Female Gender Is Associated with an Increased Left Ventricular Ejection Fraction Recovery in Patients with Heart Failure with Reduced Ejection Fraction

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- (1)
- Cohort studies (prospective or retrospective), case–control studies, cross-sectional studies, and randomized control trials conducted in HFrEF populations that reported the number of participants who had LVEF recovery, separated by gender.
- (2)
- Odds ratio (OR) with 95% confidence interval (CI), or sufficient raw data to perform the calculations were provided. Patients without LVEF recovery were used as controls.
- (1)
- Authors did not report criteria for LVEF recovery, or used parameters other than LVEF to define LVEF recovery;
- (2)
- Studies were conducted exclusively in an HF population who had received cardiac resynchronization therapy (CRT);
- (3)
- Studies were conducted in patients with left ventricular assist devices or heart transplant recipients;
- (4)
- Studies did not report the effect size in their analysis, or there was insufficient data to calculate the effect size.
2.3. Data Extraction
2.4. Definition
2.5. Statistical Analysis
3. Results
3.1. Search Results
3.2. Description of Included Studies
3.3. Quality Assessment of Included Studies
3.4. Meta-Analysis Results
3.4.1. Female and LVEF Recovery
3.4.2. Sensitivity Analysis
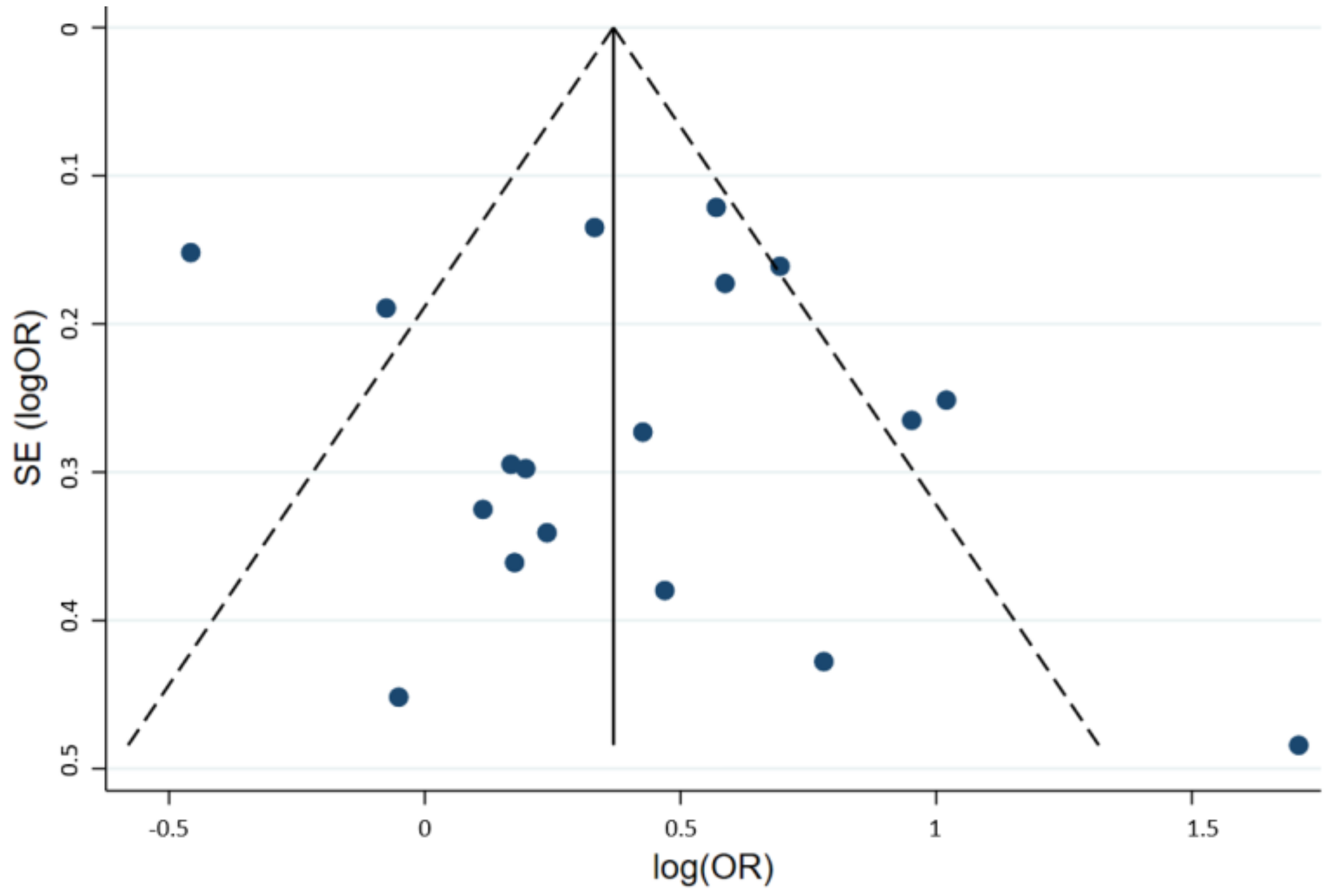
3.4.3. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| HF | Heart Failure |
| LVEF | Left ventricular ejection fraction |
| OR | Odds ratio |
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef] [PubMed]
- Basuray, A.; French, B.; Ky, B.; Vorovich, E.; Olt, C.; Sweitzer, N.K.; Cappola, T.P.; Fang, J.C. Heart failure with recovered ejection fraction: Clinical description, biomarkers, and outcomes. Circulation 2014, 129, 2380–2387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilcox, J.E.; Fang, J.C.; Margulies, K.B.; Mann, D.L. Heart Failure with Recovered Left Ventricular Ejection Fraction: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2020, 76, 719–734. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, J.E.; Yancy, C.W. Heart Failure—A New Phenotype Emerges. JAMA Cardiol. 2016, 1, 507–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorodeski, E.Z.; Magnelli-Reyes, C.; Moennich, L.A.; Grimaldi, A.; Rickard, J. Cardio Resynchronization Therapy-heart failure (CRT-HF) clinic: A Novel Model of Care. PLoS ONE 2019, 14, e0222610. [Google Scholar] [CrossRef]
- Wilcox, J.E.; Fonarow, G.C.; Yancy, C.W.; Albert, N.M.; Curtis, A.B.; Heywood, J.T.; Inge, P.J.; McBride, M.L.; Mehra, M.R.; O’Connor, C.M.; et al. Factors associated with improvement in ejection fraction in clinical practice among patients with heart failure: Findings from IMPROVE HF. Am. Heart J. 2012, 163, 49–56.e42. [Google Scholar] [CrossRef]
- Punnoose, L.R.; Givertz, M.M.; Lewis, E.F.; Pratibhu, P.; Stevenson, L.W.; Desai, A.S. Heart failure with recovered ejection fraction: A distinct clinical entity. J. Card. Fail. 2011, 17, 527–532. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Roger, V.L.; Weston, S.A.; Jiang, R.; Redfield, M.M. Longitudinal changes in ejection fraction in heart failure patients with preserved and reduced ejection fraction. Circ. Heart Fail. 2012, 5, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Kramer, D.G.; Trikalinos, T.A.; Kent, D.M.; Antonopoulos, G.V.; Konstam, M.A.; Udelson, J.E. Quantitative evaluation of drug or device effects on ventricular remodeling as predictors of therapeutic effects on mortality in patients with heart failure and reduced ejection fraction: A meta-analytic approach. J. Am. Coll. Cardiol. 2010, 56, 392–406. [Google Scholar] [CrossRef] [Green Version]
- Kalogeropoulos, A.P.; Fonarow, G.C.; Georgiopoulou, V.; Burkman, G.; Siwamogsatham, S.; Patel, A.; Li, S.; Papadimitriou, L.; Butler, J. Characteristics and Outcomes of Adult Outpatients with Heart Failure and Improved or Recovered Ejection Fraction. JAMA Cardiol. 2016, 1, 510–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanabe, K.; Sakamoto, T. Heart failure with recovered ejection fraction. J. Echocardiogr. 2019, 17, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Yancy, C.W.; Albert, N.M.; Curtis, A.B.; Stough, W.G.; Gheorghiade, M.; Heywood, J.T.; Mehra, M.; O’Connor, C.M.; Reynolds, D.; et al. Improving the use of evidence-based heart failure therapies in the outpatient setting: The IMPROVE HF performance improvement registry. Am. Heart J. 2007, 154, 12–38. [Google Scholar] [CrossRef] [PubMed]
- Lupon, J.; Diez-Lopez, C.; de Antonio, M.; Domingo, M.; Zamora, E.; Moliner, P.; Gonzalez, B.; Santesmases, J.; Troya, M.I.; Bayes-Genis, A. Recovered heart failure with reduced ejection fraction and outcomes: A prospective study. Eur. J. Heart Fail. 2017, 19, 1615–1623. [Google Scholar] [CrossRef] [PubMed]
- Kenchaiah, S.; Vasan, R.S. Heart Failure in Women—Insights from the Framingham Heart Study. Cardiovasc. Drugs Ther. 2015, 29, 377–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunlay, S.M.; Roger, V.L.; Redfield, M.M. Epidemiology of heart failure with preserved ejection fraction. Nat. Rev. Cardiol. 2017, 14, 591–602. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Patsopoulos, N.A.; Evangelou, E.; Ioannidis, J.P. Sensitivity of between-study heterogeneity in meta-analysis: Proposed metrics and empirical evaluation. Int. J. Epidemiol. 2008, 37, 1148–1157. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Abe, S.; Yoshihisa, A.; Ichijo, Y.; Sato, Y.; Kanno, Y.; Takiguchi, M.; Yokokawa, T.; Misaka, T.; Sato, T.; Oikawa, M.; et al. Recovered Left Ventricular Ejection Fraction and Its Prognostic Impacts in Hospitalized Heart Failure Patients with Reduced Ejection Fraction. Int. Heart J. 2020, 61, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Agra Bermejo, R.; Gonzalez Babarro, E.; Lopez Canoa, J.N.; Varela Roman, A.; Gomez Otero, I.; Oro Ayude, M.; Parada Vazquez, P.; Gomez Rodriguez, I.; Diaz Castro, O.; Gonzalez Juanatey, J.R. Heart failure with recovered ejection fraction: Clinical characteristics, determinants and prognosis. CARDIOCHUS-CHOP registry. Cardiol. J. 2018, 25, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.W.; Beri, N.; Nguyen, N.H.; Arbit, B.; Fox, S.; Mojaver, S.; Clopton, P.; Tam, S.W.; Taylor, A.L.; Cohn, J.N.; et al. Heart Failure with Recovered Ejection Fraction in African Americans: Results from the African-American Heart Failure Trial. J. Card. Fail. 2018, 24, 303–309. [Google Scholar] [CrossRef]
- Chang, H.Y.; Chen, K.C.; Fong, M.C.; Feng, A.N.; Fu, H.N.; Huang, K.C.; Chong, E.; Yin, W.H. Recovery of left ventricular dysfunction after sacubitril/valsartan: Predictors and management. J. Cardiol. 2020, 75, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Florea, V.G.; Rector, T.S.; Anand, I.S.; Cohn, J.N. Heart Failure with Improved Ejection Fraction: Clinical Characteristics, Correlates of Recovery, and Survival: Results from the Valsartan Heart Failure Trial. Circ. Heart Fail. 2016, 9, e003123. [Google Scholar] [CrossRef] [PubMed]
- Howlett, J.G.; Sharma, N.; Alemayehu, W.G.; Dyck, J.R.B.; Anderson, T.; Fine, N.; Becker, H.; White, J.A.; Paterson, D.I.; Thompson, R.B.; et al. Circulating troponin and further left ventricular ejection fraction improvement in patients with previously recovered left ventricular ejection fraction. ESC Heart Fail. 2020, 7, 2725–2733. [Google Scholar] [CrossRef]
- Pereira, J.; Chaves, V.; Tavares, S.; Albuquerque, I.; Gomes, C.; Guiomar, V.; Monteiro, A.; Ferreira, I.; Lourenco, P.; Bettencourt, P. Systolic function recovery in Heart Failure: Frequency, prognostic impact and predictors. Int. J. Cardiol. 2020, 300, 172–177. [Google Scholar] [CrossRef]
- Swat, S.A.; Cohen, D.; Shah, S.J.; Lloyd-Jones, D.M.; Baldridge, A.S.; Freed, B.H.; Vorovich, E.E.; Yancy, C.W.; Jonnalagadda, S.R.; Prenner, S.; et al. Baseline Longitudinal Strain Predicts Recovery of Left Ventricular Ejection Fraction in Hospitalized Patients with Nonischemic Cardiomyopathy. J. Am. Heart Assoc. 2018, 7, e09841. [Google Scholar] [CrossRef] [Green Version]
- Trullas, J.C.; Manzano, L.; Formiga, F.; Aramburu-Bodas, O.; Quesada-Simon, M.A.; Arias-Jimenez, J.L.; Garcia-Escriva, D.; Romero-Requena, J.M.; Jordana-Comajuncosa, R.; Montero-Perez-Barquero, M.; et al. Heart Failure with Recovered Ejection Fraction in a Cohort of Elderly Patients with Chronic Heart Failure. Cardiology 2016, 135, 196–201. [Google Scholar] [CrossRef]
- Shah, M.A.; Soofi, M.A.; Jafary, Z.; Alhomrani, A.; Alsmadi, F.; Wani, T.A.; Bajwa, I.A. Echocardiographic parameters associated with recovery in heart failure with reduced ejection fraction. Echocardiography 2020, 37, 1574–1582. [Google Scholar] [CrossRef] [PubMed]
- Torii, Y.; Kusunose, K.; Hirata, Y.; Nishio, S.; Ise, T.; Yamaguchi, K.; Fukuda, D.; Yagi, S.; Yamada, H.; Soeki, T.; et al. Left Atrial Strain Associated with Functional Recovery in Patients Receiving Optimal Treatment for Heart Failure. J. Am. Soc. Echocardiogr. 2021, 34, 966–975.e962. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.F.; Li, X.L.; Wang, S.M.; Wang, Y.F.; Zheng, Y.R.; Wang, L.H. Body Mass Index: An Effective Predictor of Ejection Fraction Improvement in Heart Failure. Front. Cardiovasc. Med. 2021, 8, 586240. [Google Scholar] [CrossRef] [PubMed]
- Zeller, J.; Hubauer, U.; Schober, A.; Schober, A.; Keyser, A.; Fredersdorf, S.; Uecer, E.; Maier, L.S.; Jungbauer, C. Heart failure with recovered ejection fraction (HFrecEF): A new entity with improved cardiac outcome. Pacing Clin. Electrophysiol. 2021, 44, 2015–2023. [Google Scholar] [CrossRef]
- Zhang, X.; Sun, Y.; Zhang, Y.; Chen, F.; Dai, M.; Si, J.; Yang, J.; Li, X.; Li, J.; Xia, Y.; et al. Characteristics and outcomes of heart failure with recovered left ventricular ejection fraction. ESC Heart Fail. 2021, 8, 5383–5391. [Google Scholar] [CrossRef]
- Aggarwal, N.R.; Patel, H.N.; Mehta, L.S.; Sanghani, R.M.; Lundberg, G.P.; Lewis, S.J.; Mendelson, M.A.; Wood, M.J.; Volgman, A.S.; Mieres, J.H. Sex Differences in Ischemic Heart Disease: Advances, Obstacles, and Next Steps. Circ. Cardiovasc. Qual. Outcomes 2018, 11, e004437. [Google Scholar] [CrossRef]
- Sobhani, K.; Nieves Castro, D.K.; Fu, Q.; Gottlieb, R.A.; Van Eyk, J.E.; Noel Bairey Merz, C. Sex differences in ischemic heart disease and heart failure biomarkers. Biol. Sex Differ. 2018, 9, 43. [Google Scholar] [CrossRef]
- Mendirichaga, R.; Jacobs, A.K. Sex Differences in Ischemic Heart Disease-the Paradox Persists. JAMA Cardiol. 2020, 5, 754–756. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Country | Total Participants, Female (%) | Mean Age | Definition of HFrEF and LVEF Value for Recovered EF | Participants with Recovered LVEF (n, %) | Ischemic Cardiomyopathy (n, %) | Revascularization Methods (n, %) | Participants on Beta-Blocker (n, %) | Participants on ACEI/ARB (n, %) | Participants on MRA (n, %) | Mean LVEF (%) | Mean Follow-Up Time (Months) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HFrecEF | HFperEF | HFrecEF | HFperEF | HFrecEF | HFperEF | HFrecEF | HFperEF | HFrecEF | HFperEF | HFrecEF | HFperEF | |||||||
| Abe, 2020 | Japan | 567, 28% | 64.9 ± 14.6 | LVEF < 40% with LVEF ≥ 50% at follow-up via Simpson’s method in 4C view | 250, 44% | 72, 28.8% | 88, 37.4% | PCI 67, 26.8% | PCI 65, 27.7% | 230, 92.0% | 211, 89.8% | 216, 86.4% | 187, 79.6% | 130, 52.0% | 119, 50.6% | 33.2 ± 5.7 | 28.5.2 ± 7.3 | 40 ± 26.9 |
| Basury, 2014 | USA | 1699, 32% | 56.1 ± 13.9 | LVEF < 50% with LVEF ≥ 50% at follow-up | 176, 8.4% | 29, 16.0% | 545, 36.0% | PCI 26, 15%; CABG 18, 10% | PCI 348, 23%; CABG 321, 21% | 154, 88.0% | 1399, 92.0% | 149, 85.0% | 1371, 90.0% | 35, 20.0% | 580, 38.0% | N/A | N/A | 32.7 ± 27.4 |
| Bermejo, 2018 | Spain | 242, 25% | 64.4 ± 12.1 | LVEF ≤ 40% with LVEF > 40% after 12 months via Simpson’s method | 126, 53.1% | 25, 19.8% | 57, 49.1% | PCI 12, 9.5%; CABG 9, 7.1% | PCI 29, 25%; CABG 14, 12.1% | 98, 77.8% | 97, 83.6% | 113, 90.4% | 102, 87.9% | 52, 41.3% | 63, 54.3% | 31.3 ± 6.1 | 29.1 ± 7.3 | 60 ± 30 |
| Chang KW, 2018 | USA | 318, 37.4% | 57 ± 12.7 | LVEF < 35% with LVEF > 40% after 6 months | 59, 18.6% | 15, 25.4% | 77, 29.7% | n/a | n/a | 51, 86.4% | 203, 78.4% | 52, 88.1% | 241, 93.1% | 25, 42.4% | 115, 44.4% | 29.9 ± 3.9 | 26.7 ± 5.7 | 6 |
| Chang HY, 2020 | Taiwan | 437, 25.4% | 61.2 ± 14.5 | LVEF < 40% with LVEF ≥ 50% after 6 months via biplane Simpson’s method | 77, 17.6% | 17, 22.1% | 160, 44.4% | n/a | n/a | 66, 85.7% | 300, 83.3% | 56, 72.7% | 265, 73.6% | 47, 61.0% | 263, 73.1% | 29.3 ± 8 | 26.5 ± 6.4 | 18.5 ± 4.5 |
| Florea, 2016 | USA | 3519, 20.5% | 61.9 ± 11 | LVEF < 35% with LVEF > 40% after 12 months via biplane Simpson’s method | 321, 9.1% | 119, 37.0% | 1791, 56.0% | n/a | n/a | 151, 47.0% | 1087, 34.0% | 298, 93.0% | 2974, 93.0% | 13, 4.0% | 160, 5.0% | 28.7 ± 5.6 | 25.2 ± 6.2 | 12 |
| Howlett, 2020 | Canada | 151, 24.5% | 65.2 ± 13.5 | LVEF < 35% with LVEF > 35% and absolute increase ≥5% after 12 months via biplane Simpson’s method | 95, 62.9% | 32, 33.7% | 32, 57.1% | PCI 19, 20%, CABG 10, 10.5% | PCI 22, 39.3%, CABG 14, 25% | 93, 97.9% | 55, 98.2% | 85, 89.5% | 52, 92.9% | N/A | N/A | 44.8 ± 1 | 24.7 ± 1.2 | 12 |
| Kalogeropoulos 2016 | USA | 1700, 37.1% | 64.7 ± 15.6 | LVEF ≤ 40% with LVEF > 40% at follow-up | 350, 20.6% | N/A | N/A | n/a | n/a | 310, 88.7% | 1180, 87.4% | 277, 79.1% | 1002, 74.2% | N/A | N/A | 25.3 ± 11.2 | 25.3 ± 11.1 | 32.3 ± 11.3 |
| Lupon, 2017 | Spain | 940, 21.6% | 65 ± 11.7 | LVEF < 45% with LVEF ≥ 45% after 12 months via biplane Simpson’s method | 233, 4.8% | 82, 35.2% | 453, 64.1% | n/a | n/a | 217, 93.1% | 669, 94.6% | 216, 92.7% | 669, 94.6% | 130, 55.8% | 474, 67.0% | 31.3 ± 7.7 | 28.2 ± 7.8 | 67.2 ± 37.2 |
| Pereira, 2019 | Portugal | 304, 28.9% | 66 ± 14 | LVEF < 40% with LVEF ≥ 40% during follow-up | 154, 50.7% | 39, 25.3% | 69, 46.0% | n/a | n/a | 152, 97.3% | 146, 98.7% | 147, 95.5% | 142, 94.7% | 77, 50.0% | 8758.0% | 25 ± 8 | 25.7 ± 8.7 | 60 ± 39.5 |
| Punnoose, 2011 | USA | 302, 33.4% | 57.4 ± 14.1 | LVEF < 40% with LVEF ≥ 40% and absolute increase ≥5% at follow-up | 121, 39.8% | 21, 17.0% | 57, 31.0% | n/a | n/a | 99, 82.0% | 157, 87.0% | 98, 81.0% | 146, 81.0% | 23, 19.0% | 68, 38.0% | 25 ± 8 | 28 ± 12 | 54 ± 57 |
| Shah, 2020 | Saudi Arabia | 136, 29.4% | 53.6 ± 14 | LVEF < 40% with LVEF > 40% with absolute increase ≥10% at follow-up via Simpson’s method | 67, 49.2% | 9, 13.4% | 33, 47.8% | n/a | n/a | 61, 91.0% | 62, 89.9% | 60, 89.6% | 60, 86.9% | 1, 1.4% | 0.0% | 26.4 ± 5.75 | 25.06 ± 7.06 | 11 |
| Swat, 2018 | USA | 166, 52.4% | 54.3 ± 15.6 | LVEF < 40% with LVEF ≥ 40% with absolute increase≥10% within 18 months via longitudinal strain | 59, 35.5% | 0.0% | 0.0% | 0.0% | 0.0% | 40, 68.0% | 65, 61.0% | 38, 64.0% | 64, 60.0% | 9, 15.0% | 23, 21.0% | 26.4 ± 7.4 | 24.6 ± 8.0 | 35.9 ± 36 |
| Trullas, 2016 | Spain | 108, 41.7% | 73.1 ± 10.2 | LVEF < 50% with LVEF > 50% with absolute increase ≥5% during follow-up | 27, 25% | 18, 67.0% | 46, 57.0% | n/a | n/a | 19, 70.0% | 61, 75.0% | 21, 78.0% | 60, 74.0% | 6, 22.0% | 29, 36.0% | 35.3 ± 11.4 | 31.7 ± 8.3 | median 12 |
| Torii, 2021 | Japan | 100, 30% | 67 ± 14 | LVEF < 40% with LVEF ≥ 40% with absolute increase ≥10% at 6 months via biplane Simpson’s method | 28, 28% | 7, 25.0% | 24, 33.0% | PCI 7, 25% | PCI 12, 17% | 27, 96.0% | 66, 92.0% | 20, 71.0% | 49, 68.0% | 18, 64.0% | 41, 57.0% | 32 ± 4 | 26 ± 5 | 24 ± 13 |
| Ye, 2021 | China | 184, 21.2% | 62.1 ± 17.9 | LVEF < 40% with LVEF ≥ 40% after 6 months via Simpson’s method in 4C view | 88, 21.2% | 15, 17.0% | 14, 14.6% | n/a | n/a | 77, 87.5% | 85, 88.5% | 71, 80.7% | 79, 82.3% | 73, 83.0% | 87, 90.6% | 32.5 ± 6 | 30.7 ± 6 | 6 |
| Zeller, 2021 | Germany | 237, 20.3% | 67.4 ± 14.1 | LVEF < 40% with LVEF ≥ 40% during follow-up via biplane Simpson’s method | 74, 31.2% | 29, 39.2% | 93, 57.1% | n/a | n/a | 64, 86.5% | 152, 93.3% | 67, 90.5% | 139, 85.3% | 54, 73.0% | 117, 71.8% | 31 ± 9 | 30 ± 9 | 45.6 ± 28.8 |
| Zhang, 2021 | China | 1160, 29.8% | 61.9 ± 13.3 | LVEF < 40% with LVEF ≥ 40% with absolute increase ≥10% after 3 months | 284, 26.4% | 86, 30.3% | 382, 43.6% | n/a | n/a | 273, 96.1% | 830, 94.8% | 233, 82.0% | 671, 76.6% | 160, 56.3% | 626, 71.5% | n/a | n/a | 35 ± 20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kewcharoen, J.; Trongtorsak, A.; Thangjui, S.; Kanitsoraphan, C.; Prasitlumkum, N. Female Gender Is Associated with an Increased Left Ventricular Ejection Fraction Recovery in Patients with Heart Failure with Reduced Ejection Fraction. Med. Sci. 2022, 10, 21. https://doi.org/10.3390/medsci10020021
Kewcharoen J, Trongtorsak A, Thangjui S, Kanitsoraphan C, Prasitlumkum N. Female Gender Is Associated with an Increased Left Ventricular Ejection Fraction Recovery in Patients with Heart Failure with Reduced Ejection Fraction. Medical Sciences. 2022; 10(2):21. https://doi.org/10.3390/medsci10020021
Chicago/Turabian StyleKewcharoen, Jakrin, Angkawipa Trongtorsak, Sittinun Thangjui, Chanavuth Kanitsoraphan, and Narut Prasitlumkum. 2022. "Female Gender Is Associated with an Increased Left Ventricular Ejection Fraction Recovery in Patients with Heart Failure with Reduced Ejection Fraction" Medical Sciences 10, no. 2: 21. https://doi.org/10.3390/medsci10020021
APA StyleKewcharoen, J., Trongtorsak, A., Thangjui, S., Kanitsoraphan, C., & Prasitlumkum, N. (2022). Female Gender Is Associated with an Increased Left Ventricular Ejection Fraction Recovery in Patients with Heart Failure with Reduced Ejection Fraction. Medical Sciences, 10(2), 21. https://doi.org/10.3390/medsci10020021