
Risk Factors for Exercise-Associated Sudden Cardiac Death in Thoroughbred Racehorses


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Collection
2.2. Case Selection, Case Definition and Inclusion Criteria
2.3. Data Analysis
2.3.1. Software
2.3.2. Risk Factor Analysis
2.3.3. Survival Analysis
2.3.4. Comparison to Horses in the Australian Racing Population
3. Results
3.1. Animals
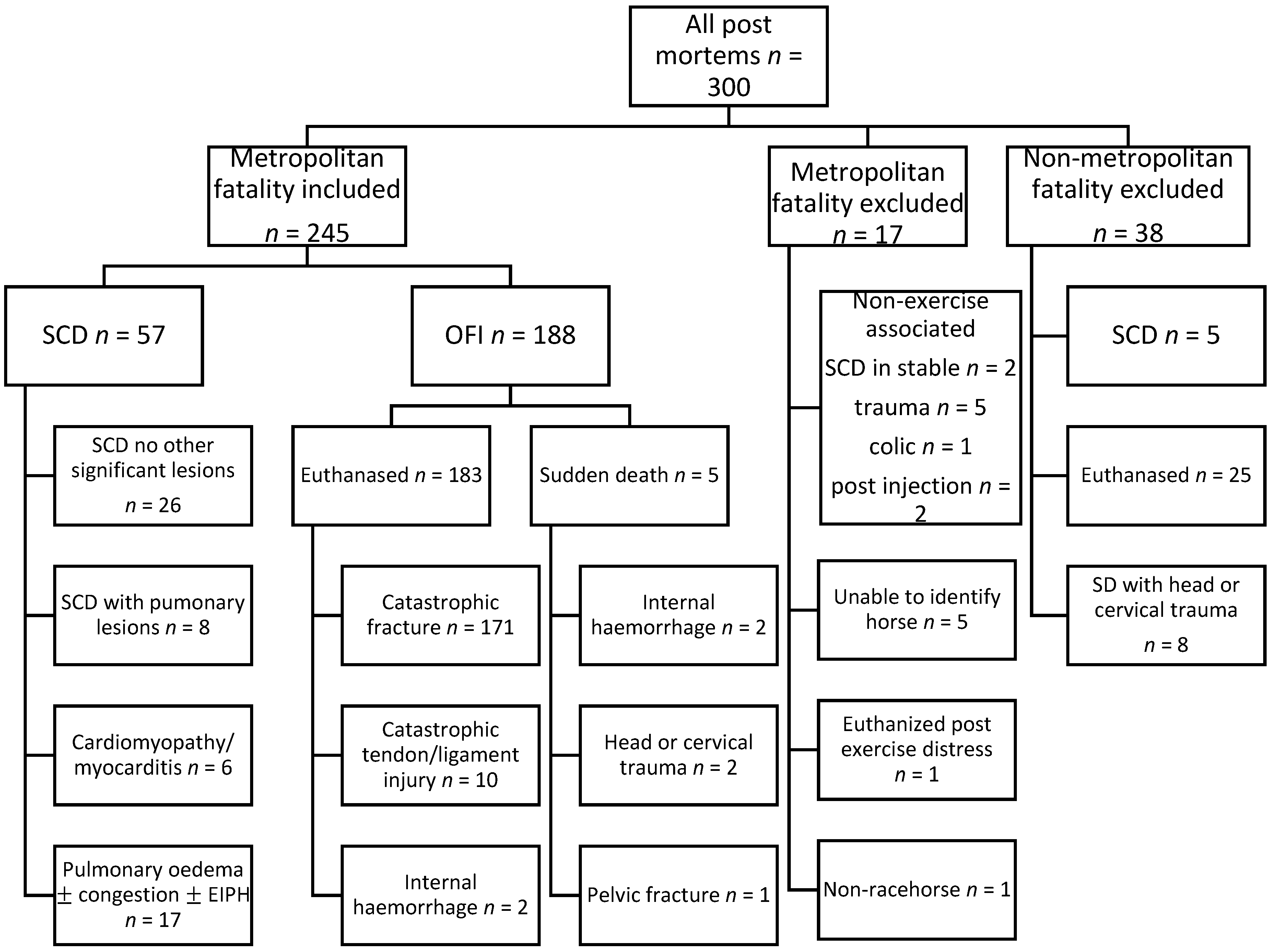
3.2. Post-Mortem Classification
3.3. Risk Factors Associated with SCD
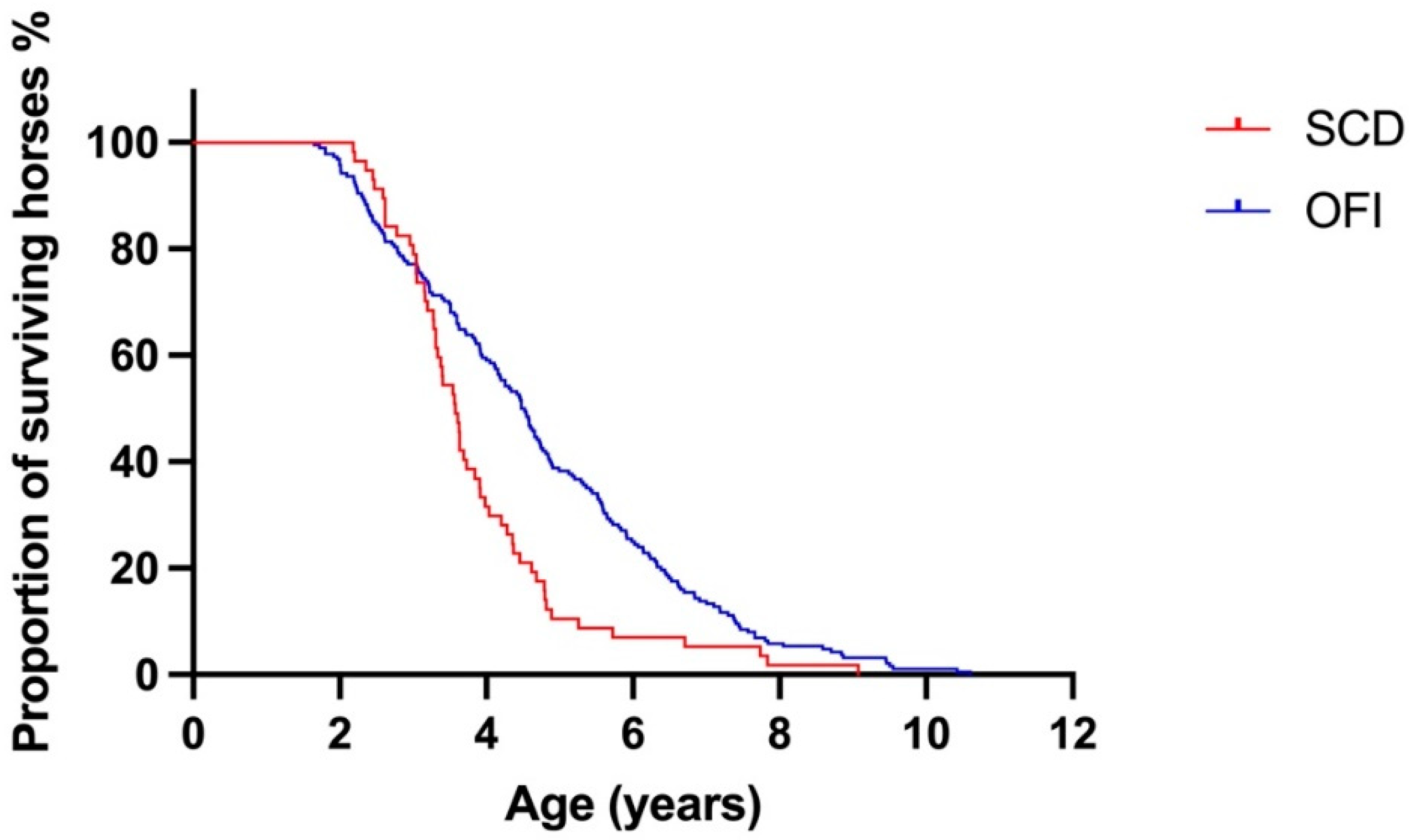
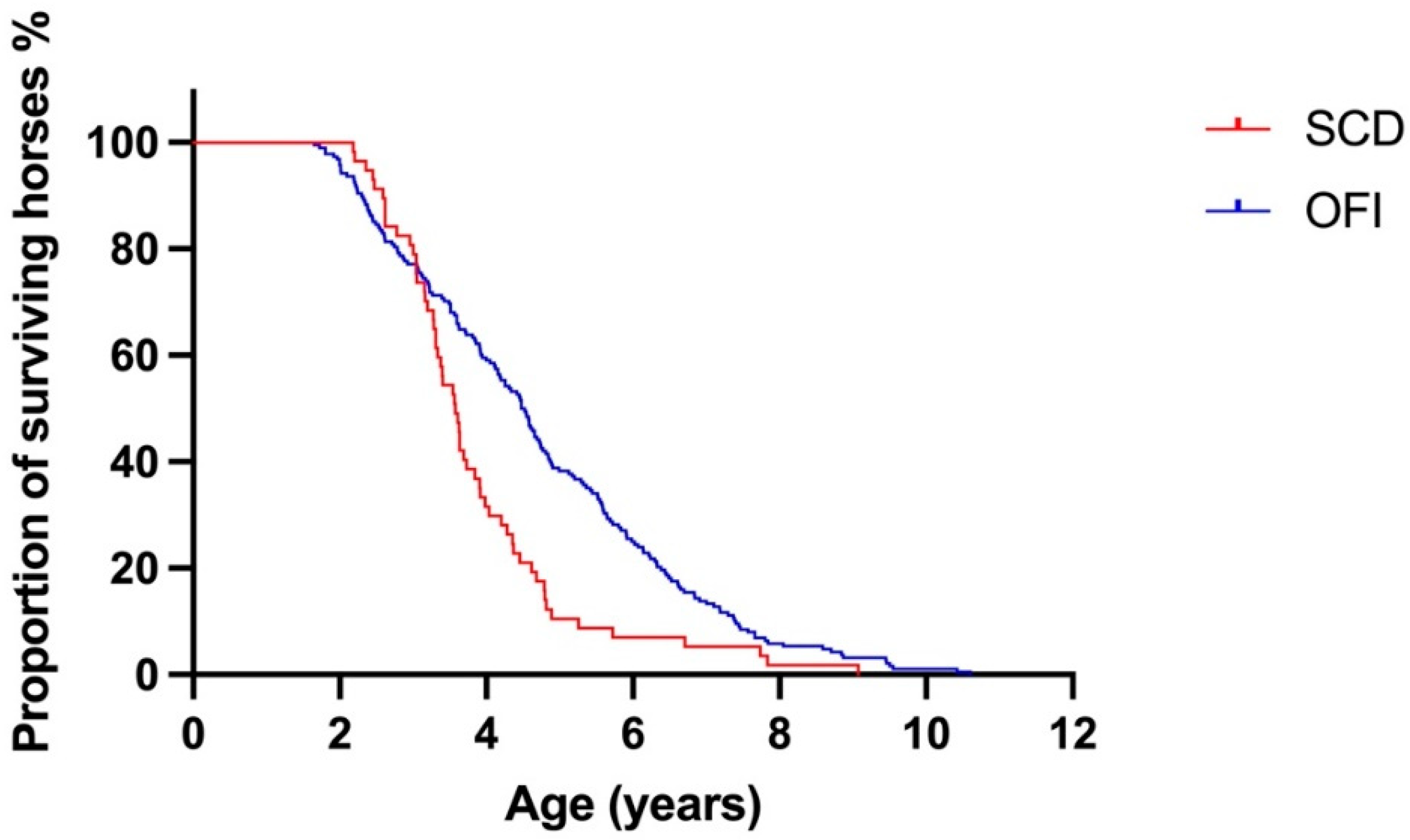
3.4. Survival Analysis
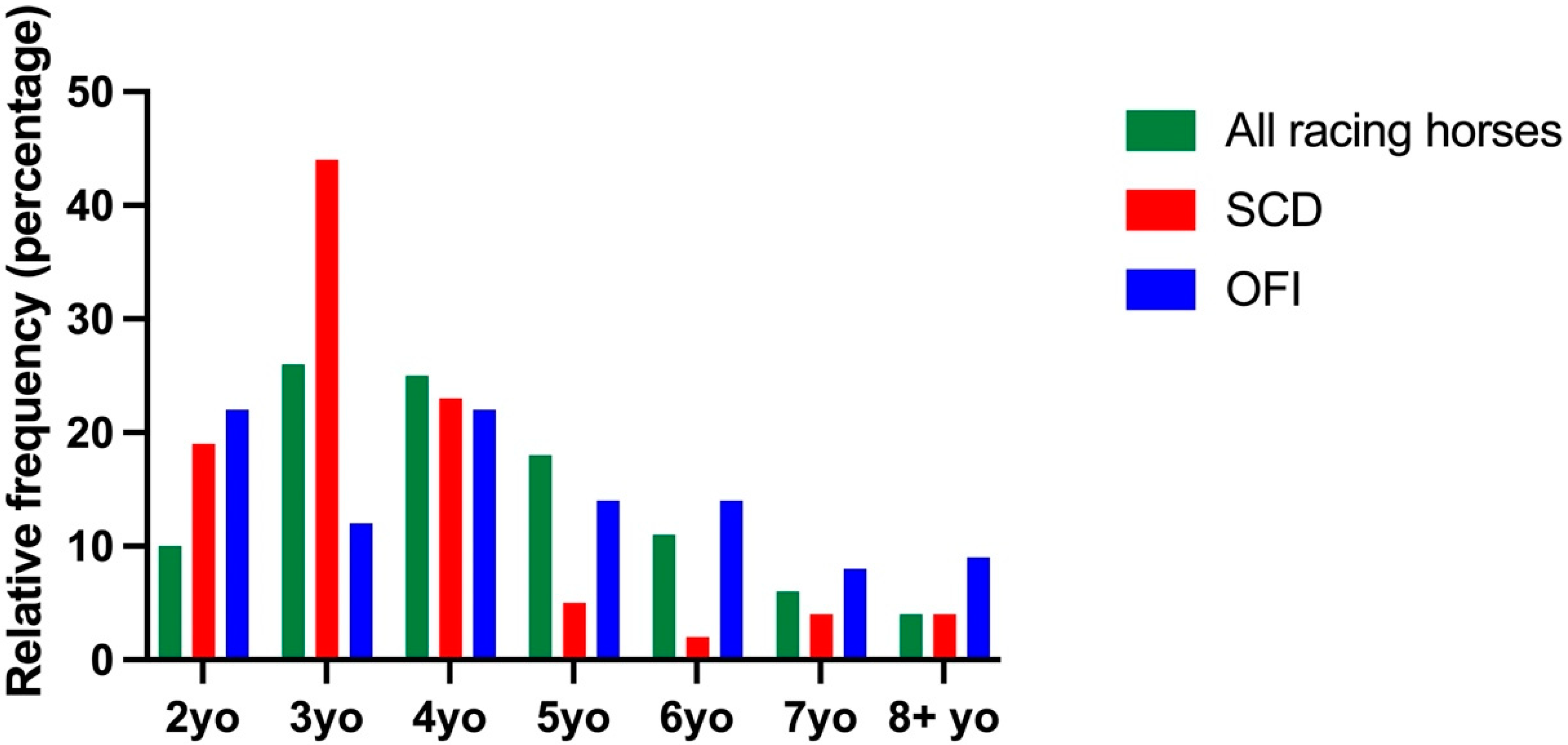
3.5. Comparison of SCD Cases to Horses in the Australian Racing Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kiryu, K.; Machida, N.; Kashida, Y.; Yoshihara, T.; Amada, A.; Yamamoto, T. Pathologic and Electrocardiographic Findings in Sudden Cardiac Death in Racehorses. J. Vet. Med. Sci. 1999, 61, 921–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Physick-Sheard, P.; Avison, A.; Sears, W. Factors Associated with Mortality in Ontario Standardbred Racing: 2003–2015. Animals 2021, 11, 1028. [Google Scholar] [CrossRef] [PubMed]
- Physick-Sheard, P.W.; Slack, J. Irregular hearts and performance horses. Equine Vet. J. 2020, 52, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.E.; Rosanowski, S.M.; Stirk, A.J.; Verheyen, K.L.P. Description of veterinary events and risk factors for fatality in National Hunt flat racing Thoroughbreds in Great Britain (2000–2013). Equine Vet. J. 2017, 49, 700–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyle, C.H.; Uzal, F.A.; McGorum, B.C.; Aida, H.; Blissitt, K.J.; Case, J.T.; Charles, J.T.; Gardner, I.; Horadagoda, N.; Kusano, K.; et al. Sudden death in racing Thoroughbred horses: An international multicentre study of post mortem findings. Equine Vet. J. 2011, 43, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Boden, L.A.; Charles, J.A.; Slocombe, R.F.; Sandy, J.R.; Finnin, P.J.; Morton, J.M.; Clarke, A.F. Sudden death in racing Thoroughbreds in Victoria, Australia. Equine Vet. J. 2005, 37, 269–271. [Google Scholar] [CrossRef]
- Rosanowski, S.M.; Chang, Y.M.; Stirk, A.J.; Verheyen, K.L.P. Descriptive epidemiology of veterinary events in flat racing Thoroughbreds in Great Britain (2000 to 2013). Equine Vet. J. 2017, 49, 275–281. [Google Scholar] [CrossRef] [Green Version]
- Gelberg, H.B.; Zachary, J.F.; Everitt, J.I.; Jensen, R.C.; Smetzer, D.L. Sudden death in training and racing Thoroughbred horses. J. Am. Vet. Med Assoc. 1985, 187, 1354–1356. [Google Scholar]
- Molesan, A.; Wang, M.; Sun, Q.; Pierce, V.; Desideri, R.; Palmer, S. Todhunter R, Kelly K Cardiac pathology and genomics of sudden death in racehorses from New York and Maryland race-tracks. Vet. Pathol. 2019, 56, 576–585. [Google Scholar] [CrossRef]
- Hellings, I.R.; Skjerve, E.; Karlstam, E.; Valheim, M.; Ihler, C.F.; Fintl, C. Racing‐associated fatalities in Norwegian and Swedish harness racehorses: Incidence rates, risk factors, and principal postmortem findings. J. Vet. Intern. Med. 2022, 36, 778–786. [Google Scholar] [CrossRef]
- Corrado, D.; Zorzi, A. Sudden death in athletes. Int. J. Cardiol. 2017, 237, 67–70. [Google Scholar] [CrossRef] [PubMed]
- La Gerche, A. The Potential Cardiotoxic Effects of Exercise. Can. J. Cardiol. 2016, 32, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Finocchiaro, G.; Papadakis, M.; Robertus, J.L.; Dhutia, H.; Steriotis, A.K.; Tome, M.; Mellor, G.; Merghani, A.; Malhotra, A.; Behr, E.; et al. Etiology of Sudden Death in Sports: Insights From a United Kingdom Regional Registry. J. Am. Coll. Cardiol. 2016, 67, 2108–2115. [Google Scholar] [CrossRef] [PubMed]
- Lyle, C.H.; Blissitt, K.J.; Kennedy, R.N.; MC Gorum, B.C.; Newton, J.R.; Parkin, T.D.H.; Stirk, A.; Boden, L.A. Risk factors for race-associated sudden death in Thoroughbred racehorses in the UK (2000–2007). Equine Vet. J. 2012, 44, 459–465. [Google Scholar] [CrossRef] [Green Version]
- Hitchens, P.; Morrice-West, A.; Stevenson, M.; Whitton, R. Meta-analysis of risk factors for racehorse catastrophic musculoskeletal injury in flat racing. Vet. J. 2019, 245, 29–40. [Google Scholar] [CrossRef]
- Verheyen, K.L.P.; Wood, J.L.N. Descriptive epidemiology of fractures occurring in British Thoroughbred racehorses in training. Equine Vet. J. 2004, 36, 167–173. [Google Scholar] [CrossRef]
- Rosanowski, S.M.; Chang, Y.-M.; Stirk, A.J.; Verheyen, K.L.P. Risk factors for race-day fatality in flat racing Thoroughbreds in Great Britain (2000 to 2013). PLoS ONE 2018, 13, e0194299. [Google Scholar] [CrossRef]
- De Solis, C.N.; Althaus, F.; Basieux, N.; Burger, D. Sudden death in sport and riding horses during and immediately after exercise: A case series. Equine Vet. J. 2018, 50, 644–648. [Google Scholar] [CrossRef]
- Ely, E.R.; Avella, C.S.; Price, J.S.; Smith, R.K.W.; Wood, J.L.N.; Verheyen, K.L.P. Descriptive epidemiology of fracture, tendon and suspensory ligament injuries in National Hunt racehorses in training. Equine Vet. J. 2009, 41, 372–378. [Google Scholar] [CrossRef]
- Racing Australia. Available online: https://www.racingaustralia.horse/ (accessed on 2 May 2022).
- Australian Studbook. Available online: https://www.studbook.org.au/ (accessed on 2 May 2022).
- Dehbi, H.-M.; Royston, P.; Hackshaw, A. Life expectancy difference and life expectancy ratio: Two measures of treatment effects in randomised trials with non-proportional hazards. BMJ 2017, 357, j2250. [Google Scholar] [CrossRef] [Green Version]
- Factbook, R.A. Table 56. Age of Individual Horses Racing 2004/05–2019/20. 2021. Available online: http://publishingservices.racingaustralia.horse/otherpublications/FactBook2019-2020/76/ (accessed on 2 May 2022).
- Navas de Solis, C. Exercising arrhythmias and sudden cardiac death in horses: Review of the literature and comparative aspects. Equine Vet. J. 2016, 48, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Boden, L.; Anderson, G.A.; Charles, J.; Morgan, K.L.; Morton, J.M.; Parkin, T.D.H.; Slocombe, R.F.; Clarke, A.F. Risk of fatality and causes of death of Thoroughbred horses associated with racing in Victoria, Australia: 1989–2004. Equine Vet. J. 2006, 38, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Physick-Sheard, P.W.; Avison, A.; Chappell, E.; MacIver, M. Ontario Racehorse Death Registry, 2003–2015: Descriptive analysis and rates of mortality. Equine Vet. J. 2019, 51, 64–76. [Google Scholar] [CrossRef]
- Palmer, S.; Gomez, A.M.M.; Mohammed, H.O. Attrition of Thoroughbred and Standardbred racehorses at New York Racetracks due to exercise and non-exercise related fatalities during the 2016–2019 racing seasons. J. Equine Vet. Sci. 2021, 104, 103703. [Google Scholar] [CrossRef]
- Verheyen, K.L.P. Reducing injuries in racehorses: Mission impossible? Equine Vet. J. 2013, 45, 6–7. [Google Scholar] [CrossRef]
- Crawford, K.L.; Ahern, B.J.; Perkins, N.R.; Phillips, C.J.; Finnane, A. The Effect of Combined Training and Racing High-Speed Exercise History on Musculoskeletal Inju-ries in Thoroughbred Racehorses: A Systematic Review and Meta-Analysis of the Current Literature. Animals 2020, 10, 2091. [Google Scholar] [CrossRef]
- Morrice-West, A.V.; Hitchens, P.L.; Walmsley, E.A.; Stevenson, M.A.; Whitton, R.C. Training practices, speed and distances undertaken by Thoroughbred racehorses in Victoria, Australia. Equine Vet. J. 2020, 52, 273–280. [Google Scholar] [CrossRef]
- Ryan, N.; Marr, C.; McGladdery, A. Survey of cardiac arrhythmias during submaximal and maximal exercise in Thor-oughbred racehorses. Equine Vet. J. 2005, 37, 265–268. [Google Scholar] [CrossRef]
- Marr, C.M.; Franklin, S.; Garrod, G.; Wylie, C.; Smith, L.; Dukes-McEwan, J.; Bright, J.; Allen, K. Exercise-associated rhythm disturbances in poorly performing Thoroughbreds: Risk factors and association with racing performance. Equine Vet. J. 2020, 53, 656–669. [Google Scholar] [CrossRef]
- Physick-Sheard, P.; McGurrin, M. Ventricular arrhythmias during race recovery in Standardbred racehorses and associa-tions with autonomic activity. J. Vet. Int. Med. 2010, 24, 1158–1166. [Google Scholar] [CrossRef]
- De Solis, C.N.; Green, C.; Sides, R.H.; Seino, K.; Bayly, W.M. Arrhythmias in Thoroughbreds During and after Treadmill and Racetrack Exercise. Equine Vet. J. 2016, 46, 24–25. [Google Scholar] [CrossRef]
- Reef, V.B.; Davidson, E.J.; Slack, J.; Stefanovski, D. Hypercapnia and hyperlactatemia were positively associated with higher-grade arrhythmias during peak exercise in horses during poor performance evaluation on a high-speed treadmill. Vet. J. 2020, 266, 105572. [Google Scholar] [CrossRef]
- Whitton, R.C.; Walmsley, E.A.; Wong, A.S.; Shannon, S.M.; Frazer, E.J.; Williams, N.J.; Guerow, J.F.; Hitchens, P.L. Associations between pre-injury racing history and tibial and humeral fractures in Australian Thor-oughbred racehorses. Vet. J. 2019, 247, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Schmied, C.; Basso, C.; Borjesson, M.; Schiavon, M.; Pelliccia, A.; Vanhees, L.; Thiene, G. Risk of sports: Do we need a pre-participation screening for competitive and leisure athletes? Eur. Heart J. 2011, 32, 934–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlstam, E.; Ho, S.Y.; Shokral, A.; Ågren, E.; Michaëlsson, M. Anomalous aortic origin of the left coronary artery in a horse. Equine Vet. J. 1999, 31, 350–352. [Google Scholar] [CrossRef]
- Viu, J.; Armengou, L.; Decloedt, A.; Jose-Cunilleras, E. Investigation of ventricular pre-excitation electrocardiographic pattern in two horses: Clinical presentation and potential causes. J. Vet. Cardiol. 2018, 20, 213–221. [Google Scholar] [CrossRef]
- Jesty, S.A.; Kraus, M.S.; Johnson, A.L.; Gelzer, A.R.; Bartol, J. An accessory bypass tract masked by the presence of atrial fibrillation in a horse. J. Vet. Cardiol. 2011, 13, 79–83. [Google Scholar] [CrossRef]
- Trachsel, D.S.; Calloe, K.; Mykkänen, A.K.; Raistakka, P.; Anttila, M.; Fredholm, M.; Tala, M.; Lamminpää, K.; Klaerke, D.A.; Buhl, R. Exercise-Associated Sudden Death in Finnish Standardbred and Coldblooded Trotters—A Case Series With Pedigree Analysis. J. Equine Vet. Sci. 2021, 104, 103694. [Google Scholar] [CrossRef]
- DeLay, J. Postmortem findings in Ontario racehorses, 2003–2015. J. Vet. Diagn. Investig. 2017, 29, 457–464. [Google Scholar] [CrossRef]
- van de Schoor, F.R.; Aengevaeren, V.L.; Hopman, M.T.; Oxborough, D.L.; George, K.P.; Thompson, P.D.; Eijsvogels, T.M. Myocardial Fibrosis in Athletes. Mayo Clin. Proc. 2016, 91, 1617–1631. [Google Scholar] [CrossRef] [Green Version]
- La Gerche, A.; Burns, A.T.; Mooney, D.J.; Inder, W.; Taylor, A.; Bogaert, J.; MacIsaac, A.I.; Heidbüchel, H.; Prior, D.L. Exercise-induced right ventricular dysfunction and structural remodelling in endurance athletes. Eur. Heart J. 2012, 33, 998–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abela, M.; Sharma, S. ECG in Athletes. In Electrocardiography of Inherited Arrhythmias and Cardiomyopathies: From Basic Science to Clinical Practice; Green, M., Krahn, A., Alqarawi, W., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 137–158. [Google Scholar]
- Mesirca, P.; Nakao, S.; Nissen, S.D.; Forte, G.; Anderson, C.; Trussell, T.; Li, J.; Cox, C.; Zi, M.; Logantha, S.J.R.; et al. Intrinsic Electrical Remodeling Underlies Atrioventricular Block in Athletes. Circ. Res. 2021, 129, e1–e20. [Google Scholar] [CrossRef] [PubMed]
- Chandra, N.; Bastiaenen, R.; Papadakis, M.; Sharma, S. Sudden Cardiac Death in Young Athletes. J. Am. Coll. Cardiol. 2013, 61, 1027–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Camp, S.P.; Bloor, C.M.; Mueller, F.O.; Cantu, R.C.; Olson, H.G. Nontraumatic sports death in high school and college athletes. Med. Sci. Sports Exerc. 1995, 27, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Kiryu, K.; Nakamura, T.; Kaneko, M.; Oikawa, M.-A.O.M.; Yoshihara, T. Cardiopathology of sudden cardiac death in the race horse. Heart Vessel. Suppl. 1987, 2, 40–46. [Google Scholar]
- Eckart, R.E.; Scoville, S.L.; Campbell, C.L.; Shry, E.A.; Stajduhar, K.C.; Potter, R.N.; Pearse, L.A.; Virmani, R. Sudden Death in Young Adults: A 25-Year Review of Autopsies in Military Recruits. Ann. Intern. Med. 2004, 141, 829–834. [Google Scholar] [CrossRef]
- de Noronha, S.V.; Behr, E.R.; Papadakis, M.; Ohta-Ogo, K.; Banya, W.; Wells, J.; Cox, S.; Cox, A.; Sharma, S.; Sheppard, M.N. The importance of specialist cardiac histopathological examination in the investigation of young sudden cardiac deaths. Europace 2014, 16, 899–907. [Google Scholar] [CrossRef]
- Hinchcliff, K.; Couetil, L.; Knight, P.; Morley, P.; Robinson, N.; Sweeney, C.; Van Erck, E. Exercise Induced Pulmonary Hemorrhage in Horses: American College of Veterinary Internal Medicine Consensus Statement. J. Vet. Intern. Med. 2015, 29, 743–758. [Google Scholar] [CrossRef]
- Takahashi, T.; Hiraga, A.; Ohmura, H.; Kai, M.; Jones, J.H. Frequency of and risk factors for epistaxis associated with exercise-induced pulmonary hemorrhage in horses: 251,609 race starts (1992–1997). J. Am. Vet. Med Assoc. 2001, 218, 1462–1464. [Google Scholar] [CrossRef]
- Weideman, H.; Schoeman, S.J.; Jordaan, G.F.; Kidd, M. Epistaxis related to exercise-induced pulmonary haemorrhage in South African Thoroughbreds. J. S. Afr. Vet. Assoc. 2003, 74, 127–131. [Google Scholar] [CrossRef]
- Morrice-West, A.V.; Hitchens, P.L.; Walmsley, E.A.; Stevenson, M.A.; Wong, A.S.; Whitton, R.C. Variation in GPS and accelerometer recorded velocity and stride parameters of galloping Thoroughbred horses. Equine Vet. J. 2021, 53, 1063–1074. [Google Scholar] [CrossRef] [PubMed]
- Frippiat, T.; van Beckhoven, C.; Moyse, E.; Art, T. Accuracy of a heart rate monitor for calculating heart rate variability parameters in exercising horses. J. Equine Vet. Sci. 2021, 104, 103716. [Google Scholar] [CrossRef] [PubMed]
- Mott, R.; Dowell, F.; Evans, N. Use of the Polar V800 and Actiheart 5 heart rate monitors for the assessment of heart rate variability (HRV) in horses. Appl. Anim. Behav. Sci. 2021, 241, 105401. [Google Scholar] [CrossRef]
- Haughan, J.; Manriquez, M.; Cohen, N.; Robinson, M.; de Solis, C.N. Comparison of novel wearable cardiac monitors to yield accurate exercising ECG and heart rate data in horses. Comp. Exerc. Physiol. 2021, 17, 457–465. [Google Scholar] [CrossRef]
- Ter Woort, F.; Dubois, G.; Didier, M.; Van Erck-Westergren, E. Validation of an equine fitness tracker: Heart rate and heart rate variability. Comp. Exerc. Physiol. 2021, 17, 189–198. [Google Scholar] [CrossRef]
- Mitchell, K.J.; Schwarzwald, C.C. Heart rate variability analysis in horses for the diagnosis of arrhythmias. Vet. J. 2021, 268, 105590. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable Continuous, Median (IQR) Categorical, Proportion (%[95% CI]) | SCD n = 57 | OFI n = 188 | Coeff | Log Odds Ratio | OR 95% CI | p Value |
|---|---|---|---|---|---|---|
| Age (years) | 3.58 (3.05–4.36) | 4.50 (3.12–6.02) | −0.27 | 0.76 | 0.62–0.91 | <0.001 |
| Sex | ||||||
| Gelding Female Entire male | 27 (47[35–60]%) 21 (37[25–50]%) 9 (16[8–28]%) | 94 (50[43–57]%) 48 (25[10–32]%) 46 (24[19–31]%) | −0.11 1.18 −2.90 | 0.90 3.24 0.05 | 0.50–1.63 1.76–6.03 0.00–0.26 | 0.73 <0.001 <0.001 |
| Hemisphere of origin | ||||||
| Southern hemi (REF) Northern hemi | 53 (93[83–98]%) 4 (7[2–17]%) | 171 (91[86–94]%) 17 (9[6–14]%) | −0.27 | 0.76 | 0.21–2.17 | 0.63 |
| Sire hemisphere of origin | ||||||
| Southern hemi (REF) Northern hemi | 36 (63[50–75]%) 21 (37[25–50]%) | 98 (52[45–69]%) 90 (48[41–55]%) | −0.45 | 0.64 | 0.34–1.16 | 0.14 |
| Dam hemisphere of origin | ||||||
| Southern hemi (REF) Northern hemi | 48 (83[71–91]%) 9 (17[9–29]%) | 155 (82[76–87]%) 33 (18[23–34]%) | −0.13 | 0.88 | 0.37–1.90 | 0.76 |
| Exercise type | ||||||
| Racing (REF) Training | 15 (26[17–39]%) 42 (74[63–81]%) | 106 (56[49–63]%) 82 (44[37–51]%) | 1.29 | 3.62 | 1.91–7.16 | <0.001 |
| Lifetime starts | 3 (0–9.0) | 9 (0–22.75) | −0.05 | 0.95 | 0.91–0.97 | <0.001 |
| Season | ||||||
| Summer Autumn Winter Spring | 16 (28[18–41]%) 11 (19[11–31]%) 15 (26[17–39]%) 15 (26[17–39]%) | 46 (24[19–31]%) 46 (24[19–31]%) 42 (22[17–29]%) 54 (29[23–36]%) | 0.19 −0.30 0.22 −0.12 | 1.20 0.74 1.24 0.89 | 0.61–2.32 0.34–1.50 0.61–2.42 0.44–1.70 | 0.58 0.42 0.53 0.72 |
| Variable Continuous, Median (IQR) Categorical, Proportion (%[95% CI}) | SCD n = 57 | OFI n = 188 | Coeff | Log Odds Ratio | OR 95% CI | p Value |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Gelding (REF) Female Entire male | 27 (47[35–60]%) 21 (37[25–50]%) 9 (16[8–28]%) | 94 (50[43–57]%) 48 (25[10–32]%) 46 (25[19–31]%) | −0.04 −1.00 | 0.96 0.37 | 0.45–2.02 0.14–0.89 | 0.91 0.03 |
| Sire hemisphere of origin | ||||||
| Southern hemi (REF) Northern hemi | 36 (63[50–75]%) 21 (37[25–50]%) | 98 (52[45–69]%) 90 (48[41–55]%) | −0.28 | 0.76 | 0.39–1.44 | 0.40 |
| Exercise type | ||||||
| Racing (REF) Training | 15 (26[17–39]%) 42 (74[63–81]%) | 106 (56[49–63]%) 82 (44[37–51]%) | 0.93 | 2.53 | 1.22–5.41 | 0.01 |
| Lifetime starts | 3 (0–9.0) | 9 (0–22.75) | −0.04 | 0.96 | 0.92–0.99 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nath, L.; Stent, A.; Elliott, A.; La Gerche, A.; Franklin, S. Risk Factors for Exercise-Associated Sudden Cardiac Death in Thoroughbred Racehorses. Animals 2022, 12, 1297. https://doi.org/10.3390/ani12101297
Nath L, Stent A, Elliott A, La Gerche A, Franklin S. Risk Factors for Exercise-Associated Sudden Cardiac Death in Thoroughbred Racehorses. Animals. 2022; 12(10):1297. https://doi.org/10.3390/ani12101297
Chicago/Turabian StyleNath, Laura, Andrew Stent, Adrian Elliott, Andre La Gerche, and Samantha Franklin. 2022. "Risk Factors for Exercise-Associated Sudden Cardiac Death in Thoroughbred Racehorses" Animals 12, no. 10: 1297. https://doi.org/10.3390/ani12101297
APA StyleNath, L., Stent, A., Elliott, A., La Gerche, A., & Franklin, S. (2022). Risk Factors for Exercise-Associated Sudden Cardiac Death in Thoroughbred Racehorses. Animals, 12(10), 1297. https://doi.org/10.3390/ani12101297