
Hierarchically Structured Role-Playing Simulation as a Tool for Promoting Soft Skills in Veterinary Undergraduates
 ,
,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
- -
- Phase 1: Initial role-playing. This simulation was performed in the facilities of the Veterinary Teaching Hospital of the University of Cordoba (Cordoba, Spain). Duration: 34–35 min. Dates for this phase were agreed with each group.
- -
- Phase 2: Lecture about soft skills and their application to veterinary clinical settings. This part was carried out in a classroom with a maximum of 40 attendees (a total of 5 sessions were scheduled). Duration: 90 min. This phase was conducted once all of the participants had completed phase 1.
- -
- Phase 3: Second role-playing after the lecture. This second simulation was performed in the same facilities as phase 1. Duration: 34–35 min. Dates for this phase were agreed upon with each group after every participant completed phase 2.
2.2. Role-Playing Activities (Phases 1 and 3)
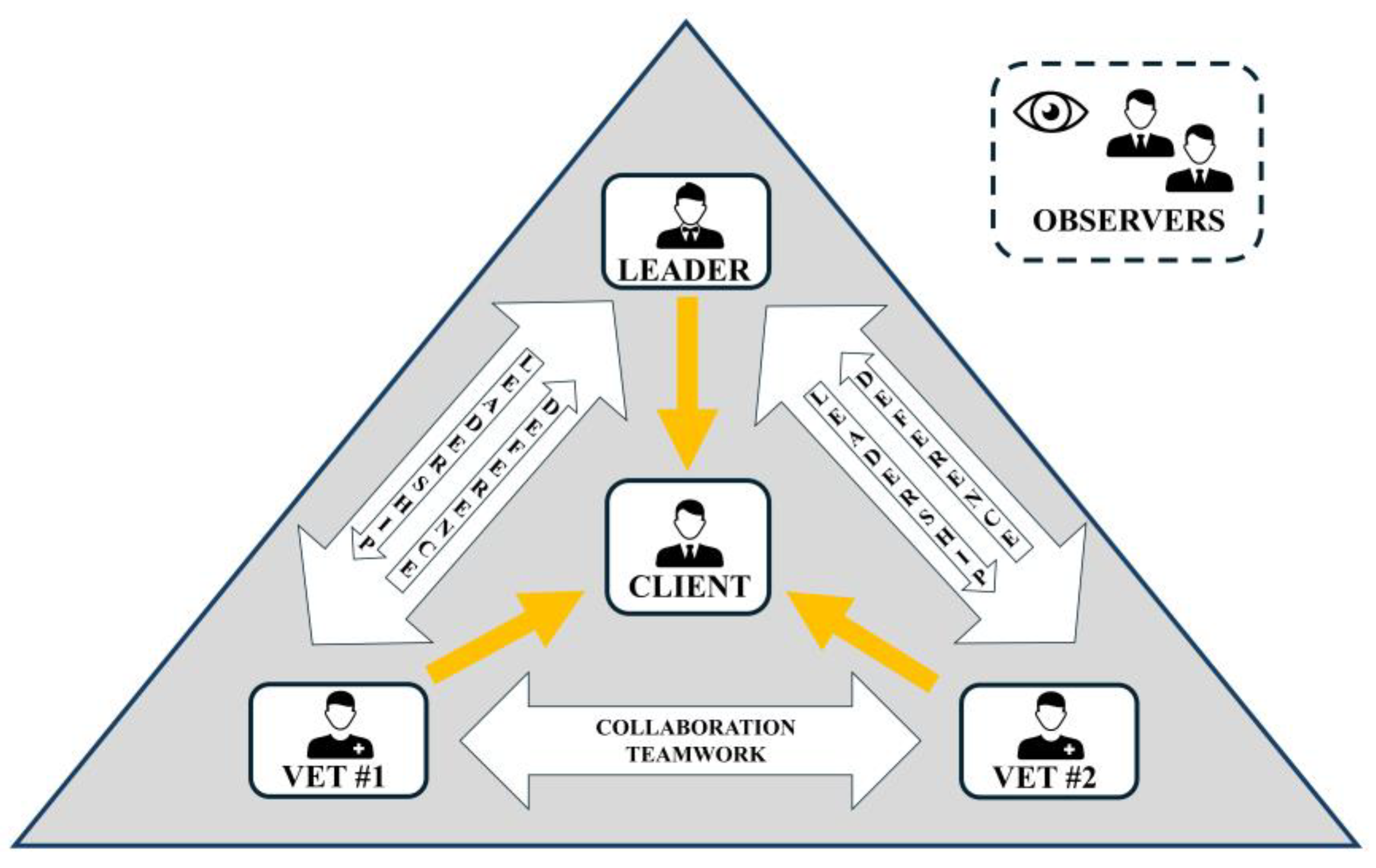
2.2.1. Roles and General Activity Design
2.2.2. Scenario and Prompt Description
2.3. Lecture About Soft Skills (Phase 2)
- -
- Stages of the veterinary consultation as described by the Calgary–Cambridge observation guide (CCOG): preparation, initiation, gathering information, explanation/planning, and closure [22].
- -
- Verbal and non-verbal communication in veterinary practice: communication strategies for veterinarians, categories of non-verbal behavior, how to shape spaces, how to address mixed messages, etc. [23].
- -
- The six-step SPIKES protocol for delivering bad news in veterinary clinical settings [24].
- -
- Shared decision making and effective client communication: the 4-E model for client communication [25].
- -
- Teamwork-oriented skills in the veterinary setting: task management, workload distribution, dependability, and delegation [21].
- -
2.4. Evaluation of the Role-Playing Simulations and Project Suitability
2.5. Statistical Analysis
3. Results
3.1. Participants and Simulations
3.2. Total Count of Incidents and Incidents per Soft Skill (Evaluation by the Authors)
3.3. Role Evaluation (Evaluation by the Students)
3.4. Overall Activity Evaluation by the Students
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CCOG | Calgary-Cambridge Observation -Guide |
| MDPI | Multidisciplinary Digital Publishing Institute |
References
- Kleinsorgen, C.; Steinberg, E.; Dömötör, R.; Piano, J.Z.; Rugelj, J.; Mandoki, M.; Radin, L. “The SOFTVETS Competence Model”—A preliminary project report. GMS J. Med. Educ. 2021, 38, Doc50. [Google Scholar] [CrossRef] [PubMed]
- van Gelderen Mabin, I.; Taylor, R. Developing communication competency in the veterinary curriculum. Animals 2023, 13, 3668. [Google Scholar] [CrossRef]
- Pato, N.F.; Ruíz-Rosillo, M.A.; Bueno, L.C.; Hurtado, I.R.; Vivas Urias, M.D. A novel teaching model using a massive online open course for soft skills development in the veterinary medicine curriculum. Front. Vet. Sci. 2025, 12, 1558473. [Google Scholar] [CrossRef]
- Kustritz, M.V.; Nault, A.J. Professional development training through the veterinary curriculum at the University of Minnesota. J. Vet. Med. Educ. 2010, 37, 233–237. [Google Scholar] [CrossRef] [PubMed]
- EAEVE. List of Subjects and Day One Competences: (As Approved by ECCVT on 17 January 2019). Available online: https://www.eaeve.org/fileadmin/downloads/eccvt/List_of_subjects_and_Day_One_Competences_approved_on_17_January_2019.pdf (accessed on 14 May 2025).
- Mills, P.C. Education and communication in veterinary clinical practice. Animals 2024, 14, 2622. [Google Scholar] [CrossRef]
- Bahramsoltani, M.; Bröer, S.; Langforth, S.; Eule, C.; Prior, A.; Vogt, L.; Li, T.T.; Schirone, R.; Pohl, A.; Jensen, K.C. Outcome of communication training in veterinary studies: Influence on the perception of the relevance of veterinary competencies and self-assessment of communication skills. Animals 2023, 13, 1516. [Google Scholar] [CrossRef]
- Pereira, M.M.; Artemiou, E.; De Pedro, P.; Adams, C.; Ritter, C. The use of the roter interaction analysis system in assessing veterinary student clinical communication skills during equine wellness examinations in rural Kentucky, USA: A pilot study. Vet. Rec. Open 2021, 8, e23. [Google Scholar] [CrossRef] [PubMed]
- Janke, N.; Coe, J.B.; Sutherland, K.A.K.; Bernardo, T.M.; Dewey, C.E.; Stone, E.A. Evaluating shared decision-making between companion animal veterinarians and their clients using the Observer OPTION5 instrument. Vet. Rec. 2021, 189, e778. [Google Scholar] [CrossRef]
- Ünsal Adaca, A.; Başağaç Gül, R.T. First experimental study in turkey teaches veterinary students how to break bad news. J. Vet. Med. Educ. 2020, 47, 720–727. [Google Scholar] [CrossRef]
- Blokland, K.; Janke, N.; Coe, J.B. Veterinary team relational coordination is associated with healthier perception of workplace psychological climate, increased job satisfaction, and reduced intention to leave. J. Am. Vet. Med. Assoc. 2025, 263, 746–754. [Google Scholar] [CrossRef]
- Kinnison, T.; May, S.A.; Guile, D. Inter-professional practice: From veterinarian to the veterinary team. J. Vet. Med. Educ. 2014, 41, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Perry, M.D. Building a veterinary practice team. Vet. Clin. N. Am. Small Anim. Pract. 2024, 54, 293–305. [Google Scholar] [CrossRef]
- Heise, S.A.C.; Wissing, S.; Nerschbach, V.; Preussing, E.; Tipold, A.; Kleinsorgen, C. Evaluation of an interprofessional blended learning course focusing on communication within veterinary teams. Animals 2024, 27, 729. [Google Scholar] [CrossRef]
- Sanford, J.R.; DeBowes, R.M. Top veterinary practice issues that negatively affect culture, retention, and performance. Vet. Clin. N. Am. Small Anim. Pract. 2024, 54, 423–440. [Google Scholar] [CrossRef]
- Nicol, D. Leadership in veterinary practice. Vet. Clin. N. Am. Small Anim. Pract. 2024, 54, 277–291. [Google Scholar] [CrossRef] [PubMed]
- Rauch, M.; Bettermann, V.; Tipold, A.; Wissing, S.; Kleinsorgen, C. Use of actors or peers as simulated clients in veterinary communication training. J. Vet. Med. Educ. 2022, 26, e20210055. [Google Scholar] [CrossRef]
- Radford, A.; Stockley, P.; Taylor, I.; Turner, R.; Gaskell, C.; Kaney, S.; Humphris, G.; Magrath, C. Use of simulated clients in training veterinary undergraduates in communication skills. Vet. Rec. 2003, 152, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Englar, R.E. A novel approach to simulation-based education for veterinary medical communication training over eight consecutive pre-clinical quarters. J. Vet. Med. Educ. 2017, 44, 502–522. [Google Scholar] [CrossRef]
- Fraser, D.R.; McGregor, D.D. An exercise in leadership training for veterinary students aiming for careers in biomedical research. J. Vet. Med. Educ. 2002, 29, 162–166. [Google Scholar] [CrossRef]
- Hanley, A.; Kedrowicz, A.A.; Hammond, S.; Hardie, E.M. Impact of team communication training on performance and self-assessment of team functioning during sophomore surgery. J. Vet. Med. Educ. 2019, 46, 45–55. [Google Scholar] [CrossRef]
- Radford, A.; Stockley, P.; Silverman, J.; Taylor, I.; Turner, R.; Gray, C. Development, teaching, and evaluation of a consultation structure model for use in veterinary education. J. Vet. Med. Educ. 2006, 33, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Carson, C.A. Nonverbal communication in veterinary practice. Vet. Clin. N. Am. Small Anim. Pract. 2007, 37, 49–63. [Google Scholar] [CrossRef]
- Shaw, J.R.; Lagoni, L. End-of-life communication in veterinary medicine: Delivering bad news and euthanasia decision making. Vet. Clin. N. Am. Small Anim. Pract. 2007, 37, 95–108. [Google Scholar] [CrossRef]
- Cornell, K.K.; Kopcha, M. Client-veterinarian communication: Skills for client centered dialogue and shared decision making. Vet. Clin. N. Am. Small Anim. Pract. 2007, 37, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Klingborg, D.J.; Moore, D.A.; Varea-Hammond, S. What is leadership? J. Vet. Med. Educ. 2006, 33, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Bosse, H.M.; Nickel, M.; Huwendiek, S.; Jünger, J.; Schultz, J.H.; Nikendei, C. Peer role-play and standardised patients in communication training: A comparative study on the student perspective on acceptability, realism, and perceived effect. BMC Med. Educ. 2010, 10, 27. [Google Scholar] [CrossRef]
- Thornhill-Miller, B.; Camarda, A.; Mercier, M.; Burkhardt, J.M.; Morisseau, T.; Bourgeois-Bougrine, S.; Vinchon, F.; El Hayek, S.; Augereau-Landais, M.; Mourey, F.; et al. Creativity, critical thinking, communication, and collaboration: Assessment, certification, and promotion of 21st century skills for the future of work and education. J. Intell. 2023, 11, 54. [Google Scholar] [CrossRef]
- Gray, C.; Moffett, J. Handbook of Veterinary Communication Skills; Wiley-Blackwell: Ames, IA, USA, 2010; pp. 25–46. [Google Scholar]
- Brandt, J.C.; Bateman, S.W. Senior veterinary students’ perceptions of using role play to learn communication skills. J. Vet. Med. Educ. 2006, 33, 76–80. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Scenario 1. The Beginning of the Consultation | |
| Role | Prompts |
| Client | Check notes about your imaginary pet. You can make up any information about you or your pet not specifically included in them. This is your first time in this Hospital. |
| Vets | Receive this new client, establish initial rapport, and identify the reasons for the consultation. Consider collecting all of the client’s concerns about the pet. |
| Leader | Prepare your team to receive this new client. Distribute the workload between the team members according to your own criteria. |
| Scenario 2. Proposing and Considering Two Conflicting Options | |
| Role | Prompts |
| Client | Several options are going to be discussed for your imaginary pet. You can make up any consideration (economical, ethical, previous experience, knowledge, etc.) about them. |
| Vets | In face of the diagnosis (check notes), there are 2 different options for this case. Based on your background, experience, and knowledge, you have a preferred one (check notes). Consult with your colleagues about the better option. Once you have reached a consensus, this should be discussed with the client. |
| Leader | In face of the diagnosis (check notes), there are 2 different options for this case. Try to collect the preferences of each of your team members and reach a consensus prior to talking to the client. Remember that you are the leader of this team. |
| Scenario 3. Delivering Bad News | |
| Role | Prompts |
| Client | The veterinary team is going to present you with some news about your pet. |
| Vets | The pet has died unexpectedly during a routine process. This must be reported to the client. |
| Leader | The pet has died unexpectedly during a routine process. This must be reported to the client. Remember that you are the leader of this team. |
| Client-Oriented Communication Errors |
| Fail to welcome/greet the client or attend to his/her comfort |
| Fail to introduce him/herself or any member of the team |
| Fail to ease the situation and establish a relaxed environment (lack of previous chit-chat) |
| Inadequate verbal expressions or inadequate non-verbal clues (i.e., lack of eye contact, inadequate posture and position or facial expression, incorrect use of tone, awkward spacing, etc.) |
| Fail to identify the primary reason for the consultation |
| Lack of open questions (avoiding the client to further express concerns and opinions) |
| Neglect of secondary/additional concerns and perspectives by the client |
| Lack of active listening skills (interrupting the client, directing their responses, etc.) |
| Fail to provide a structured planning during the consultation (steps, times, etc.) |
| Inappropiate shared decision making with the client (fail to consider the client’s perspective and preferences, use of bias, directing the decision, etc.) |
| Inadequate delivery of bad news (lack of warning shots, excessive jargon, etc.) |
| Lack of empathy |
| Teamwork Mistakes |
| Inappropiate teamwork (overshadowing other vet roles, absenteeism) |
| Contradicting other veterinary roles in front of the client |
| Lack of coordination with the rest of the team |
| Inadequate teamwork during the conflict (fail to listen actively, fail to give and receive feedback to/from other members of the team) |
| Leadership Failures |
| Inadequate distribution of workload by the team leader (or carelessness) |
| Fail to motivate the members of the team (support, empathy, validation) |
| Inadequate leadership during decision making (fail to promote a consensus, authoritarianism, avoiding responsibilities, inappropiate conflict solving, etc.) |
| Fail to assume responsibilities by the leader during the delivery of bad news (absenteeism during this step or excessive delegation) |
| Phase 1 | Phase 3 | |||||
|---|---|---|---|---|---|---|
| Client | Vet (both) | Leader | Vet (both) | Leader | ||
| 6.85 ± 2.2 (7) | 6.64 ± 1.8 (7) | 8.04 ± 1.3 (8) 1,2 | 7.06 ± 1.7 (7) 1 | |||
| Leader | Vet (both) | Self | Vet (both) | Self | ||
| 6.06 ± 1.5 (6) 2 | 4.62 ± 1.4 (5) | 6.54 ± 1.1 (7) 1,2 | 5.42 ± 0.8 (5) 1 | |||
| Vet | Self | Cross | Leader | Self | Cross | Leader |
| 6.47 ± 1.2 (7) 2 | 5.99 ± 1.6 (6) 2 | 4.41 ± 1.9 (4) | 6.71 ± 0.8 (7) 2 | 6.24 ± 1.3 (6) 2 | 4.97 ± 1.7 (5) 1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perez-Ecija, A.; Buzon-Cuevas, A.; De Las Heras, A.; Mendoza, F.J. Hierarchically Structured Role-Playing Simulation as a Tool for Promoting Soft Skills in Veterinary Undergraduates. Animals 2025, 15, 1638. https://doi.org/10.3390/ani15111638
Perez-Ecija A, Buzon-Cuevas A, De Las Heras A, Mendoza FJ. Hierarchically Structured Role-Playing Simulation as a Tool for Promoting Soft Skills in Veterinary Undergraduates. Animals. 2025; 15(11):1638. https://doi.org/10.3390/ani15111638
Chicago/Turabian StylePerez-Ecija, Alejandro, Antonio Buzon-Cuevas, Adelaida De Las Heras, and Francisco J. Mendoza. 2025. "Hierarchically Structured Role-Playing Simulation as a Tool for Promoting Soft Skills in Veterinary Undergraduates" Animals 15, no. 11: 1638. https://doi.org/10.3390/ani15111638
APA StylePerez-Ecija, A., Buzon-Cuevas, A., De Las Heras, A., & Mendoza, F. J. (2025). Hierarchically Structured Role-Playing Simulation as a Tool for Promoting Soft Skills in Veterinary Undergraduates. Animals, 15(11), 1638. https://doi.org/10.3390/ani15111638