
Repetitive Transcranial Magnetic Stimulation for the Treatment of Resistant Depression: A Scoping Review




Abstract
:1. Introduction
2. Methodology
2.1. Inclusion and Exclusion Criteria
2.2. Data Extraction
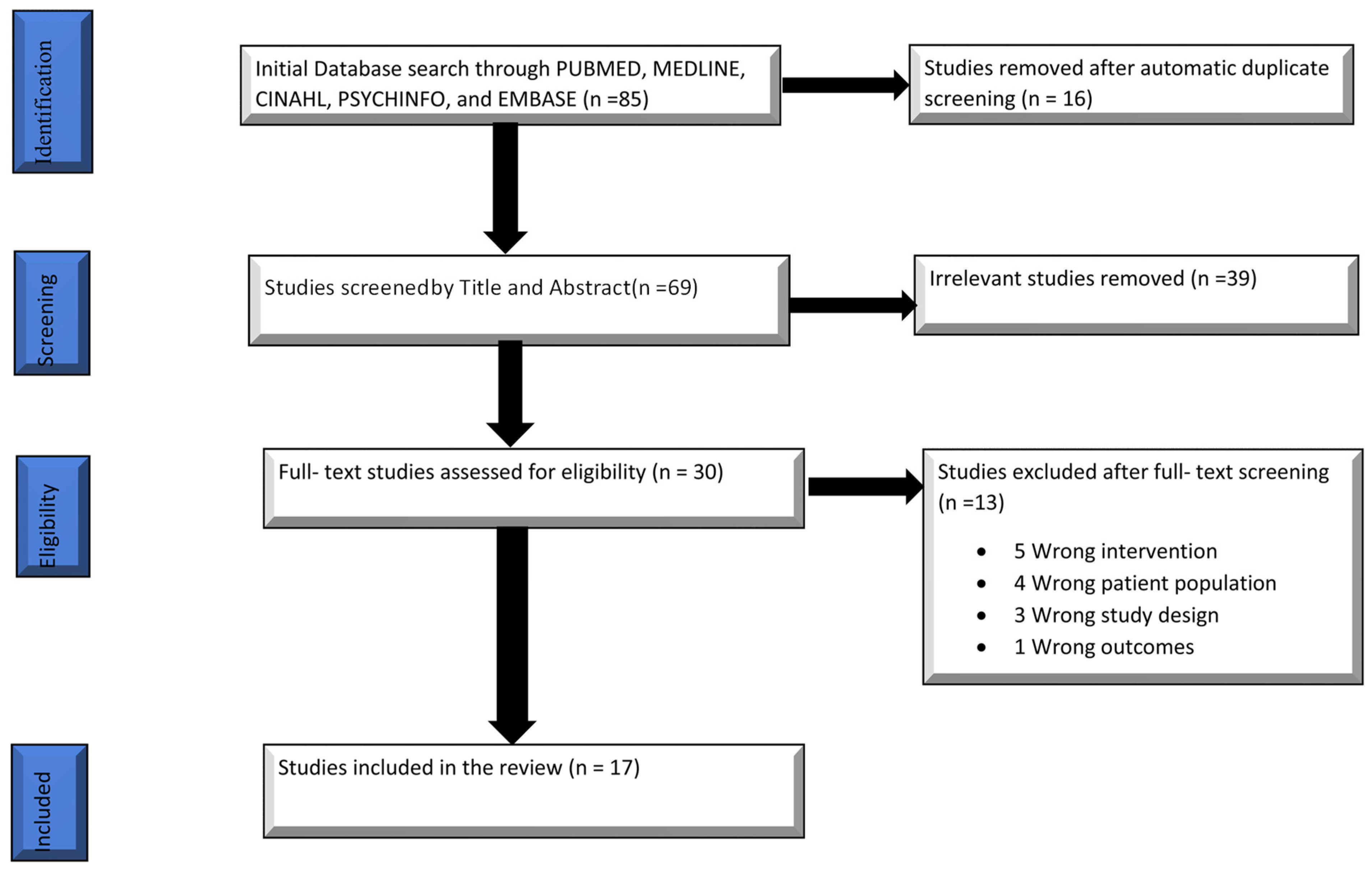
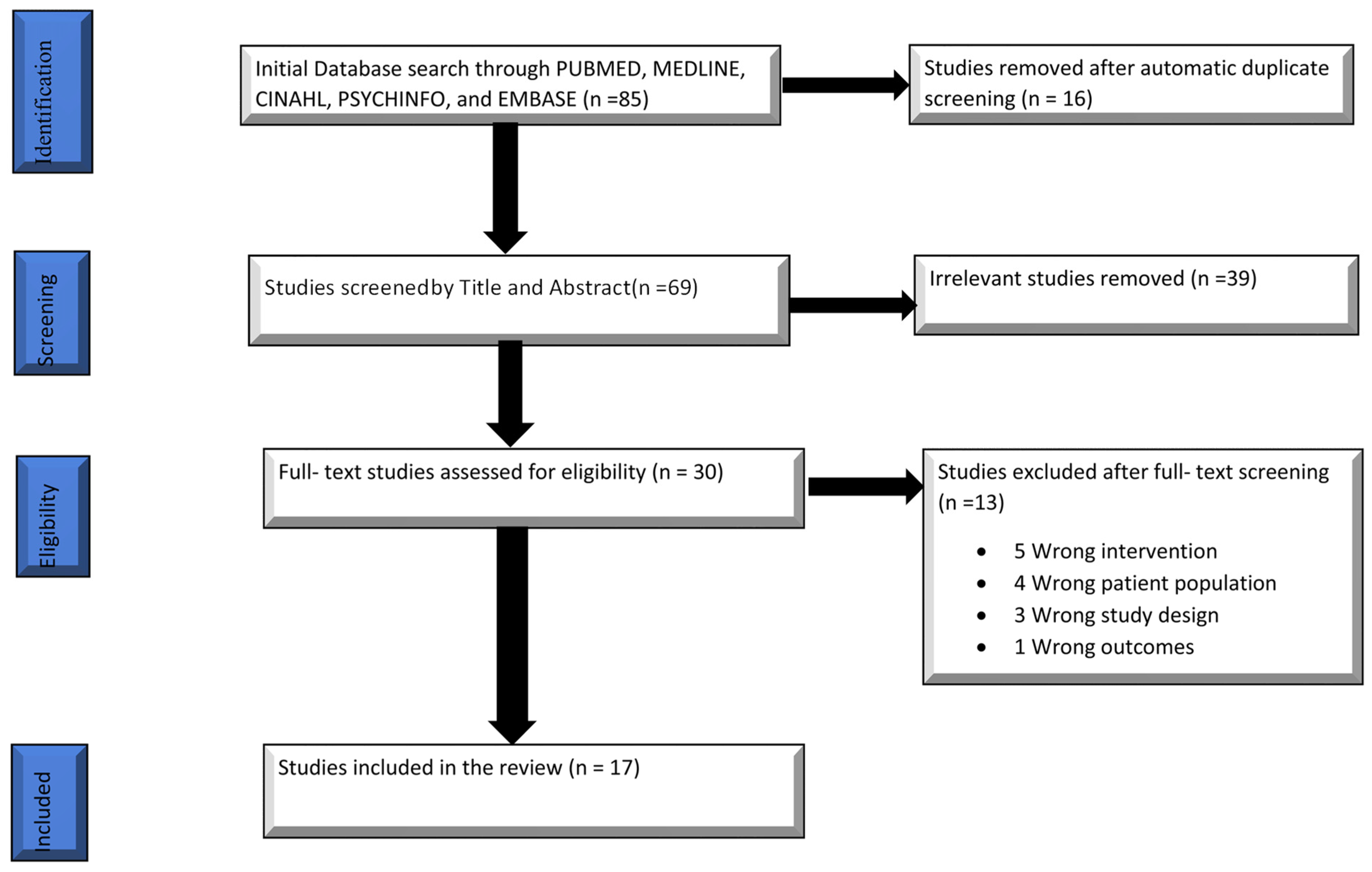
3. Results

{kind=link}
| Researcher R.S. | ||||
|---|---|---|---|---|
| Yes | No | Total | ||
| Researcher M.A. | Yes | 15 | 4 | 19 |
| No | 1 | 10 | 11 | |
| Total | 16 | 14 | 30 | |
3.1. Overview of the Extracted Studies
3.2. Targeted Symptoms
3.3. rTMS Protocol
3.4. Targeted Brain Region of rTMS
3.5. Outcome Measures
3.6. Outcome Results
3.7. Efficacy of the Two-coil rTMS Device
3.8. Tolerability and Side Effects
| Author (Year) | Country of Origin | Study Design | Age Range | Number of Participants | Targeted Brain Region | Targeted Symptom | Measurement | Duration of Treatment | Coil/ rTMS Parameters/Stimulation Method | Outcome/Significant Improvements/Effect Size | Assessment and Follow-Up | Conclusions | Side Effects |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rosen et al. (2021) [51] | USA | RCT | 27–78 years | 49 | DLPFC | Change in depression symptoms | HAM-D 24 item | 5–12 calendar days | MagPro R30 stimulator with a B65-A/P coil (10 Hz, 4 s on, 10 s off, 120% MT, 4000 pulses/session, 25 min per session) daily in blocks of 5 for a min. of 20 sessions (80,000 pulses), max. of 30 sessions (120,000 pulses) | Average stimulation location for responders vs. non-responders differed in the active but not in the sham condition (p = 0.02) Average responder location derived from the active condition showed significant negative functional connectivity with the subgenual cingulate (p < 0.001), while the non responder location did not (p = 0.17) | Baseline and acute phase | Clinical response to rTMS is related to accuracy in targeting the region within DLPFC that is negatively correlated with subgenual cingulate. Results support the validity of a neuro-functionally informed rTMS therapy target in veterans. | None reported |
| Theleritis et al. (2017) [42] | Greece | Parallel-group RCT | 18–59 years | 98 | L-DLPFC | Change in depressive symptom severity | HDRS CGI-I | 3 weeks | Magstim ultrarapid stimulator with a figure-8 magnetic coil. 40 trains of 20 Hz at 100% MT for 2 s and intertrain 1 min, yielding 1600 pulses per session | Twice-daily sessions might be more effective in both response and remission rates. Patients who had lower baseline HDRS (OR = 0.75, p = 0.014) and CGI-S scores (OR = 0.18, p = 0.001) were more likely to achieve remission | Baseline, and at the end of the first, second, third, and fifth week (follow up) | Twice per day, active HF-rTMS might be more effective than once per day, active HF-rTMS Practically none of the subjects in either sham group achieved remission | Discomfort at the site of stimulation Exacerbation of preexisting headache |
| Kavanaugh et al. (2018) [43] | USA | Double-blind, sham-controlled trial | 18–70 years | 84 | L-DLPFC & dorso-medial PFC | Neurocognitive safety of the 2-coil device | HAM-D 24 CGI QLESQ-SF | 4–6 weeks | 2 Magstim Rapid2 stimulators. 70 mm figure-eight coil 10 Hz 120 MT of 4 s and 26 s rest Total of 3000 pulses per session | No observed negative neurocognitive effects of the 2-coil rTMS device. A significant effect of active rTMS was observed on the quality of episodic memory. Baseline quality of episodic memory predicted depression treatment response and remission. | Baseline, one month | 2-coil rTMS device is a cognitively safe treatment for TRD that may possess episodic memory-enhancing capabilities. | Nil |
| Carpenter et al. (2017) [44] | USA | Randomized double-blind sham-controlled trial | 18–70 years | 92 | L-DLPFC & dorso-medial PFC | Safety and efficacy of an investigational 2-coil rTMS device on depression symptoms | HAM-D 24 C-SSRS ATRQ | 4–6 weeks | 2 Magstim Rapid2 stimulators. single Magstim 70 mm figure eight coil 10 Hz 120 MT in trains of 4 s 26 s rest. 20 daily rTMS. A total 3000 pulses per session | n = 75 showed significantly greater improvement (mean HAMD-24 change) over time for the active (n = 38) versus sham (n = 37) group after 20 sessions (F = 7.174; p = 0.008) & also at the one-month follow-up (F = 6.748; p = 0.010) Effect size (Cohen’s d) for 4-week efficacy of rTMS with the two-coil device (ITT d = 0.58; PP = 0.52) | Baseline, Four weeks | Significant antidepressant effects after only 4-weeks of treatment and was well tolerated. | Headache Muscle twitch/spasms |
| Trevizol et al. (2019) [54] | USA | RCT | ≥60 years | 43 | Unilateral & bilateral L- DLPFC | The primary outcome was the remission of depression. | HDRS SCID-II | 3 weeks | Magventure RX-100 Stimulation with a cool B-65 figure-of-8 coil. 120% of RMT 10 Hz 15 sessions at five sessions/week over three weeks | Participants receiving bilateral rTMS experienced greater remission rates (40%) compared to unilateral (0%) or sham (0%) groups Response to rTMS in the HDRS similarly favoured the efficacy of bilateral rTMS | Baseline, week 3 week 6. | Sequential bilateral treatment may be an optimal form of rTMS when used for TRD in older adults | nil |
| DM Blumberger et al. (2018) [35] | Canada | Randomized non-inferiority trial | 18–65 years | 414 | L-DLPFC | Change in the score of depression symptoms as read on HRSD-17 | HRSD-17 QIDS-SR BSI-A DS-30 | Five days a week for 4–6 weeks | MagPro X100 or R30 stimulator with B70 fluid-cooled coil. 10 Hz rTMS at 120% RMT 4 s on and 26 s off; 3000 pulses/session; total of 37.5 min. 120% RMT iTBS triplet 50 Hz bursts, repeated at 5 Hz; 2 s on and 8 s off; 600 pulses/ session; a total of 3 min 9 s | HRSD-17 scores improved from 23.5 (SD 4.4) to 13.4 (7.8) in the 10 Hz rTMS group and from 23.6 (4.3) to 13.4 (7.9) in the iTBS group (adjusted difference 0.103, lower 95% CI–1.16; p = 0.0011) | Baseline, after every five treatments and one week, Four weeks, and 12 weeks after treatment | iTBS is non-inferior to standard 10 Hz rTMS in reducing depressive symptoms. | Headache |
| Iwabuchi et al. (2019) [45] | Canada | RCT | 18–70 years | 27 | DLPFC | rTMS Treatment response in TRD | HAM-D BDI | 4 weeks | Magstim Super Rapid 2 Plus 1 stimulator 70 mm Double Air Film Coil. iTBS at ten bursts of 3 pulses 80%MT at 50 Hz applied at 5 Hz repeated at five runs of 600 pulses with 5 min rest. rTMS at 75 trains of 10 Hz 4 s per train rest 26 s intertrain intervals | rTMS treatment response rate was (55% for rTMS, 69% for iTBS). HAMD scores were significantly reduced at both one month (p < 0.001) and three months (p < 0.001) compared to baseline. | Baseline, Four weeks, 12 weeks | The study demonstrates that resting-state connectivity signatures can predict response to rTMS treatment in patients with resistant depression (irrespective of methodological variations in stimulus delivery). | Nil |
| BARBINI et al. (2021) [55] | UK | Randomized single-blinded study | - | 80 | DLPFC | Depressive symptoms in TRD | HDRS | 3 weeks | rTMS applied MagstimVR stimulator with a figure-8 coil over the DLPFC. | rANOVA (F = 2.766, p = 0.043) & post-hoc in HDRS-17 showed significant better scores in favor of group B (rTMS plus BLT) every week (p < 0.025, T1: 22.075 vs. 17.200; T2: 16.100 vs. 12.775; T3: 12.225 vs. 8.900) | Baseline, week 1, week 2, week 3 | The antidepressant effect of rTMS was enhanced and accelerated by its combination with BLT in treating resistant depression. Both treatment protocols were effective in reducing depressive symptomatology. | Nil |
| P.F.P. van Eijndhoven, et al. (2020) [46] | Netherlands | RCT | Adults | 31 | L-PFC | Depression symptoms in severe TRD patients | HDRS | 4 weeks | Magstim Rapid 2 TMS with a focal, 8-figure shaped 70 mm coil. 110%RMT, 10 Hz 60 trains. 5 s with a resting period of 25 s between each train. 30 min with 3000 pulses/session, five days for four weeks, a total of 60,000 pulses | Interim analysis in the form of a mixed ANOVA indicated that there was a main effect of time (F (1,30) = 25.4; p < 0.01), but not for treatment (F(1,30) = 1.5; p = 0.23), and there was no interaction between time and treatment (F(1,30) = 0.45; p = 0.50) | Baseline, after 5, 10, 15, 20 sessions and one-week post-treatment | “Standard” 4-week rTMS treatment is not effective in chronic, severe TRD | Mild to moderate headache |
| Kito et al. (2019) [50] | Japan | Randomized open-label trial | 25–75 years | 30 (28 completed) | L-PFC | Remissions in depression symptoms | QIDS PHQ-9 YMRS | 4–6 weeks | MagPro R30 magnetic stimulator and a Cool-B65 coil. rTMS at 120%MT, 10 HZ a total of 3000 pulses/d five days a week, for 4–6 weeks (Standardized rTMS) conventional rTMS 75 trains “4 s on and 26 s off” for 37.5 min with 3000 pulses | 13/30 patients (43.3%) showed remission at week 6 There were no significant differences in the remission rate between the conventional 37.5-min and 18.75-min protocol groups (46.7% and 40.0%, respectively) | Baseline, week 2, week 4, and week 6. | Compared with conventional, rTMS with 18.75-min protocol might be equally effective and clinically beneficial in saving the treatment session length | Stimulation pain or discomfort |
| Filipčić et al. (2020) [47] | Croatia | Two-arm, unicentric, double-blind pilot randomized trial | 18–68 years | 28 | DLPFC | Change in depression symptoms and rate of remissions | HDRS BDI-II | 10–15 days | Magstim Rapid2 stimulator at 120% MT Each the session lasted for 20 min at 18 Hz: 2-s trains; 20-s intertrain intervals; 55 trains; a total of 1980 pulses per session or 3960 pulses per day | HDRS scores decreased by 13 (95% CI 11–17; 59%, 95% CI 45–73%) and 13 (95% CI 11–14; 62%, 95% CI 54–69%) points in the 10- and 15-day protocols, respectively | Baseline and daily adTMS | adTMS with H1-coil regimen twice daily for ten days or 15 days can be a safe and effective alternative for the treatment of TRD. | Nil |
| Benadhira, et al. (2017) [48] | France | Randomized sham-controlled study | 22–79 years | 58 | L-DLPFC | Depression symptoms of TRD | HDRS | 1 month (phase 1) 11 months (phase 11) | Magstim Super Rapid stimulator with figure-eight 70-mm coils 10 Hz at 110% MT 25 trains of 8 s interval of 30 s, for 5 days per week, for one month (20 sessions, M1) for a total of 2000 pulses per session. | Phase I, 35 patients were responders (60%) and 16 were partial responders (28%) 16 patients (28%) were in remission after one month of active rTMS HDRS scores, a significant difference was found between baseline and M1 (t (57) = 17.476; p < 0.001) | Baseline, weekly during the first month (M1) & monthly for the maintenance phase (M2 to M6) | rTMS could represent a novel strategy for preventing relapse in TRD patients who respond to rTMS treatment Weekly maintenance sessions could be useful, showing beneficial effects during the fourth month of treatment. | Nil |
| Roach et al. (2020) [52] | USA | Clinical trial | ≥18 years | 61 | L-DLPFC | To test whether depressive symptoms changed significantly throughout treatment | PHQ-9 | 4–6 weeks | NeuroStar TMS 120% MT at 10 Hz 4 s followed by 10- to 26-s rest for a total of 3000 pulses/session. Five days a week for 4 to 6 weeks, for a total of 90,000 pulses | Average (SD) pretreatment and posttreatment PHQ-9 scores were 15.8 (6.2) and 12.6 (7.6), respectively. Statistically significant reduction in post–PHQ-9 was demonstrated (p < 0.001) with 69% of patients lowering their ratings & 31% demonstrating reliable change (improvement >5.64) Effect size (Cohen d = 0.46 on the paired t-test of pre–/post–PHQ-9) | Baseline, week 4, week 6 | rTMS for TRD is an adequate treatment or augmentation option for ADSMs with MDD | Nil |
| Yesavage, et al. (2018) [49] | USA | A double-blind, sham-controlled randomized clinical | 18–80 years | 164 | L-PFC | Remission of depression symptoms And the severity of depression symptoms | HRSD BDI | 3 weeks | MagPro R30 device with Cool-B65-A/P coil. 10 Hz, 120%MT 5 sessions over 5 to 12 days A total of 4000 pulses/ session. | Overall remission rate was 39%, with no significant difference between the active and sham groups No significant effect of treatment (odds ratio, 1.16; 95% CI, 0.59–2.26; p = 0.67) | Baseline, end of treatment & 24-week follow up. | This study supports the clinical observation that a combination of interventions, including rTMS, effectively achieves symptom remission in 39.0% of veterans with MDD who were previously treatment-resistant. | Headache Naso- pharyngitis Suicidal ideation |
| Croarkin, et al. (2021) [53] | USA | Double-blind, randomized, sham-controlled trial | 12–21 years | 103 Sham (n = 55) Active (n = 48) | L-PFC | Change in the HAM-D 24 score | HAM-D, MADRS, CDRS-R, QIDS-A17-SR, CGI-S | 6 weeks | NeuroStar XPLOR TMS 120%MT 10 pulses per sec (10 Hz) for 4 s, and with an interval of 26 s Each treatment session was 37.5 min (75 trains) for 3000 pulses per session. | Improvement in HAM-D-24 scores was similar between the active (−11.1 [2.03]) & sham groups (−10.6 [2.00]; p = 0.8; difference [95% CI], −0.5 [−4.2 to 3.3]) Response rates were 41.7% in the active group and 36.4% in the sham group (p = 0.6) Remission rates were 29.2% in the active group and 29.0% in the sham group (p = 0.95) | Baseline Week 4 and Weeks 6 | Left prefrontal 10-Hz TMS monotherapy in adolescents with TRD is feasible, tolerable, and safe A statistically significant difference between 6 weeks of sham and active TMS was not observed. | Suicidal ideation, worsening depression during week 4, suicide attempt during week 6 |
| Fitzgerald et al. (2020) [27] | Australia | Four arm RCT | Adults | 300 | L-DLPFC & R DLPFC | Response and remission rates of depression symptoms | HRSD-17 | 4 weeks | Medtronic Magpro30 magnetic stimulators with fluid-filled 70 mm figure-of-8 coils rTMS at 120% RMT 10 Hz for groups (1 and 2), 1 Hz for groups (3 and 4). (left standard = 50 trains, left high = 125 trains, right standard = 20 min, right high = 60 min, all per day in a single session). | The rate of response exceeded 45% in all groups No significant difference between groups on initial analysis of the primary or secondary outcome measures (response rates: standard left = 52.5%, high left = 47.3%, standard right = 49.1%, high right = 48.4%) Greater remission rate with high compared to moderate dose left- sided treatment when controlling for illness duration | Baseline and after 1, 2, 3, and 4 weeks | No consistent association between the antidepressant effect of rTMS & the number of TMS pulses provided across the ranges investigated in this study. Increasing TMS pulse number in individual sessions seems unlikely to be a method to substantially improve clinical outcomes. | Nil |
| Zhao et al. (2019) [56] | China | RCT | ≥60 years | 58 | L-DLPFC | Serum levels of brain-derived neurotrophic factor (BDNF), interleukin (IL)-1b, and tumour necrosis factor (TNF)-a in elderly patients with refractory depression. | HAM-D 24 | 1 month | YRDCCY-I TMR apparatus 10 Hz at 80% MT | BDNF levels gradually increased with treatment duration in the rTMS group and were significantly higher compared with the control group In contrast, IL-1b and TNF-a levels gradually decreased and were significantly lower than in the control group None of the serum factors was affected by rTMS in healthy individuals | Baseline, at 48 h and 1, 2, 3, and 4 weeks after the first TMS treatment | rTMS increased serum BDNF levels and decreased serum IL-1b and TNF-a levels in patients with depression but had no effect on any of these factors in healthy individuals Results suggest that rTMS may increase BDNF and decrease IL-1b and TNF-a serum levels in elderly patients with refractory depression. | Nil |
3.9. Frequency, Intensity of Stimulation, and Duration of Treatment
3.10. Variations in the Brain Target
3.11. Comparing the Efficacy and Tolerability of the Different Forms of rTMS
3.12. Maintenance rTMS Treatment
3.13. Relationship between the Pulse Number and the Response to rTMS in TRD
- Standard-dose HFL-rTMS: 50 trains of 10 Hz rTMS; 4.5 s trains at 120% RMT with a 20.5 s inter-train interval (2250 pulses/session).
- High-dose HFL-rTMS:125 trains of 10 Hz rTMS; 4.5 s trains at 120% RMT; a 15.5 s inter-train interval (5625 pulses/session).
- Standard-dose LFR-rTMS: one continuous train of 1 Hz rTMS; 20 min at 120% RMT (1200 pulses).
- High-dose LFR-rTMS: two trains of 1 Hz rTMS; 30 min at 120% RMT (3600 pulses/session).
3.14. Effect of rTMS on the Serum BDNF, IL-1b, and TNF-a Levels in TRD
4. Discussions
4.1. Cost and Policy Implications for rTMS in TRD
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Doktorchik, C.; Patten, S.; Eastwood, C.; Peng, M.; Chen, G.; Beck, C.A.; Jetté, N.; Williamson, T.; Quan, H. Validation of a case definition for depression in administrative data against primary chart data as a reference standard. BMC Psychiatry 2019, 19, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hovington, C.L.; McGirr, A.; Lepage, M.; Berlim, M.T. Repetitive transcranial magnetic stimulation (rTMS) for treating major depression and schizophrenia: A systematic review of recent meta-analyses. Ann. Med. 2013, 45, 308–321. [Google Scholar] [CrossRef] [PubMed]
- Barbui, C.; Butler, R.; Cipriani, A.; Geddes, J.; Hatcher, S. Depression in adults: Drug and physical treatments. BMJ Clin. Evid. 2007, 2007, 1003. [Google Scholar] [PubMed]
- Pradhan, B.; Parikh, T.; Makani, R.; Sahoo, M. Ketamine, transcranial magnetic stimulation, and depression specific yoga and mindfulness based cognitive therapy in management of treatment resistant depression: Review and some data on efficacy. Depress. Res. Treat. 2015, 2015, 842817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serafini, G.; Pompili, M.; Innamorati, M.; Dwivedi, Y.; Brahmachari, G.; Girardi, P. Pharmacological properties of glutamatergic drugs targeting NMDA receptors and their application in major depression. Curr. Pharm. Des. 2013, 19, 1898–1922. [Google Scholar] [CrossRef] [PubMed]
- Greer, T.L.; Kurian, B.T.; Trivedi, M.H. Defining and measuring functional. CNS Drugs 2010, 24, 267–284. [Google Scholar] [CrossRef]
- Hawton, K.; i Comabella, C.C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef]
- Trevino, K.; McClintock, S.M.; Fischer, N.M.; Vora, A.; Husain, M.M. Defining treatment-resistant depression: A comprehensive review of the literature. Ann. Clin. Psychiatry 2014, 26, 222–232. [Google Scholar]
- Fava, M. Diagnosis and definition of treatment-resistant depression. Biol. Psychiatry 2003, 53, 649–659. [Google Scholar] [CrossRef]
- Üstün, T.B.; Ayuso-Mateos, J.L.; Chatterji, S.; Mathers, C.; Murray, C.J. Global burden of depressive disorders in the year 2000. Br. J. Psychiatry 2004, 184, 386–392. [Google Scholar] [CrossRef]
- Greden, J.F. The burden of disease for treatment-resistant depression. J. Clin. Psychiatry 2001, 62, 26–31. [Google Scholar] [PubMed]
- Fawcett, J.; Kravitz, H. Treatment refractory depression. Common Treat. Probl. Depress. 1985, 5, 1–27. [Google Scholar]
- Heimann, H. Therapy-Resistant Depressions: Symptoms and Syndromes: Contibutions to Symptomatology and Syndromes. Pharmacopsychiatry 1974, 7, 139–144. [Google Scholar] [CrossRef]
- Nierenberg, A.; Keck, P.; Samson, J.; Rothschild, A.; Schatzberg, A. Methodological considerations for the study of treatment-resistant depression. Adv. Neuropsychiatry Psychopharmacol. 1991, 2, 83–91. [Google Scholar]
- Fava, M.; Davidson, K.G. Definition and epidemiology of treatment-resistant depression. Psychiatr. Clin. N. Am. 1996, 19, 179–200. [Google Scholar] [CrossRef]
- Berman, R.M.; Narasimhan, M.; Charney, D.S. Treatment-refractory depression: Definitions and characteristics. Depress. Anxiety 1997, 5, 154–164. [Google Scholar] [CrossRef]
- Russell, J.M.; Hawkins, K.; Ozminkowski, R.J.; Orsini, L.; Crown, W.H.; Kennedy, S.; Finkelstein, S.; Berndt, E.; Rush, A.J. The cost consequences of treatment-resistant depression. J. Clin. Psychiatry 2004, 65, 3839. [Google Scholar] [CrossRef] [PubMed]
- Gaynes, B.N.; Lloyd, S.W.; Lux, L.; Gartlehner, G.; Hansen, R.A.; Brode, S.; Jonas, D.E.; Evans, T.S.; Viswanathan, M.; Lohr, K.N. Repetitive transcranial magnetic stimulation for treatment-resistant depression: A systematic review and meta-analysis. J. Clin. Psychiatry 2014, 75, 477–489. [Google Scholar] [CrossRef]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D.; Niederehe, G.; Thase, M.E.; Lavori, P.W.; Lebowitz, B.D. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR* D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Gartlehner, G.; Gaynes, B.N.; Hansen, R.A.; Thieda, P.; DeVeaugh-Geiss, A.; Krebs, E.E.; Moore, C.G.; Morgan, L.; Lohr, K.N. Comparative benefits and harms of second-generation antidepressants: Background paper for the American College of Physicians. Ann. Intern. Med. 2008, 149, 734–750. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Li, C.; Wang, J. Updated review on the clinical use of repetitive transcranial magnetic stimulation in psychiatric disorders. Neurosci. Bull. 2017, 33, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Somani, A.; Kar, S.K. Efficacy of repetitive transcranial magnetic stimulation in treatment-resistant depression: The evidence thus far. Gen. Psychiatry 2019, 32, e100074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, A.T.; Jalinous, R.; Freeston, I.L. Non-invasive magnetic stimulation of human motor cortex. Lancet 1985, 325, 1106–1107. [Google Scholar] [CrossRef]
- Klomjai, W.; Katz, R.; Lackmy-Vallée, A. Basic principles of transcranial magnetic stimulation (TMS) and repetitive TMS (rTMS). Ann. Phys. Rehabil. Med. 2015, 58, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Eitan, R.; Lerer, B. Nonpharmacological, somatic treatments of depression: Electroconvulsive therapy and novel brain stimulation modalities. Dialogues Clin. Neurosci. 2006, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef]
- Fitzgerald, P.B.; Hoy, K.E.; Reynolds, J.; Singh, A.; Gunewardene, R.; Slack, C.; Ibrahim, S.; Daskalakis, Z.J. A pragmatic randomized controlled trial exploring the relationship between pulse number and response to repetitive transcranial magnetic stimulation treatment in depression. Brain Stimul. 2020, 13, 145–152. [Google Scholar]
- George, M.S.; Wassermann, E.M.; Kimbrell, T.A.; Little, J.T.; Williams, W.E.; Danielson, A.L.; Greenberg, B.D.; Hallett, M.; Post, R.M. Mood improvement following daily left prefrontal repetitive transcranial magnetic stimulation in patients with depression: A placebo-controlled crossover trial. Am. J. Psychiatry 1997, 154, 1752–1756. [Google Scholar]
- George, M.S.; Wassermann, E.M.; Williams, W.A.; Callahan, A.; Ketter, T.A.; Basser, P.; Hallett, M.; Post, R.M. Daily repetitive transcranial magnetic stimulation (rTMS) improves mood in depression. Neuroreport Int. J. Rapid Commun. Res. Neurosci. 1995, 6, 1853–1856. [Google Scholar] [CrossRef] [PubMed]
- O’Reardon, J.P.; Solvason, H.B.; Janicak, P.G.; Sampson, S.; Isenberg, K.E.; Nahas, Z.; McDonald, W.M.; Avery, D.; Fitzgerald, P.B.; Loo, C. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: A multisite randomized controlled trial. Biol. Psychiatry 2007, 62, 1208–1216. [Google Scholar] [CrossRef]
- George, M.S.; Lisanby, S.H.; Avery, D.; McDonald, W.M.; Durkalski, V.; Pavlicova, M.; Anderson, B.; Nahas, Z.; Bulow, P.; Zarkowski, P. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: A sham-controlled randomized trial. Arch. Gen. Psychiatry 2010, 67, 507–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimm, S.; Beck, J.; Schuepbach, D.; Hell, D.; Boesiger, P.; Bermpohl, F.; Niehaus, L.; Boeker, H.; Northoff, G. Imbalance between left and right dorsolateral prefrontal cortex in major depression is linked to negative emotional judgment: An fMRI study in severe major depressive disorder. Biol. Psychiatry 2008, 63, 369–376. [Google Scholar] [CrossRef] [PubMed]
- George, M.S.; Nahas, Z.; Molloy, M.; Speer, A.M.; Oliver, N.C.; Li, X.-B.; Arana, G.W.; Risch, S.C.; Ballenger, J.C. A controlled trial of daily left prefrontal cortex TMS for treating depression. Biol. Psychiatry 2000, 48, 962–970. [Google Scholar] [CrossRef]
- Klein, E.; Kreinin, I.; Chistyakov, A.; Koren, D.; Mecz, L.; Marmur, S.; Ben-Shachar, D.; Feinsod, M. Therapeutic efficacy of right prefrontal slow repetitive transcranial magnetic stimulation in major depression: A double-blind controlled study. Arch. Gen. Psychiatry 1999, 56, 315–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blumberger, D.M.; Vila-Rodriguez, F.; Thorpe, K.E.; Feffer, K.; Noda, Y.; Giacobbe, P.; Knyahnytska, Y.; Kennedy, S.H.; Lam, R.W.; Daskalakis, Z.J. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): A randomised non-inferiority trial. Lancet 2018, 391, 1683–1692. [Google Scholar] [CrossRef]
- Chen, J.; Zhou, C.; Wu, B.; Wang, Y.; Li, Q.; Wei, Y.; Yang, D.; Mu, J.; Zhu, D.; Zou, D. Left versus right repetitive transcranial magnetic stimulation in treating major depression: A meta-analysis of randomised controlled trials. Psychiatry Res. 2013, 210, 1260–1264. [Google Scholar] [CrossRef]
- Nierenberg, A.A.; Katz, J.; Fava, M. A critical overview of the pharmacologic management of treatment-resistant depression. Psychiatr. Clin. N. Am. 2007, 30, 13–29. [Google Scholar] [CrossRef] [PubMed]
- McPherson, S.; Cairns, P.; Carlyle, J.; Shapiro, D.; Richardson, P.; Taylor, D. The effectiveness of psychological treatments for treatment-resistant depression: A systematic review. Acta Psychiatr. Scand. 2005, 111, 331–340. [Google Scholar] [CrossRef]
- Schatzberg, A.F.; Demitrack, M.A.; O’Reardon, J.P.; Richelson, M.; Thase, M.E. Transcranial magnetic stimulation: Potential new treatment for resistant depression. J. Clin. Psychiatry 2007, 68. Available online: https://www.psychiatrist.com/wp-content/uploads/2021/02/18249_transcranial-magnetic-stimulation-potential-treatment.pdf (accessed on 17 June 2021).
- Glen, S. Cohen’s Kappa Statistic [WWW Document]. Stat. How To. Available online: https://www.statisticshowto.com/cohens-kappa-statistic/ (accessed on 10 December 2020).
- Pham, M.T.; Rajić, A.; Greig, J.D.; Sargeant, J.M.; Papadopoulos, A.; McEwen, S.A. A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res. Synth. Methods 2014, 5, 371–385. [Google Scholar] [CrossRef] [PubMed]
- Theleritis, C.; Sakkas, P.; Paparrigopoulos, T.; Vitoratou, S.; Tzavara, C.; Bonaccorso, S.; Politis, A.; Soldatos, C.R.; Psarros, C. Two Versus One High-Frequency Repetitive Transcranial Magnetic Stimulation Session per Day for Treatment-Resistant Depression: A Randomized Sham-Controlled Trial. J. ECT 2017, 33, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, B.C.; Aaronson, S.T.; Clarke, G.N.; Holtzheimer, P.E.; Johnson, C.W.; McDonald, W.M.; Schneider, M.B.; Carpenter, L.L. Neurocognitive Effects of Repetitive Transcranial Magnetic Stimulation with a 2-Coil Device in Treatment-Resistant Major Depressive Disorder. J. ECT 2018, 34, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, L.L.; Aaronson, S.T.; Clarke, G.N.; Holtzheimer, P.E.; Johnson, C.W.; McDonald, W.M.; Stannard, E.L.; Schneider, M.B. rTMS with a two-coil array: Safety and efficacy for treatment resistant major depressive disorder. Brain Stimul. 2017, 10, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Iwabuchi, S.; Auer, D.; Lankappa, S.; Palaniyappan, L. Baseline effective connectivity predicts response to repetitive transcranial magnetic stimulation in patients with treatment-resistant depression. Eur. Neuropsychopharmacol. 2019, 29, 681–690. [Google Scholar] [CrossRef] [PubMed]
- van Eijndhoven, P.; Bartholomeus, J.; Möbius, M.; De Bruijn, A.; Ferrari, G.; Mulders, P.; Schene, A.; Schutter, D.; Spijker, J.; Tendolkar, I. A randomized controlled trial of a standard 4-week protocol of repetitive transcranial magnetic stimulation in severe treatment resistant depression. J. Affect. Disord. 2020, 274, 444–449. [Google Scholar] [CrossRef]
- Filipčić, I.; Šimunović Filipčić, I.; Sučić, S.; Milovac, Ž.; Gereš, N.; Matić, K.; Čelić-Ružić, M.; Zečević Penić, S.; Orgulan, I.; Požgaj, V. A pilot investigation of accelerated deep transcranial magnetic stimulation protocols in treatment-resistant depression. Eur. Arch. Psychiatry Clin. Neurosci. 2021, 271, 49–59. [Google Scholar] [CrossRef]
- Benadhira, R.; Thomas, F.; Bouaziz, N.; Braha, S.; Andrianisaina, P.S.-K.; Isaac, C.; Moulier, V.; Januel, D. A randomized, sham-controlled study of maintenance rTMS for treatment-resistant depression (TRD). Psychiatry Res. 2017, 258, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Fairchild, J.K.; Mi, Z.; Biswas, K.; Davis-Karim, A.; Phibbs, C.S.; Forman, S.D.; Thase, M.; Williams, L.M.; Etkin, A. Effect of repetitive transcranial magnetic stimulation on treatment-resistant major depression in US veterans: A randomized clinical trial. JAMA Psychiatry 2018, 75, 884–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kito, S.; Miyazi, M.; Nakatani, H.; Matsuda, Y.; Yamazaki, R.; Okamoto, T.; Igarashi, Y. Effectiveness of high-frequency left prefrontal repetitive transcranial magnetic stimulation in patients with treatment-resistant depression: A randomized clinical trial of 37.5-minute vs 18.75-minute protocol. Neuropsychopharmacol. Rep. 2019, 39, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, A.; Bhat, J.; Cardenas, V.; Ehrlich, T.; Horwege, A.; Mathalon, D.; Roach, B.; Glover, G.; Badran, B.; Forman, S. Targeting location relates to treatment response in active but not sham rTMS stimulation. Brain Stimul. 2021, 14, 703–709. [Google Scholar] [CrossRef] [PubMed]
- Roach, A.E.; Hines, C.; Stafford, J.; Mooney, S. Repetitive transcranial magnetic stimulation for treatment-resistant depression in active-duty service members improves depressive symptoms. J. ECT 2020, 36, 279. [Google Scholar] [CrossRef] [PubMed]
- Croarkin, P.E.; Elmaadawi, A.Z.; Aaronson, S.T.; Schrodt, G.R.; Holbert, R.C.; Verdoliva, S.; Heart, K.L.; Demitrack, M.A.; Strawn, J.R. Left prefrontal transcranial magnetic stimulation for treatment-resistant depression in adolescents: A double-blind, randomized, sham-controlled trial. Neuropsychopharmacology 2021, 46, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Trevizol, A.P.; Goldberger, K.W.; Mulsant, B.H.; Rajji, T.K.; Downar, J.; Daskalakis, Z.J.; Blumberger, D.M. Unilateral and bilateral repetitive transcranial magnetic stimulation for treatment-resistant late-life depression. Int. J. Geriatr. Psychiatry 2019, 34, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Barbini, B.; Attanasio, F.; Manfredi, E.; Cavallini, M.C.; Zanardi, R.; Colombo, C. Bright light therapy accelerates the antidepressant effect of repetitive transcranial magnetic stimulation in treatment resistant depression: A pilot study. Int. J. Psychiatry Clin. Pract. 2021, 25, 375–377. [Google Scholar] [CrossRef]
- Zhao, X.; Li, Y.; Tian, Q.; Zhu, B.; Zhao, Z. Repetitive transcranial magnetic stimulation increases serum brain-derived neurotrophic factor and decreases interleukin-1β and tumor necrosis factor-α in elderly patients with refractory depression. J. Int. Med. Res. 2019, 47, 1848–1855. [Google Scholar] [CrossRef]
- Philip, N.S.; Dunner, D.L.; Dowd, S.M.; Aaronson, S.T.; Brock, D.G.; Carpenter, L.L.; Demitrack, M.A.; Hovav, S.; Janicak, P.G.; George, M.S. Can medication free, treatment-resistant, depressed patients who initially respond to TMS be maintained off medications? A prospective, 12-month multisite randomized pilot study. Brain Stimul. 2016, 9, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Maes, M.; Song, C.; Yirmiya, R. Targeting IL-1 in depression. Expert Opin. Ther. Targets 2012, 16, 1097–1112. [Google Scholar] [CrossRef]
- Karson, A.; Demirtaş, T.; Bayramgürler, D.; Balcı, F.; Utkan, T. Chronic Administration of Infliximab (TNF-α Inhibitor) decreases depression and anxiety-like behaviour in rat model of chronic mild stress. Basic Clin. Pharmacol. Toxicol. 2013, 112, 335–340. [Google Scholar] [CrossRef]
- Qin, T.; Fang, F.; Song, M.; Li, R.; Ma, Z.; Ma, S. Umbelliferone reverses depression-like behavior in chronic unpredictable mild stress-induced rats by attenuating neuronal apoptosis via regulating ROCK/Akt pathway. Behav. Brain Res. 2017, 317, 147–156. [Google Scholar] [CrossRef]
- Molendijk, M.L.; Bus, B.A.; Spinhoven, P.; Penninx, B.W.; Kenis, G.; Prickaerts, J.; Voshaar, R.; Elzinga, B. Serum levels of brain-derived neurotrophic factor in major depressive disorder: State–trait issues, clinical features and pharmacological treatment. Mol. Psychiatry 2011, 16, 1088–1095. [Google Scholar] [CrossRef] [Green Version]
- Ebmeier, K.P.; Donaghey, C.; Steele, J.D. Recent developments and current controversies in depression. Lancet 2006, 367, 153–167. [Google Scholar] [CrossRef]
- Sartorius, N. The economic and social burden of depression. J. Clin. Psychiatry 2001, 62, 8–11. [Google Scholar] [PubMed]
- Lopez, A.D.; Mathers, C.D.; Ezzati, M.; Jamison, D.T.; Murray, C.J. Global and regional burden of disease and risk factors, 2001: Systematic analysis of population health data. Lancet 2006, 367, 1747–1757. [Google Scholar] [CrossRef]
- Hernández-Ribas, R.; Deus, J.; Pujol, J.; Segalàs, C.; Vallejo, J.; Menchón, J.M.; Cardoner, N.; Soriano-Mas, C. Identifying brain imaging correlates of clinical response to repetitive transcranial magnetic stimulation (rTMS) in major depression. Brain Stimul. 2013, 6, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Wiegand, R.; Kharraz, A.; Landgrebe, M.; Marienhagen, J.; Frick, U.; Hajak, G.; Eichhammer, P. Pre-treatment anterior cingulate activity as a predictor of antidepressant response to repetitive transcranial magnetic stimulation (rTMS). Neuroendocrinol. Lett. 2007, 28, 633–638. [Google Scholar]
- Arnsten, A.F.; Rubia, K. Neurobiological circuits regulating attention, cognitive control, motivation, and emotion: Disruptions in neurodevelopmental psychiatric disorders. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 356–367. [Google Scholar] [CrossRef]
- Pascual-Leone, A.; Rubio, B.; Pallardó, F.; Catalá, M.D. Rapid-rate transcranial magnetic stimulation of left dorsolateral prefrontal cortex in drug-resistant depression. Lancet 1996, 348, 233–237. [Google Scholar] [CrossRef]
- Fitzgerald, P.B.; Benitez, J.; de Castella, A.; Daskalakis, Z.J.; Brown, T.L.; Kulkarni, J. A randomized, controlled trial of sequential bilateral repetitive transcranial magnetic stimulation for treatment-resistant depression. Am. J. Psychiatry 2006, 163, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Kedzior, K.K.; Rajput, V.; Price, G.; Lee, J.; Martin-Iverson, M. Cognitive correlates of repetitive transcranial magnetic stimulation (rTMS) in treatment-resistant depression-a pilot study. BMC Psychiatry 2012, 12, 163. [Google Scholar]
- Schönfeldt-Lecuona, C.; Cardenas-Morales, L.; Freudenmann, R.; Kammer, T.; Herwig, U. Transcranial magnetic stimulation in depression–lessons from the multicentre trials. Restor. Neurol. Neurosci. 2010, 28, 569–576. [Google Scholar] [CrossRef] [Green Version]
- Valero-Cabré, A.; Payne, B.R.; Pascual-Leone, A. Opposite impact on 14C-2-deoxyglucose brain metabolism following patterns of high and low frequency repetitive transcranial magnetic stimulation in the posterior parietal cortex. Exp. Brain Res. 2007, 176, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Tarhan, N.; Sayar, F.G.H.; Tan, O.; Kağan, G. Efficacy of high-frequency repetitive transcranial magnetic stimulation in treatment-resistant depression. Clin. EEG Neurosci. 2012, 43, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Croarkin, P.E.; Wall, C.A.; King, J.D.; Kozel, F.A.; Daskalakis, Z.J. Pain during transcranial magnetic stimulation in youth. Innov. Clin. Neurosci. 2011, 8, 18. [Google Scholar]
- Segev, A.; Spellun, J.; Bloch, Y. Anxiety as a central outcome measure in an adolescent with major depressive disorder treated with repetitive transcranial magnetic stimulation. J. ECT 2014, 30, e54–e55. [Google Scholar] [CrossRef] [PubMed]
- Wall, C.A.; Croarkin, P.E.; Maroney-Smith, M.J.; Haugen, L.M.; Baruth, J.M.; Frye, M.A.; Sampson, S.M.; Port, J.D. Magnetic resonance imaging-guided, open-label, high-frequency repetitive transcranial magnetic stimulation for adolescents with major depressive disorder. J. Child Adolesc. Psychopharmacol. 2016, 26, 582–589. [Google Scholar] [CrossRef]
- Wall, C.A.; Croarkin, P.E.; Sim, L.A.; Husain, M.M.; Janicak, P.G.; Kozel, F.A.; Emslie, G.J.; Dowd, S.M.; Sampson, S.M. Adjunctive use of repetitive transcranial magnetic stimulation in depressed adolescents: A prospective, open pilot study. J. Clin. Psychiatry 2011, 72, 487. [Google Scholar] [CrossRef]
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.; Vos, T.; Whiteford, H.A. Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.J.; Tor, P.C.; Khoo, A.L.; Teng, M.; Lim, B.P.; Mok, Y.M. Cost-effectiveness modeling of repetitive transcranial magnetic stimulation compared to electroconvulsive therapy for treatment-resistant depression in Singapore. Neuromodulation Technol. Neural Interface 2018, 21, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Kozel, F.A.; George, M.S.; Simpson, K.N. Decision analysis of the cost-effectiveness of repetitive transcranial magnetic stimulation versus electroconvulsive therapy for treatment of nonpsychotic severe depression. CNS Spectr. 2004, 9, 476–482. [Google Scholar] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adu, M.K.; Shalaby, R.; Chue, P.; Agyapong, V.I.O. Repetitive Transcranial Magnetic Stimulation for the Treatment of Resistant Depression: A Scoping Review. Behav. Sci. 2022, 12, 195. https://doi.org/10.3390/bs12060195
Adu MK, Shalaby R, Chue P, Agyapong VIO. Repetitive Transcranial Magnetic Stimulation for the Treatment of Resistant Depression: A Scoping Review. Behavioral Sciences. 2022; 12(6):195. https://doi.org/10.3390/bs12060195
Chicago/Turabian StyleAdu, Medard Kofi, Reham Shalaby, Pierre Chue, and Vincent I. O. Agyapong. 2022. "Repetitive Transcranial Magnetic Stimulation for the Treatment of Resistant Depression: A Scoping Review" Behavioral Sciences 12, no. 6: 195. https://doi.org/10.3390/bs12060195
APA StyleAdu, M. K., Shalaby, R., Chue, P., & Agyapong, V. I. O. (2022). Repetitive Transcranial Magnetic Stimulation for the Treatment of Resistant Depression: A Scoping Review. Behavioral Sciences, 12(6), 195. https://doi.org/10.3390/bs12060195