
Immunohistochemical Expression of Neurokinin-A and Interleukin-8 in the Bronchial Epithelium of Horses with Severe Equine Asthma Syndrome during Asymptomatic, Exacerbation, and Remission Phase

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Horses
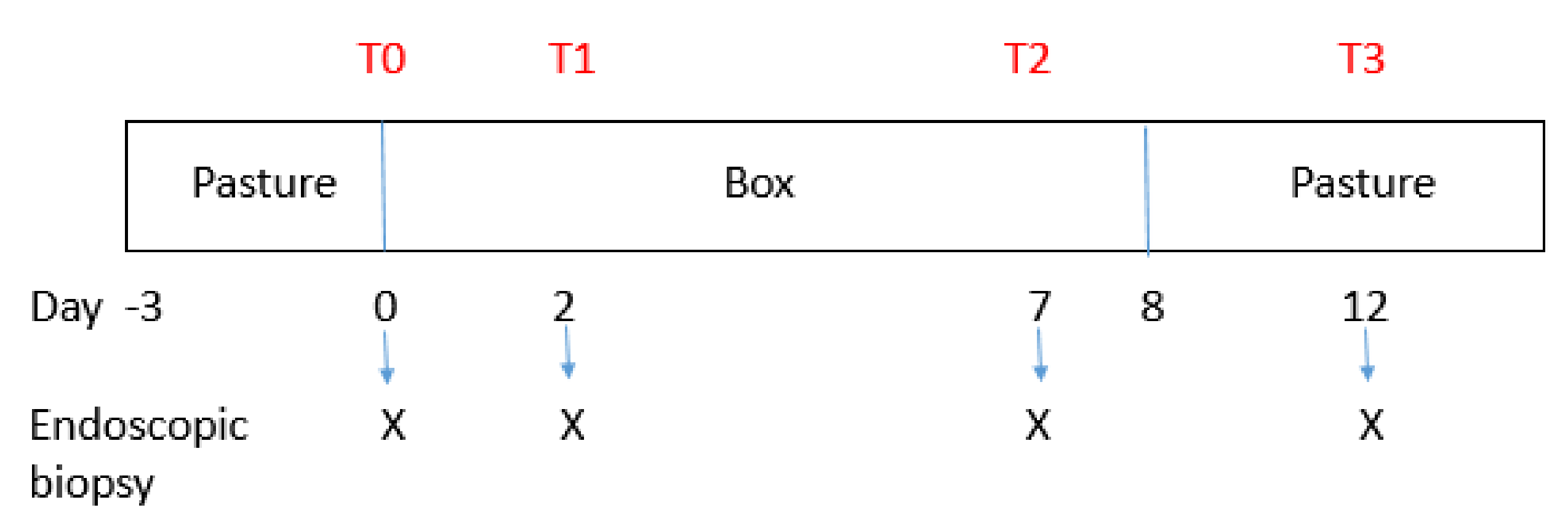
2.2. Experimental Design
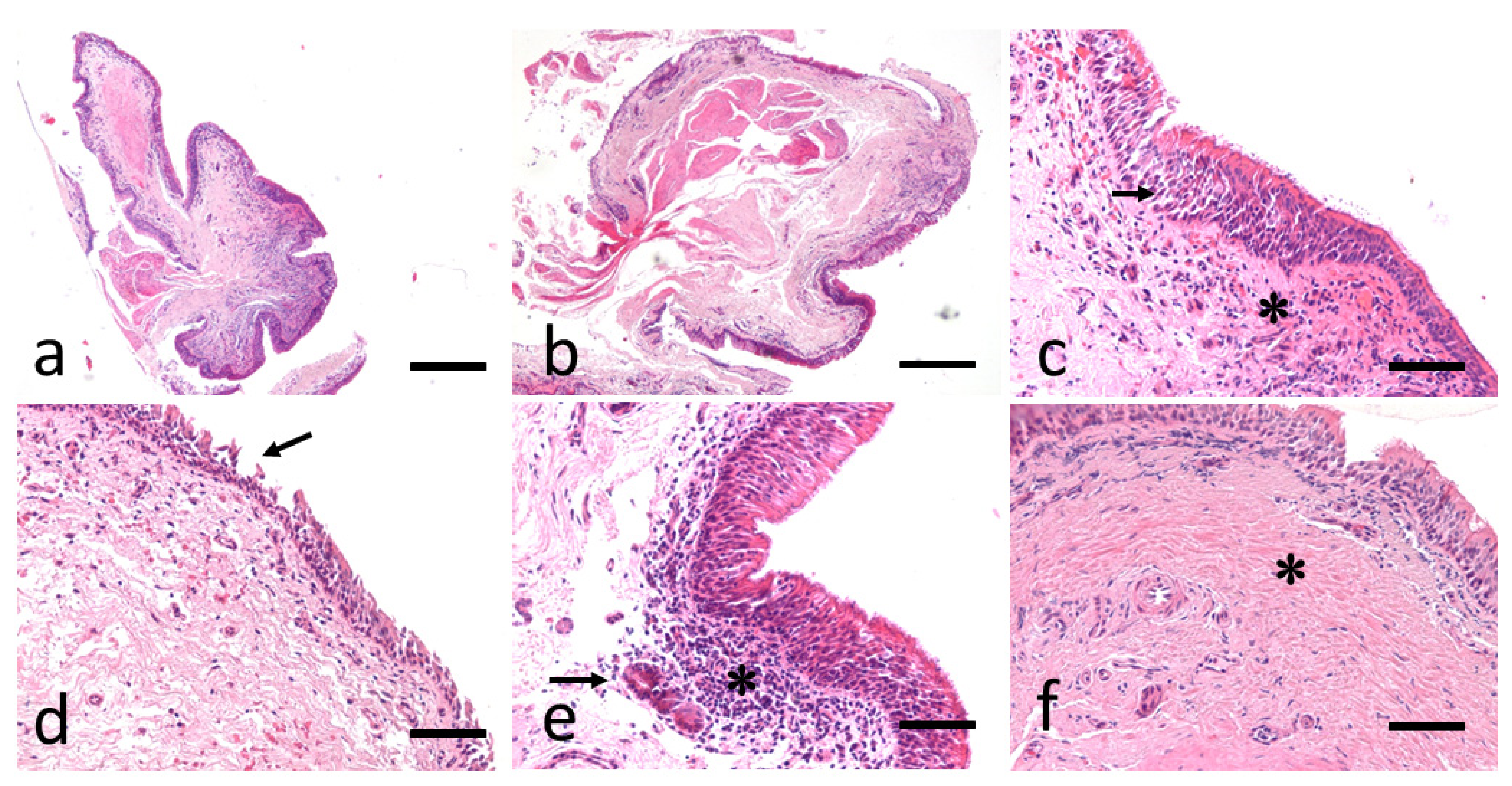
2.3. Bronchial Biopsy Histology
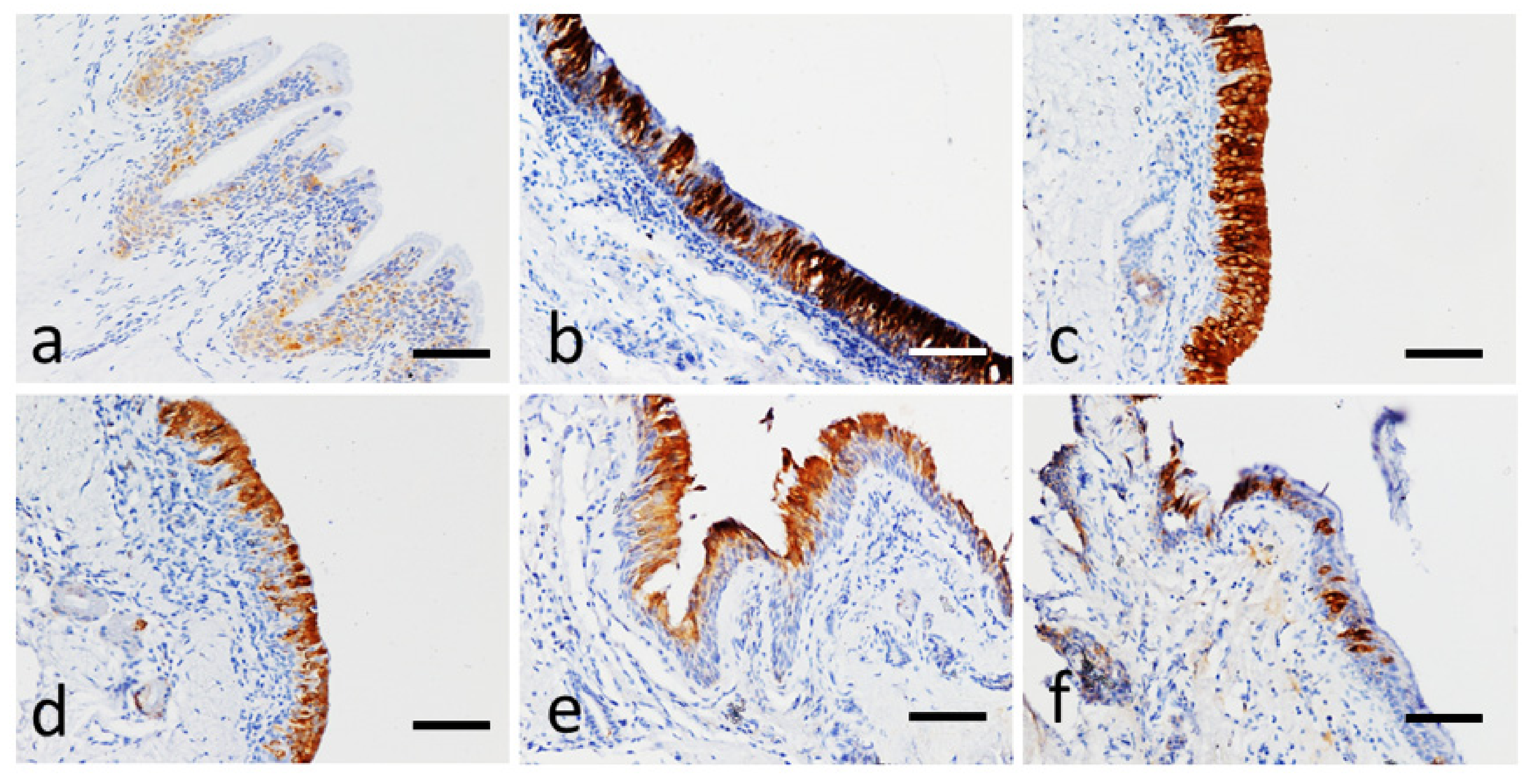
2.4. Immunohistochemical Analysis for Neurokinin A and IL-8
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martin, B.B., Jr.; Reef, V.B.; Parente, E.J.; Sage, A.D. Causes of poor performance of horses during training, racing, or showing: 348 cases (1992–1996). J. Am. Vet. Med. Assoc. 2000, 216, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Bullone, M.; Lavoie, J.P. Science-in-brief: Equine asthma diagnosis: Beyond bronchoalveolar lavage cytology. Equine Vet. J. 2017, 49, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Couetil, L.; Cardwell, J.M.; Leguillette, R.; Mazan, M.; Richard, E.; Bienzle, D.; Bullone, M.; Gerber, V.; Ivester, K.; Lavoie, J.P.; et al. Equine Asthma: Current Understanding and Future Directions. Front. Vet. Sci. 2020, 7, 450. [Google Scholar] [CrossRef]
- Couetil, L.L.; Cardwell, J.M.; Gerber, V.; Lavoie, J.P.; Leguillette, R.; Richard, E.A. Inflammatory airway disease of horses–revised Consensus statement. J. Vet. Intern. Med. 2016, 30, 503–515. [Google Scholar] [CrossRef] [PubMed]
- Tessier, L.; Côté, O.; Clark, M.E.; Viel, L.; Diaz-Méndez, A.; Anders, S.; Bienzle, D. Impaired response of the bronchial epithelium to inflammation characterizes severe equine asthma. BMC Genom. 2017, 18, 708. [Google Scholar] [CrossRef]
- Bond, S.; Léguillette, R.; Richard, E.A.; Couetil, L.; Lavoie, J.P.; Martin, J.G.; Pirie, R.S. Equine asthma: Integrative biologic relevance of a recently proposed nomenclature. J. Vet. Int. Med. 2018, 32, 2088–2098. [Google Scholar] [CrossRef]
- Seahorn, T.L.; Beadle, R.E. Summer pasture-associated obstructive pulmonary disease in horses: 21 cases (1983–1991). J. Am. Vet. Med. Assoc. 1993, 202, 779–782. [Google Scholar]
- McGorum, B.C.; Ellison, J.; Cullen, R.T. Total and respirable airborne dust endotoxin concentrations in three management systems. Equine Vet. J. 1998, 30, 430–434. [Google Scholar] [CrossRef]
- Vandenput, S.; Votion, D.; Duvivier, D.H.; van Erck, E.; Anciaux, N.; Art, T.; Lekeux, P. Effect of a set stabled environmental control on pulmonary function and airway reactivity of COPD affected horses. Vet. J. 1998, 155, 189–195. [Google Scholar] [CrossRef]
- Tremblay, G.M.; Ferland, C.; Lapointe, J.M.; Vrins, A.; Lavoie, J.P.; Cormier, Y. Effect of stabling on bronchoalveolar cells obtained from normal al COPD horses. Equine Vet. J. 1993, 25, 194–197. [Google Scholar] [CrossRef]
- Pirie, R.S. Recurrent airway obstruction: A review. Equine Vet. J. 2014, 46, 276–288. [Google Scholar] [CrossRef]
- Fogarty, U.; Buckley, T. Bronchoalveolar lavage findings in horses with exercise intolerance. Equine Vet. J. 1991, 23, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Holcombe, S.J.; Jackson, C.; Gerber, V.; Jefcoat, A.; Berney, C.; Eberhardt, S.; Robinson, N.E. Stabling is associated with airway inflammation in young Arabian horses. Equine Vet. J. 2001, 33, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Jean, D.; Vrins, A.; Beauchamp, G.; Lavoie, J.P. Evaluation of variations in bronchoalveolar lavage fluid in horses with recurrent airway obstruction. Am. J. Vet. Res. 2011, 72, 838–842. [Google Scholar] [CrossRef]
- Hoffman, A.M. Bronchoalveolar lavage: Sampling technique and guidelines for cytologic preparation and interpretation. Vet. Clin. N. Am. Equine Pract. 2008, 24, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Couetil, L.L.; Thompson, C.A. Airway Diagnostics: Bronchoalveolar Lavage, Tracheal Wash, and Pleural Fluid. Vet. Clin. N. Am. Equine Pract. 2020, 36, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Bullone, M.; Helie, P.; Joubert, P.; Lavoie, J.P. Development of a Semiquantitative Histological Score for the Diagnosis of Heaves Using Endobronchial Biopsy Specimens in Horses. J. Vet. Intern. Med. 2016, 30, 1739–1746. [Google Scholar] [CrossRef]
- Niedzwiedz, A.; Mordak, R.; Jaworski, Z.; Nicponc, J. Utility of the Histological Examination of the Bronchial Mucosa in the Diagnosis of Severe Equine Asthma Syndrome in Horses. J. Equine Vet. Sci. 2018, 67, 44–49. [Google Scholar] [CrossRef]
- Ainsworth, D.M.; Grünig, G.; Matychak, M.B.; Young, J.; Wagner, B.; Erb, H.N.; Antczak, D.F. Recurrent airway obstruction (RAO) in horses is characterized by IFN-γ and IL-8 production in bronchoalveolar lavage cells. Vet. Immun. Immunopathol. 2003, 96, 83–91. [Google Scholar] [CrossRef]
- Venugopal, C.S.; Holmes, E.P.; Polikepahad, S.; Laborde, M.K.; Moore, R.M. Neurokinin receptors in recurrent airway obstruction; a comparative study of affected and unaffected horses. Can. J. Vet. Res. 2009, 73, 25–33. [Google Scholar]
- Buechner-Maxwell, V. Airway hyperresponsiveness. Compend. Contin. Educ. Pract. Vet. 1993, 15, 1379–1389. [Google Scholar]
- Brazil, T.J.; McGorum, B.C. Molecules and inflammation in equine heaves: Mechanism and markers of disease. Equine Vet. J. 2001, 33, 113–115. [Google Scholar] [CrossRef]
- Calzetta, L.; Rogliani, P.; Pistocchini, E.; Mattei, M.; Cito, G.; Alfonsi, P.; Page, C.; Matera, M.G. Effect of lipopolysaccharide on the responsiveness of equine bronchial tissue. Pulm. Pharmacol. Ther. 2018, 49, 88–94. [Google Scholar] [CrossRef]
- Wada, R.; Aida, H.; Kaneko, M.; Oikawa, M.; Yoshihara, T.; Tomioka, Y.; Nitta, M. Identification of the bronchi for bronchoscopy in the horse and segmentation of the horse lung. Jpn. J. Equine Sci. 1992, 3, 37–43. [Google Scholar] [CrossRef]
- Rush, B.R.; Raub, E.S.; Rhoads, W.S.; Flaminio, M.J.; Matson, C.J.; Hakala, J.E.; Gillespie, J.R. Pulmonary function in horses with recurrent airway obstruction after aerosol and parenteral administration of beclomethasone dipropionate and dexamethasone, respectively. Am. J. Vet. Res. 1998, 59, 1039–1043. [Google Scholar]
- Leclere, M.; Lavoie-Lamoureux, A.; Lavoie, J.P. Heaves, an asthma-like disease of horses. Respirology 2011, 16, 1027–1046. [Google Scholar] [CrossRef]
- Ferrari, C.R.; Cooley, J.; Mujahid, N.; Costa, L.R.; Wills, R.W.; Johnson, M.E.; Swiderski, C.E. Horses with pasture asthma have airway remodelling that is characteristic of human asthma. Vet. Pathol. 2018, 55, 144–158. [Google Scholar] [CrossRef]
- Bullone, M.; Lavoie, J.P. Asthma “of horses and men”—How can equine heaves help us better understand human asthma immunopathology and its functional consequences? Mol. Immunol. 2015, 66, 97–105. [Google Scholar] [CrossRef]
- Woort, F.T.; Caswell, J.L.; Arroyo, L.G.; Viel, L. Histologic investigation of airway inflammation in postmortem lung samples from racehorses. Am. J. Vet. Res. 2018, 79, 342–347. [Google Scholar] [CrossRef]
- Giguère, S.; Prescott, J.F. Quantitation of equine cytokine mRNA expression by transcription-competitive polymerase chain reaction. Vet. Immunol. Immunopathol. 1999, 67, 1–15. [Google Scholar] [CrossRef]
- Swiderski, C.E.; Klei, T.R.; Horohov, D.W. Quantitative measurement of equine cytokine mRNA expression by polymerase chain reaction using target-specific standard curves. J. Immunol. Methods 1999, 222, 155–169. [Google Scholar] [CrossRef]
- Joubert, P.; Silversides, D.W.; Lavoie, J.P. Equine neutrophils express mRNA for tumor necrosis factor-α, interleukin (IL)-1β, IL-6, IL-8, macrophage-inflammatory-protein-2 but not for IL-4, IL-5 and interferon-γ. Equine Vet. J. 2001, 33, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Beadle, R.E.; Horohov, D.W.; Gaunt, S.D. Interleukin-4 and interferon-gamma gene expression in summer pasture-associated obstructive pulmonary disease affected horses. Equine Vet. J. 2002, 34, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Joubert, P.; Cordeau, M.E.; Boyer, A.; Silversides, D.W.; Lavoie, J.P. Quantification of mRNA expression by peripheral neutrophils in an animal model of asthma. Am. J. Respir. Crit. Care Med. 2002, 165, A317. [Google Scholar]
- Horohov, D.W.; Beadle, R.E.; Mouch, S.; Pourciau, S.S. Temporal regulation of cytokine mRNA expression in equine recurrent airway obstruction. Vet. Immunol. Immunopathol. 2005, 108, 237–245. [Google Scholar] [CrossRef]
- Laan, T.T.; Bull, S.; Pirie, R.S.; Fink-Gremmels, J. Evaluation of cytokine production by equine alveolar macrophages exposed to lipopolysaccharide, Aspergillus fumigatus, and a suspension of hay dust. Am. J. Vet. Res. 2005, 66, 1584–1589. [Google Scholar] [CrossRef]
- Ainsworth, D.M.; Wagner, B.; Franchini, M.; Grünig, G.; Erb, H.N.; Tan, J.Y. Time-dependent alterations in gene expression of interleukin-8 in the bronchial epithelium of horses with recurrent airway obstruction. Am. J. Vet. Res. 2006, 67, 669–677. [Google Scholar] [CrossRef]
- Riihimäki, M.; Raine, A.; Art, T.; Lekeux, P.; Couëtil, L.; Pringle, J. Partial divergence of cytokine mRNA expression in bronchial tissues compared to bronchoalveolar lavage cells in horses with recurrent airway obstruction. Vet. Immunol. Immunopathol. 2008, 122, 256–264. [Google Scholar] [CrossRef]
- Klukowska-Rotzler, J.; Swinburne, J.E.; Drogemuller, C.; Dolf, G.; Janda, J.; Leeb, T.; Gerber, V. The interleukin 4 receptor gene and its role in recurrent airway obstruction in Swiss Warmblood horses. Anim. Genet. 2012, 43, 450–453. [Google Scholar] [CrossRef]
- Padoan, E.; Ferraresso, S.; Pegolo, S.; Castagnaro, M.; Barnini, C.; Bargelloni, L. Real time RT-PCR analysis of inflammatory mediator expression in recurrent airway obstruction-affected horses. Vet. Immunol. Immunopathol. 2013, 156, 190–199. [Google Scholar] [CrossRef]
- Barton, A.K.; Gehlen, G. Pulmonary Remodelling in Equine Asthma: What Do We Know about Mediators of Inflammation in the Horse? Mediat. Inflamm. 2016, 2016, 5693205. [Google Scholar] [CrossRef]
- Kraneveld, A.D.; Nijkamp, F.P.; Van Oosterhout, A.J. Role for neurokinin-2 receptor in interleukin-5-induced airway hyperresponsiveness but not eosinophilia in guinea pigs. Am. J. Respir. Crit. Care Med. 1997, 156, 367–374. [Google Scholar] [CrossRef]
- Fattori, D.; Altamura, M.; Maggi, C.A. Small molecule antagonists of the tachykinin NK 2 receptor. Mini-Rev. Med. Chem. 2004, 4, 331–340. [Google Scholar] [CrossRef]
- Pennefather, J.N.; Lecci, A.; Candenas, M.L.; Patak, E.; Pinto, F.M.; Maggi, C.A. Tachykinins and tachykinin receptors: A growing family. Life Sci. 2004, 74, 1445–1463. [Google Scholar] [CrossRef]
- Maggi, C.A.; Patacchini, R.; Santicioli, P.; Giuliani, S. Tachykinin antagonists and capsaicin-induced contraction of the rat isolated urinary bladder: Evidence for tachykinin-mediated cotransmission. Br. J. Pharmacol. 1991, 103, 1535–1541. [Google Scholar] [CrossRef]
- Krishnakumar, S.; Holmes, E.P.; Moore, R.M.; Kappel, L.; Venugopal, C.S. Non-adrenergic non-cholinergic excitatory innervation in the airways: Role of neurokinin-2 receptors. Auton. Autacoid Pharmacol. 2002, 22, 215–224. [Google Scholar] [CrossRef]
- Schelfhout, V.; Van De Velde, V.; Maggi, C.; Pauwels, R.; Joo, G. The effect of the tachykinin NK2 receptor antagonist MEN11420 (nepadutant) on neurokinin A induced bronchoconstriction in asthmatics. Ther. Adv. Respir. Dis. 2009, 3, 219–226. [Google Scholar] [CrossRef]
- Calzetta, L.; Luongo, L.; Cazzola, M.; Page, C.; Rogliani, P.; Facciolo, F.; Maione, S.; Capuano, A.; Rinaldi, B.; Matera, M.G. Contribution of sensory nerves to LPS-induced hyperresponsiveness of human isolated bronchi. Life Sci. 2015, 131, 44–50. [Google Scholar] [CrossRef]
- Advenier, C.; Lagente, V.; Boichot, E. The role of tachykinin receptor antagonists in the prevention of bronchial hyperresponsiveness, airway inflammation and cough. Eur. Respir. J. 1997, 10, 1892–1906. [Google Scholar] [CrossRef]
- Solinger, N.; Sonea, I.M. Distribution of the neurokinin-1 receptor in equine intestinal smooth muscle. Equine Vet. J. 2008, 40, 321–325. [Google Scholar] [CrossRef]
- Lavoie, J.P.; Maghni, K.; Desnoyers, M.; Rame, T.; Martin, J.G.; Hamid, Q.A. Neutrophilic airway inflammation in horses with heaves is characterized by a Th2-type cytokine profile. Am. J. Respir. Crit. Care Med. 2001, 164, 1410–1413. [Google Scholar] [CrossRef]
- Giguere, S.; Viel, L.; Lee, E.; MacKay, R.J.; Hernandez, J.; Franchini, M. Cytokine induction in pulmonary airways of horses with heaves and effect of therapy with inhaled fluticasone propionate. Vet. Immunol. Immunopathol. 2002, 85, 147–158. [Google Scholar] [CrossRef]
- Cordeau, M.E.; Joubert, P.; Dewachi, O.; Hamid, Q.; Lavoie, J.P. IL-4, IL-5 and IFNgamma mRNA expression in pulmonary lymphocytes in equine heaves. Vet. Immunol. Immunopathol. 2004, 97, 87–96. [Google Scholar] [CrossRef]
- Hansen, S.; Otten, N.D.; Bircha, K.; Skovgaard, K.; Hopster-Iversen, C.; Fjeldborg, J. Bronchoalveolar lavage fluid cytokine, cytology and IgE allergen in horses with equine asthma. Vet. Immunol. Immunopathol. 2020, 220, 109976. [Google Scholar] [CrossRef]
- Moran, G.; Folch, H. Recurrent airway obstruction in horses—An allergic inflammation: A review. Vet. Med. 2011, 56, 1–13. [Google Scholar] [CrossRef]
- Leguillette, R. Recurrent airway obstruction—Heaves. Vet. Clin. Equine 2003, 19, 63–86. [Google Scholar] [CrossRef]
- Laan, T.T.J.M.; Bull, S.; Pirie, R.S.; Fink-Gremmels, J. The role of alveolar macrophages in the pathogenesis of recurrent airway obstruction in horses. J. Vet. Intern. Med. 2006, 20, 167–174. [Google Scholar] [CrossRef]
- Franchini, M.; Gill, U.; Von Fellenberg, R.; Bracher, V.D. Interleukin-8 concentration and neutrophil chemotactic activity in bronchoalveolar lavage fluid of horses with chronic obstructive pulmonary disease following exposure to hay. Am. J. Vet. Res. 2000, 61, 1369–1374. [Google Scholar] [CrossRef]
- Ainsworth, D.M.; Matychak, M.; Reyner, C.L.; Erb, H.N.; Young, J.C. Effects of in vitro exposure to hay dust on the gene expression of chemokines and cell-surface receptors in primary bronchial epithelial cell cultures established from horses with chronic recurrent airway obstruction. Am. J. Vet. Res. 2009, 70, 365–372. [Google Scholar] [CrossRef]
- Ainsworth, D.M.; Wagner, B.; Erb, H.N.; Young, J.C.; Retallick, D.E. Effects of in vitro exposure to hay dust on expression of interleukin-17, -23, -8, and -1beta and chemokine (C-X-C motif) ligand 2 by pulmonary mononuclear cells isolated from horses chronically affected with recurrent airway disease. Am. J. Vet. Res. 2007, 68, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Berndt, A.; Derksen, F.J.; Venta, P.J.; Ewart, S.; Yuzbasiyan-Gurkan, V.; Robinson, N.E. Elevated amount of Toll-like receptor 4 mRNA in bronchial epithelial cells is associated with airway inflammation in horses with recurrent airway obstruction. Am. J. Physiol. Lung Cell. Mol. Physiol. 2007, 292, L936–L943. [Google Scholar] [CrossRef] [PubMed]
- Reyner, C.L.; Wagner, B.; Young, J.C.; Ainsworth, D.M. Effects of in vitro exposure to hay dust on expression of interleukin-23, -17, -8, and -1beta and chemokine (C-X-C motif) ligand 2 by pulmonary mononuclear cells from horses susceptible to recurrent airway obstruction. Am. J. Vet. Res. 2009, 70, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Pietra, M.; Peli, A.; Bonato, A.; Ducci, A.; Cinotti, S. Equine bronchoalveolar lavage cytokines in the development of Recurrent Airway Obstruction. Vet. Res. Commun. 2007, 31, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Pietra, M.; Cinotti, S.; Ducci, A.; Giunti, M.; Peli, A. Time-dependent changes of cytokines mRNA in bronchoalveolar lavage fluid from symptomatic recurrent airway obstruction-affected horses. Pol. J. Vet. Sci. 2011, 14, 343–351. [Google Scholar] [CrossRef][Green Version]
- Hansen, S.; Baptiste, K.E.; Fjeldborg, J.; Betancourt, A.; Horohov, D.W. A comparison of pro-inflammatory cytokine mRNA expression in equine bronchoalveolar lavage (BAL) and peripheral blood. Vet. Immunol. Immunopathol. 2014, 158, 238–243. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | EA-Affected | EA-Affected | EA-Affected | EA-Affected | |
|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | ||
| Histological score (0–10) | 3 | 5.5 | 5 | 6.5 | 7.5 |
| median (min-max) | (2–4) | (4–6) | (4–8) | (5–10) | (5–9) |
| p | p = 0.92 | p = 0.48 | p = 0.16 | p = 0.63 | p = 0.81 |
| NKA immunoreactivity score | |||||
| Intensity of positivity (0–4) | 2 | 3 | 3 | 3 | 4 |
| median (min-max) | (2–3) | (1–4) | (2–4) | (2–4) | (2–4) |
| p | p = 0.5 | p = 0.88 | p = 0.49 | p = 0.83 | p = 0.06 |
| Signal distribution (1–2) | 1 | 1 | 2 | 1 | 1 |
| median (min-max) | (1–1) | (1–2) | (1–2) | (1–2) | (1–2) |
| p | p = 0.27 | p = 0.99 | p = 0.54 | p = 0.91 | |
| Cell localization (1–3) | 1 | 1.5 | 1 | 1.5 | 2 |
| median (min-max) | (1–1) | (1–3) | (1–3) | (1–3) | (1–3) |
| p | p = 0.58 | p = 0.96 | p = 0.41 | p = 0.85 | |
| IL-8 immunoreactivity score | |||||
| Intensity of positivity (0–4) | 2 | 3 | 3 | 3 | 3 |
| median (min-max) | (1–3) | (3–4) | (2–4) | (2-4) | (2-4) |
| p | p = 0.07 | p = 0.65 | p = 0.87 | p = 0.35 | p = 0.34 |
| Signal distribution (1–2) | 2 | 1 | 2 | 1 | 1 |
| median (min-max) | (1–2) | (1–2) | (1–2) | (1–2) | (1–2) |
| p | p = 0.5 | p = 0.56 | p = 0.63 | p = 0.48 | p = 0.41 |
| Control | EA-Affected | EA-Affected | EA-Affected | EA-Affected | |
|---|---|---|---|---|---|
| T0 | T1 | T2 | T3 | ||
| Histological score (0–10) | 3 | 5.5 | 5 | 6.5 | 7.5 |
| median (min-max) | (2–4) A | (4–6) B | (4–8) B | (5–10) B | (5–9) B |
| NKA immunoreactivity score | |||||
| Intensity of positivity (0–4) | 2 | 3 | 3 | 3 | 4 |
| median (min-max) | (2–3) a | (1–4) | (2–4) | (2–4) b | (2–4) b |
| Signal distribution (1–2) | 1 | 1 | 2 | 1 | 1 |
| median (min-max) | (1–1) | (1–2) | (1–2) | (1–2) | (1–2) |
| Cell localization (1–3) | 1 | 1.5 | 1 | 1.5 | 2 |
| median (min-max) | (1–1) | (1–3) | (1–3) | (1–3) | (1–3) |
| IL-8 immunoreactivity score | |||||
| Intensity of positivity (0–4) | 2 | 3 | 3 | 3 | 3 |
| median (min-max) | (1–3) | (3–4) | (2–4) | (2–4) | (2–4) |
| Signal distribution (1–2) | 2 | 1 | 2 | 1 | 1 |
| median (min-max) | (1–2) | (1–2) | (1–2) | (1–2) | (1–2) |
| EA-Affected | EA-Affected | EA-Affected | EA-Affected | |
|---|---|---|---|---|
| T0 | T1 | T2 | T3 | |
| Histological score (0–10) | 5.5 | 5 | 6.5 | 7.5 |
| median (min-max) | (4–6) a | (4–8) | (5–10) | (5–9) b |
| NKA immunoreactivity score | ||||
| Intensity of positivity (0–4) | 3 | 3 | 3 | 4 |
| median (min-max) | (1–4) | (2–4) | (2–4) | (2–4) |
| Signal distribution (1–2) | 1 | 2 | 1 | 1 |
| median (min-max) | (1–2) | (1–2) | (1–2) | (1–2) |
| Cell localization (1–3) | 1.5 | 1 | 1.5 | 2 |
| median (min-max) | (1–3) | (1–3) | (1–3) | (1–3) |
| IL-8 immunoreactivity score | ||||
| Intensity of positivity (0–4) | 3 | 3 | 3 | 3 |
| median (min-max) | (3–4) | (2–4) | (2–4) | (2–4) |
| Signal distribution (1–2) | 1 | 2 | 1 | 1 |
| median (min-max) | (1–2) | (1–2) | (1–2) | (1–2) |
| NKA | EA-Case 1 | EA-Case 2 | EA-Case 3 | EA-Case 4 | EA-Case 5 | EA-Case 6 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B Right | B Left | B Right | B Left | B Right | B Left | B Right | B Left | B Right | B Left | B Right | B Left | |||||||||||||
| P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | |
| T0 | n.e. | n.e. | n.e. | n.e. | 2, N, diffuse | 2, C, diffuse | 3, N, diffuse | 2, C, diffuse | n.e. | n.e. | n.e. | n.e. | 2, C, diffuse | 3, CN, diffuse | n.e. | 2, N, diffuse | 3, C, focal | n.e. | n.e. | 3, CN, diffuse | 1, C, focal | n.e. | 1, C, diffuse | n.e. |
| T1 | n.e. | 2, C, diffuse | n.e. | 2, C, diffuse | 1, C, diffuse | 3, N, diffuse | 2, C, diffuse | 3, CN, diffuse | 2, CN, diffuse | 3, CN, diffuse | 2, CN, diffuse | 3, CN, diffuse | 1, C, focal | 1, C, focal | 1, C, focal | 1, C, focal | n.e. | 3, C, focal | 3, C, focal | 3, C, focal | 1, CN, focal | 2, CN, focal | 3, CN, focal | 2, C, focal |
| T2 | n.e. | 2, C, diffuse | n.e. | 3, CN, diffuse | 2, C, diffuse | 2, C, diffuse | 2, C, diffuse | 1, C, diffuse | 2, C, diffuse | 3, CN, diffuse | 2, C, diffuse | 3, CN, diffuse | 1, C, focal | 2, CN, diffuse | 2, C, diffuse | 3, CN, diffuse | 2, CN, focal | 3, CN, diffuse | 2, C, focal | 3, N, focal | 2, CN, focal | 1, CN, focal | 1, C, focal | 1, C, focal |
| T3 | 3, N, diffuse | 3, N, diffuse | 3, N, diffuse | 2, N, diffuse | n.e. | 3, CN, diffuse | 3, CN, diffuse | 1, C, diffuse | 3, CN, diffuse | 3, CN, diffuse | 3, C, diffuse | 3, C, diffuse | 3, CN, focal | n.e. | 3, CN, diffuse | 3, CN, diffuse | 3, CN, diffuse | 3, CN, focal | 3, N, focal | 2, CN, focal | 1, C, focal | n.e. | n.e. | 1, C, focal |
| IL-8 | EA-Case 1 | EA-Case 2 | EA-Case 3 | EA- Case 4 | EA- Case 5 | EA- Case 6 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B Right | B Left | B Right | B Left | B Right | B Left | B Right | B Left | B Right | B Left | B Right | B Left | |||||||||||||
| P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | P | D | |
| T0 | 3, focal | n.e. | 3, focal | n.e. | 3, diffuse | 4, diffuse | 4, diffuse | 2, diffuse | n.e. | n.e. | n.e. | n.e. | 3, focal | 4, diffuse | n.e. | 3, diffuse | 4, diffuse | 3, focal | n.e. | 3, diffuse | n.e. | n.e. | n.e. | n.e. |
| T1 | n.e. | 2, focal | n.e. | 3, focal | 3, diffuse | 3, focal | 3, focal | 4, diffuse | n.e. | 3, diffuse | 4, diffuse | 3, focal | 2, focal | 3, focal | 2, focal | 3, focal | 4, diffuse | 4, diffuse | 4, diffuse | 4, diffuse | 4, diffuse | 4, focal | 3, focal | 4, diffuse |
| T2 | n.e. | 4, diffuse | 3, diffuse | 3, focal | 3, diffuse | 3, diffuse | 3, focal | 4, diffuse | 2, focal | 2, diffuse | 2, focal | 2, diffuse | 2, focal | 3, diffuse | 3, diffuse | 3, focal | 3, diffuse | 3, diffuse | 4, focal | 2, diff | 2, focal | 4, focal | 3, diffuse | 2, focal |
| T3 | 4, diffuse | 4, diffuse | 3, diffuse | 3, focal | n.e. | n.e. | 4, diffuse | 4, diffuse | 3, diffuse | 4, diffuse | 3, diffuse | 4, diffuse | 4, diffuse | n.e. | 3, diffuse | 3, diffuse | 4, diffuse | 4, focal | 4, focal | n.e. | n.e. | 3, focal | 2, focal | 2, focal |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morini, M.; Peli, A.; Rinnovati, R.; Magazzù, G.; Romagnoli, N.; Spadari, A.; Pietra, M. Immunohistochemical Expression of Neurokinin-A and Interleukin-8 in the Bronchial Epithelium of Horses with Severe Equine Asthma Syndrome during Asymptomatic, Exacerbation, and Remission Phase. Animals 2021, 11, 1376. https://doi.org/10.3390/ani11051376
Morini M, Peli A, Rinnovati R, Magazzù G, Romagnoli N, Spadari A, Pietra M. Immunohistochemical Expression of Neurokinin-A and Interleukin-8 in the Bronchial Epithelium of Horses with Severe Equine Asthma Syndrome during Asymptomatic, Exacerbation, and Remission Phase. Animals. 2021; 11(5):1376. https://doi.org/10.3390/ani11051376
Chicago/Turabian StyleMorini, Maria, Angelo Peli, Riccardo Rinnovati, Giuseppe Magazzù, Noemi Romagnoli, Alessandro Spadari, and Marco Pietra. 2021. "Immunohistochemical Expression of Neurokinin-A and Interleukin-8 in the Bronchial Epithelium of Horses with Severe Equine Asthma Syndrome during Asymptomatic, Exacerbation, and Remission Phase" Animals 11, no. 5: 1376. https://doi.org/10.3390/ani11051376
APA StyleMorini, M., Peli, A., Rinnovati, R., Magazzù, G., Romagnoli, N., Spadari, A., & Pietra, M. (2021). Immunohistochemical Expression of Neurokinin-A and Interleukin-8 in the Bronchial Epithelium of Horses with Severe Equine Asthma Syndrome during Asymptomatic, Exacerbation, and Remission Phase. Animals, 11(5), 1376. https://doi.org/10.3390/ani11051376