.P.; Garcia-Hermoso, A.; Villa-Gonzalez, E.; Esteban-Cornejo, I.; Correa-Rodriguez, M.; et al. Acute Effect of Three Different Exercise Training Modalities on Executive Function in Overweight Inactive Men: A Secondary Analysis of the BrainFit Study. Physiol. Behav. 2018, 197, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Li, Y.; Cai, L.; Wang, Y. Effects of Physical Activity Interventions on Cognitive Performance of Overweight or Obese Children and Adolescents: A Systematic Review and Meta-Analysis. Pediatr. Res. 2021, 89, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.-T.; Etnier, J.L.; Chan, K.-H.; Chiu, P.-K.; Hung, T.-M.; Chang, Y.-K. Effects of Exercise Training Interventions on Executive Function in Older Adults: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 1451–1467. [Google Scholar] [CrossRef] [PubMed]
- Xue, D.; Li, P.W.C.; Yu, D.S.F.; Lin, R.S.Y. Combined Exercise and Cognitive Interventions for Adults with Mild Cognitive Impairment and Dementia: A Systematic Review and Network Meta-Analysis. Int. J. Nurs. Stud. 2023, 147, 104592. [Google Scholar] [CrossRef]
- Chang, Y.-K.; Hung, C.-L.; Huang, C.-J.; Hatfield, B.D.; Hung, T.-M. Effects of an Aquatic Exercise Program on Inhibitory Control in Children with ADHD: A Preliminary Study. Arch. Clin. Neuropsychol. 2014, 29, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-H.; Alderman, B.L.; Song, T.-F.; Chen, F.-T.; Hung, T.-M.; Chang, Y.-K. A Randomized Controlled Trial of Coordination Exercise on Cognitive Function in Obese Adolescents. Psychol. Sport Exerc. 2018, 34, 29–38. [Google Scholar] [CrossRef]
- Budde, H.; Voelcker-Rehage, C.; Pietrabyk-Kendziorra, S.; Ribeiro, P.; Tidow, G. Acute Coordinative Exercise Improves Attentional Performance in Adolescents. Neurosci. Lett. 2008, 441, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Best, J.R. Effects of Physical Activity on Children’s Executive Function: Contributions of Experimental Research on Aerobic Exercise. Developmental Review 2010, 30, 331–351. [Google Scholar] [CrossRef] [PubMed]
- Niemann, C.; Godde, B.; Voelcker-Rehage, C. Not Only Cardiovascular, but Also Coordinative Exercise Increases Hippocampal Volume in Older Adults. Front. Aging Neurosci. 2014, 6, 170. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, B.; Pesola, A.J.; Rao, C.R.; Arumugam, A. Does Breaking up Prolonged Sitting Improve Cognitive Functions in Sedentary Adults? A Mapping Review and Hypothesis Formulation on the Potential Physiological Mechanisms. BMC Musculoskelet. Disord. 2021, 22, 274. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Kingwell, B.A.; Owen, N.; Dunstan, D.W. Breaking up Workplace Sitting Time with Intermittent Standing Bouts Improves Fatigue and Musculoskeletal Discomfort in Overweight/Obese Office Workers. Occup. Environ. Med. 2014, 71, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Van Cauwenbergh, D.; Nijs, J.; Kos, D.; Van Weijnen, L.; Struyf, F.; Meeus, M. Malfunctioning of the Autonomic Nervous System in Patients with Chronic Fatigue Syndrome: A Systematic Literature Review. Eur. J. Clin. Investig. 2014, 44, 516–526. [Google Scholar] [CrossRef]
- Meeus, M.; Goubert, D.; De Backer, F.; Struyf, F.; Hermans, L.; Coppieters, I.; De Wandele, I.; Da Silva, H.; Calders, P. Heart Rate Variability in Patients with Fibromyalgia and Patients with Chronic Fatigue Syndrome: A Systematic Review. Semin. Arthritis Rheum. 2013, 43, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, G.; Maillard, P.; Himali, J.J.; Beiser, A.S.; Au, R.; Wolf, P.A.; Seshadri, S.; DeCarli, C. Glucose Indices Are Associated with Cognitive and Structural Brain Measures in Young Adults. Neurology 2015, 84, 2329–2337. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, M.J.; Green, D.J.; Ellis, K.A.; Cerin, E.; Heinonen, I.; Naylor, L.H.; Larsen, R.; Wennberg, P.; Boraxbekk, C.-J.; Lewis, J.; et al. Distinct Effects of Acute Exercise and Breaks in Sitting on Working Memory and Executive Function in Older Adults: A Three-Arm, Randomised Cross-over Trial to Evaluate the Effects of Exercise with and without Breaks in Sitting on Cognition. Br. J. Sports Med. 2020, 54, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Pindus, D.M.; Edwards, C.G.; Walk, A.M.; Reeser, G.; Burd, N.A.; Holscher, H.D.; Khan, N.A. The Relationships between Prolonged Sedentary Time, Physical Activity, Cognitive Control, and P3 in Adults with Overweight and Obesity. Int. J. Obes. 2021, 45, 746–757. [Google Scholar] [CrossRef]
- Vints, W.A.J.; Gökçe, E.; Šeikinaitė, J.; Kušleikienė, S.; Česnaitienė, V.J.; Verbunt, J.; Levin, O.; Masiulis, N. Resistance Training’s Impact on Blood Biomarkers and Cognitive Function in Older Adults with Low and High Risk of Mild Cognitive Impairment: A Randomized Controlled Trial. Eur. Rev. Aging Phys. Act. 2024, 21, 9. [Google Scholar] [CrossRef] [PubMed]
- Febbraio, M.A.; Steensberg, A.; Keller, C.; Starkie, R.L.; Nielsen, H.B.; Krustrup, P.; Ott, P.; Secher, N.H.; Pedersen, B.K. Glucose Ingestion Attenuates Interleukin-6 Release from Contracting Skeletal Muscle in Humans. J. Physiol. 2003, 549, 607–612. [Google Scholar] [CrossRef]
- Febbraio, M.A.; Hiscock, N.; Sacchetti, M.; Fischer, C.P.; Pedersen, B.K. Interleukin-6 Is a Novel Factor Mediating Glucose Homeostasis during Skeletal Muscle Contraction. Diabetes 2004, 53, 1643–1648. [Google Scholar] [CrossRef] [PubMed]
- Lumeng, C.N.; Saltiel, A.R. Inflammatory Links between Obesity and Metabolic Disease. J. Clin. Investig. 2011, 121, 2111–2117. [Google Scholar] [CrossRef] [PubMed]
- Koutentaki, E.; Basta, M.; Antypa, D.; Zaganas, I.; Panagiotakis, S.; Simos, P.; Vgontzas, A.N. IL-6 Enhances the Negative Impact of Cortisol on Cognition among Community-Dwelling Older People without Dementia. Healthcare 2023, 11, 951. [Google Scholar] [CrossRef]
- McAfoose, J.; Baune, B.T. Evidence for a Cytokine Model of Cognitive Function. Neurosci. Biobehav. Rev. 2009, 33, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Godbout, J.P.; Johnson, R.W. Age and Neuroinflammation: A Lifetime of Psychoneuroimmune Consequences. Immunol. Allergy Clin. N. Am. 2009, 29, 321–337. [Google Scholar] [CrossRef] [PubMed]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be Smart, Exercise Your Heart: Exercise Effects on Brain and Cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Martinez-Gomez, D.; Del Rosario Fernández-Santos, J.; Ortega, F.B.; Castro-Piñero, J.; Hillman, C.H.; Veiga, O.L.; Esteban-Cornejo, I. Longitudinal Associations of Physical Fitness and Body Mass Index with Academic Performance. Scand. J. Med. Sci. Sports 2021, 31, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Cornejo, I.; Cadenas-Sanchez, C.; Contreras-Rodriguez, O.; Verdejo-Roman, J.; Mora-Gonzalez, J.; Migueles, J.H.; Henriksson, P.; Davis, C.L.; Verdejo-Garcia, A.; Catena, A.; et al. A Whole Brain Volumetric Approach in Overweight/Obese Children: Examining the Association with Different Physical Fitness Components and Academic Performance. The ActiveBrains Project. Neuroimage 2017, 159, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Real, C.C.; Garcia, P.C.; Britto, L.R.G.; Pires, R.S. Different Protocols of Treadmill Exercise Induce Distinct Neuroplastic Effects in Rat Brain Motor Areas. Brain Res. 2015, 1624, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Audiffren, M.; André, N. The Exercise-Cognition Relationship: A Virtuous Circle. J. Sport Health Sci. 2019, 8, 339–347. [Google Scholar] [CrossRef]
- Chang, Y.-K.; Chen, F.-T.; Kuan, G.; Wei, G.-X.; Chu, C.-H.; Yan, J.; Chen, A.-G.; Hung, T.-M. Effects of Acute Exercise Duration on the Inhibition Aspect of Executive Function in Late Middle-Aged Adults. Front. Aging Neurosci. 2019, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-K.; Chu, C.-H.; Wang, C.-C.; Wang, Y.-C.; Song, T.-F.; Tsai, C.-L.; Etnier, J.L. Dose-Response Relation between Exercise Duration and Cognition. Med. Sci. Sports Exerc. 2015, 47, 159–165. [Google Scholar] [CrossRef] [PubMed]
- McCrady, S.K.; Levine, J.A. Sedentariness at Work: How Much Do We Really Sit? Obesity 2009, 17, 2103–2105. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Kukkonen-Harjula, K.T.; Verbeek, J.H.; Ijaz, S.; Hermans, V.; Bhaumik, S. Workplace Interventions for Reducing Sitting at Work. Cochrane Database Syst. Rev. 2016, 3, CD010912. [Google Scholar] [CrossRef]
- Dogra, S.; Dunstan, D.W.; Sugiyama, T.; Stathi, A.; Gardiner, P.A.; Owen, N. Active Aging and Public Health: Evidence, Implications, and Opportunities. Ann. Rev. Public Health. 2022, 43, 439–459. [Google Scholar] [CrossRef]
- Roschel, H.; Artioli, G.G.; Gualano, B. Risk of Increased Physical Inactivity During COVID-19 Outbreak in Older People: A Call for Actions. J. Am. Geriatr. Soc. 2020, 68, 1126–1128. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.; Bluck, S.; McAdams, D.P. More Vulnerable? The Life Story Approach Highlights Older People’s Potential for Strength During the Pandemic. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e45–e48. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-J.; Fox, K.R.; Ku, P.-W.; Chang, Y.-W. Effects of Aquatic Exercise on Sleep in Older Adults with Mild Sleep Impairment: A Randomized Controlled Trial. Int. J. Behav. Med. 2016, 23, 501–506. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Study; Country/Region | Participant Characteristics | Intervention | Outcome Measures | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample | Participants (Age Range; Sex-M%) | Sample Size (IG/CG) | Design | Type | Intensity | Frequency | Length (mins) | |||
| 1 | Abel et al., 2023; Spain | OW/OB | 10.03 ± 1.51; 59% | 101 (51/50) | AE+RT (60 min of AE and 30 min of RT) | Chronic | 80% of the maximal heart rate and at the level of the anaerobic threshold | 90 min/session, 3–5 × wk | 20 wk (9000) | 1. CF:Design Fluency Test and Trail Making Test; 2. Inhibition:modified version of the Stroop test; 3. WM:Delayed Nonmatch-to-Sample (DNMS) computerized task; 4. AP:Spanish version of the Woodcock-Johnson III Tests of Achievement |
| 2 | Furlano et al., 2023; Canada | OW/OB | 68.7 ± 5.7; 50% | 24 (13/11) | RT (2 sets of 6 to 8 repetitions of exercises) | Chronic | 80% × 1RM | 60 min/session, 3 × wk | 24 wk (1440) | 1. inhibition:Stroop Test (condition C–B); 2. WM:Digit Span Test; |
| 3 | Domal et al., 2023; India | OW/OB | 24 ± 4.5 (65%) | 13 (7/6) | PTE (individualized graded target for each week via step count) | Chronic | - | - | 8 wk (-) | 1. inhibition:Eriksen flanker test |
| 4 | Chou et al., 2023; China | OW | 10.0 ± 1.1 (58.7%) | 50 (25/25) | AE (competitive team games, i.e., running, jump rope) | Chronic | MVPA | 40 min/session, 5 × wk | 10 wk (2000) | 1. inbibition:Stroop Test of the Vienna Test System; 2. AP:Taiwan’s Ministry of Education was used to measure competence in Chinese language and mathematics in fifth and sixth graders. |
| 5 | Oliveira et al., 2022; Brazil | OW/OB | 31.3 ± 7.1 (40.6%) | 64 (20/21/23) | HIIT | Chronic | VPA | 30 min/session, 3 × wk | 12 wk (1080) | 1. inhibition:the Stroop Color-Words Test |
| AE | MVPA | |||||||||
| PTE | - | |||||||||
| 6 | Zhang et al., 2022, China | OW/OB | 11.56 ± 1.03 (79.2%) | 57 (19/19/19) | HIIT | Acute | VPA | 30 min/session | - | 1. Inhibition: the Stroop Color and Word Test. |
| AE | VPA | |||||||||
| CT | - | |||||||||
| 7 | Zlibinaite et al., 2021, Lithuania | OW/OB | 46.8 ± 6.2 (0%) | 33 (17/16) | AE (cycling sessions) | Chronic | MPA | 60 min/session, 5 × wk | 8 wk (2400) | 1. Inhibition: the Stroop Color and Word Test: go/no-go task; 2. WM: mathematical processing task; 3. CF: 2-choice reaction time task. |
| 8 | Zlibinaite et al., 2020, Lithuania | OW/OB | 44.9 ± 6.2 (0%) | 26 (13/13) | AE | Chronic | MPA | 50 min/session, 3 × wk | 24 wk (3600) | 1. WM: mathematical processing task; 2. CF: 2-choice reaction time task; 3. Memory: verbal working memory. |
| 9 | Zhang et al., 2020, China | OB | 14.6 ± 0.7 (47.4%) | 38 (19/19) | CPA (jump rope) | Acute | MPA | - | 30 min | 1. Inhibition: modified food-cue-related Stroop test. |
| 10 | Chou et al., 2020, China | OW | 12.19 ± 0.68 (61.9%) | 84 (44/40) | CPA (movement game) | Chronic | - | 40 min/session, 3 × wk | 8 wk (960) | 1. Inhibition: Stroop test. |
| 11 | Inoue et al., 2020 | OB | 30.0 ± 5.4 (100%) | 20 (10/10) | HIIT/AE | Chronic | VPA | 40 min/session, 3 × wk | 6 wk (720) | 1. Inhibition: Stroop Color and Word Test. |
| 12 | Liu et al., 2018, China | OB | 14.06 ± 0.83 (57.1%) | 70 (35/35) | CPA (jump rope) | Chronic | VPA | 75 min/session, 2 × wk | 12 wk (1800) | 1. Inhibition: classic Stroop color–word conflict task/food-cue condition. |
| 13 | Allom et al., 2018, Australia | OB | 41.39 ± 7.85 (13.75%) | 80 (42/38) | PTE | Chronic | - | - | 5 wk | 1. CF: Wisconsin Card Sorting Test/paper and pencil Trail Making Test. |
| 14 | Quintero Gacharná et al., 2018 | OW/OB | 44.38 ± 8.59 (21.6%) | 95 (50/45) | RT/HIIT/RT+HIIT | Acute | MPA | - | 1. Inhibition: Stroop Color and Word Test. | |
| 15 | Chen et al., 2017, China | OB | 14.05 ± 0.83 (57.6%) | 66 (33/33) | CPA (jump rope) | Chronic | MVPA | 120 min/session, 6 × wk | 12 wk (8640) | 1. CF: Tower of London—Drexel task. |
| 16 | Wennberg et al., 2015, Australia | OW/OB | 59.7 ± 8.1 (52.6%) | 38 (19/19) | PTE | Acute | - | - | - | 1. Inhibition: modified Stroop color–word task. |
| 17 | Chen et al., 2016, China | OB | 12.74 ± 0.73 (56%) | 50 (25/25) | AE | Chronic | MVPA | 40 min/session, 4 × wk | 12 wk (1920) | 1. CF: Wisconsin Card Sorting Test. |
| 18 | Dao et al., 2013, Canada | OW | 69.44 ± 2.91 (0%) | 77 (41/36) | RT | Chronic | MVPA | 40 min/session, 2 × wk | 13 wk (3840) | 1. Inhibition: the Stroop test. |
| 19 | Davis et al., 2007, USA | OW | 9.3 ± 1.0 (44%) | 116 (56/60) | CPA (jump rope) | Chronic | MVPA | 40 min/session, 7 × wk | 16 wk (1080) | 1. AP: Woodcock–Johnson Tests of Achievement III. |
| 20 | Smith et al., 2010, USA | OW/OB | 52.3 ± 9.6 (36%) | 81 (43/38) | AE | Chronic | MVPA | 40 min/session, 5 × wk | 12 wk (3641) | 1. Inhibition: Stroop Interference; 2. CF: Trail Making Test B-A; 3. WM: Digit span. |
| CT | 2.72 (2.35, 3.09) | 7.15 (5.03, 9.27) | 12.79 (7.55, 18.03) | 0.04 (−1.33, 1.41) | CF–accuracy | |||
| CF-RT | 13.65 (10.31, 16.99) | MIX | 4.43 (2.28, 6.58) | 10.07 (4.82, 15.32) | −2.68 (−4.10, −1.26) | |||
| −20.54 (−33.86, −7.22) | −34.19 (−47.92, −20.46) | PTE | 5.64 (−0.01, 11.29) | −7.11 (−9.64, −4.59) | ||||
| −39.12 (−68.02, −10.22) | −52.77 (−81.86, −23.68) | −18.58 (−50.40, 13.24) | CPA | −12.75 (−18.17, −7.33) | ||||
| 0.02 (−0.03, 0.07) | −13.63 (−16.97, −10.29) | 20.56 (7.24, 33.88) | 39.14 (10.24, 68.04) | AE | ||||
| CT | 0.08 (−0.17, 0.33) | 0.06 (−0.17, 0.29) | 1.40 (−15.66, 18.46) | 0.02 (−0.23, 0.27) | inhibition–accuracy | |||
| inhibition–RT | −2.19 (−6.20, 1.82) | HIIT | −0.02 (−0.14, 0.11) | 1.32 (−15.74, 18.38) | −0.06 (−0.21, 0.09) | |||
| −0.61 (−6.60, 5.37) | 1.58 (−3.95, 7.11) | PTE | 1.34 (−15.72, 18.40) | −0.04 (−0.17, 0.08) | ||||
| −1.52 (−7.37, 4.33) | 0.68 (−5.40, 6.75) | −0.91 (−8.78, 6.96) | RT | −1.38 (−18.44, 15.68) | ||||
| −0.74 (−3.93, 2.45) | 1.45 (−2.23, 5.12) | −0.13 (−5.55, 5.29) | 0.77 (−5.49, 7.04) | AE | ||||
| 0.75 (−4.29, 5.80 | 1.44 (−4.34, 7.22) | −0.14 (−7.56, 7.28) | 4.40 (−2.23, 11.03) | 0.76 (−5.47, 7.00) | MIX | |||
| −5.15 (−9.37, −0.93) | −2.96 (−8.70, 2.79) | −4.54 (−12.09, 3.01) | −3.64 (−10.77, 3.50) | −4.41 (−9.73, 0.91) | −4.40 (−11.03, 2.23) | CPA | ||
| CT | −0.30 (−1.52, 0.92) | 2.20 (−0.72, 5.12) | −0.50 (−1.96, 0.97) | WM–accuracy | WM-RT | CT | ||
| AP | CT | MIX | 2.50 (−0.66, 5.66) | −0.20 (−2.11, 1.71) | 0.01 (−0.35, 0.32) | AE | ||
| 3.54 (3.12, 3.96) | MIX | RT | −2.70 (−5.96, 0.57) | |||||
| 2.00 (0.89, 3.11) | −1.54 (−2.72, −0.36) | CPA | AE | |||||
| −2.88 (−4.27, −1.49) | −6.42 (−7.87, −4.97) | −4.88 (−6.66, −3.10) | AE |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, J.; Liu, J.; Zhu, R.; Liu, G.; Zheng, M.; Cao, C. The Impact of Different Types of Exercise on Executive Functions in Overweight/Obese Individuals: A Systematic Review and Network Meta-Analysis. Behav. Sci. 2024, 14, 1227. https://doi.org/10.3390/bs14121227
Guo J, Liu J, Zhu R, Liu G, Zheng M, Cao C. The Impact of Different Types of Exercise on Executive Functions in Overweight/Obese Individuals: A Systematic Review and Network Meta-Analysis. Behavioral Sciences. 2024; 14(12):1227. https://doi.org/10.3390/bs14121227
Chicago/Turabian StyleGuo, Jia, Jingqi Liu, Ruihan Zhu, Guochun Liu, Man Zheng, and Chunmei Cao. 2024. "The Impact of Different Types of Exercise on Executive Functions in Overweight/Obese Individuals: A Systematic Review and Network Meta-Analysis" Behavioral Sciences 14, no. 12: 1227. https://doi.org/10.3390/bs14121227
APA StyleGuo, J., Liu, J., Zhu, R., Liu, G., Zheng, M., & Cao, C. (2024). The Impact of Different Types of Exercise on Executive Functions in Overweight/Obese Individuals: A Systematic Review and Network Meta-Analysis. Behavioral Sciences, 14(12), 1227. https://doi.org/10.3390/bs14121227