Preference for Masculine or Feminine Gender Roles and Its Relationship to Well-Being in Transgender Persons: Comparing Pre-Treatment, Hormonal Therapy, and Post-Surgery Groups

Abstract
:1. Introduction
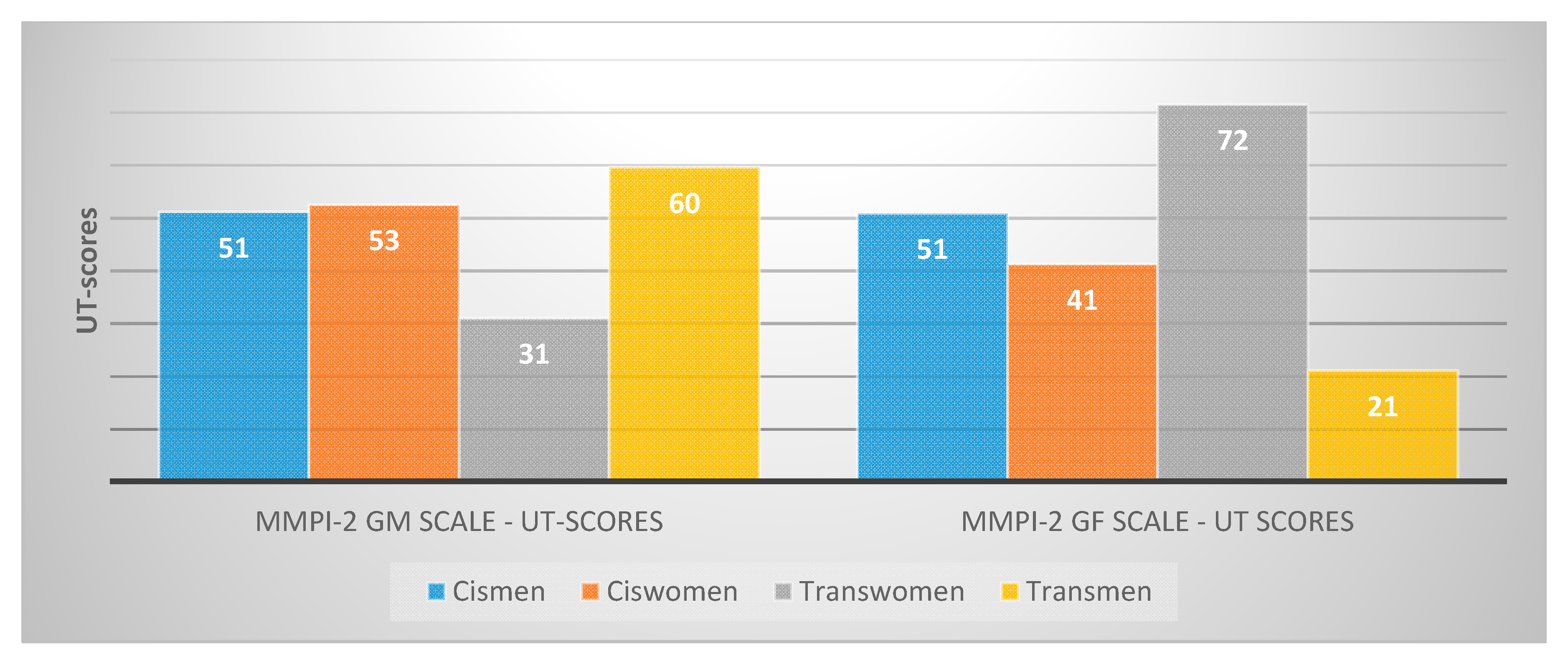
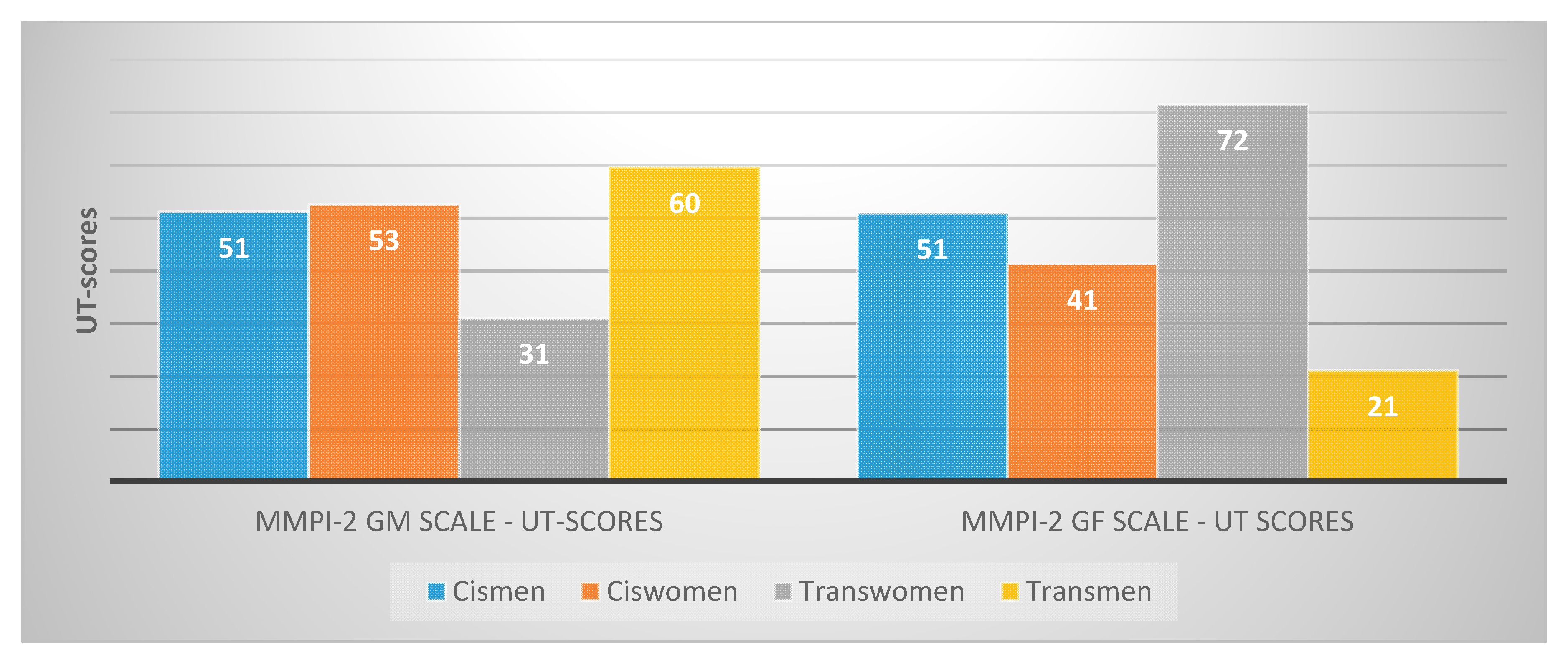
- Russian people who define themselves as transgender prefer roles typical of the desired gender and reject roles typical of their sex assigned at birth.
- The lower level of well-being in Russian transgender people in comparison with Russian cisgender persons is more pronounced in the pre-treatment group and the least pronounced in the after-surgery group.
- The lower level of well-being in Russian transgender people is not fully explained by their preferences for masculine or feminine gender roles.
2. Methods
3. Results
3.1. Preferences for Gender Roles and the Association of the Preferences with Well-Being in Transgender and Cisgender Participants
3.2. Stage of Transgender Transformations, Gender Roles, and Well-Being
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WPATH De-Psychopathologisation Statement. Available online: https://www.wpath.org/media/cms/Documents/Public%20Policies/2020/FINAL%20Joint%20WPATH%20USPATH%20Statement%20On%20Resumption%20of%20Medically%20Necessary%20Surgeries%20During%20COVID.pdf (accessed on 14 September 2019).
- Motmans, J.; Meier, P.; Ponnet, K. Female and Male Transgender Quality of Life: Socioeconomic and Medical Differences. J. Sex. Med. 2012, 9, 743–750. [Google Scholar] [CrossRef] [PubMed]
- Standards of Care (SOC) for the Health of Transsexual, Transgender, and Gender Nonconforming People. Int. J. Transgenderism 2012, 13, 165–232. [CrossRef]
- Burnes, T.; Richmond, K.; Dexter, M.; Singh, A.; Cherrington, A. The Experiences of Transgender Survivors of Trauma Who Undergo Social and Medical Transition. Traumatology 2016, 22, 75–84. [Google Scholar] [CrossRef]
- Grossman, A.; D’augelli, A. Transgender Youth: Invisible and Vulnerable. J. Homosex. 2006, 51, 111–128. [Google Scholar] [CrossRef] [PubMed]
- Girshick, L.B. Transgender Voices: Beyond Women and Men; University Press of New England: Hannover, Germany; London, UK, 2008; pp. 133–144. [Google Scholar]
- Chrisler, J.C.; McCreary, D.R. Handbook of Gender Research in Psychology; Springer: Berlin, Germany, 2010; Volume 2, p. 366. [Google Scholar]
- Gorodetskaya, O.; Kovalisidi, C. Current Socio-Economic Situation of Transgender and Queer People in the Former Soviet Union; Report; Trans*Feminist Initiative Group AdamanT*: Kiev, Ukraine, 2016; p. 39. [Google Scholar]
- LGBT Organization «Vyhod». Gender Identity in the Epicenter of Discrimination: The Life of Trans*People in Russia; Brochure; LGBT Organization «Vyhod»: Saint Petersbur, Russia, 2013; 44p. [Google Scholar]
- Colizzi, M.; Costa, R.; Todarello, O. Transsexual patients’ psychiatric comorbidity and positive effect of cross-sex hormonal treatment on mental health: Results from a longitudinal study. Psychoneuroendocrinology 2014, 39, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Gil, E.; Zubiaurre-Elorza, L.; Esteva, I.; Guillamon, A.; Godás, T.; Cruz Almaraz, M.; Halperin, I.; Salamero, M. Hormone-treated transsexuals report less social distress, anxiety and depression. Psychoneuroendocrinology 2012, 37, 662–670. [Google Scholar] [CrossRef] [PubMed]
- Newfield, E.; Hart, S.; Dibble, S. Female-to-male transgender quality of life. Qual Life Res. 2006, 15, 1447–1457. [Google Scholar] [CrossRef] [PubMed]
- Matevosyan, S.; Vvedensky, G. Gender Dysphoria (Clinical Phenomenological Characteristics, Treatment and Rehabilitation of the Gender Rejection Syndrome); Medical Information Agency: Moscow, Russia, 2012; p. 400. [Google Scholar]
- Yang, X.; Wang, L.; Hao, C.; Gu, Y.; Song, W.; Wang, J.; Chang, M.M.; Zhao, Q. Sex Partnership and Self-Efficacy Influence Depression in Chinese Transgender Women: A Cross-Sectional Study. PLoS ONE 2015, 14. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhao, L.; Wang, L.; Hao, C.; Gu, Y.; Song, W.; Zhao, Q.; Wang, X. Quality of Life of Transgender Women from China and Associated Factors: A Cross-Sectional Study. J. Sex. Med. 2016, 13, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Butcher, J.N.; Graham, J.R.; Ben-Porath, Y.S.; Tellegen, A.; Dahlstrom, W.G.; Kaemmer, B. MMPI-2 (Minnesota Multiphasic Personality Inventory-2): Manual for Administration and Scoring, 2nd ed.; University of Minnesota Press: Minneapolis, MN, USA, 2001. [Google Scholar]
- Diener, E.; Ryan, K. Subjective well-being: A general overview. S. Afr. J. Psychol. 2009, 39, 391–406. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Diener, E.; Wirtz, D.; Tov, W.; Kim-Prieto, C.; Choi, D.; Oishi, S.; Bisqas-Diener, R. New well-being measures: Short scales to assess flourishing and positive and negative feelings. Soc. Indic. Res. 2010, 97, 143–156. [Google Scholar] [CrossRef]
- Rasskazova, E.; Bogomaz, S.; Dorfman, L.; Leontiev, D.; Neyaskina, J.; Sulimina, O.V.; Chetoshikova, E. Psychometric characteristics of the Russian version of MMPI-2. Psichol. Issled. 2013, 6, 2. [Google Scholar]
- Kumchenko, S.; Demedetskaya, J. Specific ratio of transsexuals in Russian-speaking countries. Psychol. Hist. Crit. Rev. Mod. Res. 2018, 7, 145–155. [Google Scholar]
- Rasskazova, E.; Tkhostov, A. Identity as a psychological construct: Possibilities and limitations of an interdisciplinary approach. Psichologicheskie Issled. 2012, 5, 26. [Google Scholar]
- Ilyin, E. Sex and gender. Peter 2010, 1, 688. [Google Scholar]
- Kumchenko, S. Medical operations as a way to reduce a sense of uncertainty in transgender people. In Personality in the Age of Change: Mobilis in Mobili, Proceedings of the International Scientific and Practical Conference, Moscow, Russia, 17–18 December 2018; Smysl: Moscow, Russia, 2018; pp. 331–334. [Google Scholar]
- Bem, S. The measurement of psychological androgyny. J. Consult. Clin. Psychol. 1974, 42, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Tkhostov, A. Disease as a Semiotic System. Part 1; Series 14: Psychology; Vestnik of the Moscow University: Moscow, Russia, 1993; Volume 1, pp. 3–16. [Google Scholar]
- Kumchenko, S.; Tkhostov, A.; Rasskazova, E.; Chepeliuk, A. Subjective quality of life of transsexual people in different stages of medical transition. Eur. Psychiatry 2019, 56S, S211. [Google Scholar]
- Kumchenko, S. Resource features in different transgender identities. In Actual Problems of Psychological Science, Proceedings of the Collection of Articles and Speeches of the International Scientific Conference, Moscow, Russia, 10–12 May 2018; Krasnoyarsk Research and Innovation Center: Krasnoyarsk, Russia, 2019; pp. 217–219. [Google Scholar]
- Vygotsky, L. The Collected Works: Child Psychology; Springer Science & Business Media: Berlin, Germany, 2012; 362p. [Google Scholar]

{kind=link}
| Scales | Cisgender People | Transgender People | Major Effect of Group *** | Interaction between Group and Gender *** | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cisgender Men | Cisgender Women | Transwomen | Transmen | |||||||||
| Mean | St. dev. | Mean | St. dev. | Mean | St. dev. | Mean | St. dev. | F | η2 | F | η2 | |
| Satisfaction with life | 21.28 | 5.06 | 21.83 | 5.82 | 16.52 | 7.11 | 16.12 | 5.72 | 45.38 ** | 0.15 | 0.37 | 0.00 |
| Positive emotions | 20.03 | 4.75 | 20.64 | 4.96 | 18.39 | 5.30 | 16.84 | 5.12 | 16.81 ** | 0.06 | 2.67 | 0.01 |
| Negative emotions | 15.33 | 4.05 | 15.73 | 5.15 | 17.65 | 5.33 | 19.38 | 5.28 | 2.10 ** | 0.07 | 0.99 | 0.00 |
| MMPI-2 GM scale (raw scores) | 35.08 | 5.19 | 27.60 | 6.28 | 26.26 | 8.12 | 30.61 | 6.76 | 1.97 ** | 0.04 | 45.74 ** | 0.15 |
| MMPI-2 GF scale (raw scores) | 25.10 | 3.54 | 31.18 | 4.88 | 31.30 | 5.19 | 25.00 | 5.06 | 0.00 | 0.00 | 95.19 ** | 0.26 |
| Scales | Transgender People without Hormonal Therapy or Surgery | Transgender People in Hormonal Therapy | Transgender People in Hormonal Therapy and after Surgery | Major Effect of Stage of Transformation | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Transwomen | Transmen | Transwomen | Transmen | Transwomen | Transmen | |||||||||
| Mean | St. dev. | Mean | St. dev. | Mean | St. dev. | Mean | St. dev. | Mean | St. dev. | Mean | St. dev. | F | η2 | |
| Satisfaction with life | 16.17 | 6.51 | 14.00 | 5.07 | 11.25 | 3.11 | 17.68 | 6.46 | 21.44 | 6.78 | 19.04 | 4.71 | 13.77 ** | 0.16 |
| Positive emotions | 17.08 | 6.08 | 15.54 | 5.17 | 17.19 | 4.75 | 17.04 | 5.25 | 20.33 | 4.89 | 19.16 | 4.30 | 5.17 ** | 0.07 |
| Negative emotions | 19.08 | 6.14 | 21.06 | 4.93 | 19.13 | 4.38 | 18.56 | 6.09 | 15.39 | 5.01 | 16.56 | 3.78 | 7.09 ** | 0.09 |
| MMPI-2 GM scale (raw scores) | 24.83 | 7.31 | 29.42 | 7.34 | 25.44 | 6.91 | 30.56 | 6.34 | 27.94 | 9.64 | 33.60 | 4.21 | 2.99 * | 0.04 |
| MMPI-2 GF scale (raw scores) | 30.92 | 3.78 | 24.81 | 5.20 | 30.50 | 6.31 | 24.88 | 4.59 | 32.28 | 5.02 | 24.96 | 5.12 | 0.38 | 0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumchenko, S.; Rasskazova, E.; Tkhostov, A.; Emelin, V. Preference for Masculine or Feminine Gender Roles and Its Relationship to Well-Being in Transgender Persons: Comparing Pre-Treatment, Hormonal Therapy, and Post-Surgery Groups. Behav. Sci. 2020, 10, 100. https://doi.org/10.3390/bs10060100
Kumchenko S, Rasskazova E, Tkhostov A, Emelin V. Preference for Masculine or Feminine Gender Roles and Its Relationship to Well-Being in Transgender Persons: Comparing Pre-Treatment, Hormonal Therapy, and Post-Surgery Groups. Behavioral Sciences. 2020; 10(6):100. https://doi.org/10.3390/bs10060100
Chicago/Turabian StyleKumchenko, Sergey, Elena Rasskazova, Aleksander Tkhostov, and Vadim Emelin. 2020. "Preference for Masculine or Feminine Gender Roles and Its Relationship to Well-Being in Transgender Persons: Comparing Pre-Treatment, Hormonal Therapy, and Post-Surgery Groups" Behavioral Sciences 10, no. 6: 100. https://doi.org/10.3390/bs10060100
APA StyleKumchenko, S., Rasskazova, E., Tkhostov, A., & Emelin, V. (2020). Preference for Masculine or Feminine Gender Roles and Its Relationship to Well-Being in Transgender Persons: Comparing Pre-Treatment, Hormonal Therapy, and Post-Surgery Groups. Behavioral Sciences, 10(6), 100. https://doi.org/10.3390/bs10060100