
Eating Disorders and Disordered Eating in Competitive Cycling: A Scoping Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Methodological Rationale
2.2. Stage 1: Identifying the Research Question
2.3. Stage 2: Identifying Relevant Studies
- Key search terms for all databases:
- “Disordered eating” “cyclists” “competitive cycling”
- “Eating disorders” “cyclists” “competitive cycling”
- “Eating patterns” “cyclists” “competitive cycling”
- “Eating attitudes” “cyclists” “competitive cycling”
- “Nutrition habits” “cyclists” “competitive cycling”
- “Race weight” “cyclists” “competitive cycling”
- “leanness” “cyclists” “competitive cycling”
- “Eating disorders” “anorexia” “bulimia” “disordered eating” “cyclists” “competitive cycling”
- Inclusion criteria were:
- Articles written in English;
- Peer-reviewed articles;
- Articles that include specific reference to Eating Disorders and/or Disorder Eating in competitive cycling;
- Articles related to the areas above with the addition of eating patterns, attitudes and nutrition habits in competitive cycling;
- Articles with any reference to race weight and leanness;
- Articles related to any of the above in any competitive cycling setting.
- Exclusion criteria were:
- If dietary or nutrient intake were measured with no reference to disordered eating patterns or eating disorders;
- Articles not published;
- Articles without full-text access;
- Grey literature;
- Articles not written in English.
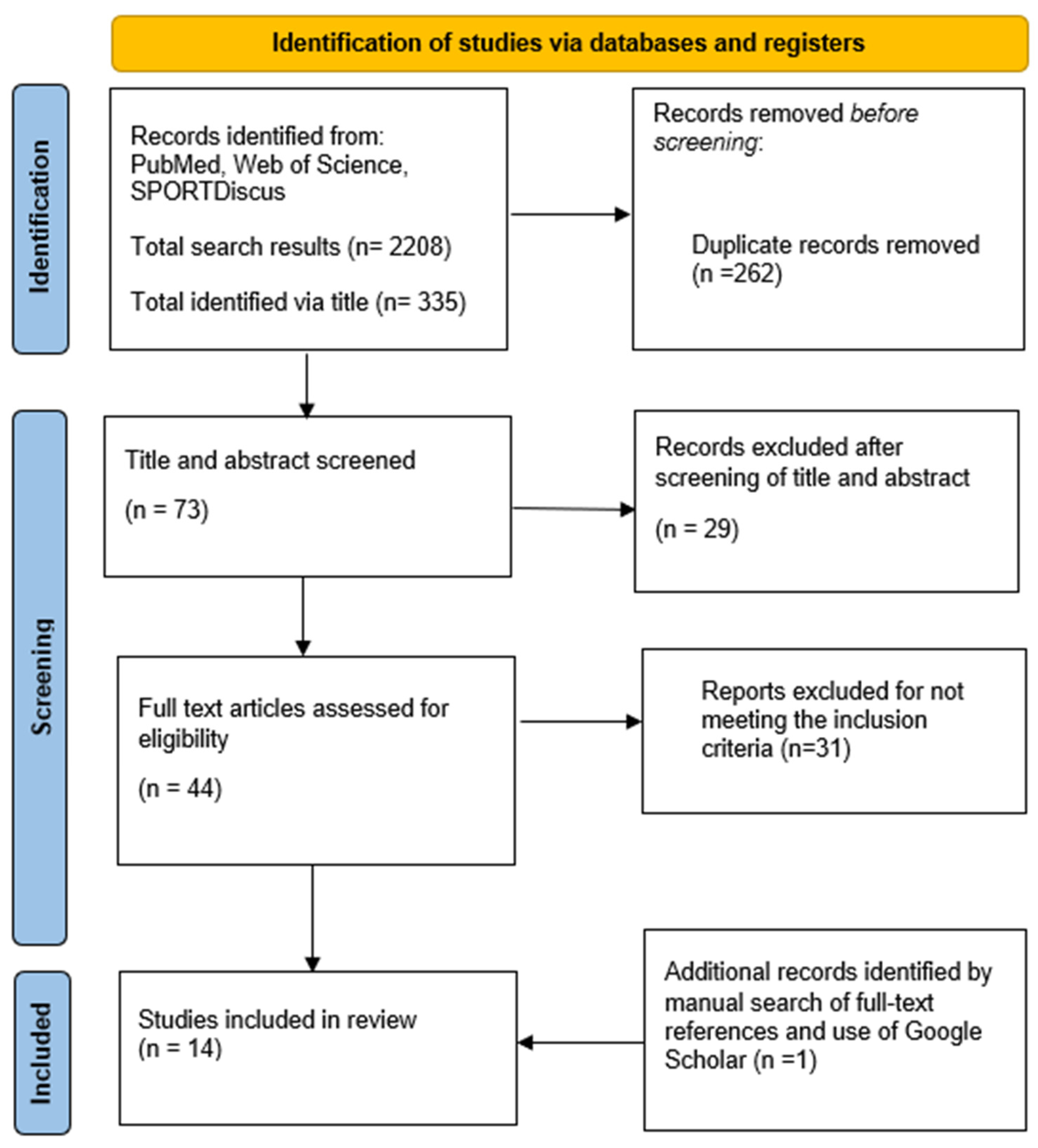
2.4. Stage 3: Study Selection
2.5. Stage 4: Charting the Data
2.6. Stage 5: Collating, Summarising and Reporting the Results
3. Findings and Discussion
3.1. Cycling as an ‘at-Risk’ Sport
3.2. Power to Weight Ratio
3.3. Energy Requirements and Low Energy Availability
3.4. The Social Environment of Competitive Cycling
3.5. Nutrition Support
3.6. Relationship between Eating Disorders/Disordered Eating and Exercise Addiction
3.7. Recommendations from Identified Literature
4. Conclusions and Recommendations

{kind=link}
| Year Location | Sample Number (Sex) | Age (Years) | Body Mass | Height | Discipline | Level | Reported Cycling Hours | Study Aims | Study Design | Measurement Instrument | Findings Relevant to Scoping Review | Reported Limitations in Paper |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ferrand and Brunet 2004 [41] France | 42 (M) | 21.8 ± 3.7 | Only BMI reported. 20.5 ± 1.4 kg/m2 | Not reported | Not reported | Amateur classified as Regional (n = 12), National (n = 13) and elite (n = 17) | Not reported | To examine the associations between dimensions of perfectionism and eating disorder symptoms among 42 young male amateur cyclists (M = 21.8 yr., SD = 3.7) over the three performance categories (Elite, National, Regional). | Cross-sectional self-reported survey | Eating Attitudes Test (EAT-26); Multidimensional Perfectionism Scale |
|
|
| Riebl et al., 2007 [58] USA | 124 (61 cyclists and 63 non cyclists as control) (M) | 31.6 ± 10.4 (cyclists) and 23 ± 6.3 (control) | 72.5 ± 7.6 (cyclists) and 80.5 ± 16.1 kg (control) | Not reported | Not reported | Not reported | Inclusion criteria included training a minimum of 5 h on a bicycle each week throughout the year; have participated in cycling for no less than 1 year. | To determine the prevalence of subclinical disordered eating behaviours among male cyclists, whether male cyclists self-report having an eating disorder, and whether male cyclists meet the daily recommendations for the major food groups according to the Dietary Guidelines for Americans. | Cross-sectional self-reported survey | The Eating Attitudes Test-26 (EAT-26) (7–9), Survey of Eating Disorders Among Cyclists (SEDAC) (10), and a nutrition questionnaire were completed by the study participants. |
|
|
| Gorrell et al., 2019 [55] USA | 612 mixed sport (24 cyclists) (M) | 18–26 (M = 20.99) | Not reported | Not reported | Not reported | Not reported. Sample from National College Athletics Association (NCAA) schools | Not reported | To characterise unhealthy exercise and eating behaviour according to competitive athlete status, as well as per sport type. | Cross-sectional self-reported survey | Eating disorder examination questionnaire EDE-Q |
|
|
| Muros et al., 2020 [12] Spain | 4037 cyclists and triathletes (cyclists = 2037) (F and M) | 37.72 ± 9.67 | Only BMI reported 23.74 ± 2.69 kg/m2 | Not reported | Not reported | Not reported. Federated cyclists in Spain | 10.94 ± 4.64 | To describe and predict eating disorders according to sex, body mass index, age and sport discipline within a sample of athletes. | Cross-sectional self-reported survey | The revised restraint scale (RRS); the five-item SCOFF; the Mediterranean diet (MD) adherence screener (MEDAS) |
|
|
| Filaire et al., 2007 [40] France | 15 cyclists (44 full sample) (M) | 21.2 ± 2.8 | 68.0 ± 6.5 kg | 180 ± 0.06 cm | Road cycling | National | Weekly distance covered ranged between 600 and 750 km. The athletes took part in races each weekend, with distance ranging from 100 to 150 km. | To test the hypothesis that male athletes who feel pressured to maintain a specific body weight present an elevated risk of subclinical eating disorders. | Cross-sectional self-reported survey | Eating Attitudes Test (EAT-26); Multidimensional Perfectionism Scale; Body Esteem Scale; Profile of Mood States |
|
|
| Yates et al., 2003 [60] Not reported | 190 (36 cyclists) (F and M) | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | To differentiate groups of highly conditioned, competitive athletes on the basis of Exercise Orientation Questionnaire (EOQ) scores and self-reported psychiatric symptoms. | Cross-sectional self-reported survey | Exercise Orientation Questionnaire (EOQ) |
|
|
| Haakonssen et al., 2015 [25] Australia | 37 (F) | 18–36 | 58.4 ± 5.9 kg | 170 ± 7 cm | Road cycling | Professional and amateur | Not reported | To investigate the satisfaction of elite female cyclists with their body weight (BW) in the context of race performance, the magnitude of BW manipulation, and the association of these variables with menstrual function. | Cross-sectional self-reported survey | Female Cyclist Weight Management Questionnaire (Created by research team) |
|
|
| Hoon et al., 2019 [24] Australia | 97 (M) | 32.0 ± 1.7 | 73.1 ± 1.4 kg | 180.4 ± 1.0 cm | Road, Track and Mountain Bike | Participants were categorized as Local, National (i.e., top domestic competition) or International level | 13.9 ± 0.8 h | To investigate the perceptions and practices of achieving ‘race weight’ in a population of trained male cyclists. A secondary focus was to investigate the use of gym-based strength training, a possible attenuator of the side effects associated with weight reduction. | Cross-sectional self-reported survey | Survey created by research team |
|
|
| Sousa Fortes et al., 2017 [57] Brazil | 43 | Risk of ED: 21.33 ± 1.84 No risk of ED: 21.49 ± 1.75 | Not reported | Not reported | Road cycling | Not reported | Risk of ED: 10.23 ± 1.12 No risk of ED: 10.26 ± 1.07 per week | The aim of this study was to compare the maximum oxygen consumption (VO2max) between road cyclists with and without risk for eating disorders. | Cross-sectional self-reported survey | Eating Attitudes Test 26 (EAT-26) |
|
|
| Hale and Divin [61] 2011 USA | 98 (M) | 34 ± 4.1 | Not reported | Not reported | Not reported | Amateur to professional | Not reported | To examine eating behaviours in competitive male cyclists across racing categories. | Cross-sectional self-reported survey | Eating Attitudes Test 26 (EAT-26) |
|
|
| Viner et al., 2015 [35] USA | 10 (F and M) | Male: 42.0 ± 7.7 Female: 38.4 ± 10.3 | Male: 72.4 ± 6.8 kg Female: 62.8 ± 12.2 kg | Male: 177.9 ± 4.2 cm Female: 165.4 ± 6.4 cm | Road cycling and mountain biking | Competitive | Male: 1.4 ± 0.6 Female: 0.8 ± 0.4 per day | To analyse eating behaviours that may contribute to LEA. | Cross-sectional self-reported survey | The Three-Factor Eating Questionnaire (TFEQ)—participants who scored 10 or higher were considered restrained eaters (RE) who consciously limit EI as a means of weight control |
|
|
| de Bruin and Oudejans 2018 [39] Netherlands | 8 mixed sport (1 cyclist) (F) | Not reported | Not reported | Not reported | Not reported | International | Not reported | To explore the role of contextual body image in the development of EDs in female athletes participating in at-risk sports. | Qualitative | Interview |
|
|
| Cook and Dobbin 2022 [36] UK | 36 (M) | 23.1 ± 3.9 (18–30) | 70.4 ± 7.1 kg | 180.5 ± 6.1 cm | Road cycling | Elite (n = 8), category 1 (n = 9), category 2 (n = 19) | 16.4 ± 3.2 (10–22) per week | To assess the association between sports nutrition knowledge, nutrition intake, energy availability and training characteristics with the risk of an eating disorder amongst highly trained, competitive male cyclists. | Cross-sectional self-reported survey | The Brief Eating Disorder in Athletes Questionnaire (BEDA-Q) |
|
|
| Cook and Luke 2017 [56] USA | 179 (F and M) | 32.5 ± 12.9 | Not reported | Not reported | Not reported | High school to professional | Not reported | To establish prevalence rates for primary and secondary EXD in a sample of cyclists. Our secondary purpose was to examine potential differences in EXD and level of competition, competition history and exercise amount. | Cross-sectional self-reported survey | Drive for Thinness subscale of the Eating Disorder Inventory-2 |
|
|
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Himmerich, H.; Treasure, J. Psychopharmacological advances in eating disorders. Expert Rev. Clin. Pharmacol. 2018, 11, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.Y.; Yin, W.Q.; Sun, H.W.; Yang, S.X.; Li, X.Y.; Liu, H.Q. The association between disordered eating and health-related quality of life among children and adolescents: A systematic review of population-based studies. PLoS ONE 2019, 14, e0222777. [Google Scholar] [CrossRef] [PubMed]
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M.P. Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. Am. J. Clin. Nutr. 2019, 109, 1402–1413. [Google Scholar] [CrossRef]
- McArdle, S.; Meade, M.M.; Moore, P. Exploring attitudes toward eating disorders among elite athlete support personnel. Scand. J. Med. Sci. Sport. 2016, 26, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Erskine, H.E.; Whiteford, H.A.; Pike, K.M. The global burden of eating disorders. Curr. Opin. Psychiatry 2016, 29, 346–353. [Google Scholar] [CrossRef]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. American College of Sports Medicine Joint Position Statement. Nutrition and Athletic Performance. Med. Sci. Sport. Exerc. 2016, 48, 543–568. [Google Scholar]
- Wells, K.R.; Jeacocke, N.A.; Appaneal, R.; Smith, H.D.; Vlahovich, N.; Burke, L.M.; Hughes, D. The Australian Institute of Sport (AIS) and National Eating Disorders Collaboration (NEDC) position statement on disordered eating in high performance sport. Br. J. Sport. Med. 2020, 54, 1247–1258. [Google Scholar] [CrossRef]
- Reardon, C.L.; Hainline, B.; Aron, C.M.; Baron, D.; Baum, A.L.; Bindra, A.; Budgett, R.; Campriani, N.; Castaldelli-Maia, J.M.; Currie, A.; et al. Mental health in elite athletes: International Olympic Committee consensus statement (2019). Br. J. Sport. Med. 2019, 53, 667–699. [Google Scholar] [CrossRef]
- Bratland-Sanda, S.; Sundgot-Borgen, J. Eating disorders in athletes: Overview of prevalence, risk factors and recommendations for prevention and treatment. Eur. J. Sport Sci. 2013, 13, 499–508. [Google Scholar] [CrossRef]
- Doley, J.R.; Hart, L.M.; Stukas, A.A.; Petrovic, K.; Bouguettaya, A.; Paxton, S.J. Interventions to reduce the stigma of eating disorders: A systematic review and meta-analysis. Int. J. Eat. Disord. 2017, 50, 210–230. [Google Scholar] [CrossRef]
- Phillips, K.E.; Hopkins, W.G. Determinants of Cycling Performance: A Review of the Dimensions and Features Regulating Performance in Elite Cycling Competitions. Sport. Med. Open 2020, 6, 23. [Google Scholar] [CrossRef] [PubMed]
- Muros, J.J.; Ávila-Alche, Á.; Knox, E.; Zabala, M. Likelihood of suffering from an eating disorder in a sample of Spanish cyclists and triathletes. J. Eat. Disord. 2020, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Krosshaug, T.; Bahr, R. Overuse injuries in professional road cyclists. Am. J. Sport. Med. 2010, 38, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Olaso-Gonzalez, G.; Corella, D.; Gomez-Cabrera, M.C.; Vina, J. Increased average longevity among the Tour de France cyclists. Int. J. Sport. Med. 2011, 32, 644–647. [Google Scholar] [CrossRef] [PubMed]
- Wasserfurth, P.; Palmowski, J.; Hahn, A.; Krüger, K. Reasons for and Consequences of Low Energy Availability in Female and Male Athletes: Social Environment, Adaptations, and Prevention. Sport. Med. Open 2020, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Schofield, K.L.; Thorpe, H.; Sims, S.T. Where are all the men? Low energy availability in male cyclists: A review. Eur. J. Sport Sci. 2021, 21, 1567–1578. [Google Scholar] [CrossRef] [PubMed]
- Keay, N.; Francis, G.; Entwistle, I.; Hind, K. Clinical evaluation of education relating to nutrition and skeletal loading in competitive male road cyclists at risk of relative energy deficiency in sports (RED-S): 6-month randomised controlled trial. BMJ Open Sport Exerc. Med. 2019, 5, e000523. [Google Scholar] [CrossRef]
- Cycling Weekly. Cycling and Eating Disorders: My Relationship with Body Weight and the Bicycle. 2022. Available online: https://www.cyclingnews.com/features/cycling-and-eating-disorders-my-relationship-with-body-weight-and-the-bicycle/ (accessed on 22 September 2022).
- Cycling Weekly. Sports Dietician Says Eating Disorders in Cycling Are Becoming a Serious Problem. 2020. Available online: https://www.cyclingweekly.com/news/latest-news/sports-dietician-says-eating-disorders-cycling-becoming-serious-problem-445709 (accessed on 22 September 2022).
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef]
- Marí-Sanchis, A.; Burgos-Balmaseda, J.; Hidalgo-Borrajo, R. Eating disorders in sport. Update and proposal for an integrated approach. Endocrinol. Diabetes Nutr. 2022, 69, 131–143. [Google Scholar] [CrossRef]
- Atkinson, G.; Davison, R.; Jeukendrup, A.; Passfield, L. Science and cycling: Current knowledge and future directions for research. J. Sport. Sci. 2003, 21, 767–787. [Google Scholar] [CrossRef] [PubMed]
- Hoon, M.W.; Haakonssen, E.C.; Menaspà, P.; Burke, L.M. Racing weight and resistance training: Perceptions and practices in trained male cyclists. Physician Sportsmed. 2019, 47, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Haakonssen, E.C.; Martin, D.T.; Jenkins, D.G.; Burke, L.M. Race weight: Perceptions of elite female road cyclists. Int. J. Sport. Physiol. Perform 2015, 10, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Mountjoy, M.; Sundgot-Borgen, J.; Burke, L.; Ackerman, K.E.; Blauwet, C.; Constantini, N.; Lebrun, C.; Lundy, B.; Melin, A.; Meyer, N.; et al. International Olympic Committee (IOC) Consensus statement on relative energy deficiency in sport (red-s): 2018 update. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 316–331. [Google Scholar] [CrossRef] [PubMed]
- Hilton, L.K.; Loucks, A.B. Low energy availability, not exercise stress, suppresses the diurnal rhythm of leptin in healthy young women. Am. J. Physiol. Endocrinol. Metab. 2000, 278, E43–E49. [Google Scholar] [CrossRef]
- Melin, A.; Tornberg, B.; Skouby, S.; Møller, S.S.; Sundgot-Borgen, J.; Faber, J.; Sidelmann, J.J.; Aziz, M.; Sjödin, A. Energy availability and the female athlete triad in elite endurance athletes. Scand. J. Med. Sci. Sport. 2015, 25, 610–622. [Google Scholar] [CrossRef] [PubMed]
- Logue, D.M.; Madigan, S.M.; Melin, A.; Delahunt, E.; Heinen, M.; Mc Donnell, S.-J.; Corish, C.A. Low energy availability in athletes 2020: An updated narrative review of prevalence, risk, within-day energy balance, knowledge, and impact on sports performance. Nutrients 2020, 12, 835. [Google Scholar] [CrossRef]
- Heaney, S.; O’Connor, H.; Naughton, G.; Gifford, J. Towards an Understanding of the Barriers to Good Nutrition for Elite Athletes. Int. J. Sport. Sci. Coach 2008, 3, 391–401. [Google Scholar] [CrossRef]
- Hutson, M.J.; O’Donnell, E.; Brooke-Wavell, K.; Sale, C.; Blagrove, R.C. Effects of Low Energy Availability on Bone Health in Endurance Athletes and High-Impact Exercise as A Potential Countermeasure: A Narrative Review. Sport. Med. 2021, 51, 391–403. [Google Scholar] [CrossRef]
- Martin, D.; Papageorgiou, M.; Colgan, M.H.; Bandelow, S.; Greeves, J.; Tang, J.C.Y.; Fraser, W.; Cooper, S.B.; Sale, C.; Elliott-Sale, K.J. The effects of short-term low energy availability, achieved through diet or exercise, on cognitive function in oral contraceptive users and eumenorrheic women. Appl. Physiol. Nutr. Metab. 2021, 46, 781–789. [Google Scholar] [CrossRef]
- Koehler, K.; Hoerner, N.R.; Gibbs, J.C.; Zinner, C.; Braun, H.; De Souza, M.J.; Schaenzer, W. Low energy availability in exercising men is associated with reduced leptin and insulin but not with changes in other metabolic hormones. J. Sport. Sci. 2016, 34, 1921–1929. [Google Scholar] [CrossRef] [PubMed]
- Park, H.K.; Ahima, R.S. Physiology of leptin: Energy homeostasis, neuroendocrine function and metabolism. Metab. Clin. Exp. 2015, 64, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Viner, R.T.; Harris, M.; Berning, J.R.; Meyer, N.L. Energy availability and dietary patterns of adult male and female competitive cyclists with lower than expected bone mineral density. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Cook, O.; Dobbin, N. The association between sport nutrition knowledge, nutritional intake, energy availability, and training characteristics with the risk of an eating disorder amongst highly trained competitive road cyclists. Sport Sci. Health 2022, 18, 1243–1251. [Google Scholar] [CrossRef]
- Jagim, A.R.; Fields, J.; Magee, M.K.; Kerksick, C.M.; Jones, M.T. Contributing Factors to Low Energy Availability in Female Athletes: A Narrative Review of Energy Availability, Training Demands, Nutrition Barriers, Body Image, and Disordered Eating. Nutrients 2022, 14, 986. [Google Scholar] [CrossRef]
- Sundgot-Borgen, J.; Torstveit, M.K. Aspects of disordered eating continuum in elite high-intensity sports. Scand. J. Med. Sci. Sport 2010, 20, 112–121. [Google Scholar] [CrossRef]
- de Bruin, A.K.; Oudejans, R.R. Athletes’ body talk: The role of contextual body image in eating disorders as seen through the eyes of elite women athletes. J. Clin. Sport Psychol. 2018, 12, 675–698. [Google Scholar] [CrossRef]
- Filaire, E.; Rouveix, M.; Pannafieux, C.; Ferrand, C. Eating attitudes, perfectionism and body-esteem of elite male judoists and cyclists. J. Sport. Sci. Med. 2007, 6, 50. [Google Scholar]
- Ferrand, C.; Brunet, E. Perfectionism and risk for disordered eating among young French male cyclists of high performance. Percept. Mot. Ski. 2004, 99, 959–967. [Google Scholar] [CrossRef]
- Eck, K.; Byrd-Bredbenner, C. Food choice decisions of collegiate division I athletes: A qualitative exploratory study. Nutrients 2021, 13, 2322. [Google Scholar] [CrossRef]
- Spronk, I.; Kullen, C.; Burdon, C.; O’Connor, H. Relationship between nutrition knowledge and dietary intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [PubMed]
- Birkenhead, K.L.; Slater, G. A review of factors influencing athletes’ food choices. Sport. Med. 2015, 45, 1511–1522. [Google Scholar] [CrossRef] [PubMed]
- Soh, N.L.-W.; Touyz, S.W.; Dobbins, T.A.; Surgenor, L.J.; Clarke, S.; Kohn, M.R.; Lee, E.L.; Leow, V.; Rieger, E.; Ung, K.E.K.; et al. Nutrition knowledge in young women with eating disorders in Australia and Singapore: A pilot study. Aust. N. Z. J. Psychiatry 2009, 43, 1178–1184. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, N.E.; Hecht, L.M.; Haedt-Matt, A.A. Nutrition knowledge moderates the association between perfectionism and shape/weight concerns. Eur. J. Clin. Nutr. 2021, 75, 1433–1439. [Google Scholar] [CrossRef]
- Godoy-Izquierdo, D.; Ramírez, M.J.; Díaz, I.; López-Mora, C. A systematic review on exercise addiction and the disordered eating-eating disorders continuum in the competitive sport context. Int. J. Ment. Health Addict. 2021. [Google Scholar] [CrossRef]
- Lavender, J.M.; De Young, K.P.; Wonderlich, S.A.; Crosby, R.D.; Engel, S.G.; Mitchell, J.E.; Crow, S.J.; Peterson, C.B.; Le Grange, D. Daily patterns of anxiety in anorexia nervosa: Associations with eating disorder behaviors in the natural environment. J. Abnorm. Psychol. 2013, 122, 672. [Google Scholar] [CrossRef]
- Trott, M.; Jackson, S.E.; Firth, J.; Jacob, L.; Grabovac, I.; Mistry, A.; Stubbs, B.; Smith, L. A comparative meta-analysis of the prevalence of exercise addiction in adults with and without indicated eating disorders. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 37–46. [Google Scholar] [CrossRef]
- The Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2022.
- Potenza, M.N. Non-substance addictive behaviors in the context of DSM-5. Addict. Behav. 2014, 39, 1–2. [Google Scholar] [CrossRef]
- Lichtenstein, M.B.; Hinze, C.J.; Emborg, B.; Thomsen, F.; Hemmingsen, S.D. Compulsive exercise: Links, risks and challenges faced. Psychol. Res. Behav. Manag. 2017, 10, 85. [Google Scholar] [CrossRef]
- Hausenblas, H.A.; Symons Downs, D. Exercise Dependence Scale-21 Manual; University of Florida: Gainesville, FL, USA, 2002. [Google Scholar]
- Berg, K.C.; Peterson, C.B.; Frazier, P.; Crow, S.J. Psychometric evaluation of the eating disorder examination and eating disorder examination-questionnaire: A systematic review of the literature. Int. J. Eat. Disord. 2012, 45, 428–438. [Google Scholar] [CrossRef]
- Gorrell, S.; Nagata, J.M.; Hill, K.B.; Carlson, J.L.; Shain, A.F.; Wilson, J.; Timko, C.A.; Hardy, K.K.; Lock, J.; Peebles, R. Eating behavior and reasons for exercise among competitive collegiate male athletes. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2021, 26, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Cook, B.; Luke, R. Primary and secondary exercise dependence in a sample of cyclists. Int. J. Ment. Health Addict. 2017, 15, 444–451. [Google Scholar] [CrossRef]
- Fortes, L.; Mendonça, L.C.V.; Paes, P.P.; Vianna, J.M.; Diefenthaeler, F. Can power and anaerobic capacity reduce according to disordered eating behaviors in cyclists? Mot. Rev. Educ. Física 2017, 23, 60–64. [Google Scholar] [CrossRef][Green Version]
- Riebl, S.K.; Subudhi, A.W.; Broker, J.P.; Schenck, K.; Berning, J.R. The prevalence of subclinical eating disorders among male cyclists. J. Am. Diet. Assoc. 2007, 107, 1214–1217. [Google Scholar] [CrossRef] [PubMed]
- Sundgot-Borgen, J.; Torstveit, M.K. Prevalence of eating disorders in elite athletes is higher than in the general population. Clin. J. Sport Med. 2004, 14, 25–32. [Google Scholar] [CrossRef]
- Yates, A.; Edman, J.D.; Crago, M.; Crowell, D. Eating disorder symptoms in runners, cyclists, and paddlers. Addict. Behav. 2007, 28, 1473–1480. [Google Scholar] [CrossRef]
- Hale, W.; Divin, A. Examining Eating Behaviors in Competitive Male Cyclists across Racing Categories. Med. Sci. Sport Exerc. 2011, 43, 942. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roberts, C.J.; Hurst, H.T.; Hardwicke, J. Eating Disorders and Disordered Eating in Competitive Cycling: A Scoping Review. Behav. Sci. 2022, 12, 490. https://doi.org/10.3390/bs12120490
Roberts CJ, Hurst HT, Hardwicke J. Eating Disorders and Disordered Eating in Competitive Cycling: A Scoping Review. Behavioral Sciences. 2022; 12(12):490. https://doi.org/10.3390/bs12120490
Chicago/Turabian StyleRoberts, Charlie Jon, Howard Thomas Hurst, and Jack Hardwicke. 2022. "Eating Disorders and Disordered Eating in Competitive Cycling: A Scoping Review" Behavioral Sciences 12, no. 12: 490. https://doi.org/10.3390/bs12120490
APA StyleRoberts, C. J., Hurst, H. T., & Hardwicke, J. (2022). Eating Disorders and Disordered Eating in Competitive Cycling: A Scoping Review. Behavioral Sciences, 12(12), 490. https://doi.org/10.3390/bs12120490