
Low-Field Magnetic Resonance Imaging for the Detection of Medial Meniscal Lesions in Cranial Cruciate-Deficient Stifle Joints in Dogs


Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Diagnostic and Surgical Procedures
2.3. Data Analysis
3. Results
3.1. Signalment and Descriptive Statistics
3.2. Clinical and Orthopedic Examination
3.3. Diagnostic and Surgical Procedures
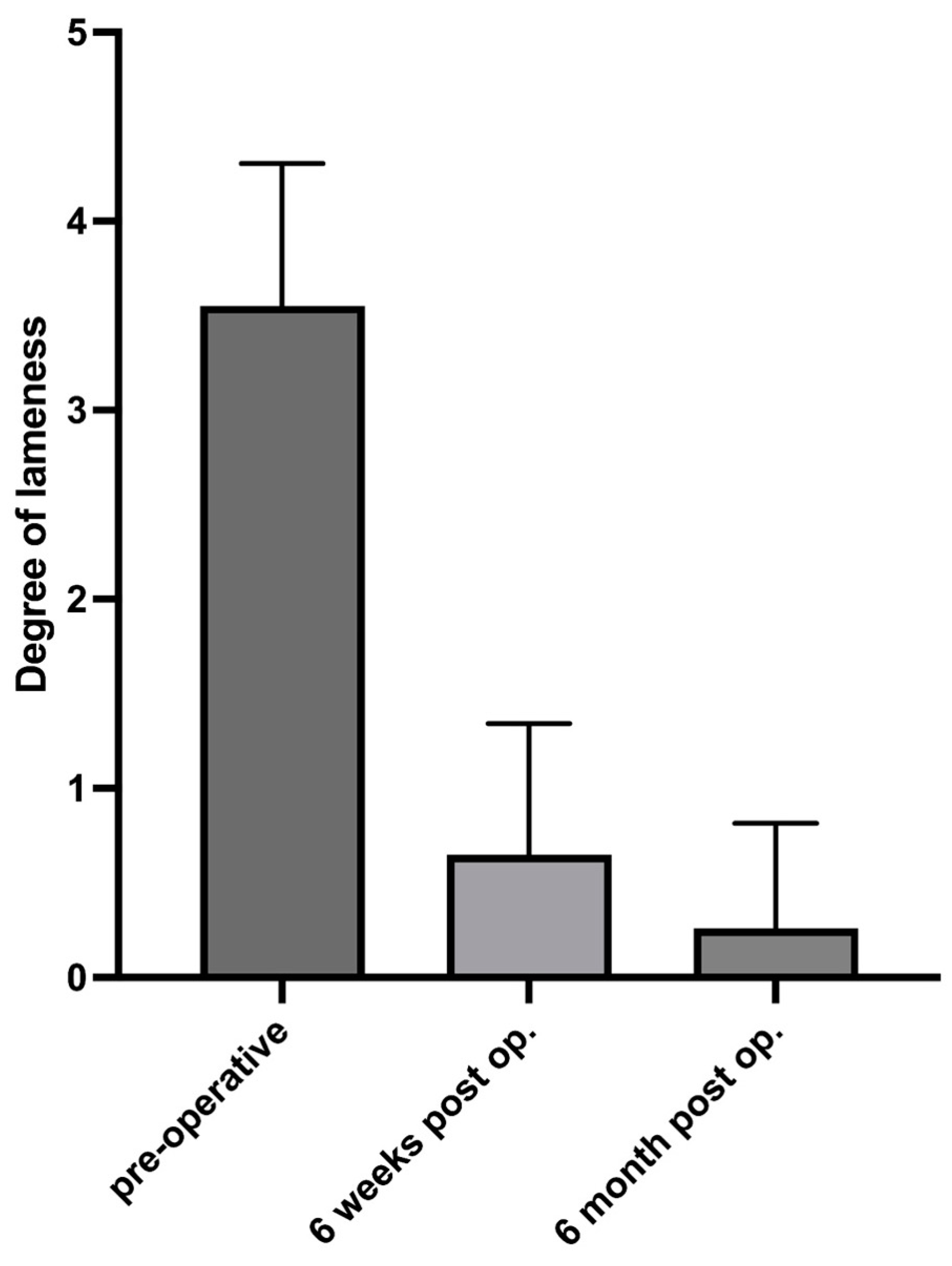
3.4. Evaluation 6 Weeks and 6 Months Postoperatively
4. Discussion
4.1. Meniscal Evaluation
4.2. Minimally Invasive Versus Noninvasive Diagnostic Imaging
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martig, S.; Konar, M.; Schmökel, H.G.; Rytz, U.; Spreng, D.; Scheidegger, J.; Höhl, B.; Kircher, P.R.; Boisclair, J.; Lang, J. Low-field Mri and arthroscopy of meniscal lesions in ten dogs with experimentally induced cranial cruciate ligament insufficiency. Vet. Radiol. Ultrasound 2006, 47, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Pownder, S.L.; Hayashi, K.; Caserto, B.G.; Breighner, R.E.; Norman, M.L.; Potter, H.G.; Koff, M.F. Quantitative Magnetic Resonance Imaging and Histological Comparison of Normal Canine Menisci. Vet. Comp. Orthop. Traumatol. 2018, 31, 452–457. [Google Scholar] [PubMed]
- Pozzi, A.; Kowaleski, M.P.; Apelt, D.; Meadows, C.; Andrews, C.M.; Johnson, K.A. Effect of medial meniscal release on tibial translation after tibial plateau leveling osteotomy. Vet. Surg. 2006, 35, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Ralphs, S.C.; Whitney, W.O. Arthroscopic evaluation of menisci in dogs with cranial cruciate ligament injuries: 100 cases (1999–2000). J. Am. Vet. Med. Assoc. 2002, 221, 1601–1604. [Google Scholar] [CrossRef] [PubMed]
- Casale, S.A.; McCarthy, R.J. Complications associated with lateral fabellotibial suture surgery for cranial cruciate ligament injury in dogs: 363 cases (1997–2005). J. Am. Vet. Med. Assoc. 2009, 234, 229–235. [Google Scholar] [CrossRef]
- Case, J.B.; Hulse, D.; Kerwin, S.C.; Peycke, L.E. Meniscal injury following initial cranial cruciate ligament stabilization surgery in 26 dogs (29 stifles). Vet. Comp. Orthop. Traumatol. 2008, 21, 365–367. [Google Scholar]
- Fitzpatrick, N.; Solano, M.A. Predictive variables for complications after TPLO with stifle inspection by arthrotomy in 1000 consecutive dogs. Vet. Surg. 2010, 39, 460–474. [Google Scholar] [CrossRef]
- Knebel, J.; Eberle, D.; Steigmeier-Raith, S.; Reese, S.; Meyer-Lindenberg, A. Outcome after Tibial Plateau Levelling Osteotomy and Modified Maquet Procedure in Dogs with Cranial Cruciate Ligament Rupture. Vet. Comp. Orthop. Traumatol. 2020, 33, 189–197. [Google Scholar] [CrossRef]
- Kalff, S.; Meachem, S.; Preston, C. Incidence of medial meniscal tears after arthroscopic assisted tibial plateau leveling osteotomy. Vet. Surg. 2011, 40, 952–956. [Google Scholar] [CrossRef]
- Barrett, E.; Barr, F.; Owen, M.; Bradley, K. A retrospective study of the MRI findings in 18 dogs with stifle injuries. J. Small Anim. Pract. 2009, 50, 448–455. [Google Scholar] [CrossRef]
- Blond, L.; Thrall, D.E.; Roe, S.C.; Chailleux, N.; Robertson, I.D. Diagnostic accuracy of magnetic resonance imaging for meniscal tears in dogs affected with naturally occuring cranial cruciate ligament rupture. Vet. Radiol. Ultrasound 2008, 49, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Böttcher, P.; Brühschwein, A.; Winkels, P.; Werner, H.; Ludewig, E.; Grevel, V.; Oechtering, G. Value of low-field magnetic resonance imaging in diagnosing meniscal tears in the canine stifle: A prospective study evaluating sensitivity and specificity in naturally occurring cranial cruciate ligament deficiency with arthroscopy as the gold standard. Vet. Surg. 2010, 39, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Böttcher, P.; Armbrust, L.; Blond, L.; Brühschwein, A.; Gavin, P.R.; Gielen, I.; Hecht, S.; Jurina, K.; Kneissl, S.; Konar, M.; et al. Effects of observer on the diagnostic accuracy of low-field MRI for detecting canine meniscal tears. Vet. Radiol. Ultrasound 2012, 53, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Winkels, P.; Pozzi, A.; Cook, R.; Böttcher, P. Prospective Evaluation of the Leipzig Stifle Distractor. Vet. Surg. 2016, 45, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Gemmill, T.J.; Farrell, M. Evaluation of a joint distractor to facilitate arthroscopy of the canine stifle. Vet. Surg. 2009, 38, 588–594. [Google Scholar] [CrossRef]
- Kim, J.H.; Heo, S.Y.; Lee, H.B. Arthroscopic detection of medial meniscal injury with the use of a joint distractor in small-breed dogs. J. Vet. Sci. 2017, 18, 515–520. [Google Scholar] [CrossRef]
- Pozzi, A.; Hildreth, B.; Rajala-Schultz, P. Comparison of Arthroscopy and Arthrotomy for Diagnosis of Medial Meniscal Pathology: An Ex Vivo Study. Vet. Surg. 2008, 37, 749–755. [Google Scholar] [CrossRef]
- Crues III, J.V.; Ryu, R.; Morgan, F.W. Meniscal pathology. The expanding role of magnetic resonance imaging. Clin. Orthop. Relat. Res. 1990, 252, 80–87. [Google Scholar]
- Adams, R.W.; Holmes, S.P.; Franklin, S.P. Magnetic resonance imaging diagnosis and arthroscopic treatment of medial meniscal injury in a dog with a palpably stable stifle. Can. Vet. J. 2018, 59, 654–658. [Google Scholar]
- Slocum, B.; Slocum, T.D. Tibial plateau leveling osteotomy for repair of cranial cruciate ligament rupture in the canine. Vet. Clin. N. Am. Small Anim. Pract. 1993, 23, 777–795. [Google Scholar] [CrossRef]
- Piermattei, D.L.; Johnson, K.A. Approach to the stifle joint through medial incision. In An Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat, 4th ed.; Piermattei, D.L., Johnson, K.A., Eds.; Saunders: Philadelphia, PA, USA, 2004; Volume 4, pp. 346–349. [Google Scholar]
- Beale, B.; Hulse, D.; Schulz, K.; Whitney, W. Arthroscopically assisted surgery of the stifle joint. In Small Animal Arthroscopy; Saunders: Philadelphia, PA, USA, 2003. [Google Scholar]
- Beale, B.; Hulse, D.; Schulz, K.; Whitney, W. Small Animal Arthroscopy; Saunders: Philadelphia, PA, USA, 2003. [Google Scholar]
- Flo, G.L. Classification of meniscal lesiona in twenty-six consecutive canine meniscectomies. J. Am. Anim. Hosp. Assoc. 1983, 19, 335–340. [Google Scholar]
- Wörtler, K. MRT des Kniegelenks MRI of the knee joint. Orthopaede 2008, 37, 157–172. [Google Scholar]
- Hoelzler, M.G.; Millis, D.L.; Francis, D.A.; Weigel, J.P. Results of arthroscopic versus open arthrotomy for surgical management of cranial cruciate ligament deficiency in dogs. Vet. Surg. 2004, 33, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Stauffer, K.D.; Tuttle, T.A.; Elkins, A.D.; Wehrenberg, A.P.; Character, B.J. Complications associated with 696 tibial plateau leveling osteotomies (2001-2003). J. Am. Anim. Hosp. Assoc. 2006, 42, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Pacchiana, P.D.; Morris, E.; Gillings, S.L.; Jessen, C.R.; Lipowitz, A.J. Surgical and postoperative complications associated with tibial plateau leveling osteotomy in dogs with cranial cruciate ligament rupture: 397 cases (1998-2001). J. Am. Vet. Med. Assoc. 2003, 222, 184–193. [Google Scholar] [CrossRef]
- Lineberger, J.A.; Allen, D.A.; Wilson, E.R.; Tobias, T.A.; Shaiken, L.G.; Shiroma, J.T.; Biller, D.S.; Lehenbauer, T.W. Comparison of radiographic arthritic changes associated with two variations of tibial plateau leveling osteotomy. Vet. Comp. Orthop. Traumatol. 2005, 18, 13–17. [Google Scholar]
- Priddy, N.H.; Tomlinson, J.L.; Dodam, J.R.; Hornbostel, J.E. Complications with and owner assessment of the outcome of tibial plateau leveling osteotomy for treatment of cranial cruciate ligament rupture in dogs: 193 cases (1997–2001). J. Am. Vet. Med. Assoc. 2003, 222, 1726–1732. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Sequence | Slice Thickness/ Slice Separation | Time to Repeat (TR) | Time to Echo (TE) | Flip Angle (FA) | Acquisition Time |
|---|---|---|---|---|---|
| Prescout | 0:13 min | ||||
| Scout transversal | 4.0/0.4 mm | 0:41 min | |||
| Scout dorsal | 4.0/0.4 mm | 0:40 min | |||
| Scout sagittal | 4.0/0.4 mm | 0:40 min | |||
| Fast Stir dorsal | 3.0/0.3 mm | 4220 ms | 30 ms | 90° | 5:46 min |
| GE T2* dorsal | 2.5/0.2 mm | 1675 ms | 26 ms | 65° | 6:24 min |
| GE T2* sagittal | 2.5/0.2 mm | 1675 ms | 26 ms | 65° | 6:24 min |
| FSE T2 transversal | 3.0/0.2 mm | 7220 ms | 120 ms | 90° | 6:31 min |
| 3D SST1 sagittal | 0,35 mm in 3D | 22 ms | 9 ms | 30° | 4:15 min |
| Total acquisition time | 31:57 min | ||||
| Grade | Meniscal Pathology |
|---|---|
| 0 | without pathological findings |
| 1 | diffusely increased signal—degeneration |
| 2 | mild axial fibrillation; mildly irregular axial border |
| 3 | severe axial fibrillation; blunt axial border without presence of fragments |
| 4 | nondisplaced rupture (linear signal increase with contact to one or two surfaces) |
| 5 | rupture with displaced fragment, bucket handle tear |
| 6 | folded meniscus |
| 7 | large parts of meniscus missing, multiple fragments |
| Grade | Meniscal Pathology |
|---|---|
| 0 | without pathological findings |
| 1 | meniscus degeneration |
| 2 | mild axial fraying |
| 3 | severe axial fraying |
| 4 | not displaced rupture |
| 5 | bucket handle tear |
| 6 | folded medial meniscus |
| 7 | multiple dislocated parts of meniscus |
| Patient | Lameness Preoperative | lfMRI Observer 1 | fMRI Observer 2 | Grading Intraoperative |
|---|---|---|---|---|
| 1 | 4 | 5 | 5 | 5 |
| 2 | 3 | 5 | 5 | 5 |
| 3 | 5 | 5 | 0 | 5 |
| 4 | 4 | 5 | 7 | 5 |
| 5 | 4 | 3 | 3 | 4 |
| 6 | 5 | 5 | 5 | 5 |
| 7 | 5 | 0 | 0 | 0 |
| 8 | 3 | 5 | 5 | 5 |
| 9 | 5 | 5 | 6 | 5 |
| 10 | 4 | 5 | 5 | 5 |
| 11 | 3 | 3 | 0 | 3 |
| 12 | 4 | 5 | 5 | 5 |
| 13 | 3 | 5 | 3 | 5 |
| 14 | 4 | 4 | 1 | 4 |
| 15 | 4 | 5 | 5 | 5 |
| 16 | 4 | 5 | 5 | 5 |
| 17 | 3 | 5 | 5 | 5 |
| 18 | 5 | 5 | 5 | 5 |
| 19 | 3 | 5 | 5 | 5 |
| 20 | 5 | 5 | 5 | 5 |
| 21 | 3 | 5 | 5 | 5 |
| 22 | 3 | 7 | 5 | 6 |
| 23 | 4 | 5 | 5 | 5 |
| 24 | 4 | 7 | 5 | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knebel, J.; Wilke, S.K.; Neumann, S.; Klatt, A.-L.; Schenk, H.C.; Konar, M. Low-Field Magnetic Resonance Imaging for the Detection of Medial Meniscal Lesions in Cranial Cruciate-Deficient Stifle Joints in Dogs. Animals 2024, 14, 3097. https://doi.org/10.3390/ani14213097
Knebel J, Wilke SK, Neumann S, Klatt A-L, Schenk HC, Konar M. Low-Field Magnetic Resonance Imaging for the Detection of Medial Meniscal Lesions in Cranial Cruciate-Deficient Stifle Joints in Dogs. Animals. 2024; 14(21):3097. https://doi.org/10.3390/ani14213097
Chicago/Turabian StyleKnebel, Julia, Svenja K. Wilke, Stephan Neumann, Anna-Lena Klatt, Henning C. Schenk, and Martin Konar. 2024. "Low-Field Magnetic Resonance Imaging for the Detection of Medial Meniscal Lesions in Cranial Cruciate-Deficient Stifle Joints in Dogs" Animals 14, no. 21: 3097. https://doi.org/10.3390/ani14213097
APA StyleKnebel, J., Wilke, S. K., Neumann, S., Klatt, A.-L., Schenk, H. C., & Konar, M. (2024). Low-Field Magnetic Resonance Imaging for the Detection of Medial Meniscal Lesions in Cranial Cruciate-Deficient Stifle Joints in Dogs. Animals, 14(21), 3097. https://doi.org/10.3390/ani14213097