Acute Sleep Curtailment Increases Sweet Taste Preference, Appetite and Food Intake in Healthy Young Adults: A Randomized Crossover Trial


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
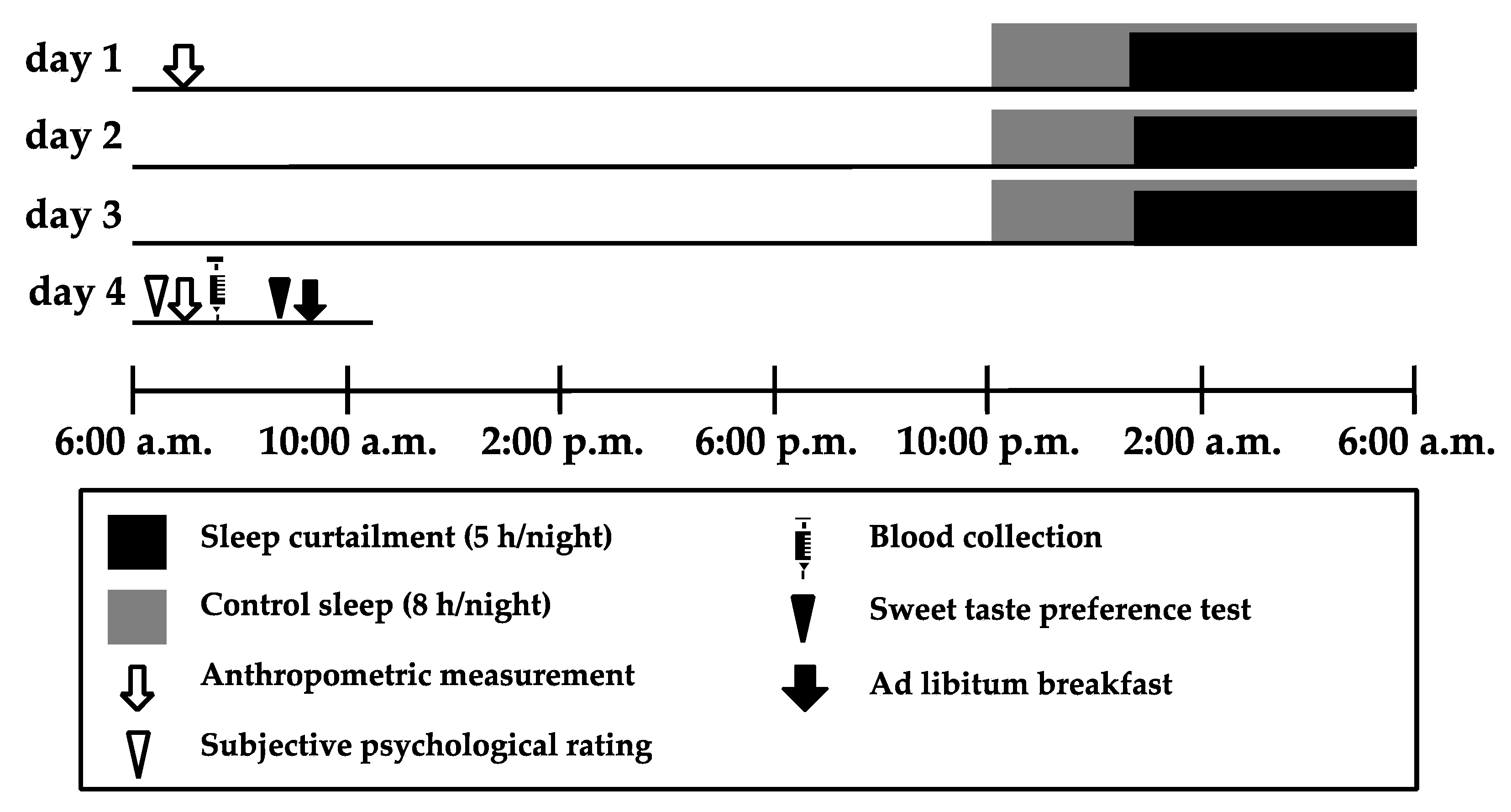
2.2. Study Design and Procedure
2.3. Sleep Assessment
2.4. Anthropometric Measurements
2.5. Subjective Psychological Rating
2.6. Blood Collection
2.7. Sweet Taste Preference Test
2.8. Ad libitum Breakfast
2.9. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Body Composition and Sleep Characteristics
3.3. Subjective Psychological Rating and Blood Biochemistry
3.4. Sweet Taste Preference
3.5. Food Intake during the Ad libitum Breakfast
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [PubMed]
- Nedeltcheva, A.V.; Scheer, F.A. Metabolic effects of sleep disruption, links to obesity and diabetes. Curr. Opin. Endocrinol. Diabetes Obes. 2014, 21, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Al Khatib, H.K.; Harding, S.V.; Darzi, J.; Pot, G.K. The effects of partial sleep deprivation on energy balance: A systematic review and meta-analysis. Eur. J. Clin. Nutr. 2017, 71, 614–624. [Google Scholar] [CrossRef] [PubMed]
- Nedeltcheva, A.V.; Kilkus, J.M.; Imperial, J.; Kasza, K.; Schoeller, D.A.; Penev, P.D. Sleep curtailment is accompanied by increased intake of calories from snacks. Am. J. Clin. Nutr. 2009, 89, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Spaeth, A.M.; Dinges, D.F.; Goel, N. Effects of Experimental Sleep Restriction on Weight Gain, Caloric Intake, and Meal Timing in Healthy Adults. Sleep 2013, 36, 981–990. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Roberts, A.L.; Chen, J.; Kelleman, M.; O’Keeffe, M.; RoyChoudhury, A.; Jones, P.J. Short sleep duration increases energy intakes but does not change energy expenditure in normal-weight individuals. Am. J. Clin. Nutr. 2011, 94, 410–416. [Google Scholar] [CrossRef]
- Markwald, R.R.; Melanson, E.L.; Smith, M.R.; Higgins, J.; Perreault, L.; Eckel, R.H.; Wright, K.P. Impact of insufficient sleep on total daily energy expenditure, food intake, and weight gain. Proc. Natl. Acad. Sci. USA 2013, 110, 5695–5700. [Google Scholar] [CrossRef]
- Broussard, J.L.; Kilkus, J.M.; Delebecque, F.; Abraham, V.; Day, A.; Whitmore, H.R.; Tasali, E. Elevated ghrelin predicts food intake during experimental sleep restriction. Obesity (Silver Spring) 2016, 24, 132–138. [Google Scholar] [CrossRef]
- St-Onge, M.P.; Wolfe, S.; Sy, M.; Shechter, A.; Hirsch, J. Sleep restriction increases the neuronal response to unhealthy food in normal-weight individuals. Int. J. Obes. (Lond.) 2014, 38, 411–416. [Google Scholar] [CrossRef]
- Tan, S.Y.; Tucker, R.M. Sweet Taste as a Predictor of Dietary Intake: A Systematic Review. Nutrients 2019, 11, 94. [Google Scholar] [CrossRef]
- Smith, S.L.; Ludy, M.J.; Tucker, R.M. Changes in taste preference and steps taken after sleep curtailment. Physiol. Behav. 2016, 163, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004, 1, e62. [Google Scholar] [CrossRef]
- Capers, P.L.; Fobian, A.D.; Kaiser, K.A.; Borah, R.; Allison, D.B. A systematic review and meta-analysis of randomized controlled trials of the impact of sleep duration on adiposity and components of energy balance. Obes. Rev. 2015, 16, 771–782. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Hinrichs, S.; Jauch-Chara, K.; Hitze, B.; Later, W.; Wilms, B.; Settler, U.; Peters, A.; Kiosz, D.; Muller, M.J. Influence of partial sleep deprivation on energy balance and insulin sensitivity in healthy women. Obes. Facts 2008, 1, 266–273. [Google Scholar] [CrossRef]
- Calvin, A.D.; Carter, R.E.; Adachi, T.; Macedo, P.G.; Albuquerque, F.N.; van der Walt, C.; Bukartyk, J.; Davison, D.E.; Levine, J.A.; Somers, V.K. Effects of experimental sleep restriction on caloric intake and activity energy expenditure. Chest 2013, 144, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Schmid, S.M.; Hallschmid, M.; Jauch-Chara, K.; Wilms, B.; Benedict, C.; Lehnert, H.; Born, J.; Schultes, B. Short-term sleep loss decreases physical activity under free-living conditions but does not increase food intake under time-deprived laboratory conditions in healthy men. Am. J. Clin. Nutr. 2009, 90, 1476–1482. [Google Scholar] [CrossRef]
- Klingenberg, L.; Chaput, J.P.; Holmbäck, U.; Jennum, P.; Astrup, A.; Sjödin, A. Sleep restriction is not associated with a positive energy balance in adolescent boys. Am. J. Clin. Nutr. 2012, 96, 240–248. [Google Scholar] [CrossRef]
- Shibui, K.; Uchiyama, M.; Okawa, M.; Kudo, Y.; Kim, K.; Kamei, Y.; Hayakawa, T.; Akamatsu, T.; Ohta, K.; Ishibashi, K. Diurnal fluctuation of sleep propensity across the menstrual cycle. Psychiatry Clin. Neurosci. 1999, 53, 207–209. [Google Scholar] [CrossRef]
- Gorczyca, A.M.; Sjaarda, L.A.; Mitchell, E.M.; Perkins, N.J.; Schliep, K.C.; Wactawski-Wende, J.; Mumford, S.L. Changes in macronutrient, micronutrient, and food group intakes throughout the menstrual cycle in healthy, premenopausal women. Eur. J. Nutr. 2016, 55, 1181–1188. [Google Scholar] [CrossRef]
- Matsuo, M.; Masuda, F.; Sumi, Y.; Takahashi, M.; Yamada, N.; Ohira, M.H.; Fujiwara, K.; Kanemura, T.; Kadotani, H. Comparisons of Portable Sleep Monitors of Different Modalities: Potential as Naturalistic Sleep Recorders. Front. Neurol. 2016, 7, 110. [Google Scholar] [CrossRef]
- Brondel, L.; Romer, M.A.; Nougues, P.M.; Touyarou, P.; Davenne, D. Acute partial sleep deprivation increases food intake in healthy men. Am. J. Clin. Nutr. 2010, 91, 1550–1559. [Google Scholar] [CrossRef] [PubMed]
- Asao, K.; Luo, W.; Herman, W.H. Reproducibility of the measurement of sweet taste preferences. Appetite 2012, 59, 927–932. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; McReynolds, A.; Trivedi, Z.B.; Roberts, A.L.; Sy, M.; Hirsch, J. Sleep restriction leads to increased activation of brain regions sensitive to food stimuli. Am. J. Clin. Nutr. 2012, 95, 818–824. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; O’Keeffe, M.; Roberts, A.L.; RoyChoudhury, A.; Laferrère, B. Short sleep duration, glucose dysregulation and hormonal regulation of appetite in men and women. Sleep 2012, 35, 1503–1510. [Google Scholar] [CrossRef]
- Nakazato, M.; Murakami, N.; Date, Y.; Kojima, M.; Matsuo, H.; Kangawa, K.; Matsukura, S. A role for ghrelin in the central regulation of feeding. Nature 2001, 409, 194–198. [Google Scholar] [CrossRef]
- Qian, J.; Morris, C.J.; Caputo, R.; Garaulet, M.; Scheer, F.A.J.L. Ghrelin is impacted by the endogenous circadian system and by circadian misalignment in humans. Int. J. Obes. (Lond.) 2018, 43, 1644–1649. [Google Scholar] [CrossRef]
- Tajiri, E.; Yoshimura, E.; Hatamoto, Y.; Tanaka, H.; Shimoda, S. Effect of sleep curtailment on dietary behavior and physical activity: A randomized crossover trial. Physiol. Behav. 2018, 184, 60–67. [Google Scholar] [CrossRef]
- McNeil, J.; St-Onge, M.P. Increased energy intake following sleep restriction in men and women: A one-size-fits-all conclusion? Obesity (Silver Spring) 2017, 25, 989–992. [Google Scholar] [CrossRef]
- Hanlon, E.C.; Tasali, E.; Leproult, R.; Stuhr, K.L.; Doncheck, E.; de Wit, H.; Hillard, C.J.; Van Cauter, E. Sleep Restriction Enhances the Daily Rhythm of Circulating Levels of Endocannabinoid 2-Arachidonoylglycerol. Sleep 2016, 39, 653–664. [Google Scholar] [CrossRef]
- McHill, A.W.; Hull, J.T.; McMullan, C.J.; Klerman, E.B. Chronic Insufficient Sleep Has a Limited Impact on Circadian Rhythmicity of Subjective Hunger and Awakening Fasted Metabolic Hormones. Front. Endocrinol. (Lausanne) 2018, 9, 319. [Google Scholar] [CrossRef]
- Herz, R.S.; Van Reen, E.; Barker, D.H.; Hilditch, C.J.; Bartz, A.L.; Carskadon, M.A. The Influence of Circadian Timing on Olfactory Sensitivity. Chem. Senses 2017, 43, 45–51. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 24) | Men (n = 11) | Women (n = 13) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 21.4 | ± | 1.0 | 21.5 | ± | 0.8 | 21.3 | ± | 0.8 |
| Body weight (kg) | 55.6 | ± | 7.2 | 61.0 | ± | 5.6 | 51.0 | ± | 5.0 |
| BMI (kg/m2) | 19.8 | ± | 1.7 | 20.5 | ± | 1.9 | 19.2 | ± | 1.1 |
| PSQI Score | 4.9 | ± | 1.8 | 5.5 | ± | 1.4 | 4.4 | ± | 1.9 |
| Bed time | 12:37 a.m. | ± | 0:47 | 12:51 a.m. | ± | 0:48 | 12:25 a.m. | ± | 0:43 |
| Wake-up time | 7:41 a.m. | ± | 0:44 | 8:05 a.m. | ± | 0:42 | 7:20 a.m. | ± | 0:35 |
| Time in bed (min/night) | 423 | ± | 38 | 433 | ± | 33 | 415 | ± | 40 |
| Total sleep time (min/night) | 408 | ± | 49 | 409 | ± | 52 | 407 | ± | 49 |
| Sleep efficiency (%) | 96.5 | ± | 9.2 | 94.4 | ± | 10.3 | 98.2 | ± | 8.3 |
| Habitual caffeine intake (mg/day) | 159 | ± | 105 | 184 | ± | 100 | 137 | ± | 109 |
| Habitual alcohol intake (mg/day) | 10 | ± | 26 | 20 | ± | 36 | 1 | ± | 1 |
| Chronotype (n, %) | |||||||||
| Moderate morning type | 2 | , | 8.3 | 1 | , | 9.1 | 1 | , | 7.7 |
| Intermediate type or neither type | 19 | , | 79.2 | 8 | , | 72.7 | 11 | , | 84.6 |
| Moderate evening type | 3 | , | 12.5 | 2 | , | 18.2 | 1 | , | 7.7 |
| Definite evening type or definite morning type | 0 | , | 0 | 0 | , | 0 | 0 | , | 0 |
| Sleep Curtailment Condition | Control Sleep Condition | F | P | |||||
|---|---|---|---|---|---|---|---|---|
| Bed time | 1:32 a.m. | ± | 0:31 | 10:43 p.m. | ± | 0:38 | 1566.676 | <0.001 |
| Sleep-onset time | 1:43 a.m. | ± | 0:31 | 10:58 p.m. | ± | 0:38 | 751.825 | <0.001 |
| Awakening time | 6:48 a.m. | ± | 0:35 | 6:48 a.m. | ± | 0:40 | 0.057 | 0.814 |
| Getting-up time | 6:54 a.m. | ± | 0:34 | 6:56 a.m. | ± | 0:40 | 0.208 | 0.653 |
| Sleep period time (min/day) | 304 | ± | 20 | 471 | ± | 22 | 1030.272 | <0.001 |
| Time in bed (min/day) | 321 | ± | 16 | 493 | ± | 19 | 2251.343 | <0.001 |
| Sleep Curtailment Condition | Control Sleep Condition | |||||||
|---|---|---|---|---|---|---|---|---|
| Ave | ± | SD | Ave | ± | SD | F | P | |
| Subjective psychological ratings | ||||||||
| Hungry (cm) | 6.0 | ± | 2.6 | 5.4 | ± | 2.3 | 3.284 | 0.084 |
| Appetite (cm) | 5.4 | ± | 2.6 | 5.4 | ± | 1.8 | 0.001 | 0.976 |
| Desire to sweets (cm) | 4.2 | ± | 2.2 | 4.4 | ± | 2.4 | 0.482 | 0.495 |
| Desire to fatty foods (cm) | 3.5 | ± | 2.6 | 2.7 | ± | 2.4 | 2.129 | 0.159 |
| Sleepiness (cm) | 6.4 | ± | 2.1 | 3.0 | ± | 2.4 | 47.015 | <0.001 |
| Fatigue (cm) | 5.6 | ± | 2.1 | 2.8 | ± | 2.2 | 38.574 | <0.001 |
| Blood biochemistry | ||||||||
| Active ghrelin (fmol/ml)* | 22.8 | ± | 10.6 | 20.1 | ± | 8.7 | 5.020 | 0.035 |
| Leptin (ng/ml) | 17.4 | ± | 10.6 | 17.4 | ± | 10.9 | 0.005 | 0.946 |
| Ad libitum food intake | ||||||||
| Energy intake (kcal) | 788 | ± | 384 | 674 | ± | 281 | 6.547 | 0.018 |
| Protein (kcal) | 88 | ± | 52 | 76 | ± | 40 | 3.081 | 0.093 |
| Fat (kcal) | 308 | ± | 173 | 272 | ± | 149 | 3.287 | 0.083 |
| Carbohydrate (kcal) | 397 | ± | 187 | 330 | ± | 120 | 8.109 | 0.009 |
| P (%/Energy) | 10.9 | ± | 2.1 | 11.1 | ± | 2.2 | 0.183 | 0.673 |
| F (%/Energy) | 38.4 | ± | 6.9 | 39.7 | ± | 7.8 | 0.846 | 0.367 |
| C (%/Energy) | 51.5 | ± | 7.7 | 49.7 | ± | 8.0 | 1.210 | 0.283 |
| Weight of food intake (g) | 573 | ± | 256 | 492 | ± | 193 | 4.674 | 0.041 |
| Weight of macronutrient intake (g) | 155 | ± | 74 | 132 | ± | 52 | 7.189 | 0.013 |
| Energy density (kcal/g) | 1.4 | ± | 0.3 | 1.4 | ± | 0.3 | 0.058 | 0.812 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tajiri, E.; Yoshimura, E.; Hatamoto, Y.; Shiratsuchi, H.; Tanaka, S.; Shimoda, S. Acute Sleep Curtailment Increases Sweet Taste Preference, Appetite and Food Intake in Healthy Young Adults: A Randomized Crossover Trial. Behav. Sci. 2020, 10, 47. https://doi.org/10.3390/bs10020047
Tajiri E, Yoshimura E, Hatamoto Y, Shiratsuchi H, Tanaka S, Shimoda S. Acute Sleep Curtailment Increases Sweet Taste Preference, Appetite and Food Intake in Healthy Young Adults: A Randomized Crossover Trial. Behavioral Sciences. 2020; 10(2):47. https://doi.org/10.3390/bs10020047
Chicago/Turabian StyleTajiri, Eri, Eiichi Yoshimura, Yoichi Hatamoto, Hideki Shiratsuchi, Shigeho Tanaka, and Seiya Shimoda. 2020. "Acute Sleep Curtailment Increases Sweet Taste Preference, Appetite and Food Intake in Healthy Young Adults: A Randomized Crossover Trial" Behavioral Sciences 10, no. 2: 47. https://doi.org/10.3390/bs10020047
APA StyleTajiri, E., Yoshimura, E., Hatamoto, Y., Shiratsuchi, H., Tanaka, S., & Shimoda, S. (2020). Acute Sleep Curtailment Increases Sweet Taste Preference, Appetite and Food Intake in Healthy Young Adults: A Randomized Crossover Trial. Behavioral Sciences, 10(2), 47. https://doi.org/10.3390/bs10020047