1. Introduction
Burnout was originally defined as “the extinction of motivation or incentive, especially where one’s devotion to a cause or relationship fails to produce the desired results” [
1,
2]. The term burnout was first used by Californian poverty lawyers to describe peers who exhibited signs of gradual cynicism and emotional exhaustion [
3]. Around the same time, Maslach, a social psychologist, focused on stressors among workers in human services and how they coped with such stressors [
3,
4]. Later on, Maslach and colleagues conceptualized burnout along three dimensions: emotional exhaustion, depersonalization, and personal accomplishment [
4].
Employment is generally perceived as an essential element of the overall well-being of an individual. In developed countries, burnout syndrome (BOS) is ranked next to cardiovascular disease and diabetes in prevalence [
5,
6]. America’s Physicians Practice Patterns Perspectives reported that 78% of physicians had BOS in 2018. This was a 4% increase since 2016. The British Medical Association survey in 2019 demonstrated that 80% of doctors were suffering from BOS [
7]. Moreover, BOS often begins when workers have unrealistic expectations of themselves, others, and their career development [
8,
9,
10]. The failure to meet these expectations leads to maladaptive coping strategies, which subsequently results in chronic job stress and, eventually, burnout [
8,
9,
11]. Although it is challenging to classify the symptoms of BOS precisely, the BOS symptoms can be categorized into physical, affective, cognitive, behavioral, and motivational components [
12].
Burnout is commonly observed in individuals who work with people, particularly in educators at all levels and healthcare workers, whose careers are characterized by high levels of work-related stress [
11]. Burnout is a global concern with deleterious effects on an individual’s psychological and physical health and on an organization as a whole [
13]. Understanding the factors that contribute to burnout is essential for creating a healthy and productive workplace.
Clinician faculty educators are at significant risk of burnout, since many are practicing clinicians and researchers expected to handle the pressures associated with multiple roles simultaneously [
14].
Educators have been particularly prone to burnout and well-studied in a variety of educators, including elementary [
15,
16], middle school [
17,
18], high school [
15], and university teachers [
18,
19]. The prevalence of burnout amongst physicians has been extensively researched [
20,
21]. When physicians take the educator role (i.e., academic physicians), this might put them at a higher risk of burnout [
22]. Administrative duties—including the Electronic Health Record (EHR)—with insufficient documentation time have been linked to BOS in academic clinicians [
23]. In a study done on academic physicians, only 3% of the physicians reported administration work to be meaningful [
20]. Thus, the present study hypothesized three main sources of burnout among academic clinicians, which are: interactions with patients, trainees, and/or administration.
The current study aims to measure the prevalence of burnout within the Faculty of Health Sciences at McMaster University—a tertiary academic referral health center in Ontario, Canada. The study also aims to investigate potential demographic and workload variables that contribute to self-reported measures of burnout.
We hypothesize that administrative interaction serves as a main source of burnout compared to interaction with trainees and patients.
2. Methods
A Research Ethics Board (REB) approval (13-800) was obtained prior to the study commencement for the study protocol, survey, recruitment email, and poster. The participants’ personal information was not reported in any of the findings. Data for this study were collected from February to July, 2014.
2.1. Study Population
The survey was completed by 326 clinical academic faculty members in clinical specialties working at McMaster University in the departments of Medicine, Critical Care, Surgery, Family Medicine, Obstetrics, and Gynecology, Pediatrics, Anesthesia, Psychiatry, Emergency Medical Oncology, Radiology, and Pathology (
Table 1). The total population surveyed was approximately 900, while our sample that responded was 326. The survey response rate was 36.2%. The highest response rate was in Surgery (60%) and lowest in Medicine (38%).
The specialties were further polarized into two main categories: surgically focused specialties (Surgery, Obstetrics, and Gynecology and Anesthesia), which represented 35%, and non-surgically focused specialties (Medicine, Critical Care, Family Medicine, Pediatrics, Psychiatry, Emergency Medicine, Pathology, Radiology, and Medical/Radiation Oncology), representing 65%. The study population was further categorized based on their academic rank, their highest level of education, living status, gender, and marital status (
Table 1).
2.2. Instrument Used for the Survey
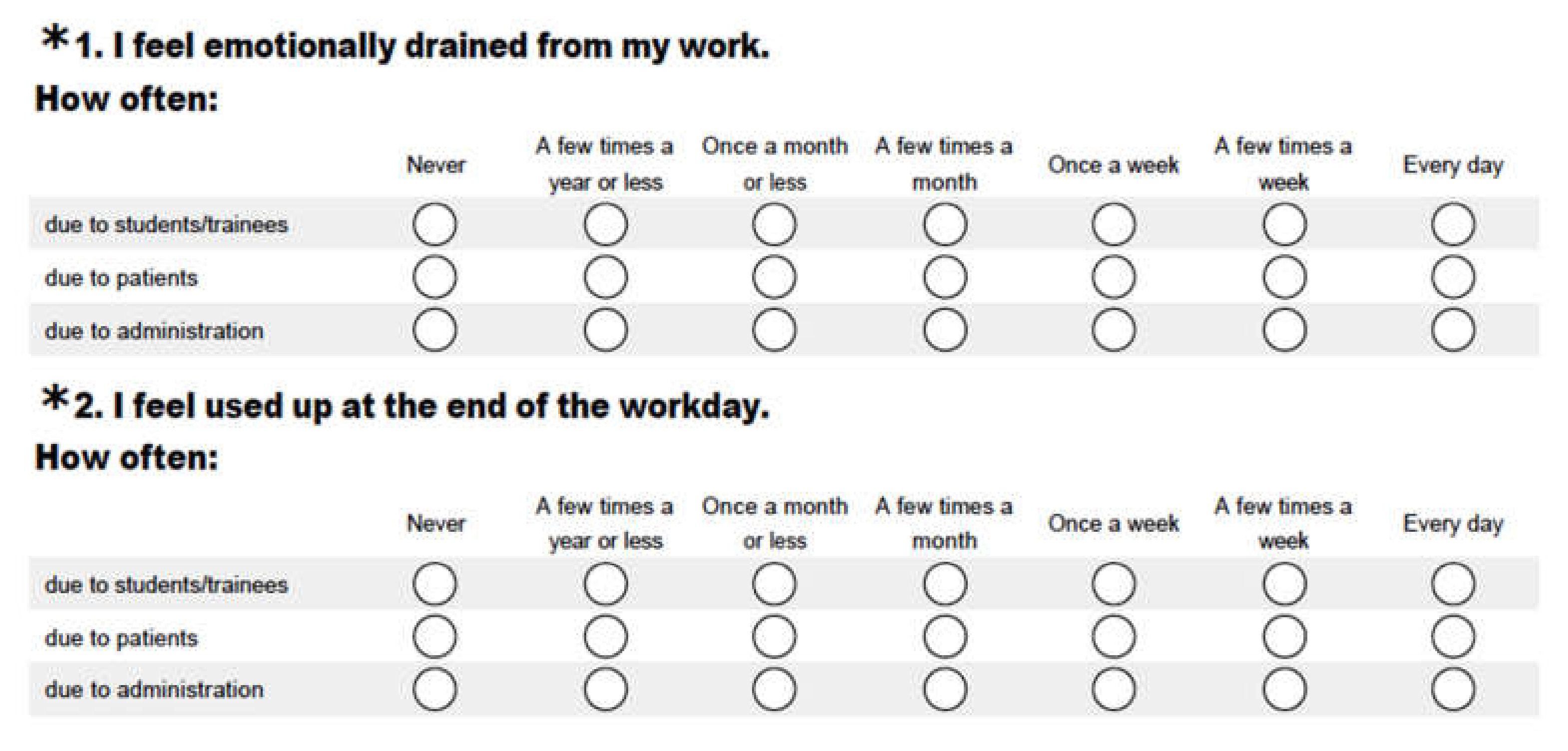
The Maslach Burnout Inventory (MBI) was used for measuring burnout among academic healthcare providers (
Table 2). The original version of MBI consisted of 22 items, each composed of a seven-point rating scale indicating the frequency of such an experience. To fit the goal of the study, an innovative MBI scale modification was performed with permission from the publisher (Mind Garden
®). The modification of the scale included the three hypothesized categories of burnout—trainees, patients, and administration—within the same modified version on the same scale administered at the same setting (
Figure 1).
2.3. Data Collection
Survey Monkey®, a web-based survey platform, was used for data collection. The survey link was distributed to participants via email by their corresponding department chairs.
Statistical Analysis
A statistical analysis was performed using SPSS Statistical Software 22, (IBM, Chicago, Illinois, USA). All statistical tests were two-tailed, and p-values < 0.05 were considered statistically significant. An exploratory factor analysis was used to investigate the construct validity for the modified scale of the three sources of interactions (trainees, patients, or administration) to each of the 22 items of the scale. A multiple regression analysis was carried out to examine the contribution of each of the study variables and how these variables explained the variance of the burnout scores.
These variables included age, gender, marital status, living situation, total years of work experience as faculty, majority of practice community vs. academic, academic rank, specialty, level of higher education achieved, number of night/shifts call per month, average number of patients, patient load per month, number of active research projects the physicians were currently involved in, nature of work, and whether the job was full-time or part-time.
3. Results
3.1. Psychometric Properties of MBI: Psychometric Properties of the Scale Were Tested to Ensure That Our Modified Scale Bore the Same Dimensionality as That of the Original Unmodified MBI Scale
3.1.1. Construct Validity Index
A principal axis factoring with Varimax rotation was used to investigate the dimensionality of MBI according to the population of the study and to give an index of construct validity (see
Appendix A Table A1,
Table A2 and
Table A3). The factor retention criteria were (1) Eigenvalues greater than 1, (2) evidence from the screen plots, and (3) factor loadings greater than 0.30. A separate factor analysis was conducted for all three categories of responses: due to trainees, due to patients, and due to administration. The three prerequisites for principal axis factoring that the study met were:
The determinant analysis was larger than zero for all responses, which were deemed significant.
Kaiser–Meyer–Olkin (KMO) of sampling adequacy: KMO for the category due to students was 0.92, due to patients was 0.92, and due to administration was 0.91.
Bartlett’s test for sphericity was significant for the three responses (p < 0.001).
The extracted sum squared loading indicated what percentage of the variance in an original variable was explained by a factor (
Table 3).
3.1.2. Reliability (Internal Consistency)
Nine internal consistencies (Cronbach’s alpha) indexes were calculated and are presented in
Table 4. The results indicated that the reliability of the modified scale ranged between 0.86–0.97 (good–excellent) across the three types of human interactions.
3.1.3. Burnout Prevalence
To estimate the prevalence of burnout among the academic clinicians, the burnout percentages for the three types of interaction categories (interactions with trainees, with patients, and with administration) were calculated and are presented in
Table 5. Academic clinicians reported higher levels of burnout due to interactions with administration relative to that caused by patients and trainees in both emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA) (percentages are interpreted in reverse to the other two subscales). The mean squares with standard deviation for the three types of interaction categories were calculated and are presented in
Table 6.
3.2. Variables Contributing to Burnout
A regression analysis was used to determine the contributing variables for burnout syndrome. Thirteen variables were included as predictors for burnout: age, gender, marital status, living situation, years of work experience, practice type (community vs. academic), academic rank, specialty, education achieved, number of work hours/month, patient load per month, number of active research projects, and full or part-time practice.
To satisfy the requirement of multiple regressions, categorical and ordinal data variables were converted to dummy variables of two values: 0 and 1. The sample size variable ratio was calculated to be 25, which is acceptable for a regression analysis.
The following variables were converted to dummy variables:
Marital status: single and separated were coded as 0 and married as 1.
Specialty: surgical specialties (Surgery, OBGYN, and Anesthesia) were coded as 0, while non-surgical specialties (Medicine, Critical Care, Family Medicine, Pediatrics, Psychiatry, Emergency Medicine, and Medical Oncology) were coded as 1.
Academic rank: professor and associate professor were coded as 0; while assistant professor, associate clinical professor, assistant clinical professor, and clinical scholar were coded as 1.
Living situation: alone was 0, while living with others was 1.
Educational level: postgraduate education, Ph.D., MBA, Masters, and diploma was coded as 0, while no postgraduate degree was coded as 1.
Multiple regressions with stepwise methods in entering the predictor (independent) variable were used. The results are summarized in
Table A4,
Table A5 and
Table A6 (see
Appendix A).
3.2.1. Emotional Exhaustion Dimension of Burnout
Multiple regression was used to compare three sources of EE (burnout due to trainees, burnout due to patients, and burnout due to administration) according to the contribution of the 13 predictors, and to explain the variance of the EE burnout.
Specialty and age contributed to the variance of the emotional exhaustion subscale of burnout due to interaction with trainees. These two variables explained 6% of the EE burnout variance. Four variables (age, number of night/shifts per month, living alone or with others, and specialty) accounted for 10% of the EE due to patients’ variance. Five variables (specialty, number of night/shifts per month, the setting of practice community versus hospital, marital status, and academic rank) contributed significantly to the regression model and accounted for 20% of the variance of EE due to interactions with administration.
Specialty contributed to the variance of all the three types of interactions of the EE burnout subscale. The beta weights of this variable in EE burnout due to patients’ interaction (−0.12) were lower than both EE burnout due to administration interactions (−0.22) and EE burnout due to trainees’ interaction (−0.22). The negative direction of beta indicated that non-surgical specialties negatively contributed to the EE subscale of burnout compared to surgical specialties.
3.2.2. Depersonalization Dimension of Burnout
To analyze the DP burnout dimension, the same 13 variables were used as predictors. The same scales of measurements and coding of the dummy variables were used. Multiple regressions with stepwise methods in entering the predictors’ variables were used to analyze DP burnout. The results for the DP burnout are summarized in
Table A5 in the
Appendix A).
Three out of the 13 variables contributed to the variance of the students’ DP burnout. The three variables were: specialty, number of night shifts per month, and setting of practice (community versus academic). The contribution of these three variables was 0.14% of the DP burnout variance. Five variables (specialty, age, academic degree, marital status, and night shifts) explained 0.15% of the variance of DP due to patients. Six variables (specialty, night shifts, setting of practice, academic position, marital status, and gender) contributed significantly to DP and explained 0.25% of the variance of DP due to administration.
Only specialty and number of night shifts contributed to the variance of all three categories of the sources of DP burnout. The beta weights of these variables were higher in DP burnout due to administration in both categories (specialty: −0.25 and night shift: 0.22) than both DP burnout due to students (specialty: −0.23 and night shifts: 0.19) and due to patients (specialty: −0.20 and night shifts: 0.13). The results indicated a negative direction of beta for specialty and a positive direction for night shifts in all the three categories of DP. Furthermore, DP burnout for the non-surgical specialty was less than the surgical specialty. This suggests that the more night shifts, the higher the DP burnout for the three categories.
3.2.3. Personal Accomplishment Dimension of Burnout
To analyze the PA burnout dimension, the same 13 variables were used as predictors (
Table A6 in
Appendix A). The results of PA burnout were as follows:
Two variables (specialty and number of in-patients per month) out of the 13 predictors contributed to the students’ PA burnout variance. These variables explained 5% of the PA burnout variance. Specialty, setting of practice (community versus academic), number of in-patients per month, and academic rank explained 14% of the PA due to patients. Specialty and setting of practice (community versus academic) contributed significantly to PA and explained 0.12% of the variance of PA due to administration.
Only specialty contributed to the variance of all three categories of the interactions of PA burnout. The beta weights of this variable were higher in PA burnout due to administration (0.30) than both due to students (0.16) and due to patients (0.19). The results indicated a significant positive direction of beta for specialty in all three main burnout interactions of PA burnout. This suggests that PA for the non-surgical specialties is higher than the surgical specialties for the three categories of burnout.
4. Discussion
Academic clinicians have more human interactions in comparison with non-academic clinicians: specifically, interactions with trainees and administration. Therefore, academic clinicians were hypothesized to be at a higher risk of burnout. We hypothesized that the three main sources of burnout in academic physicians are: interactions with trainees, with patients, and with administration. This study utilized a novel modification of Maslach’s Burnout Inventory to identify the main sources and prevalence of burnout for academic clinicians. In addition, we investigated the contributing factors to burnout, as it relates to demographic and workload variables.
Due to this novel modification, the psychometric properties of the scale were tested to ensure that our modified scale bore the same dimensionality as that of the original unmodified MBI scale.
4.1. Burnout Source and Prevalence in Academic Clinicians
This is the first study investigating the three main interactions related to burnout in a single scale in one administration. Our study showed that the least source of burnout in academic clinicians was associated with trainee interactions, followed by patient interactions, while the highest burnout levels were related to interactions with administration. The impact of administrative interactions on burnout symptoms was a particularly interesting and novel finding. Respondents may have perceived interactions with administration in different ways: e.g., office work, EHR (Electronic Health Records), secretaries, charts, academic, or hospital roles. Further studies are required to pinpoint the specific administrative interactions related to burnout in academic clinicians.
A study on 465 academic clinicians showed that the majority (68%) reported patient care as the aspect of work they found most meaningful, followed by research (19%), and education (9%). The least was administration (3%). Those spending less than 20% of their time on the most meaningful activity had higher rates of burnout on the multivariate analysis. This study concluded that spending more time on administrative responsibilities predisposes academic physicians to burnout. EHR were shown to be a source of burnout [
24]. Although patient care was shown to be most meaningful to academic physicians [
23], it was also a significant source of burnout, depending on the nature of specialty and workload.
Trainee interactions demonstrated the least source of burnout for academic clinicians in the present study. This might be because trainees (medical students, residents, and fellows) share a great deal of the workload in an academic institute. In addition, trainees work under the supervision of the academic physician; therefore, they are under their authority, which may render the interaction less stressful for clinicians.
4.2. Variables Contributing to Burnout
One of the main objectives of this study was to investigate the independent variables contributing to burnout to implement better interventional methods to target these variables in the workplace.
Our results showed that younger physicians reported higher levels of emotional exhaustion due to interactions with trainees and patients, as well as more depersonalization in response to patient interaction. This is consistent with previous research showing that burnout is more prevalent in younger workers [
25,
26] and younger physicians [
26,
27,
28]. A possible explanation is that younger workers are less experienced; they may become more cognitively overwhelmed with the workload of the “routine workday” of a senior physician. Moreover, for technical specialties, such as surgery, young surgeons may still be on the steep portion of their technical learning curve, with associated performance anxiety and fear of complications.
The current study revealed that females rated higher on the DP subscale due to interactions with administration than males. The Physicians Work Life study of a random stratified sample of 6000 physicians revealed that female physicians were 60% more likely to report burnout than male physicians [
29]. Furthermore, female physicians generally have more domestic responsibilities than male physicians, which might contribute to burnout [
30,
31].
In this study, marital status was a contributing variable to burnout, with single physicians being more prone to burnout. It was hypothesized that the reason married workers experienced lower levels of burnout is that they were usually older, psychologically mature, and stable. Furthermore, they had higher interpersonal skills and were more skillful in problem-solving and adaptability due to their involvement with their families [
11].
Certain specialties are more prone to burnout. This study showed that surgical specialties contributed to burnout. Studies from various surgical subspecialty societies in the US estimated that burnout rates among surgeons ranged from 30–48% [
32,
33]. Surgical specialties have been reported to be stressful [
34,
35,
36,
37]. Personality characteristics may be related to the higher levels of burnout associated with surgical specialties. For example, although some surgeons may believe that they are more resilient than their colleagues, the inherent personality traits that define a surgeon put them at an increased risk of distress and burnout [
26,
33]. Since research has shown that the number of medical errors reported by surgeons is related to the level of burnout and the quality of their mental life [
38], it is imperative to continue to study burnout to better understand its origins and prevention.
Lower academic rank was positively correlated with burnout and inversely correlated with PA due to patient interactions. This may be due to a similar explanation as the age above.
Patient load was reported to play a critical role in burnout amongst clinicians. In this study, the number of patients under the care of an academic clinician per month had a significant positive correlation with PA due to the student and patient interactions. This corroborates other studies showing that the most meaningful aspect of an academic clinician’s job is patient care [
38]. Patient care gives clinicians a sense of personal accomplishment, since it is the essence of being a doctor. In academic settings, an increased patient load may be associated with increased trainee assistance in sharing the workload and, hence, more opportunities for teaching interactions. This could lead to an increased sense of personal accomplishment.
5. Limitations
This study was a single center study, and, therefore, the results could be institution-specific. Another limitation was that the exact survey response rate for this study could not be accurately calculated. This was because the email distribution list was outdated: it included faculty that had vacated their position, retired, or ones with duplicated emails, including that of their admins. Furthermore, some were non-clinical faculty (PhD, researchers, etc.). This led to an estimated response rate of 36.2%.
6. Conclusions
This study investigated the prevalence of burnout and the potential etiological variables of the work-related stressors of burnout in academic physicians in a single academic center. Our results demonstrated, as hypothesized, that academic clinicians have an increased risk of burnout syndrome, and this is primarily due to interaction with administration.
This study used a novel modification of Maslach’s Burnout Inventory to identify the potential etiological factors associated with burnout in clinician educators. Three different interactions were queried: students/trainees, patients, and administration. Our results indicated that the interactions with the administration were the primary source of burnout for faculty members, followed by patients, and, lastly, trainees. Our results also demonstrated that burnout is more common in young physicians, surgical specialties, and among individuals who are single or separated. More studies in this area are required to solidify the contributing variables of burnout in our healthcare system.
In addition to having psychological implications, burnout syndrome causes workers to become disengaged in their work and become less confident. More seriously, burnout has been linked to significant clinical errors. This has substantial repercussions on patient care, as well as the quality of training for future physicians. Treating burnout is resource-intensive and still experimental. The best remedy is prevention. Therefore, it is essential to investigate the contributing variables to burnout for academic clinicians and to develop effective preventative measures to render the work environment less stressful, more productive, and, ultimately, transpire to better patient care.
Author Contributions
Conceptualization, M.M., S.R. and A.K.N.; Data curation, M.M. and A.K.N.; Investigation, A.N. and M.M.; Methodology, K.K., A.K.N., and M.M.; Project administration, A.K.N.; Resources, S.R.; Supervision, M.M., S.R. and K.K.; Validation, M.M. and A.K.N.; Visualization, M.M., A.K.N., S.R., and K.K.; Writing—original draft, A.N.; Writing—review & editing, F.T. and A.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Rotated factor Matrix for Burnout due to Student’s Interaction.
Table A1.
Rotated factor Matrix for Burnout due to Student’s Interaction.
| Due to Students/Trainees | Factor |
|---|
| EE | PA | DP |
|---|
| I feel emotionally drained from my work (1) | 0.873 | −0.093 | 0.036 |
| I feel used up at the end of the workday (2) | 0.877 | −0.066 | 0.158 |
| I feel fatigued when I get up in the morning and have to face another day on the job (3) | 0.773 | −0.094 | 0.26 |
| Working with people all day is really a strain for me (6) | 0.678 | −0.174 | 0.366 |
| I feel burned out from my work (8) | 0.775 | −0.068 | 0.336 |
| I feel frustrated by my job (13) | 0.757 | −0.103 | 0.208 |
| I feel I’m working too hard on my job (14) | 0.66 | 0.104 | 0.23 |
| I feel like I’m at the end of my rope (20) | 0.569 | −0.18 | 0.49 |
| I feel very energetic (12) | −0.371 | 0.722 | −0.047 |
| I can easily create a relaxed atmosphere with my students (17) | −0.184 | 0.712 | −0.182 |
| I feel exhilarated after working closely with my students (18) | −0.224 | 0.714 | 0.156 |
| I have accomplished many worthwhile things in this job (19) | −0.064 | 0.774 | −0.057 |
| I don’t really care what happens to some of my students (15) | 0.148 | −0.273 | 0.71 |
| I feel students blame me for some of their problems (22) | 0.299 | −0.06 | 0.473 |
| I’ve become more callous (emotionally hardened) toward people since I took this job (10) | 0.471 | −0.18 | 0.555 |
| I worry that this job is hardening me emotionally (11) | 0.512 | −0.064 | 0.591 |
| Working with people directly puts too much stress on me (16) | 0.481 | −0.18 | 0.481 |
Table A2.
Rotated Factor Matrix for Burnout due to Patient’s.
Table A2.
Rotated Factor Matrix for Burnout due to Patient’s.
| Due to Patients | Factor |
|---|
| EE | PA | DP |
|---|
| I feel emotionally drained from my work (1) | 0.853 | 0.006 | 0.163 |
| I feel used up at the end of the workday (2) | 0.832 | 0.053 | 0.194 |
| I feel fatigued when I get up in the morning and have to face another day on the job (3) | 0.775 | −0.062 | 0.32 |
| Working with people all day is really a strain for me (6) | 0.701 | −0.139 | 0.33 |
| I feel burned out from my work (8) | 0.797 | −0.082 | 0.351 |
| I feel frustrated by my job (13) | 0.722 | 0.063 | 0.334 |
| I feel I’m working too hard on my job (14) | 0.642 | 0.173 | 0.147 |
| I can easily understand how my patients feel about things (4) | 0.149 | 0.564 | −0.23 |
| I deal very effectively with the problems of my patients (7) | 0.13 | 0.757 | −0.159 |
| I feel I’m positively influencing other people’s lives through my work (9) | 0.023 | 0.748 | −0.09 |
| I feel very energetic (12) | −0.366 | 0.688 | −0.003 |
| I can easily create a relaxed atmosphere with my patients (17) | 0.006 | 0.761 | −0.34 |
| I feel exhilarated after working closely with my patients (18) | −0.175 | 0.644 | 0.155 |
| I have accomplished many worthwhile things in this job (19) | −0.042 | 0.735 | −0.08 |
| In my work, I deal with emotional problems very calmly (21) | 0.084 | 0.709 | −0.301 |
| I feel I treat some patients as if they were impersonal objects (5) | 0.282 | −0.192 | 0.653 |
| I’ve become more callous (emotionally hardened) toward people since I took this job (10) | 0.447 | −0.054 | 0.621 |
| I worry that this job is hardening me emotionally (11) | 0.458 | −0.179 | 0.672 |
| I don’t really care what happens to some of my patients (15) | 0.198 | −0.277 | 0.645 |
| I feel patients blame me for some of their problems (22) | 0.258 | −0.046 | 0.55 |
| Working with people directly puts too much stress on me (16) | 0.465 | −0.177 | 0.512 |
| I feel like I’m at the end of my rope (20) | 0.507 | −0.216 | 0.604 |
Table A3.
Rotated Factor Matrix for Burnout due to Administration.
Table A3.
Rotated Factor Matrix for Burnout due to Administration.
| Due to Administration | Factor |
|---|
| EE | PA | DP |
|---|
| I feel emotionally drained from my work (1) | 0.861 | −0.222 | 0.028 |
| I feel used up at the end of the workday (2) | 0.883 | −0.184 | 0.112 |
| I feel fatigued when I get up in the morning and have to face another day on the job (3) | 0.873 | −0.207 | 0.119 |
| I feel I treat some administration as if they were impersonal objects (5) | 0.512 | −0.18 | 0.546 |
| Working with people all day is really a strain for me (6) | 0.783 | −0.256 | 0.28 |
| I feel burned out from my work (8) | 0.887 | −0.23 | 0.063 |
| I’ve become more callous (emotionally hardened) toward people since I took this job (10) | 0.747 | −0.207 | 0.35 |
| I worry that this job is hardening me emotionally (11) | 0.774 | −0.206 | 0.325 |
| I feel frustrated by my job (13) | 0.847 | −0.239 | 0.053 |
| I feel I’m working too hard on my job (14) | 0.831 | −0.04 | 0.104 |
| Working with people directly puts too much stress on me (16) | 0.685 | −0.319 | 0.36 |
| I feel like I’m at the end of my rope (20) | 0.794 | −0.286 | 0.315 |
| I feel administration blame me for some of their problems (22) | 0.645 | −0.164 | 0.465 |
| I can easily understand how my administration feel about things (4) | −0.106 | 0.502 | −0.438 |
| I deal very effectively with the problems of my administration (7) | −0.13 | 0.64 | −0.422 |
| I feel I’m positively influencing other people’s lives through my work (9) | −0.187 | 0.817 | −0.116 |
| I feel very energetic (12) | −0.29 | 0.727 | −0.049 |
| I can easily create a relaxed atmosphere with my administration (17) | −0.277 | 0.644 | −0.378 |
| I feel exhilarated after working closely with my administration (18) | −0.148 | 0.74 | −0.016 |
| I have accomplished many worthwhile things in this job (19) | −0.237 | 0.801 | −0.162 |
| I don’t really care what happens to some of my administration (15) | 0.56 | −0.308 | 0.557 |
| In my work, I deal with emotional problems very calmly (21) | −0.11 | 0.463 | −0.478 |
Table A4.
Linear Regression for emotional exhaustion (EE) subscale.
Table A4.
Linear Regression for emotional exhaustion (EE) subscale.
| EE Students | Model 1 | Model 2 | | | | | | | | | |
| Variable | B | SE B | β | B | SE B | β | | | | | | | | | |
| Constant | 16.64 | 1.046 | | 23.05 | 3.264 | | | | | | | | | | |
| Specialty | −4.75 | 1.31 | −0.22 | −4.68 | 1.30 | −0.22 | | | | | | | | | |
| Age | | | | −0.14 | 0.07 | −0.12 | | | | | | | | | |
| R2 | | 0.05 | | | 0.06 | | | | | | | | | | |
| F | | 13.161 ** | | | 8.808 ** | | | | | | | | | | |
| EE Patients | Model 1 | Model 2 | Model 3 | Model 4 | | | |
| Variable | B | SE B | β | B | SE B | β | B | SE B | B | B | SE B | β | | | |
| Constant | 30.973 | 3.348 | | 27.428 | 3.571 | | 36.376 | 5.156 | | 38.431 | 5.219 | | | | |
| Age | −0.221 | 0.069 | −0.195 | −0.189 | 0.069 | −0.166 | −0.181 | 0.069 | −0.159 | −0.180 | 0.068 | −0.158 | | | |
| Night shift | | | | 0.341 | 0.129 | 0.161 | 0.337 | 0.128 | 0.159 | 0.305 | 0.128 | 0.144 | | | |
| Living condition | | | | | | | −4.926 | 2.064 | −0.142 | −4.990 | 2.052 | −0.144 | | | |
| Specialty | | | | | | | | | | −2.779 | 1.364 | −0.123 | | | |
| R2 | | 0.04 | | | 0.06 | | | 0.08 | | | 0.10 | | | | |
| F | | 10.271 ** | | | 8.75 ** | | | 7.841 ** | | | 7.020 ** | | | | |
| EE Administration | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 |
| Variable | B | SE B | β | B | SE B | β | B | SE B | B | B | SE B | β | B | SE B | β |
| Constant | 33.705 | 1.56 | | 28.453 | 1.921 | | 35.473 | 3.368 | | 44.422 | 5.153 | | 38.182 | 5.958 | |
| Specialty | −9.491 | 1.951 | −2.88 | −8.460 | 1.9 | −0.257 | −7.670 | 1.907 | −0.233 | −7.618 | 1.892 | −0.231 | −7.351 | 1.885 | −0.223 |
| Night Shifts | | | | 0.785 | 0.178 | 0.255 | 0.68 | 0.181 | 221 | 0.662 | 0.18 | 0.215 | 0.649 | 0.179 | 0.211 |
| Community vs. academic | | | | | | | −5.612 | 2.222 | −0.150 | −5.255 | 2.21 | −0.140 | −5.564 | 2.201 | −0.148 |
| Marital status | | | | | | | | | | −5.157 | 2.261 | −0.129 | −4.845 | 2.252 | −1.21 |
| Academic position | | | | | | | | | | | | | 3.724 | 1.817 | 0.115 |
| R2 | | 0.08 | | | 0.15 | | | 0.17 | | | 0.18 | | | 0.197 | |
| F | | 23.656 ** | | | 22.387 ** | | | 17.360 ** | | | 14.532 * | | | 12.610 ** | |
Table A5.
Linear Regression for depersonalization (DP) subscale.
Table A5.
Linear Regression for depersonalization (DP) subscale.
| DP Students | Model 1 | Model 2 | Model 3 | | | | | | | | | |
| Variable | B | SE B | B | B | SE B | β | B | SE B | β | | | | | | | | | |
| Constant | 7.411 | 0.498 | | 5.926 | 0.618 | | 8.072 | 1.085 | | | | | | | | | | |
| Specialty | −2.988 | 0.623 | −0.285 | −2.697 | 0.611 | −0.257 | −2.455 | 0.614 | −0.234 | | | | | | | | | |
| Night shift | | | | 0.222 | 0.057 | 0.226 | 0.19 | 0.058 | 0.193 | | | | | | | | | |
| Community vs. Academic | | | | | | | −1.715 | 0.716 | −0.144 | | | | | | | | | |
| R2 | | 0.08 | | | 0.131 | | | 0.140 | | | | | | | | | | |
| F | | 23.007 ** | | | 19.625 ** | | | 15.236 ** | | | | | | | | | | |
| DP Patients | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | | | |
| Variable | B | SE B | B | B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β | | | |
| Constant | 9.716 | 0.596 | | 15.508 | 1.837 | | 12.552 | 2.158 | | 15.828 | 2.525 | | 14.363 | 2.603 | | | | |
| Specialty | −2.829 | 0.746 | −0.228 | −2.768 | 0.732 | −0.224 | −2.679 | 0.726 | −0.216 | −2.629 | 0.719 | −0.212 | −2.455 | 0.719 | −0.198 | | | |
| Age | | | | −0.123 | 0.037 | −0.197 | −0.122 | 0.036 | −0.196 | −0.110 | 0.036 | −0.177 | −0.097 | 0.037 | −0.156 | | | |
| Academic Degree | | | | | | | 1.802 | 0.708 | 0.149 | 1.808 | 0.702 | 0.15 | 1.649 | 0.701 | 0.136 | | | |
| Marital | | | | | | | | | | −2.145 | 0.88 | −0.143 | −2.070 | 0.875 | −0.138 | | | |
| Night shifts | | | | | | | | | | | | | 14.363 | 2.603 | 0.125 | | | |
| R2 | | 0.052 | | | 0.091 | | | 0.113 | | | 0.133 | | | 0.148 | | | | |
| F | | 14.370 ** | | | 12.995 ** | | | 11.002 ** | | | 9.892 ** | | | 8.907 ** | | | | |
| DP administration | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 |
| Variable | B | SE B | B | B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β | B | SE B | β |
| Constant | 16.936 | 0.901 | | 13.435 | 1.1 | | 18.289 | 1.9 | | 14.002 | 2.447 | | 18.851 | 3.346 | | 22.092 | 3.685 | |
| Specialty | −6.466 | 1.125 | −0.336 | −5.749 | 1.083 | −0.299 | −5.162 | 1.082 | −0.268 | −4.930 | 1.072 | −0.256 | −4.910 | 1.065 | −0.255 | −4.709 | 1.063 | −0.245 |
| Night Shifts | | | | 0.517 | 0.101 | 0.287 | 0.447 | 0.102 | 0.248 | 0.438 | 0.101 | 0.243 | 0.429 | 0.1 | 0.238 | 0.402 | 0.101 | 0.223 |
| Community vs. academic | | | | | | | −3.921 | 1.262 | −0.178 | −4.172 | 1.25 | −0.190 | −3.981 | 1.245 | −0.181 | −3.783 | 1.241 | −0.172 |
| Academic position | | | | | | | | | | 2.807 | 1.029 | 0.149 | 2.665 | 1.024 | 0.141 | 2.927 | 1.026 | 0.155 |
| Marital status | | | | | | | | | | | | | −2.668 | 1.264 | −0.114 | −3.131 | 1.277 | −0.134 |
| Gender | | | | | | | | | | | | | | | | −2.132 | 1.045 | −0.114 |
| R2 | | 0.11 | | | 0.19 | | | 0.22 | | | 0.23 | | | 0.24 | | | 0.25 | |
| F | | 33.053 ** | | | 31.160 ** | | | 24.686 ** | | | 20.840 * | | | 17.786 ** | | | 15.699 ** | |
Table A6.
Linear Regression for personal accomplishment (PA) subscale.
Table A6.
Linear Regression for personal accomplishment (PA) subscale.
| PA Students | Model 1 | Model 2 | | | | | | |
| Variable | B | SE B | β | B | SE B | B | | | | | | |
| Constant | 33.695 | 0.873 | | 33.096 | 0.903 | | | | | | | |
| Specialty | 3.026 | 1.092 | 0.169 | 2.772 | 1.088 | 0.155 | | | | | | |
| MRP/Month | | | | 0.035 | 0.015 | 0.142 | | | | | | |
| R2 | | 0.029 | | | 0.049 | | | | | | | |
| F | | 7.672 ** | | | 6.637 ** | | | | | | | |
| PA Patients | Model 1 | Model 2 | Model 3 | Model 4 |
| Variable | B | SE B | β | B | SE B | B | B | SE B | β | B | SE B | β |
| Constant | 33.737 | 0.824 | | 29.428 | 1.549 | | 27.975 | 1.617 | | 31.894 | 2.233 | |
| Specialty | 4.513 | 1.031 | 0.262 | 3.881 | 1.031 | 0.225 | 3.482 | 1.028 | 0.202 | 3.316 | 1.019 | 0.192 |
| Community vs. Academic | | | | 3.826 | 1.173 | 0.195 | 4.52 | 1.185 | 0.23 | 4.649 | 1.174 | 0.237 |
| MRP/Month | | | | | | | 0.039 | 0.014 | 0.165 | 0.037 | 0.014 | 0.157 |
| Academic position | | | | | | | | | | −2.455 | 0.975 | −0.145 |
| R2 | | 0.068 | | | 0.098 | | | 0.121 | | | 0.139 | |
| F | | 19.176 ** | | | 15.263 ** | | | 13.003 ** | | | 11.537 ** | |
| PA administration | Model 1 | Model 2 | | | | | | |
| Variable | B | SE B | β | B | SE B | B | | | | | | |
| Constant | 14.632 | 1.133 | | 10.426 | 2.153 | | | | | | | |
| Specialty | 7.892 | 1.418 | 0.326 | 7.275 | 1.432 | 0.300 | | | | | | |
| Community vs. Academic | | | | 3.734 | 1.630 | 0.135 | | | | | | |
| R2 | | 0.106 | | | 0.124 | | | | | | | |
| F | | 30.983 ** | | | 18.368 ** | | | | | | | |
References
- Freudenberger, H.J. Staff burn-out. J. Soc. Issues 1974, 30, 159–165. [Google Scholar] [CrossRef]
- Hillert, A. Burnout—A new disease? Versicherungsmedizin 2008, 60, 163–169. [Google Scholar] [PubMed]
- Maslach, C. Burnout. Hum. Behav. 1976, 5, 16–22. [Google Scholar]
- Maslach, C.; Jackson, S.E. A social psychological analysis. Soc. Psychol. Health Illn. 1982, 227–251. Available online: https://www.researchgate.net/publication/322937117_Burnout_in_Health_Professions_A_social_psychological_analysis (accessed on 27 May 2020).
- Akerstedt, T.; Knutsson, A.; Westerholm, P.; Theorell, T.; Alfredsson, L.; Kecklund, G. Mental fatigue, work and sleep. J. Psychosom. Res. 2004, 57, 427–433. [Google Scholar] [CrossRef]
- Weber, A.; Jaekel-Reinhard, A. Burnout syndrome: A disease of modern societies? Occup. Med. (Oxf. Engl.) 2000, 50, 512–517. [Google Scholar] [CrossRef]
- Lancet, T. Physician burnout: A global crisis. Lancet 2019, 394, 93. [Google Scholar] [CrossRef]
- Rella, S.; Winwood, P.C.; Lushington, K. When does nursing burnout begin? An investigation of the fatigue experience of Australian nursing students. J. Nurs. Manag. 2009, 17, 886–897. [Google Scholar] [CrossRef]
- Burke, R.J.; Greenglass, E.R. A longitudinal examination of the Cherniss model of psychological burnout. Soc. Sci. Med. 1995, 40, 1357–1363. [Google Scholar] [CrossRef]
- Nassar, A.K.; Waheed, A.; Tuma, F. Academic Clinicians’ Workload Challenges and Burnout Analysis. Cureus 2019, 11, e6108. [Google Scholar] [CrossRef]
- Maslach, C. Burnout: The Cost of Caring; ISHK: Los Atlos, CA, USA, 2003. [Google Scholar]
- Wilmar Schaufeli, D.E.; Dirk, E. The Burnout Companion to Study and Practice; A Critical Analysis, 1st ed.; Taylor & Francis: London, UK, 2016. [Google Scholar]
- Yester, M. Work-Life Balance, Burnout, and Physician Wellness. Health Care Manag. 2019, 38, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Glasheen, J.J.; Misky, G.J.; Reid, M.B.; Harrison, R.A.; Sharpe, B.; Auerbach, A. Career satisfaction and burnout in academic hospital medicine. Arch. Intern. Med. 2011, 171, 782–785. [Google Scholar] [CrossRef]
- Antoniou, A.S.G. Handbook of Managerial Behavior and Occupational Health; Edward Elgar Publishing: Cheltenham, UK, 2009. [Google Scholar]
- McCarthy, C.J.; Lambert, R.G.; O’Donnell, M.; Melendres, L.T. The relation of elementary teachers’ experience, stress, and coping resources to burnout symptoms. Elem. Sch. J. 2009, 103, 282–300. [Google Scholar] [CrossRef]
- Skaalvik, E.M.; Skaalvik, S. Job Satisfaction, Stress and Coping Strategies in the Teaching Profession—What Do Teachers Say? Int. Educ. Stud. 2015, 8, 181–192. [Google Scholar] [CrossRef]
- Skaalvik, E.M.; Valås, H. Relations among achievement, self-concept and motivation in mathematics and language arts: A longitudinal study. J. Exp. Educ. 1999, 67, 135–149. [Google Scholar] [CrossRef]
- Azeem, S.M.; Nazir, N.A. A Study of Job Burnout among University Teachers. Psychol. Dev. Soc. 2008, 20, 51–64. [Google Scholar] [CrossRef]
- Spickard, A., Jr.; Gabbe, S.G.; Christensen, J.F. Mid-career burnout in generalist and specialist physicians. JAMA 2002, 288, 1447–1450. [Google Scholar] [CrossRef]
- Linzer, M.; Poplau, S.; Babbott, S.; Collins, T.; Guzman-Corrales, L.; Menk, J.; Murphy, M.L.; Ovington, K. Worklife and Wellness in Academic General Internal Medicine: Results from a National Survey. J. Gen. Intern. Med. 2016, 31, 1004–1010. [Google Scholar] [CrossRef]
- Olson, K.; Sinsky, C.; Rinne, S.T.; Long, T.; Vender, R.; Mukherjee, S.; Bennick, M.; Linzer, M. Cross-sectional survey of workplace stressors associated with physician burnout measured by the Mini-Z and the Maslach Burnout Inventory. Stress Health J. Int. Soc. Investig. Stress 2019, 35, 157–175. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; West, C.P.; Sloan, J.A.; Novotny, P.J.; Poland, G.A.; Menaker, R.; Rummans, T.A.; Dyrbye, L.N. Career fit and burnout among academic faculty. Arch. Intern. Med. 2009, 169, 990–995. [Google Scholar] [CrossRef]
- Tran, B.; Lenhart, A.; Ross, R.; Dorr, D.A. Burnout and EHR use among academic primary care physicians with varied clinical workloads. AMIA Jt. Summits Transl. Sci. Proc. 2019, 2019, 136–144. [Google Scholar] [PubMed]
- Maslach, C. Job Burnout: New Directions in Research and Intervention. Assoc. Psycol. Sci. 2003. [Google Scholar] [CrossRef]
- Galaiya, R.; Kinross, J.; Arulampalam, T. Factors associated with burnout syndrome in surgeons: A systematic review. Ann. R. Coll. Surg. Engl. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Breuner, C.C. Avoidance of burnout in the young athlete. Pediatr. Ann. 2012, 41, 335–339. [Google Scholar] [CrossRef][Green Version]
- Adam, S.; Mohos, A.; Kalabay, L.; Torzsa, P. Potential correlates of burnout among general practitioners and residents in Hungary: The significant role of gender, age, dependant care and experience. BMC Fam. Pract. 2018, 19, 193. [Google Scholar] [CrossRef]
- McMurray, J.E.; Linzer, M.; Konrad, T.R.; Douglas, J.; Shugerman, R.; Nelson, K.; SGIM Career Satisfaction Study Group. The Work Lives of Women Physicians. J. Gen. Intern. Med. 2000, 15, 372–380. [Google Scholar] [CrossRef]
- Gautam, M. Women in medicine: Stresses and solutions. West. J. Med. 2001, 174, 37–41. [Google Scholar] [CrossRef][Green Version]
- Cathelain, A.; Merlier, M.; Estrade, J.P.; Duhamel, A.; Phalippou, J.; Kerbage, Y.; Collinet, P. Assessment of the Quality of Life of Gynecologic Surgeons: A National Survey in France. J. Gynecol. Obstet. Hum. Reprod. 2020, 101791. [Google Scholar] [CrossRef]
- Campbell, D.A., Jr.; Sonnad, S.S.; Eckhauser, F.E.; Campbell, K.K.; Greenfield, L.J. Burnout among American surgeons. Surgery 2001, 130, 696–702; discussion 702–695. [Google Scholar] [CrossRef]
- Balch, C.M.; Freischlag, J.A.; Shanafelt, T.D. Stress and burnout among surgeons: Understanding and managing the syndrome and avoiding the adverse consequences. Arch. Surg. (Chicago, Ill: 1960) 2009, 144, 371–376. [Google Scholar] [CrossRef]
- Dyrbye, L.N.; Harris, I.; Rohren, C.H. Early clinical experiences from students’ perspectives: A qualitative study of narratives. Acad. Med. J. Assoc. Am. Med. Coll. 2007, 82, 979–988. [Google Scholar] [CrossRef] [PubMed]
- Morse, G.; Salyers, M.P.; Rollins, A.L.; Monroe-DeVita, M.; Pfahler, C. Burnout in mental health services: A review of the problem and its remediation. Adm. Policy Ment. Health 2012, 39, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Kent, G.G.; Johnson, A.G. Conflicting demands in surgical practice. Ann. R. Coll. Surg. Engl. 1995, 77 (Suppl. 5), 235–238. [Google Scholar]
- Shanafelt, T.D.; West, C.P.; Poland, G.A.; LaRusso, N.F.; Menaker, R.; Bahn, R.S. Principles to promote physician satisfaction and work-life balance. Minn. Med. 2008, 91, 41–43. [Google Scholar] [PubMed]
- Shanafelt, T.D.; Balch, C.M.; Bechamps, G.J.; Russell, T.; Dyrbye, L.; Satele, D.; Collicott, P.; Novotny, P.; Sloan, J.; Freischlag, J.A. Burnout and career satisfaction among American surgeons. Ann. Surg. 2009, 250, 463–471. [Google Scholar] [CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).


{kind=link}
