
Anxiety and Sleep Quality Amelioration in College Students: A Comparative Study between Team Sports and Individual Sports


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Methodology
2.3. Test Main Results
2.4. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
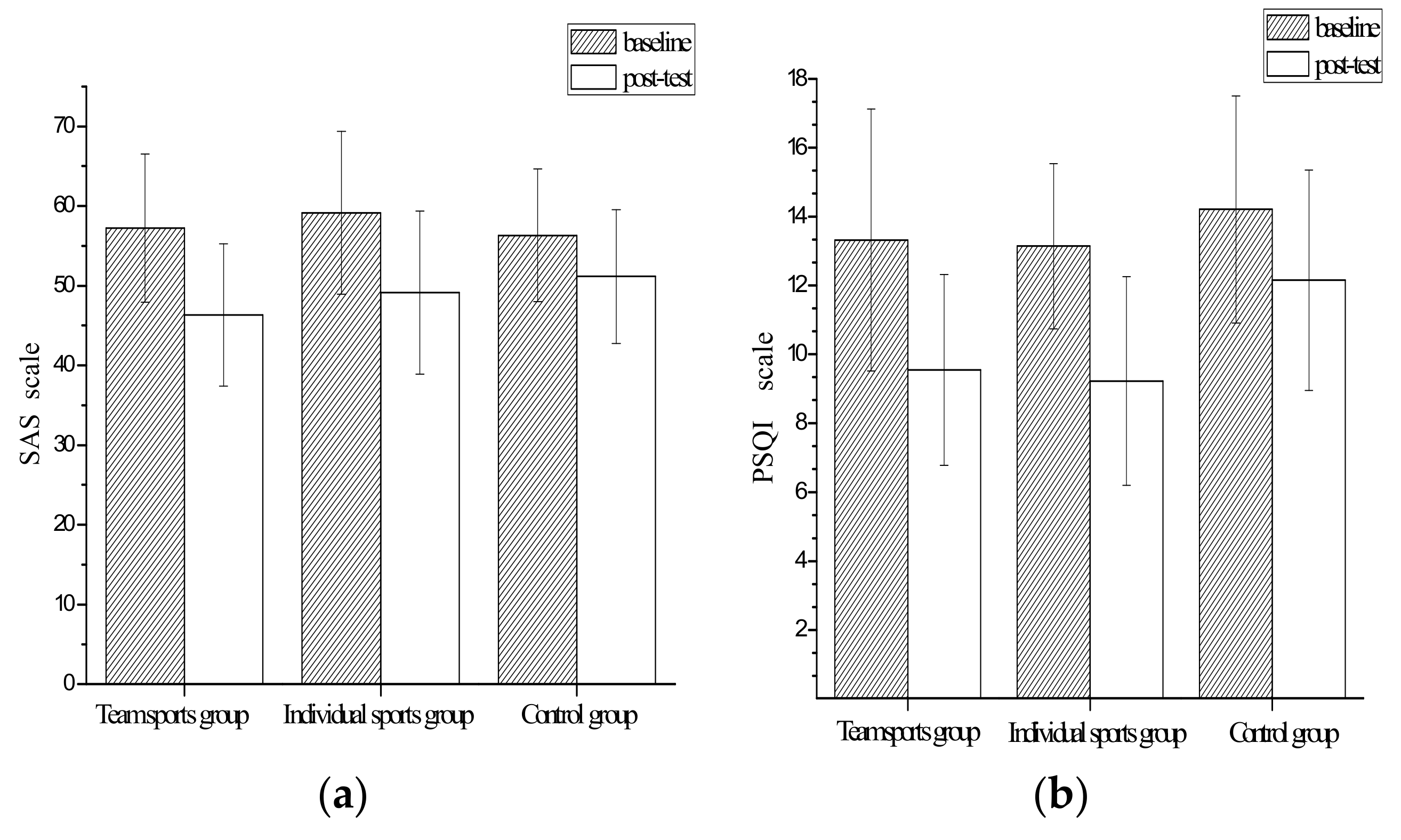
3.2. The Relief of Anxiety and the Improvement of Sleep Quality in College Students after 6 Weeks’ Intervention
3.3. Comparison of Anxiety Symptom Relief Effect and Sleep Quality Improvement Effect among College Students
3.4. Build and Revise Models
3.5. Summary
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takil, N.B.; Sari, B.A. Trait anxiety vs. career anxiety in relation to attentional control. Curr. Psychol. 2021, 40, 2366–2370. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Pine, D.S.; Holmes, E.A.; Reif, A. Anxiety disorders. Lancet 2021, 397, 914–927. [Google Scholar] [CrossRef]
- Forbes, E.J.; Byrne, G.J.; O’Sullivan, J.D.; Yang, J.; Marsh, R.; Dissanayaka, N.N. Defining atypical anxiety in parkinson’s disease. Mov. Disord. Clin. Pract. 2021, 8, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Roseman, A.; Morton, L.; Kovacs, A.H. Health anxiety among adults with congenital heart disease. Curr. Opin. Cardiol. 2021, 36, 98–104. [Google Scholar] [CrossRef]
- Henning, M.; Subic-Wrana, C.; Wiltink, J.; Beutel, M. Anxiety disorders in patients with somatic diseases. Psychosom. Med. 2020, 82, 287–295. [Google Scholar] [CrossRef]
- Mustata, A.E. The relationships between coping mechanisms, depression, anxiety and sleep disorders in cardiovascular patients. J. Evid. Based Psychother. 2021, 21, 37–55. [Google Scholar] [CrossRef]
- Dutcher, C.D.; Dowd, S.M.; Zalta, A.K.; Taylor, D.J.; Rosenfield, D.; Perrone, A.; Otto, M.W.; Pollack, M.H.; Hofmann, S.G.; Smits, J.A.J. Sleep quality and outcome of exposure therapy in adults with social anxiety disorder. Depress. Anxiety 2021, 38, 1182–1190. [Google Scholar] [CrossRef]
- Knowles, K.A.; Olatunji, B.O. Specificity of trait anxiety in anxiety and depression: Meta-analysis of the state-trait anxiety inventory. Clin. Psychol. Rev. 2020, 82, 101928. [Google Scholar] [CrossRef]
- Simon, E.K.; Berki, Z.H.K.; Gettys, G.C.; Vedak, C. Sleep problems and disorders in patients with anxiety disorders. Psychiatr. Ann. 2016, 46, 396–400. [Google Scholar] [CrossRef]
- Palmer, C.A.; Alfano, C.A. Anxiety modifies the emotional effects of sleep loss. Curr. Opin. Psychol. 2020, 34, 100–104. [Google Scholar] [CrossRef]
- Ng, H.T.H.; Zhang, C.; Phipps, D.; Zhang, R.; Hamilton, K. Effects of anxiety and sleep on academic engagement among university students. Aust. Psychol. 2022, 57, 57–64. [Google Scholar] [CrossRef]
- Gorman, J.M. Treating generalized anxiety disorder. J. Clin. Psychiatr. 2003, 642, 24–29. [Google Scholar]
- Green, S.M.; Donegan, E.; McCabe, R.E.; Streiner, D.L.; Agako, A.; Frey, B.N. Cognitive behavioral therapy for perinatal anxiety: A randomized controlled trial. Aust. N. Z. J. Psychiatr. 2020, 54, 423–432. [Google Scholar] [CrossRef]
- Philippot, A.; Dubois, V.; Lambrechts, K.; Grogna, D.; Robert, A.; Jonckheer, U.; Chakib, W.; Beine, A.; Bleyenheuft, Y.; De Volder, A.G. Impact of physical exercise on depression and anxiety in adolescent inpatients: A randomized controlled trial. J. Affect. Disord. 2022, 301, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Ji, C.; Yang, J.; Lin, L.; Chen, S. Physical exercise ameliorates anxiety, depression and sleep quality in college students: Experimental evidence from exercise intensity and frequency. Behav. Sci. 2022, 12, 61. [Google Scholar] [CrossRef] [PubMed]
- Plekhanova, T.; Rowlands, A.V.; Davies, M.; Edwardson, C.L.; Hall, A.; Yates, T. Effect of exercise on sleep and bi-directional associations with accelerometer-assessed physical activity in men with obesity. Appl. Physiol. Nutr. Metab. 2021, 46, 597–605. [Google Scholar] [CrossRef]
- Saidi, O.; Colin, E.; Rance, M.; Dore, E.; Pereira, B.; Duche, P. Effect of morning versus evening exercise training on sleep, physical activity, fitness, fatigue and quality of life in overweight and obese adults. Chronobiol. Int. 2021, 38, 1537–1548. [Google Scholar] [CrossRef]
- Borrego, C.C.; Cid, L.; Silva, C. Relationship between group cohesion and anxiety in soccer. J. Hum. Kinet. 2012, 34, 121–129. [Google Scholar]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. Resistance exercise training among young adults with analogue generalized anxiety disorder. J. Affect. Disord. 2021, 281, 153–159. [Google Scholar] [CrossRef]
- Axelsdottir, B.; Biedilae, S.; Sagatun, A.; Nordheim, L.V.; Larun, L. Review: Exercise for depression in children and adolescents—A systematic review and meta-analysis. Child Adolesc. Ment. Health 2021, 26, 347–356. [Google Scholar] [CrossRef]
- Bellon, J.A.; Conejo-Ceron, S.; Sanchez-Calderon, A.; Rodriguez-Martin, B.; Bellon, D.; Rodriguez-Sanchez, E.; Mendive, J.M.; Ara, I.; Moreno-Peral, P. Effectiveness of exercise-based interventions in reducing depressive symptoms in people without clinical depression: Systematic review and meta-analysis of randomised controlled trials. Brit. J. Psychiatr. 2021, 219, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Tang, L.; Dishman, R.K. The effects of a single session of mindful exercise on anxiety: A systematic review and meta-analysis. Ment. Health Phys. Act. 2021, 21, 100403. [Google Scholar] [CrossRef]
- Yang, W.; Zhai, F.; Gao, Y.; Zhang, Q. Collective rehabilitation training conductive to improve psychotherapy of college students with anxiety disorder. Int. J. Clin. Exp. Med. 2015, 8, 9949–9954. [Google Scholar]
- Strickland, M.G.; Anastasio, P. Co-rumination may mitigate depressive and anxious symptoms for those high in social interaction anxiety. J. Soc. Clin. Psychol. 2021, 40, 381–403. [Google Scholar] [CrossRef]
- Akungu, O.A.; Chien, K.; Chen, S. The longitudinal interaction of adolescents’ interest in physical education, school burnout, and disturbed sleep related to social media and phone use. Curr. Psychol. 2021, 1–9. [Google Scholar] [CrossRef]
- Wallace, M.L.; McMakin, D.L.; Tan, P.Z.; Rosen, D.; Forbes, E.E.; Ladouceur, C.D.; Ryan, N.D.; Siegle, G.J.; Dahl, R.E.; Kendall, P.C.; et al. The role of day-to-day emotions, sleep, and social interactions in pediatric anxiety treatment. Behav. Res. Ther. 2017, 90, 87–95. [Google Scholar] [CrossRef] [Green Version]
- Pluhar, E.; McCracken, C.; Griffith, K.L.; Christino, M.A.; Sugimoto, D.; Meehan, W.P.I. Team sport athletes may be less likely to suffer anxiety or depression than individual sport athletes. J. Sport Sci. Med. 2019, 18, 490–496. [Google Scholar]
- Baker, J.; Yardley, J.; Cote, J. Coach behaviors and athlete satisfaction in team and individual sports. Int. J. Sport Psychol. 2003, 34, 226–239. [Google Scholar]
- Dunstan, D.A.; Scott, N. Norms for zung’s self-rating anxiety scale. BMC Psychiatry 2020, 20, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Chen, Y.H. Analysis of the effect of clinical application of detailed nursing measures in ensuring the safety of nursing in operating room. Indian J. Pharm. Sci. 2021, 83, 174–179. [Google Scholar] [CrossRef]
- Shi, C.; Guo, Y.; Ma, H.; Zhang, M. Psychometric validation of the 14-item perceived stress scale in chinese medical residents. Curr. Psychol. 2019, 38, 1428–1434. [Google Scholar] [CrossRef]
- Smyth, C. The pittsburgh sleep quality index (psqi). Am. J. Nurs. 2008, 108, 47–48. [Google Scholar]
- Han, Q.; Liu, B.; Lin, S.; Li, J.; Liang, P.; Fu, S.; Zheng, G.; Yang, S.; Li, B.; Yang, Q. Pittsburgh sleep quality index score predicts all-cause mortality in chinese dialysis patients. Int. Urol. Nephrol. 2021, 53, 2369–2376. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Tian, Y.; Yu, J.; Chen, T.; An, F. Effect of at-home cognitive behavior therapy combined with nursing on revised piper fatigue scale, pittsburgh sleep quality index, self-rating anxiety scale and self-rating depression scale of ovarian cancer patients after chemotherapy. Int. J. Clin. Exp. Med. 2020, 13, 4227–4234. [Google Scholar]
- Frederiksen, K.P.; Stavestrand, S.H.; Venemyr, S.K.; Sirevag, K.; Hovland, A. Physical exercise as an add-on treatment to cognitive behavioural therapy for anxiety: A systematic review. Behav. Cogn. Psychother. 2021, 49, 626–640. [Google Scholar] [CrossRef]
- Murphy, J.; Patte, K.A.; Sullivan, P.; Leatherdale, S.T. Exploring the association between sport participation and symptoms of anxiety and depression in a sample of canadian high school students. J. Clin. Sport Psychol. 2021, 15, 268–287. [Google Scholar] [CrossRef]
- Johnston, S.A.; Roskowski, C.; He, Z.; Kong, L.; Chen, W. Effects of team sports on anxiety, depression, perceived stress, and sleep quality in college students. J. Am. Coll. Health 2021, 69, 791–797. [Google Scholar] [CrossRef]
- Jurado-Fasoli, L.; De-la-O, A.; Molina-Hidalgo, C.; Migueles, J.H.; Castillo, M.J.; Amaro-Gahete, F.J. Exercise training improves sleep quality: A randomized controlled trial. Eur. J. Clin. Investig. 2020, 50, e13202. [Google Scholar] [CrossRef]
- Lazaridou, A.; Koulouris, A.; Devine, J.K.; Haack, M.; Jamison, R.N.; Edwards, R.R.; Schreiber, K.L. Impact of daily yoga-based exercise on pain, catastrophizing, and sleep amongst individuals with fibromyalgia. J. Pain Res. 2019, 12, 2915–2923. [Google Scholar] [CrossRef] [Green Version]
- Gumus Sekerci, Y.; Kir Bicer, E. The effect of walking exercise on quality of life and sleep in elderly individuals: Randomized controlled study. Turk. J. Geriatr. 2019, 22, 443–453. [Google Scholar]
- Seol, J.; Park, I.; Kokudo, C.; Zhang, S.; Suzuki, C.; Yajima, K.; Satoh, M.; Tokuyama, K.; Okura, T. Distinct effects of low-intensity physical activity in the evening on sleep quality in older women: A comparison of exercise and housework. Exp. Gerontol. 2021, 143, 111165. [Google Scholar] [CrossRef] [PubMed]
- Rosa, C.C.; Tebar, W.R.; Soares Oliveira, C.B.; Farah, B.Q.; Casonatto, J.; Ciccotti Saraiva, B.T.; Destro Christofaro, D.G. Effect of different sports practice on sleep quality and quality of life in children and adolescents: Randomized clinical trial. Sports Med. Open 2021, 7, 83. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Team Sports Group | Individual Sports Group | Control Group | p-Value | |||
|---|---|---|---|---|---|---|---|
| Mean [SD] or n (%) | n | Mean [SD] or n (%) | n | Mean [SD] or n (%) | n | ||
| Age (years) | 21.42 [2.4] | 66 | 22.31 [3.1] | 64 | 21.90 [2.1] | 67 | 0.87 |
| Male/Female | 35/31 (53.0/47.0) | 66 | 39/25 (60.9/39.1) | 64 | 41/26(61.2/38.8) | 67 | 0.57 |
| BMI (kg/m2) | 27.43 [5.5] | 66 | 27.82 [4.9] | 64 | 27.50 [5.0] | 67 | 0.79 |
| Body fat rate | 29.43 [5.2] | 66 | 30.22 [6.3] | 64 | 28.91 [4.9] | 67 | 0.66 |
| Smoking | 9 (13.6) | 66 | 6 (9.4) | 64 | 11 (16.4) | 67 | 0.43 |
| Year with anxiety (<1 year) | 57 (86.4) | 66 | 59 (7.8) | 64 | 55 (82.1) | 67 | 0.42 |
| 1–2 years | 8 (12.1) | 66 | 5 (33.3) | 64 | 12 (17.9) | 67 | 0.32 |
| >2 years | 1 (1.5) | 66 | 0 (0.0) | 64 | 0(0.0) | 67 | 0.43 |
| insomnia | 40 (60.6) | 66 | 42 (65.6) | 64 | 45 (67.2) | 67 | 0.49 |
| Physical exercise (occasions/week) | 0.71 [1.2] | 66 | 0.80 [0.9] | 64 | 0.52 [1.1] | 67 | 0.57 |
| Physical exercise (min/week) | 32.43 [17.3] | 66 | 43.18 [13.5] | 64 | 40.42 [18.3] | 67 | 0.60 |
| Social interaction (occasions/week) | 0.31 [0.53] | 66 | 0.46 [0.67] | 64 | 0.25 [0.72] | 67 | 0.49 |
| Rating scale scores PSQI | 14.32 [3.8] | 66 | 13.14 [2.4] | 64 | 14.21 [3.3] | 67 | 0.32 |
| Rating scale scores SAS | 57.23 [9.3] | 66 | 59.14 [10.2] | 64 | 56.32 [8.3] | 67 | 0.63 |
| Team Sports Group | Individual Sports Group | Control Group | |
|---|---|---|---|
| SAS scores | |||
| All, n | 66 | 64 | 67 |
| Improvement, n (%) a | 46 (69.7) | 38 (59.4) | 26 (38.8) |
| No improvement, n (%) | 20 (30.3) | 26 (40.6) | 41 (61.2) |
| PSQI scores | |||
| All, n | 66 | 64 | 67 |
| Improvement, n (%) b | 52 (78.8) | 50 (78.1) | 19 (28.4) |
| No improvement, n (%) | 14 (21.2) | 14 (21.9) | 48 (71.6) |
| Change in SAS Scores | Effect Size (95% CI) | p-Value | |
|---|---|---|---|
| Model 1 a | |||
| Control vs. Individual sports (n = 131) | 11.32 (5.32–17.46) | 0.006 | |
| Control vs. Team sports (n = 133) | 12.28 (5.78–18.65) | 0.002 | |
| Model 2 b | |||
| Control vs. Individual sports (n = 131) | 12.99 (6.03–18.90) | 0.001 | |
| Control vs. Team sports (n = 133) | 13.68 (6.27–19.11) | 0.001 | |
| Change in PSQI scores | |||
| Model 1 a | |||
| Control vs. Individual sports (n = 131) | 5.13 (1.21–8.79) | 0.005 | |
| Control vs. Team sports (n = 133) | 5.35 (1.36–9.21) | 0.002 | |
| Model 2 b | |||
| Control vs. Individual sports (n = 131) | 5.86 (2.17–9.78) | 0.002 | |
| Control vs. Team sports (n = 133) | 6.32 (2.89–10.32) | 0.000 | |
| Model 1 a | Model 2 b | Model 3 c | Model 4 d | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | p (n) | OR (95% CI) | p (n) | OR (95% CI) | p (n) | OR (95% CI) | p (n) | |
| SAS scores | ||||||||
| Individual sports | 2.64 (2.17–9.78) | 0.02 (197) | 2.86 (2.32–10.21) | 0.01 (197) | 3.05 (2.68–10.78) | 0.03 (197) | 3.18 (2.87–11.21) | 0.01 (197) |
| Team sports | 4.05 (3.05–12.03) | 0.01 (197) | 4.49 (3.67–13.85) | 0.005 (197) | 4.89 (3.96–14.11) | 0.01 (197) | 4.99 (4.06–14.87) | 0.003 (197) |
| Compared | 1.78 (2.26–9.93) | 0.01 (197) | 2.04 (2.69–10.80) | 0.004 (197) | 2.79 (2.97–11.84) | 0.013 (197) | 2.90 (2.99–12.00) | 0.003 (197) |
| PSQI scores | ||||||||
| Individual sports | 5.78 (4.32–17.03) | 0.006 (197) | 6.32 (4.89–17.87) | 0.01 (197) | 6.98 (5.02–17.95) | 0.01 (197) | 7.32 (5.35–18.22) | 0.005 (197) |
| Team sports | 5.96 (4.49–18.42) | 0.002 (197) | 6.78 (5.76–19.13) | 0.005 (197) | 7.09 (6.16–19.66) | 0.004 (197) | 7.98 (6.69–19.98) | 0.003 (197) |
| Compared | 5.73 (4.29–16.32) | 0.41 (197) | 5.94 (4.94–17.12) | 0.30 (197) | 6.05 (5.01–17.79) | 0.33 (197) | 6.96 (6.19–18.02) | 0.21 (197) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ji, C.; Yang, J.; Lin, L.; Chen, S. Anxiety and Sleep Quality Amelioration in College Students: A Comparative Study between Team Sports and Individual Sports. Behav. Sci. 2022, 12, 149. https://doi.org/10.3390/bs12050149
Ji C, Yang J, Lin L, Chen S. Anxiety and Sleep Quality Amelioration in College Students: A Comparative Study between Team Sports and Individual Sports. Behavioral Sciences. 2022; 12(5):149. https://doi.org/10.3390/bs12050149
Chicago/Turabian StyleJi, Chaoxin, Jun Yang, Lin Lin, and Song Chen. 2022. "Anxiety and Sleep Quality Amelioration in College Students: A Comparative Study between Team Sports and Individual Sports" Behavioral Sciences 12, no. 5: 149. https://doi.org/10.3390/bs12050149
APA StyleJi, C., Yang, J., Lin, L., & Chen, S. (2022). Anxiety and Sleep Quality Amelioration in College Students: A Comparative Study between Team Sports and Individual Sports. Behavioral Sciences, 12(5), 149. https://doi.org/10.3390/bs12050149