Acute Physiological Responses Following a Bout of Vigorous Exercise in Military Soldiers and First Responders with PTSD: An Exploratory Pilot Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
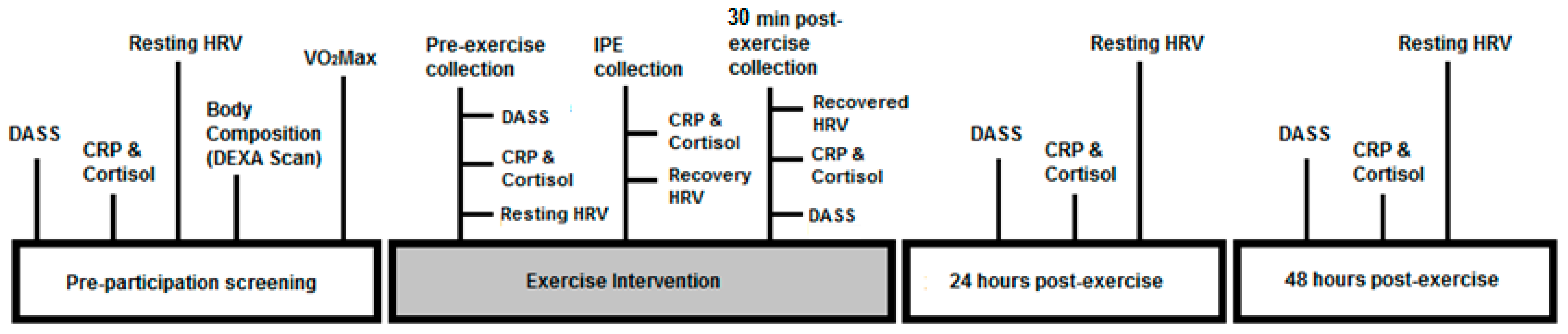
2.2. Study Design
2.3. Assessment Methods and Data Acquisition
2.4. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Exercise Protocol
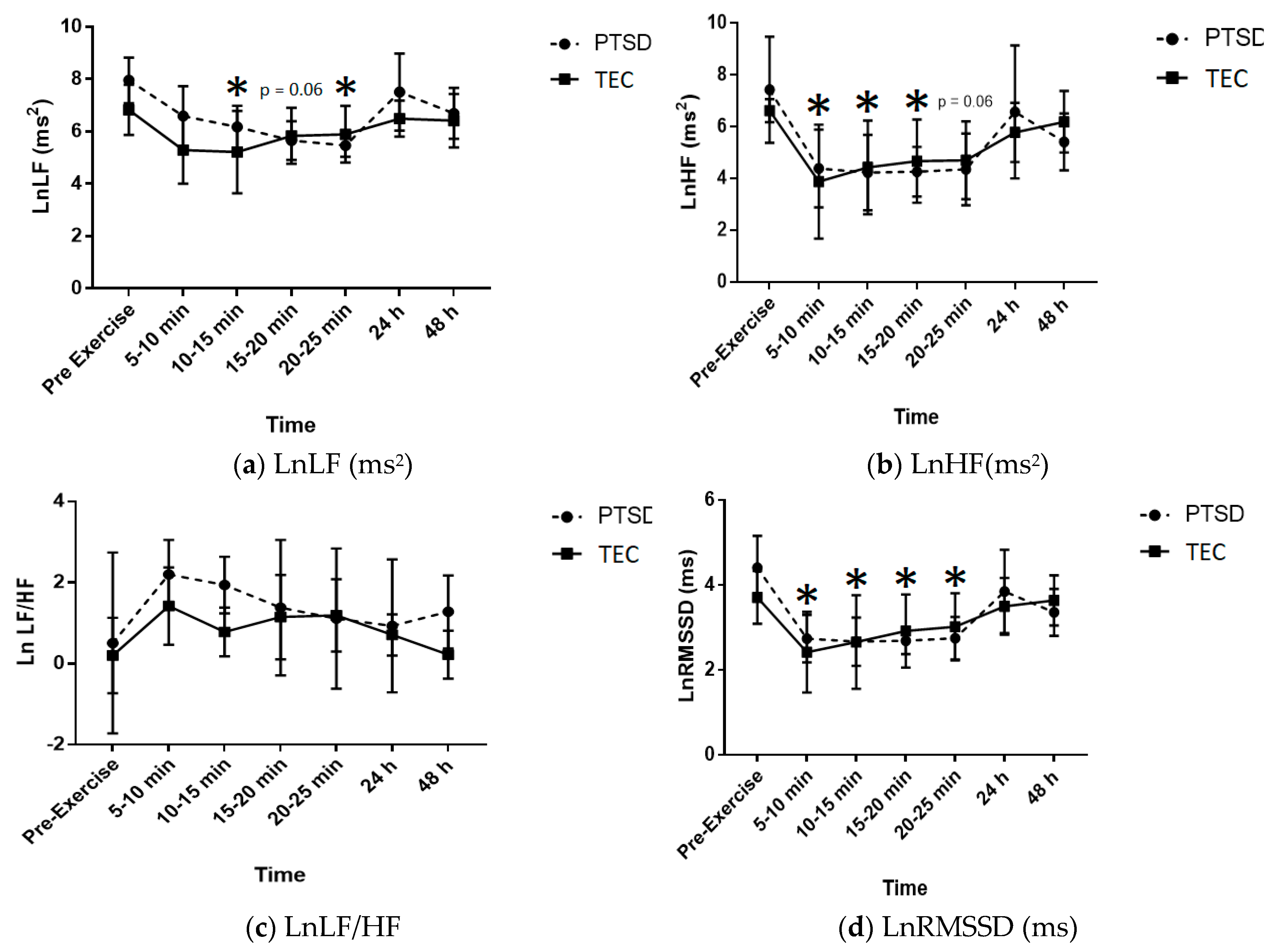
3.3. HRV Analysis
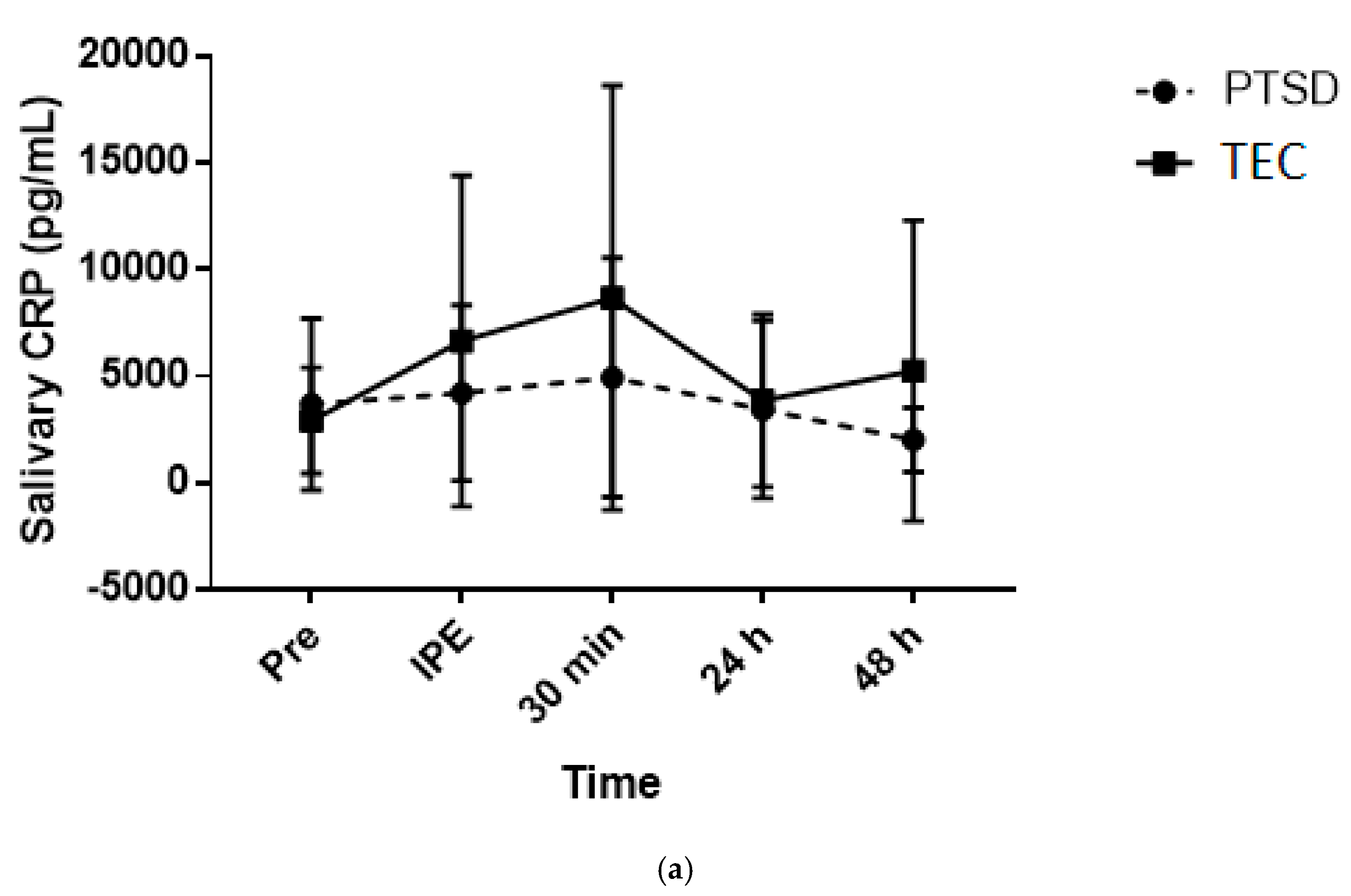
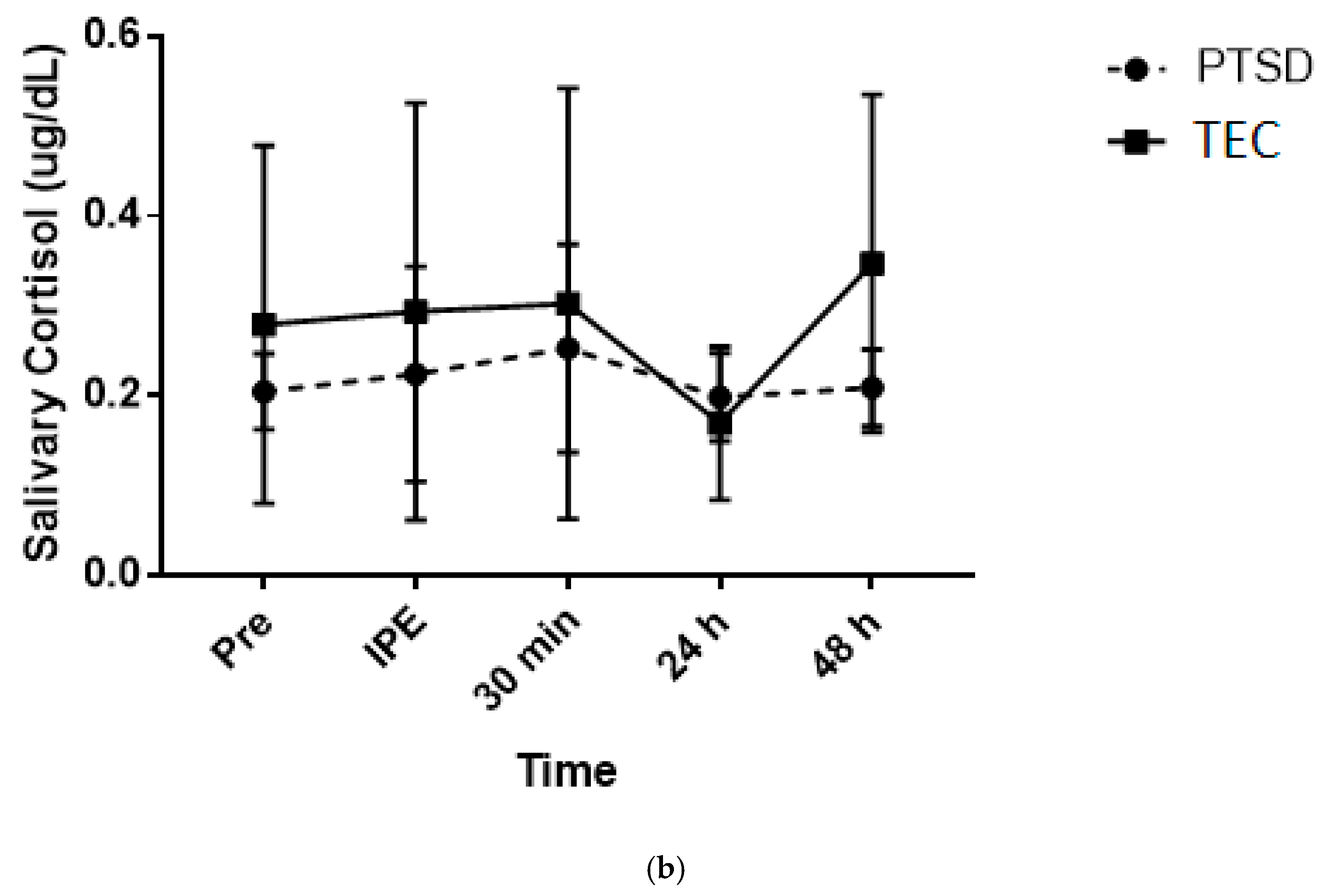
3.4. Saliva Analysis
3.5. Psychological Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- McLeay, S.C.; Harvey, W.M.; Romaniuk, M.N.; Crawford, D.H.; Colquhoun, D.M.; Young, R.M.; Dwyer, M.; Gibson, J.M.; O′Sullivan, R.A.; Cooksley, G.; et al. Physical comorbidities of post-traumatic stress disorder in Australian Vietnam War veterans. Med. J. Aust. 2017, 206, 251–257. [Google Scholar] [CrossRef]
- Daskalakis, N.P.; Lehrner, A.; Yehuda, R. Endocrine aspects of post-traumatic stress disorder and implications for diagnosis and treatment. Endocrinol. Metab. Clin. N. Am. 2013, 42, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Babson, K.A.; Heinz, A.J.; Ramirez, G.; Puckett, M.; Irons, J.G.; Bonn-Miller, M.O.; Woodward, S. The interactive role of exercise and sleep on veteran recovery from symptoms of PTSD. Ment. Health Phys. Act. 2015, 8, 15–20. [Google Scholar] [CrossRef]
- Foa, E.B.; Gillihan, S.J.; Bryant, R.A. Challenges and Successes in Dissemination of Evidence-Based Treatments for Posttraumatic Stress: Lessons Learned From Prolonged Exposure Therapy for PTSD. Psychol. Sci. Public Interest 2013, 14, 65–111. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, D.; Dhabhar, F.S.; Mellon, S.H.; Yehuda, R.; Grenon, S.M.; Flory, J.D.; Bierer, L.M.; Abu-Amara, D.; Coy, M.; Makotkine, I.; et al. Increased pro-Inflammatory milieu in combat related PTSD-A new cohort replication study. Brain Behav. Immun. 2017, 59, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Correll, C.U.; Solmi, M.; Veronese, N.; Bortolato, B.; Rosson, S.; Santonastaso, P.; Thapa-Chhetri, N.; Fornaro, M.; Gallicchio, D.; Collantoni, E.; et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: A large-Scale meta-Analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2017, 16, 163–180. [Google Scholar] [CrossRef]
- Vancampfort, D.; Richards, J.; Stubbs, B.; Akello, G.; Gbiri, C.A.; Ward, P.B.; Rosenbaum, S. Physical Activity in People With Posttraumatic Stress Disorder: A Systematic Review of Correlates. J. Phys. Act. Health 2016, 13, 910–918. [Google Scholar] [CrossRef]
- Baker, D.G.; Nievergelt, C.M.; O′Connor, D.T. Biomarkers of PTSD: Neuropeptides and immune signaling. Neuropharmacology 2012, 62, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Dennis, P.A.; Weinberg, J.B.; Calhoun, P.S.; Watkins, L.L.; Sherwood, A.; Dennis, M.F.; Beckham, J.C. An investigation of vago-Regulatory and health-Behavior accounts for increased inflammation in posttraumatic stress disorder. J. Psychosom. Res. 2016, 83, 33–39. [Google Scholar] [CrossRef][Green Version]
- Wolff, E.; Gaudlitz, K.; von Lindenberger, B.L.; Plag, J.; Heinz, A.; Strohle, A. Exercise and physical activity in mental disorders. Eur. Arch. Psychiatry Clin. Neurosci. 2011, 261 (Suppl 2), S186–S191. [Google Scholar] [CrossRef]
- Inslicht, S.S.; Otte, C.; McCaslin, S.E.; Apfel, B.A.; Henn-Haase, C.; Metzler, T.; Yehuda, R.; Neylan, T.C.; Marmar, C. Cortisol awakening response prospectively predicts peritraumatic and acute stress reactions in police officers. Biol. Psychiatry 2011, 70, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Wingenfeld, K.; Whooley, M.A.; Neylan, T.C.; Otte, C.; Cohen, B.E. Effect of current and lifetime posttraumatic stress disorder on 24-h urinary catecholamines and cortisol: Results from the Mind Your Heart Study. Psychoneuroendocrinology 2015, 52, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Hellman, N.; Abelson, J.L.; Rao, U. Cortisol, heart rate, and blood pressure as early markers of PTSD risk: A systematic review and meta-analysis. Clin. Psychol. Rev. 2016, 49, 79–91. [Google Scholar] [CrossRef] [PubMed]
- Meewisse, M.L.; Reitsma, J.B.; de Vries, G.J.; Gersons, B.P.; Olff, M. Cortisol and post-Traumatic stress disorder in adults: Systematic review and meta-analysis. Br. J. Psychiatry J. Ment. Sci. 2007, 191, 387–392. [Google Scholar] [CrossRef]
- Gill, J.M.; Saligan, L.; Woods, S.; Page, G. PTSD is associated with an excess of inflammatory immune activities. Perspect. Psychiatr. Care 2009, 45, 262–277. [Google Scholar] [CrossRef] [PubMed]
- Castro-Vale, I.; van Rossum, E.F.; Machado, J.C.; Mota-Cardoso, R.; Carvalho, D. Genetics of glucocorticoid regulation and posttraumatic stress disorder--What do we know? Neurosci. Biobehav. Rev. 2016, 63, 143–157. [Google Scholar] [CrossRef]
- Reeves, J.W.; Fisher, A.J.; Newman, M.G.; Granger, D.A. Sympathetic and hypothalamic-pituitary-Adrenal asymmetry in generalized anxiety disorder. Psychophysiology 2016, 53, 951–957. [Google Scholar] [CrossRef]
- Levine, A.B.; Levine, L.M.; Levine, T.B. Posttraumatic stress disorder and cardiometabolic disease. Cardiology 2014, 127, 1–19. [Google Scholar] [CrossRef]
- Valiente-Gomez, A.; Moreno-Alcazar, A.; Treen, D.; Cedron, C.; Colom, F.; Perez, V.; Amann, B.L. EMDR beyond PTSD: A Systematic Literature Review. Front Psychol. 2017, 8, 1668. [Google Scholar] [CrossRef]
- Shivakumar, G.; Anderson, E.H.; Suris, A.M.; North, C.S. Exercise for PTSD in Women Veterans: A Proof-Of-Concept Study. Mil. Med. 2017, 182, e1809–e1814. [Google Scholar] [CrossRef]
- Meyer, P.W.; Muller, L.E.; Zastrow, A.; Schmidinger, I.; Bohus, M.; Herpertz, S.C.; Bertsch, K. Heart rate variability in patients with post-traumatic stress disorder or borderline personality disorder: Relationship to early life maltreatment. J. Neural Transm. (Vienna) 2016, 123, 1107–1118. [Google Scholar] [CrossRef] [PubMed]
- Molina, G.E.; Fontana, K.E.; Porto, L.G.; Junqueira, L.F., Jr. Post-Exercise heart-Rate recovery correlates to resting heart-Rate variability in healthy men. Clin. Auton. Res. Off. J. Clin. Auton. Res. Soc. 2016, 26, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, K.; Stojanovska, L.; Polenakovic, M.; Bosevski, M.; Apostolopoulos, V. Exercise and mental health. Maturitas 2017, 106, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, J.W.; Craft, L.L.; Dunsiger, S.I.; Ciccolo, J.T. Direct and indirect effects of exercise on posttraumatic stress disorder symptoms: A longitudinal study. Gen. Hosp. Psychiatry 2017, 49, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.M.; Pedersen, B.K. The role of IL-6 in mediating the anti-Inflammatory effects of exercise. J. Physiol. Pharmacol. 2006, 57 (Suppl 10), 43–51. [Google Scholar]
- Koszycki, D.; Taljaard, M.; Bielajew, C.; Gow, R.M.; Bradwejn, J. Stress reactivity in healthy child offspring of parents with anxiety disorders. Psychiatry Res. 2019, 272, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Pace, T.W.; Heim, C.M. A short review on the psychoneuroimmunology of posttraumatic stress disorder: From risk factors to medical comorbidities. Brain Behav. Immun. 2011, 25, 6–13. [Google Scholar] [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J. Reference Standards for Cardiorespiratory Fitness Measured With Cardiopulmonary Exercise Testing: Data From the Fitness Registry and the Importance of Exercise National Database. Mayo Clin. Proc. 2015, 90, 1515–1523. [Google Scholar] [CrossRef]
- Naidoo, T.; Konkol, K.; Biccard, B.; Dudose, K.; McKune, A.J. Elevated salivary C-Reactive protein predicted by low cardio-Respiratory fitness and being overweight in African children. Cardiovasc. J. Afr. 2012, 23, 501–506. [Google Scholar] [CrossRef]
- Australia EaSS. Adult Pre-Exercise Screening Form Queensland, Australia 2012. Available online: https://www.essa.org.au/for-gps/adult-pre-exercise-screening-system/ (accessed on 4 April 2017).
- Bhasin, S.K.; Sharma, R.; Saini, N.K. Depression, anxiety and stress among adolescent students belonging to affluent families: A school-Based study. Indian J. Pediatr. 2010, 77, 161–165. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Henry, J.D.; Crawford, J.R. The short-Form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44 (Pt 2), 227–239. [Google Scholar] [CrossRef]
- Klika, R.J.; Golik, K.S.; Drum, S.N.; Callahan, K.E.; Thorland, W.G. Comparison of physiological response to cardiopulmonary exercise testing among cancer survivors and healthy controls. Eur. J. Appl. Physiol. 2011, 111, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Poole, D.C.; Wilkerson, D.P.; Jones, A.M. Validity of criteria for establishing maximal O2 uptake during ramp exercise tests. Eur. J. Appl. Physiol. 2008, 102, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Hawley, J.A.; Noakes, T.D. Peak power output predicts maximal oxygen uptake and performance time in trained cyclists. Eur. J. Appl. Physiol. Occup. Physiol. 1992, 65, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Weippert, M.; Kumar, M.; Kreuzfeld, S.; Arndt, D.; Rieger, A.; Stoll, R. Comparison of three mobile devices for measuring R-R intervals and heart rate variability: Polar S810i, Suunto t6 and an ambulatory ECG system. Eur. J. Appl. Physiol. 2010, 109, 779–786. [Google Scholar] [CrossRef]
- Caro-Moran, E.; Fernandez-Lao, C.; Galiano-Castillo, N.; Cantarero-Villanueva, I.; Arroyo-Morales, M.; Diaz-Rodriguez, L. Heart Rate Variability in Breast Cancer Survivors After the First Year of Treatments: A Case-Controlled Study. Biol. Res. Nurs. 2016, 18, 43–49. [Google Scholar] [CrossRef]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065.
- Sookan, T.; McKune, A.J. Heart rate variability in physically active individuals: Reliability and gender characteristics. Cardiovasc. J. Afr. 2012, 23, 67–72. [Google Scholar]
- Akselrod, S.; Gordon, D.; Ubel, F.A.; Shannon, D.C.; Berger, A.C.; Cohen, R.J. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-To-Beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef]
- Pomeranz, B.; Macaulay, R.J.; Caudill, M.A.; Kutz, I.; Adam, D.; Gordon, D.; Kilborn, K.M.; Barger, A.C.; Shannon, D.C.; Cohen, R.J.; et al. Assessment of autonomic function in humans by heart rate spectral analysis. Am. J. Physiol. 1985, 248 (Pt 2), H151–H153. [Google Scholar] [CrossRef]
- Warren, J.H.; Jaffe, R.S.; Wraa, C.E.; Stebbins, C.L. Effect of autonomic blockade on power spectrum of heart rate variability during exercise. Am. J. Physiol. 1997, 273 (Pt 2), R495–R502. [Google Scholar] [CrossRef]
- von Rosenberg, W.; Chanwimalueang, T.; Adjei, T.; Jaffer, U.; Goverdovsky, V.; Mandic, D.P. Resolving Ambiguities in the LF/HF Ratio: LF-HF Scatter Plots for the Categorization of Mental and Physical Stress from HRV. Front. Physiol. 2017, 8, 360. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M. Monitoring training status with HR measures: Do all roads lead to Rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef] [PubMed]
- Flatt, A.A.; Esco, M.R.; Nakamura, F.Y.; Plews, D.J. Interpreting daily heart rate variability changes in collegiate female soccer players. J. Sports Med. Phys. Fit. 2017, 57, 907–915. [Google Scholar]
- Nakamura, F.Y.; Flatt, A.A.; Pereira, L.A.; Ramirez-Campillo, R.; Loturco, I.; Esco, M.R. Ultra-Short-Term Heart Rate Variability is Sensitive to Training Effects in Team Sports Players. J. Sports Sci. Med. 2015, 14, 602–605. [Google Scholar]
- Plews, D.J.; Laursen, P.B.; Stanley, J.; Kilding, A.E.; Buchheit, M. Training adaptation and heart rate variability in elite endurance athletes: Opening the door to effective monitoring. Sports Med. (Auckl. NZ) 2013, 43, 773–781. [Google Scholar] [CrossRef]
- Penttila, J.; Helminen, A.; Jartti, T.; Kuusela, T.; Huikuri, H.V.; Tulppo, M.P.; Coffeng, R.; Scheinin, H. Time domain, geometrical and frequency domain analysis of cardiac vagal outflow: Effects of various respiratory patterns. Clin. Physiol. (Oxf. Engl.) 2001, 21, 365–376. [Google Scholar] [CrossRef]
- Young, H.A.; Benton, D. Heart-Rate variability: A biomarker to study the influence of nutrition on physiological and psychological health? Behav. Pharmacol. 2018, 29, 140–151. [Google Scholar] [CrossRef]
- Starzak, D.E.; Konkol, K.F.; McKune, A.J. Effects of Cardiorespiratory Fitness and Obesity on Salivary Secretory IgA and Alpha-Amylase in South African Children. Children (Basel Switz.) 2016, 3, 12. [Google Scholar] [CrossRef]
- Riebe, D.; Ehrman, J.; Liguori, G.; Magal, M. ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2017. [Google Scholar]
- Michael, S.; Graham, K.S.; Davis, G.M.O. Cardiac Autonomic Responses during Exercise and Post-Exercise Recovery Using Heart Rate Variability and Systolic Time Intervals-A Review. Front. Physiol. 2017, 8, 301. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Macias, N.; Quezada, A.D.; Flores, M.; Valencia, M.E.; Denova-Gutierrez, E.; Quiterio-Trenado, M.; Gallegos-Carrillo, K.; Barquera, S.; Salmerón, J. Accuracy of body fat percent and adiposity indicators cut off values to detect metabolic risk factors in a sample of Mexican adults. BMC Public Health 2014, 14, 341. [Google Scholar] [CrossRef]
- Lee, S.M.; Han, H.; Jang, K.I.; Huh, S.; Huh, H.J.; Joo, J.Y.; Chae, J.H. Heart rate variability associated with posttraumatic stress disorder in victims’ families of sewol ferry disaster. Psychiatry Res. 2018, 259, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.A.; Chang, C.C.; Tzeng, N.S.; Kuo, T.B.; Lu, R.B.; Huang, S.Y. Decreased cardiac vagal control in drug-naive patients with posttraumatic stress disorder. Psychiatry Investig. 2013, 10, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Thome, J.; Densmore, M.; Frewen, P.A.; McKinnon, M.C.; Theberge, J.; Nicholson, A.A.; Koenig, J.; Thayer, J.F.; Lanius, R. Desynchronization of autonomic response and central autonomic network connectivity in posttraumatic stress disorder. Hum. Brain Mapp. 2017, 38, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Cherland, E. The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, Self-Regulation. J. Can. Acad. Child Adolesc. Psychiatry 2012, 21, 313–314. [Google Scholar]
- Lewis, G.F.; Hourani, L.; Tueller, S.; Kizakevich, P.; Bryant, S.; Weimer, B.; Strange, L. Relaxation training assisted by heart rate variability biofeedback: Implication for a military predeployment stress inoculation protocol. Psychophysiology 2015, 52, 1167–1174. [Google Scholar] [CrossRef]
- Brudey, C.; Park, J.; Wiaderkiewicz, J.; Kobayashi, I.; Mellman, T.A.; Marvar, P.J. Autonomic and inflammatory consequences of posttraumatic stress disorder and the link to cardiovascular disease. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, R315–R321. [Google Scholar] [CrossRef]
- Goldstein, D.S.; Bentho, O.; Park, M.-Y.; Sharabi, Y. Low-Frequency power of heart rate variability is not a measure of cardiac sympathetic tone but may be a measure of modulation of cardiac autonomic outflows by baroreflexes. Exp. Physiol. 2011, 96, 1255–1261. [Google Scholar] [CrossRef]
- Speer, K.E.; Semple, S.; Naumovski, N.; D’Cunha, N.M.; McKune, A.J. HPA axis function and diurnal cortisol in post-traumatic stress disorder: A systematic review. Neurobiol. Stress 2019, 11, 100180. [Google Scholar] [CrossRef] [PubMed]
- Bersani, F.S.; Wolkowitz, O.M.; Milush, J.M.; Sinclair, E.; Eppling, L.; Aschbacher, K.; Lindqvist, D.; Yehuda, R.; Flory, J.; Bierer, L.M.; et al. A population of atypical CD56(-)CD16(+) natural killer cells is expanded in PTSD and is associated with symptom severity. Brain Behav. Immun. 2016, 56, 264–270. [Google Scholar] [CrossRef]
- Penedo, F.J.; Dahn, J.R. Exercise and well-Being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef]
- Groer, M.W.; Kane, B.; Williams, S.N.; Duffy, A. Relationship of PTSD Symptoms With Combat Exposure, Stress, and Inflammation in American Soldiers. Biol. Res. Nurs. 2015, 17, 303–310. [Google Scholar] [CrossRef]
- Black, P.H. The inflammatory consequences of psychologic stress: Relationship to insulin resistance, obesity, atherosclerosis and diabetes mellitus, type II. Med. Hypotheses 2006, 67, 879–891. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Sherrington, C.; Tiedemann, A. Exercise augmentation compared with usual care for post-traumatic stress disorder: A randomized controlled trial. Acta Psychiatr. Scand. 2015, 131, 350–359. [Google Scholar] [CrossRef]
- Mazzeo, R.S.; Cavanagh, P.; Evans, W.J.; Fiatarone, M.; Hagberg, J.; McAuley, E.; Startzell, J. ACSM Position Stand: Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 1998, 30, 992–1008. [Google Scholar] [CrossRef]
- Gill, J.; Vythilingam, M.; Page, G.G. Low cortisol, high DHEA, and high levels of stimulated TNF-alpha, and IL-6 in women with PTSD. J. Trauma. Stress 2008, 21, 530–539. [Google Scholar] [CrossRef]
- Viljoen, M.; Claassen, N. Allostatic load and heart rate variability as health risk indicators. Afr. Health Sci. 2017, 17, 428–435. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Characteristics | PTSD | TEC | Total |
|---|---|---|---|
| (n = 4) | (n = 4) | (n = 8) | |
| Age (years) | 53.30 (13.94) | 47 (17.05) | 50.13 (14.80) |
| Mean (SD) | |||
| Ethnicity: Caucasian N (%) | 4 (100%) | 4 (100%) | 8 (100%) |
| Smoking status: non-smoker N (%) | 4 (100%) | 4 (100%) | 8 (100%) |
| Self-reported alcoholism N (%) | 0 (0%) | 0 (0%) | 0 (100%) |
| Type of trauma N (%) | |||
| Combat | 3 (37.5%) | 3 (37.5%) | 6 (75%) |
| Physical assault | 1 (12.5%) | 0 (0%) | 1 (12.5%) |
| Child brutality crime scene | 0 (0%) | 1 (12.5%) | 1 (12.5%) |
| Currently serving N (%) | 1 (12.5%) | 1 (12.5%) | 2 (25%) |
| BMI (kg/m2) | 28.43 (1.17) | 28.03 (2.91) | 28.23 (2.06) |
| Mean (SD) | |||
| Body fat (%) | 29.85 (2.88) | 32.05 (6.40) | 30.95 (4.74) |
| Mean (SD) | |||
| VO2max (mL/min/kg) * | 35.53 (3.40) | 34.50 (8.68) | 35.01 (6.13) |
| HR max (b/min) | 167 (14.90) | 177 (19.20) | 172 (16.78) |
| (during VO2max) | |||
| Mean (SD) | |||
| HR (b/min) | 123.25 (10.5) | 135.50 (18.45) | 129.38 (15.36) |
| (during boxing session) | |||
| Mean (SD) |
| Order | Boxing Combinations | Duration |
|---|---|---|
| 1 | Jab—Cross | 1 min |
| 2 | Left Hook—Right Hook | 1 min |
| 3 | Left Upper—Right Upper | 1 min |
| 4 | Break—standing with deep breathing | 1 min |
| 5 | Jab—Cross—Left Upper—Right Hook | 2 min |
| 6 | Break—standing with deep breathing | 1 min |
| 7 | Jab—Cross—Slip—Cross | 2 min |
| 8 | Break—standing with deep breathing | 1 min |
| 9 | Jab—Jab—Cross—Movement | 2 min |
| 10 | Finish with deep breathing | 1 min |
| Time | PTSD | Interpretation | TEC | Interpretation | |
|---|---|---|---|---|---|
| Cortisol (ug/dL) | Pre vs. IPE | 0.20 (−1.20, 1.60) | Unclear | 0.10 (−1.30, 1.50) | Unclear |
| Pre vs. 30 min | 0.60 (−0.90, 1.90) | Unclear | 0.10 (−1.30, 1.50) | Unclear | |
| Pre vs. 24 h | −0.10 (−1.50, 1.30) | Unclear | −0.70 (−2.10, 0.70) | Unclear | |
| Pre vs. 48 h | −0.10 (−1.30, 1.50) | Unclear | 0.40 (−1.0, 1.70) | Unclear | |
| CRP (pg/mL) | Pre vs. IPE | 0.13 (−1.26, 1.51) | Unclear | 0.65 (−0.77, 2.07) | Unclear |
| Pre vs. 30 min | 0.26 (−1.14, 1.65) | Unclear | 0.80 (−0.64, 2.23) | Unclear | |
| Pre vs. 24 h | −0.06 (−1.45, 1.33) | Unclear | 0.28 (−1.11, 1.67) | Unclear | |
| Pre vs. 48 h | −0.55 (−1.96, 0.86) | Unclear | 0.44 (−0.96, 1.85) | Unclear | |
| LnLF (ms2) | Pre vs. 5–10 min | -1.34 (−2.88, 0.19) | Large | −1.34 (−2.87, 0.19) | Large |
| Pre vs. 10–15 min | −2.12 (−3.85, −0.39) | Very Large | −1.24 (−2.75, 0.28) | Unclear | |
| Pre vs. 15–20 min | −2.85 (−4.81, −0.88) | Very Large | −0.97 (−2.44, 0.49) | Unclear | |
| Pre vs. 20–25 min | −3.63 (−5.88, −1.37) | Very Large | −0.91 (−2.37, 0.55) | Unclear | |
| Pre vs. 24 h | −0.37 (−1.77, 1.03) | Unclear | −0.39 (−1.79, 1.01) | Unclear | |
| Pre vs. 48 h | −1.37 (−2.91, 0.17) | Large | −0.41 (−1.81, 0.99) | Unclear | |
| LnHF (ms2) | Pre vs. 5–10 min | −1.69 (−3.3, −0.07) | Large | −1.73 (−3.35, −0.10) | Large |
| Pre vs. 10–15 min | −1.80 (−3.44, −0.16) | Large | −1.66 (−3.26, −0.05) | Large | |
| Pre vs. 15–20 min | −1.97 (−3.66, −0.28) | Large | −1.65 (−3.26, −0.05) | Large | |
| Pre vs. 20–25 min | −1.75 (−3.39, −0.12) | Large | −1.73 (−3.35, −0.10) | Large | |
| Pre vs. 24 h | −0.36 (−1.76, 1.03) | Unclear | −0.97 (−2.44, 0.50) | Unclear | |
| Pre vs. 48 h | −1.23 (−2.74, 0.28) | Unclear | −0.48 (−1.89, 0.93) | Unclear | |
| LnLF/HF | Pre vs. 5–10 min | 1.0 (−0.47, 2.47) | Unclear | 1.30 (−0.23, 2.82) | Unclear |
| Pre vs. 10–15 min | 0.86 (−0.59, 2.31) | Unclear | 0.74 (−0.69, 2.17) | Unclear | |
| Pre vs. 15–20 min | 0.44 (−0.96, 1.84) | Unclear | 0.96 (−0.50, 2.43) | Unclear | |
| Pre vs. 20–25 min | 0.30 (−1.09, 1.69) | Unclear | 1.09 (−0.40, 2.57) | Unclear | |
| Pre vs. 24 h | 0.21 (−1.18, 1.60) | Unclear | 0.68 (−0.75, 2.11) | Unclear | |
| Pre vs. 48 h | 0.45 (−0.95, 1.85) | Unclear | 0.03 (−1.36, 1.41) | Unclear | |
| LnRMSSD (ms) | Pre vs. 5–10 min | −2.52 (−4.38, −0.67) | Very Large | −1.61 (−3.20, −0.01) | Large |
| Pre vs. 10–15 min | −2.61 (−4.50, −0.73) | Very Large | −1.12 (−2.68, 0.32) | Unclear | |
| Pre vs. 15–20 min | −3.00 (−5.02, −0.98) | Very Large | −1.05 (−2.53, 0.43) | Unclear | |
| Pre vs. 20–25 min | −2.60 (−4.49, −0.72) | Very Large | 0.97 (−2.44, 0.49) | Unclear | |
| Pre vs. 24 h | −0.64 (−2.06, 0.78) | Unclear | −0.33 (−1.72, 1.07) | Unclear | |
| Pre vs. 48 h | −1.60 (−3.19, −0.01) | Large | −0.11 (−1.50, 1.27) | Unclear |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Speer, K.E.; Semple, S.; McKune, A.J. Acute Physiological Responses Following a Bout of Vigorous Exercise in Military Soldiers and First Responders with PTSD: An Exploratory Pilot Study. Behav. Sci. 2020, 10, 59. https://doi.org/10.3390/bs10020059
Speer KE, Semple S, McKune AJ. Acute Physiological Responses Following a Bout of Vigorous Exercise in Military Soldiers and First Responders with PTSD: An Exploratory Pilot Study. Behavioral Sciences. 2020; 10(2):59. https://doi.org/10.3390/bs10020059
Chicago/Turabian StyleSpeer, Kathryn E, Stuart Semple, and Andrew J McKune. 2020. "Acute Physiological Responses Following a Bout of Vigorous Exercise in Military Soldiers and First Responders with PTSD: An Exploratory Pilot Study" Behavioral Sciences 10, no. 2: 59. https://doi.org/10.3390/bs10020059
APA StyleSpeer, K. E., Semple, S., & McKune, A. J. (2020). Acute Physiological Responses Following a Bout of Vigorous Exercise in Military Soldiers and First Responders with PTSD: An Exploratory Pilot Study. Behavioral Sciences, 10(2), 59. https://doi.org/10.3390/bs10020059