
Cardiac Magnetic Resonance Imaging Detects Myocardial Abnormalities in Naturally Infected Dogs with Chronic Asymptomatic Chagas Disease


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Electrocardiography
2.3. Echocardiography
2.4. Cardiac Magnetic Resonance Imaging
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barr, S.C.; Holmes, R.A.; Klei, T.R. Electrocardiographic and Echocardiographic Features of Trypanosomiasis in Dogs Inoculated with North American Trypanosoma Cruzi Isolates. Am. J. Vet. Res. 1992, 53, 521–527. [Google Scholar] [PubMed]
- Barr, S.C. Canine Chagas’ Disease (American Trypanosomiasis) in North America. Vet. Clin. North Am. Small Animal Pract. 2009, 39, 1055–1064. [Google Scholar] [CrossRef] [PubMed]
- Meyers, A.C.; Meinders, M.; Hamer, S.A. Widespread Trypanosoma Cruzi Infection in Government Working Dogs along the Texas-Mexico Border: Discordant Serology, Parasite Genotyping and Associated Vectors. PLoS Negl. Trop. Dis. 2017, 11, e0005819-19. [Google Scholar] [CrossRef] [PubMed]
- de Sousa Pereira, H.; Scofield, A.; Júnior, P.S.B.; Dos Santos, D.L.; de Sousa Siqueira, J.; Chaves, J.F.; de Jesus Cardoso, R.; dos Anjos Lima, A.S.; Sarmento, N.M.F.P.; Júnior, F.D.; et al. Chagas Disease in Urban and Peri-urban Environment in the Amazon: Sentinel Hosts, Vectors, and the Environment. Acta. Trop. 2021, 217, 105858. [Google Scholar]
- Barr, S.C.; Schmidt, S.P.; Brown, C.C.; Klei, T.R. Pathologic Features of Dogs Inoculated with North American Trypanosoma Cruzi Isolates. Am. J. Vet. Res. 1991, 52, 2033–2039. [Google Scholar] [PubMed]
- Andrade, Z.A.; Andrade, S.G.; Sadigursky, M. Damage and Healing in the Conducting Tissue of the Heart (an Experimental Study in Dogs Infected with Trypanosoma Cruzi). J. Pathol. 1984, 143, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Andrade, Z.A.; Andrade, S.G.; Sadigursky, M.; Maguire, J.H. Experimental Chagas’ Disease in Dogs. A Pathologic and ECG Study of the Chronic Indeterminate Phase of the Infection. Arch. Pathol. Lab. Med. 1981, 105, 460–464. [Google Scholar] [PubMed]
- Rassi, A.; Rezende, J.M. de American Trypanosomiasis (Chagas Disease). Infect. Dis. Clin. North Am. 2012, 26, 275–291. [Google Scholar] [CrossRef]
- Vitt, J.P.; Saunders, A.B.; O’Brien, M.T.; Mansell, J.; Ajithdoss, D.K.; Hamer, S.A. Diagnostic Features of Acute Chagas Myocarditis with Sudden Death in a Family of Boxer Dogs. J. Vet. Intern. Med. 2016, 30, 1210–1215. [Google Scholar] [CrossRef]
- Bern, C.; Messenger, L.A.; Whitman, J.D.; Maguire, J.H. Chagas Disease in the United States: A Public Health Approach. Clin. Microbiol. Rev. 2019, 33, e00023-19. [Google Scholar] [CrossRef]
- Ribeiro, A.L.P.; Marcolino, M.S.; Prineas, R.J.; Lima-Costa, M.F. Electrocardiographic Abnormalities in Elderly Chagas Disease Patients: 10-Year Follow-Up of the Bambuí Cohort Study of Aging. J. Am. Heart Assoc. 2014, 3, e000632. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Chagas Disease (Also Known as American Trypanosomiasis). Available online: https://www.who.int/en/news-room/fact-sheets/detail/chagas-disease-(american-trypanosomiasis) (accessed on 4 November 2022).
- Carvalho, E.B.; Ramos, I.P.R.; Nascimento, A.F.S.; Brasil, G.V.; Mello, D.B.; Oti, M.; Sammeth, M.; Bahia, M.T.; de Carvalho, A.C.C.; Carvalho, A.B. Echocardiographic Measurements in a Preclinical Model of Chronic Chagasic Cardiomyopathy in Dogs: Validation and Reproducibility. Front. Cell. Infect. Microbiol. 2019, 9, 332. [Google Scholar] [CrossRef] [PubMed]
- Lee-Felker, S.A.; Thomas, M.; Felker, E.R.; Traina, M.; Salih, M.; Hernandez, S.; Bradfield, J.; Lee, M.; Meymandi, S. Value of Cardiac MRI for Evaluation of Chronic Chagas Disease Cardiomyopathy. Clin. Radiol. 2016, 71, 618.e1–618.e7. [Google Scholar] [CrossRef] [PubMed]
- Acquatella, H.; Asch, F.M.; Barbosa, M.M.; Barros, M.; Bern, C.; Cavalcante, J.L.; Correa, L.E.E.; Lima, J.; Marcus, R.; Marin-Neto, J.A.; et al. Recommendations for Multimodality Cardiac Imaging in Patients with Chagas Disease: A Report from the American Society of Echocardiography in Collaboration With the InterAmerican Association of Echocardiography (ECOSIAC) and the Cardiovascular Imaging Department of the Brazilian Society of Cardiology (DIC-SBC). J. Am. Soc. Echo. 2018, 31, 3–25. [Google Scholar]
- Bocchi, E.A.; Kalil, R.; Bacal, F.; de Lourdes Higuchi, M.; Meneghetti, C.; Magalhães, A.; Belotti, G.; Ramires, J.A.F. Magnetic Resonance Imaging in Chronic Chagas’ Disease: Correlation with Endomyocardial Biopsy Findings and Gallium-67 Cardiac Uptake. Echocardiography 1998, 15, 279–288. [Google Scholar]
- Rochitte, C.E.; Nacif, M.S.; de Oliveira Júnior, A.C.; Siqueira-Batista, R.; Marchiori, E.; Uellendahl, M.; de Lourdes Higuchi, M. Cardiac Magnetic Resonance in Chagas’ Disease. Artif. Organs 2007, 31, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Uellendahl, M.; de Siqueira, M.E.M.; Calado, E.B.; Kalil-Filho, R.; Sobral, D.; Ribeiro, C.; Oliveira, W.; Martins, S.; Narula, J.; Rochitte, C.E. Cardiac Magnetic Resonance-Verified Myocardial Fibrosis in Chagas Disease: Clinical Correlates and Risk Stratification. Arq. Bras. Cardiol. 2016, 107, 460–466. [Google Scholar] [CrossRef]
- Regueiro, A.; García-Álvarez, A.; Sitges, M.; Ortiz-Pérez, J.T.; Caralt, M.T.D.; Pinazo, M.J.; Posada, E.; Heras, M.; Gascón, J.; Sanz, G. Myocardial Involvement in Chagas Disease: Insights from Cardiac Magnetic Resonance. Int. J. Cardiol. 2013, 165, 107–112. [Google Scholar] [CrossRef]
- Pinheiro, M.V.T.; Moll-Bernardes, R.J.; Camargo, G.C.; Siqueira, F.P.; de Azevedo, C.F.; de Holanda, M.T.; Mendes, F.D.S.N.S.; Sangenis, L.H.C.; Mediano, M.F.F.; de Sousa, A.S. Associations between Cardiac Magnetic Resonance T1 Mapping Parameters and Ventricular Arrhythmia in Patients with Chagas Disease. Am. J. Trop. Med. Hyg. 2020, 130, 745–751. [Google Scholar] [CrossRef]
- Buechel, E.R.V.; Grosse-Wortmann, L.; Fratz, S.; Eichhorn, J.; Sarikouch, S.; Greil, G.F.; Beerbaum, P.; Bucciarelli-Ducci, C.; Bonello, B.; Sieverding, L.; et al. Indications for Cardiovascular Magnetic Resonance in Children with Congenital and Acquired Heart Disease: An Expert Consensus Paper of the Imaging Working Group of the AEPC and the Cardiovascular Magnetic Resonance Section of the EACVI. Cardiol. Young 2015, 25, 819–838. [Google Scholar] [CrossRef]
- Winter, R.L.; Saunders, A.B.; Gordon, S.G.; Miller, M.W.; Sykes, K.T.; Suchodolski, J.S.; Steiner, J.M. Analytical Validation and Clinical Evaluation of a Commercially Available High-Sensitivity Immunoassay for the Measurement of Troponin I in Humans for Use in Dogs. J. Vet. Cardiol. 2014, 16, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Meyers, A.C.; Ellis, M.M.; Purnell, J.C.; Auckland, L.D.; Meinders, M.; Saunders, A.B.; Hamer, S.A. Selected Cardiac Abnormalities in Trypanosoma Cruzi Serologically Positive, Discordant, and Negative Working Dogs along the Texas-Mexico Border. BMC Vet. Res. 2020, 16, 101. [Google Scholar] [CrossRef] [PubMed]
- Lown, B.; Wolf, M. Approaches to Sudden Death from Coronary Heart Disease. Circulation 1971, 44, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.J.; Saunders, A.B.; Meyers, A.C.; Gordon, S.G.; Hamer, S.A. Cardiac Diagnostic Test Results and Outcomes in 44 Dogs Naturally Infected with Trypanosoma cruzi. J. Vet. Intern. Med. 2021, 35, 1800–1809. [Google Scholar] [CrossRef] [PubMed]
- Cornell, C.C.; Kittleson, M.D.; Torre, P.D.; Häggström, J.; Lombard, C.W.; Pedersen, H.D.; Vollmar, A.; Wey, A. Allometric Scaling of M-Mode Cardiac Measurements in Normal Adult Dogs. J. Vet. Intern. Med. 2004, 18, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Rishniw, M.; Erb, H.N. Evaluation of Four 2-Dimensional Echocardiographic Methods of Assessing Left Atrial Size in Dogs. J. Vet. Intern. Med. 2000, 14, 429–435. [Google Scholar] [CrossRef]
- Strohm, L.E.; Visser, L.C.; Chapel, E.H.; Drost, W.T.; Bonagura, J.D. Two-Dimensional, Long-Axis Echocardiographic Ratios for Assessment of Left Atrial and Ventricular Size in Dogs. J. Vet. Cardiol. 2018, 20, 330–342. [Google Scholar] [CrossRef]
- Gentile-Solomon, J.M.; Abbott, J.A. Conventional Echocardiographic Assessment of the Canine Right Heart: Reference Intervals and Repeatability. J. Vet. Cardiol. 2016, 18, 234–247. [Google Scholar] [CrossRef]
- Reinero, C.; Visser, L.C.; Kellihan, H.B.; Masseau, I.; Rozanski, E.; Clercx, C.; Williams, K.; Abbott, J.; Borgarelli, M.; Scansen, B.A. ACVIM Consensus Statement Guidelines for the Diagnosis, Classification, Treatment, and Monitoring of Pulmonary Hypertension in Dogs. J. Vet. Intern. Med. 2020, 34, 549–573. [Google Scholar] [CrossRef]
- Visser, L.C. Right Ventricular Function Imaging Techniques. Vet. Clin. North Am. Small Animal Pract. 2017, 47, 989–1003. [Google Scholar] [CrossRef]
- Visser, L.C.; Scansen, B.A.; Brown, N.V.; Schober, K.E.; Bonagura, J.D. Echocardiographic Assessment of Right Ventricular Systolic Function in Conscious Healthy Dogs Following a Single Dose of Pimobendan versus Atenolol. J. Vet. Cardiol. 2015, 17, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Wess, G. Screening for Dilated Cardiomyopathy in Dogs. J. Vet. Cardiol. 2022, 40, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Visser, L.C.; Ciccozzi, M.M.; Sintov, D.J.; Sharpe, A.N. Echocardiographic Quantitation of Left Heart Size and Function in 122 Healthy Dogs: A Prospective Study Proposing Reference Intervals and Assessing Repeatability. J. Vet. Intern. Med. 2019, 33, 1909–1920. [Google Scholar] [CrossRef] [PubMed]
- Visser, L.C.; Wood, J.E.; Johnson, L.R. Survival Characteristics and Prognostic Importance of Echocardiographic Measurements of Right Heart Size and Function in Dogs with Pulmonary Hypertension. J. Vet. Intern. Med. 2020, 34, 1379–1388. [Google Scholar] [CrossRef]
- Visser, L.C.; Nishimura, S.; Oldach, M.S.; Bélanger, C.; Gunther-Harrington, C.T.; Stern, J.A.; Hsue, W. Echocardiographic Assessment of Right Heart Size and Function in Dogs with Pulmonary Valve Stenosis. J. Vet. Cardiol. 2019, 26, 19–28. [Google Scholar] [CrossRef]
- Bonagura, J.D.; Visser, L.C. Echocardiographic Assessment of Dilated Cardiomyopathy in Dogs. J. Vet. Cardiol. 2022, 40, 15–50. [Google Scholar] [CrossRef]
- Fries, R.C.; Gordon, S.G.; Saunders, A.B.; Miller, M.W.; Hariu, C.D.; Schaeffer, D.J. Quantitative Assessment of Two- and Three-Dimensional Transthoracic and Two-Dimensional Transesophageal Echocardiography, Computed Tomography, and Magnetic Resonance Imaging in Normal Canine Hearts. J. Vet. Cardiol. 2019, 21, 79–92. [Google Scholar] [CrossRef]
- Clark, W.A.; Winter, R.L.; Aarnes, T.K.; Green, E.M.; Mikrut, K.; Ruz, P.; Addison, D.; Rhinehart, J.D.; Schober, K.E.; Friel, H.T. Utility of Cardiac MRI to Diagnose Myocardial Ischemia and Fibrosis in Dogs with Cardiomegaly Secondary to Myxomatous Mitral Valve Disease. Am. J. Vet. Res. 2022, 1–10. [Google Scholar] [CrossRef]
- Zhou, Z.; Xu, L.; Wang, R.; Varga-Szemes, A.; Durden, J.A.; Schoepf, U.J.; Sun, Z.; Fan, Z. Quantification of Doxorubicin-Induced Interstitial Myocardial Fibrosis in a Beagle Model Using Equilibrium Contrast-Enhanced Computed Tomography: A Comparative Study with Cardiac Magnetic Resonance T1-Mapping. Int. J. Cardiol. 2019, 281, 150–155. [Google Scholar] [CrossRef]
- Santilli, R.; Moise, N.S.; Pariuat, R.; Perego, M. Chapter 3: Formation and Interpretation of the Electrocardiographic Waves. In Electrocardiography of the Dog and Cat; Edra: Milano, Italy, 2018; pp. 35–69. [Google Scholar]
- Keene, B.W.; Atkins, C.E.; Bonagura, J.D.; Fox, P.R.; Häggström, J.; Fuentes, V.L.; Oyama, M.A.; Rush, J.E.; Stepien, R.; Uechi, M. ACVIM Consensus Guidelines for the Diagnosis and Treatment of Myxomatous Mitral Valve Disease in Dogs. J. Vet. Intern. Med. 2019, 33, 1127–1140. [Google Scholar] [CrossRef]
- Toaldo, M.B.; Glaus, T.; Campagna, I.; Matos, J.N.; Dennler, M. Echocardiographic Assessment of Right Ventricular Systolic Function in Healthy Beagle Dogs Compared to High Field Cardiac Magnetic Resonance Imaging. Vet. J. 2021, 271, 105653. [Google Scholar] [CrossRef] [PubMed]
- Curtis-Robles, R.; Lewis, B.C.; Hamer, S.A. High Trypanosoma Cruzi Infection Prevalence Associated with Minimal Cardiac Pathology among Wild Carnivores in Central Texas. Int. J. Parasitol. Parasites Wildl. 2016, 5, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Tassi, E.M.; Continentino, M.A.; Nascimento, E.M.D.; Pereira, B.D.B.; Pedrosa, R.C. Relationship between Fibrosis and Ventricular Arrhythmias in Chagas Heart Disease without Ventricular Dysfunction. Arq. Bras. Cardiol. 2014, 102, 456–464. [Google Scholar]
- Rochitte, C.E.; Oliveira, P.F.; Andrade, J.M.; Ianni, B.M.; Parga, J.R.; Ávila, L.F.; Kalil-Filho, R.; Mady, C.; Meneghetti, J.C.; Lima, J.A.C.; et al. Myocardial Delayed Enhancement by Magnetic Resonance Imaging in Patients with Chagas’ Disease. J. Amer. Coll. Cardiol. 2005, 46, 1553–1558. [Google Scholar] [CrossRef]
- Nunes, M.C.P.; Beaton, A.; Acquatella, H.; Bern, C.; Bolger, A.F.; Echeverría, L.E.; Dutra, W.O.; Gascón, J.; Morillo, C.A.; Oliveira-Filho, J.; et al. Chagas Cardiomyopathy: An Update of Current Clinical Knowledge and Management: A Scientific Statement from the American Heart Association. Circulation 2018, 138, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.C.P.; Badano, L.P.; Marin-Neto, J.A.; Edvardsen, T.; Fernández-Golfín, C.; Bucciarelli-Ducci, C.; Popescu, B.A.; Underwood, R.; Habib, G.; Zamorano, J.L.; et al. Multimodality Imaging Evaluation of Chagas Disease: An Expert Consensus of Brazilian Cardiovascular Imaging Department (DIC) and the European Association of Cardiovascular Imaging (EACVI). Eur. Heart J. Cardiovasc. Imaging. 2017, 465, S6–S16. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.S.; Oliveira, J.A.M.D.; Frederigue, U.; Filho, E.C.L. Apical Aneurysm of Chagas’s Heart Disease. Brit. Heart J. 1981, 46, 432. [Google Scholar] [CrossRef]
- Stoner, C.H.; Saunders, A.B. Cardiac Manifestations of Trypanosoma cruzi Infection in a Domestic Dog. Cardiovasc. Imaging Case Rep. 2020, 4, 410–414. [Google Scholar] [CrossRef]
- Rassi, A., Jr.; Rassi, S.G.; Rassi, A. Sudden Death in Chagas’ Disease. Arq. Bras. Cardiol. 2001, 76, 86–96. [Google Scholar] [CrossRef]
- Melendez-Ramirez, G.; Soto, M.E.; Alvarez, L.C.V.; Meave, A.; Juarez-Orozco, L.E.; Guarner-Lans, V.; Morales, J.L. Comparison of the Amount and Patterns of Late Enhancement in Chagas Disease According to the Presence and Type of Ventricular Tachycardia. J. Cardiovasc. Electrophysiol. 2019, 30, 1517–1525. [Google Scholar] [CrossRef]
- Meyers, A.C.; Hamer, S.A.; Matthews, D.; Gordon, S.G.; Saunders, A.B. Risk Factors and Select Cardiac Characteristics in Dogs Naturally Infected with Trypanosoma cruzi Presenting to a Teaching Hospital in Texas. J. Vet. Intern. Med. 2019, 33, 1695–1706. [Google Scholar] [CrossRef] [PubMed]
- Saunders, A.B.; Wesselowski, S.; Malcolm, E.; Sykes, K.T.; Collins, S.; Busselman, R.E.; Hamer, S.A.; Steiner, J.M. Prospective cardiac evaluation in 50 asymptomatic dogs naturally-infected with Trypanosoma cruzi (abstract). J. Vet. Intern. Med. 2021, 35, 2970. [Google Scholar]
- Cunningham, S.M.; Aona, B.D.; Antoon, K.; Rush, J.E.; Barton, B.A. Echocardiographic Assessment of Right Ventricular Systolic Function in Boxers with Arrhythmogenic Right Ventricular Cardiomyopathy. J. Vet. Cardiol. 2018, 20, 343–353. [Google Scholar] [CrossRef]
- Moreira, H.T.; Volpe, G.J.; Marin-Neto, J.A.; Nwabuo, C.C.; Ambale-Venkatesh, B.; Gali, L.G.; Almeida-Filho, O.C.; Romano, M.M.D.; Pazin-Filho, A.; Maciel, B.C.; et al. Right Ventricular Systolic Dysfunction in Chagas Disease Defined by Speckle-Tracking Echocardiography: A Comparative Study with Cardiac Magnetic Resonance Imaging. J. Am. Soc. Echo. 2017, 30, 493–502. [Google Scholar]
- Malcolm, E.L.; Saunders, A.B.; Vitt, J.P.; Boutet, B.G.; Hamer, S.A. Antiparasitic Treatment with Itraconazole and Amiodarone in 2 Dogs with Severe, Symptomatic Chagas Cardiomyopathy. J. Vet. Intern. Med. 2022, 36, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Appadurai, V.; Thomas, J.D. Detecting Scar in Echocardiography: Has the Power Shifted? J. Am. Soc. Echo. 2022, 35, 1156–1158. [Google Scholar] [CrossRef]
- de Lana, M.; Giunchetti, R.C. Dogs as a Model for Chemotherapy of Chagas Disease and Leishmaniasis. Curr. Pharm. Design. 2021, 27, 1741–1756. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Value | Reference Range |
|---|---|---|
| P duration (ms) | 40 (39–60) | <40 |
| PR duration (ms) | 120 (70–120) | 60–130 |
| QRS duration (ms) | 40 (40–60) | <70 |
| P amplitude (mV) | 0.2 (0.1–0.3) | <0.4 |
| R amplitude (mV) | 1.9 (0.9–2.8) | >0.5 |
| Echocardiographic Variables | Median (Range) |
|---|---|
| LVIDd (cm) | 3.78 (3.07–3.06) |
| LVIDdN | 1.57 (1.34–1.75) |
| LVIDs (cm) | 2.65 (1.96–3.20) |
| LVIDsN | 1.02 (0.80–1.16) |
| LV FS (%) | 30.7 (24.0–46.7) |
| LVEDV (mL) | 49.29 (36.83–67.38) |
| LVESV (mL) | 19.08 (15.68–26.03) |
| LV EF (%) | 59.9 (51.2–65.5) |
| MV E (m/s) | 0.65 (0.48–0.88) |
| MV E:A | 1.17 (1.00–2.85) |
| LA:Ao short axis | 1.30 (1.04–1.4) |
| LA diameter long axis (cm) | 3.52 (3.27–4.20) |
| RA diameter long axis (cm) | 2.68 (1.98–3.18) |
| RA:LA | 0.75 (0.50–0.90) |
| RVIDd (cm) | 1.51 (1.12–1.93) |
| RVIDd:LVIDd | 0.41 (0.30–0.48) |
| TAPSE (mm) | 13.5 (7.8–19.3) |
| TAPSEn | 5.12 (2.78–8.02) |
| RV S’ (cm/s) | 10 (5–14) |
| iRV S’ | 4.8 (2.2–7.3) |
| GLPS_AVE (%) | −17.4 (-15.5 to –24.7) |
| CMR Variables | |
| LV SV (mL) | 20.9 (10.7–30.5) |
| LV ECV (%)* | 24.9 (20.7–31.7) |
| HCT (%) | 43 (38–48) |
| LV native T1 time (ms) * | 1141 (1050–1198) |
| LV post T1 time (ms) * | 513 (487–675) |
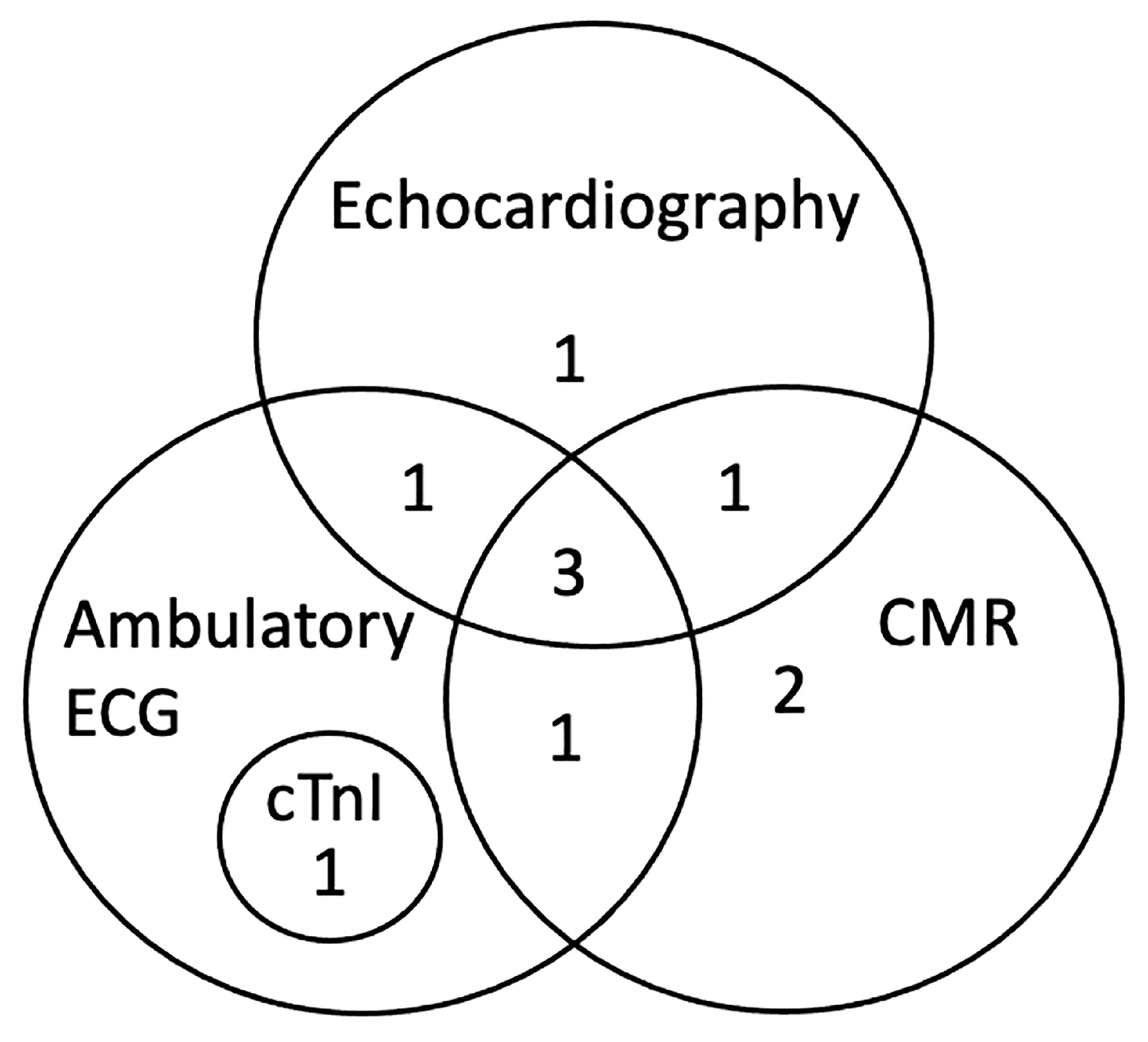
| Diagnostic Test | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Cardiac troponin I | X | |||||||||
| ECG (standard) | X | X | X | |||||||
| ECG (Ambulatory) | X | X | X | X | X | X | ||||
| Echocardiogram | X | X | X | X | X | X | ||||
| CMR | X | X | X | X | X | X | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matthews, D.J.; Fries, R.C.; Jeffery, N.D.; Hamer, S.A.; Saunders, A.B. Cardiac Magnetic Resonance Imaging Detects Myocardial Abnormalities in Naturally Infected Dogs with Chronic Asymptomatic Chagas Disease. Animals 2023, 13, 1393. https://doi.org/10.3390/ani13081393
Matthews DJ, Fries RC, Jeffery ND, Hamer SA, Saunders AB. Cardiac Magnetic Resonance Imaging Detects Myocardial Abnormalities in Naturally Infected Dogs with Chronic Asymptomatic Chagas Disease. Animals. 2023; 13(8):1393. https://doi.org/10.3390/ani13081393
Chicago/Turabian StyleMatthews, Derek J., Ryan C. Fries, Nicholas D. Jeffery, Sarah A. Hamer, and Ashley B. Saunders. 2023. "Cardiac Magnetic Resonance Imaging Detects Myocardial Abnormalities in Naturally Infected Dogs with Chronic Asymptomatic Chagas Disease" Animals 13, no. 8: 1393. https://doi.org/10.3390/ani13081393
APA StyleMatthews, D. J., Fries, R. C., Jeffery, N. D., Hamer, S. A., & Saunders, A. B. (2023). Cardiac Magnetic Resonance Imaging Detects Myocardial Abnormalities in Naturally Infected Dogs with Chronic Asymptomatic Chagas Disease. Animals, 13(8), 1393. https://doi.org/10.3390/ani13081393