
Study on the Interaction between Serum Thyrotropin and Semen Parameters in Men


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
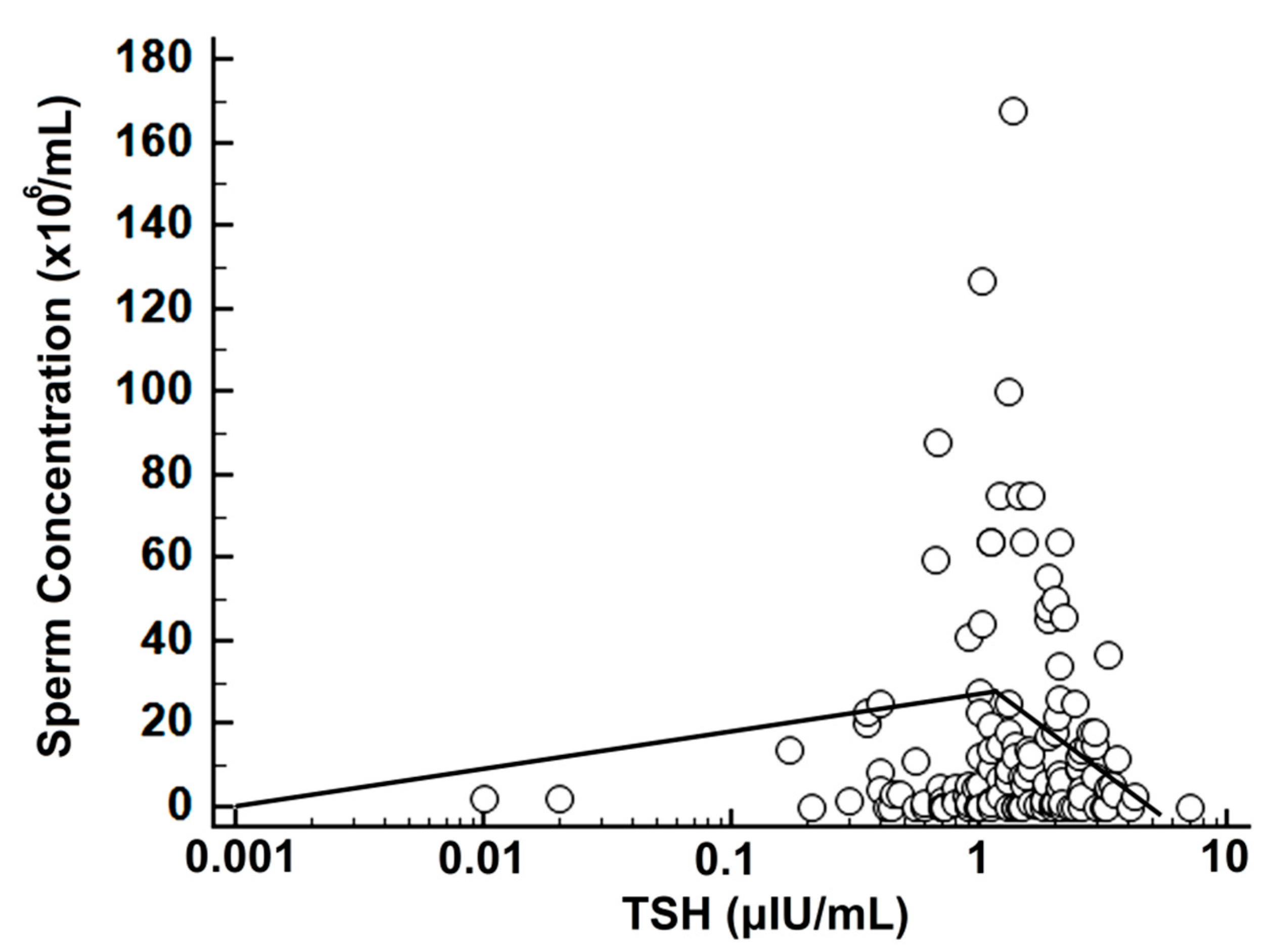
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- La Vignera, S.; Vita, R. Thyroid dysfunction and semen quality. Int. J. Immunopathol. Pharmacol. 2018, 32, 2058738418775241. [Google Scholar] [CrossRef] [PubMed]
- Rajender, S.; Monica, M.G.; Walter, L.; Agarwal, A. Thyroid, spermatogenesis, and male infertility. Front. Biosci. 2011, 3, 843–855. [Google Scholar] [CrossRef]
- Patel, N.; Kashanian, J.A. Thyroid Dysfunction and Male Reproductive Physiology. Semin. Reprod. Med. 2016, 34, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.; Martinez, M.E. Thyroid hormone action in the developing testis: Intergenerational epigenetics. J. Endocrinol. 2020, 244, R33–R46. [Google Scholar] [CrossRef]
- Ni, F.D.; Hao, S.L.; Yang, W.X. Molecular insights into hormone regulation via signaling pathways in Sertoli cells: With discussion on infertility and testicular tumor. Gene 2020, 753, 144812. [Google Scholar] [CrossRef]
- Castañeda Cortés, D.C.; Langlois, V.S.; Fernandino, J.I. Crossover of the hypothalamic pituitary-adrenal/interrenal, -thyroid, and -gonadal axes in testicular development. Front. Endocrinol. 2014, 5, 139. [Google Scholar] [CrossRef] [Green Version]
- Krassas, G.E.; Poppe, K.; Glinoer, D. Thyroid function and human reproductive health. Endocr Rev. 2010, 31, 702–755. [Google Scholar] [CrossRef] [Green Version]
- UNDP; UNFPA; WHO; HRP; RHR. WHO Laboratory Manual for the Examination and Processing of Human Semen; Department of Reproductive Health and Research, World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- LeFevre, M.L. Screening for thyroid dysfunction: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2015, 162, 641–650. [Google Scholar] [CrossRef] [Green Version]
- Hao, L.; Naiman, D.Q. Quantile Regression; Sage Publications: Thousand Oaks, CA, USA, 2007; Volume 149. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Earlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd ed.; Routledge: New York, NY, USA, 2003. [Google Scholar]
- Nicopoulou, S.C.; Alexiou, M.; Michalakis, K.; Ilias, I.; Venaki, E.; Koukkou, E.; Mitios, G.; Billa, E.; Adamopoulos, D.A. Body mass index vis-à-vis total sperm count in attendees of a single andrology clinic. Fertil. Steril. 2009, 92, 1016–1017. [Google Scholar] [CrossRef]
- Sheehan, M.T. Biochemical Testing of the Thyroid: TSH is the Best and, Oftentimes, Only Test Needed—A Review for Primary Care. Clin. Med. Res. 2016, 14, 83–92. [Google Scholar] [CrossRef] [Green Version]
- Fujisawa, M.; Kanzaki, M.; Hayashi, A.; Tanaka, H.; Okada, H.; Arakawa, S.; Kamidono, S. Alteration of the hypothalamus-pituitary-testis axis in oligozoospermic men with normal gonadotropin levels. Int. J. Urol. 1995, 2, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Heuer, H.; Visser, T.J. Minireview: Pathophysiological importance of thyroid hormone transporters. Endocrinology 2009, 150, 1078–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, A.; Shekhar, S.; Dhole, B. Thyroid and male reproduction. Indian J. Endocrinol. Metab. 2014, 18, 23–31. [Google Scholar] [CrossRef] [PubMed]
- de Kretser, D.M.; Loveland, K.L.; Meinhardt, A.; Simorangkir, D.; Wreford, N. Spermatogenesis. Hum. Reprod. 1998, 13 (Suppl. 1), 1–8. [Google Scholar] [CrossRef] [Green Version]
- Sofikitis, N.; Giotitsas, N.; Tsounapi, P.; Baltogiannis, D.; Giannakis, D.; Pardalidis, N. Hormonal regulation of spermatogenesis and spermiogenesis. J. Steroid. Biochem. Mol. Biol. 2008, 109, 323–330. [Google Scholar] [CrossRef]
- Griswold, M.D. The central role of Sertoli cells in spermatogenesis. Semin. Cell Dev. Biol. 1998, 9, 411–416. [Google Scholar] [CrossRef] [Green Version]
- Holsberger, D.R.; Cooke, P.S. Understanding the role of thyroid hormone in Sertoli cell development: A mechanistic hypothesis. Cell. Tissue Res. 2005, 322, 133–140. [Google Scholar] [CrossRef]
- Meroni, S.B.; Galardo, M.N.; Rindone, G.; Gorga, A.; Riera, M.F.; Cigorraga, S.B. Molecular Mechanisms and Signaling Pathways Involved in Sertoli Cell Proliferation. Front. Endocrinol. 2019, 10, 224. [Google Scholar] [CrossRef]
- Wagner, M.S.; Wajner, S.M.; Maia, A.L. Is there a role for thyroid hormone on spermatogenesis? Microsc. Res. Tech. 2009, 72, 796–808. [Google Scholar] [CrossRef]
- Rotondo, J.C.; Lanzillotti, C.; Mazziotta, C.; Tognon, M.; Martini, F. Epigenetics of Male Infertility: The Role of DNA Methylation. Front. Cell Dev. Biol. 2021, 9, 689624. [Google Scholar] [CrossRef]
- Gunes, S.; Agarwal, A.; Henkel, R.; Mahmutoglu, A.M.; Sharma, R.; Esteves, S.C.; Aljowair, A.; Emirzeoglu, D.; Alkhani, A.; Pelegrini, L.; et al. Association between promoter methylation of MLH1 and MSH2 and reactive oxygen species in oligozoospermic men—A pilot study. Andrologia 2018, 50, e12903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.; Hamada, A.J.; Agarwal, A. Thyroid hormones in male reproduction and fertility. Open Reprod. Sci. J. 2011, 3, 98–104. [Google Scholar] [CrossRef] [Green Version]
- Abalovich, M.; Levalle, O.; Hermes, R.; Scaglia, H.; Aranda, C.; Zylbersztein, C.; Oneto, A.; Aquilano, D.; Gutierrez, S. Hypothalamic-pituitary-testicular axis and seminal parameters in hyperthyroid males. Thyroid 1999, 9, 857–863. [Google Scholar] [CrossRef] [PubMed]
- Corrales Hernández, J.J.; Miralles García, J.M.; García Diez, L.C. Primary hypothyroidism and human spermatogenesis. Arch. Androl. 1990, 25, 21–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikoobakht, M.R.; Aloosh, M.; Nikoobakht, N.; Mehrsay, A.R.; Biniaz, F.; Karjalian, M.A. The role of hypothyroidism in male infertility and erectile dysfunction. Urol. J. 2012, 9, 405–409. [Google Scholar] [PubMed]
- Krassas, G.E.; Papadopoulou, F.; Tziomalos, K.; Zeginiadou, T.; Pontikides, N. Hypothyroidism has an adverse effect on human spermatogenesis: A prospective, controlled study. Thyroid 2008, 18, 1255–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lotti, F.; Maseroli, E.; Fralassi, N.; Degl'Innocenti, S.; Boni, L.; Baldi, E.; Maggi, M. Is thyroid hormones evaluation of clinical value in the work-up of males of infertile couples? Hum. Reprod. 2016, 31, 518–529. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Chen, C.; Liu, G.G.; Wang, M.; Shi, C.; Yu, G.; Lv, F.; Wang, N.; Zhang, S. The association between iodine intake and semen quality among fertile men in China. BMC Public Health 2020, 20, 461. [Google Scholar] [CrossRef] [Green Version]
- La Vignera, S.; Vita, R.; Condorelli, R.A.; Mongioì, L.M.; Presti, S.; Benvenga, S.; Calogero, A.E. Impact of thyroid disease on testicular function. Endocrine 2017, 58, 397–407. [Google Scholar] [CrossRef]
- Wang, Y.X.; Zhou, B.; Chen, Y.J.; Liu, C.; Huang, L.L.; Liao, J.Q.; Hu, X.J.; Lu, W.Q.; Zeng, Q.; Pan, A. Thyroid function, phthalate exposure and semen quality: Exploring associations and mediation effects in reproductive-aged men. Environ. Int. 2018, 116, 278–285. [Google Scholar] [CrossRef]
- Xian, H.; Wang, F.; Teng, W.; Yang, D.; Zhang, M. Thyroid hormone induce a p53-dependent DNA damage through PI3K/Akt activation in sperm. Gene 2017, 615, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Rehman, R.; Zafar, A.; Fatima, S.S.; Mohib, A.; Sheikh, A. Altered sperm parameters and subclinical hypothyroidism; A cross sectional study in Karachi, Pakistan. Int. J. Clin. Pract. 2020, 74, e13555. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Total Sperm Count | <5 × 106 | 5–19 × 106 | 20–39 × 106 | ≥40 × 106 |
|---|---|---|---|---|
| n | 43 | 30 | 16 | 41 |
| TSH in μIU/mL (mean ± SD) * | 1.58 ± 1.23 | 1.59 ± 1.14 | 1.69 ± 0.79 | 1.53 ± 0.76 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kakoulidis, I.; Ilias, I.; Stergiotis, S.; Togias, S.; Michou, A.; Lekkou, A.; Mastrodimou, V.; Pappa, A.; Milionis, C.; Venaki, E.; et al. Study on the Interaction between Serum Thyrotropin and Semen Parameters in Men. Med. Sci. 2022, 10, 22. https://doi.org/10.3390/medsci10020022
Kakoulidis I, Ilias I, Stergiotis S, Togias S, Michou A, Lekkou A, Mastrodimou V, Pappa A, Milionis C, Venaki E, et al. Study on the Interaction between Serum Thyrotropin and Semen Parameters in Men. Medical Sciences. 2022; 10(2):22. https://doi.org/10.3390/medsci10020022
Chicago/Turabian StyleKakoulidis, Ioannis, Ioannis Ilias, Stefanos Stergiotis, Stefanos Togias, Aikaterini Michou, Anastasia Lekkou, Vasiliki Mastrodimou, Athina Pappa, Charalampos Milionis, Evangelia Venaki, and et al. 2022. "Study on the Interaction between Serum Thyrotropin and Semen Parameters in Men" Medical Sciences 10, no. 2: 22. https://doi.org/10.3390/medsci10020022
APA StyleKakoulidis, I., Ilias, I., Stergiotis, S., Togias, S., Michou, A., Lekkou, A., Mastrodimou, V., Pappa, A., Milionis, C., Venaki, E., & Koukkou, E. (2022). Study on the Interaction between Serum Thyrotropin and Semen Parameters in Men. Medical Sciences, 10(2), 22. https://doi.org/10.3390/medsci10020022