
Canine Epithelial Thymic Tumors: Outcome in 28 Dogs Treated by Surgery



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Signalment and Clinical Findings
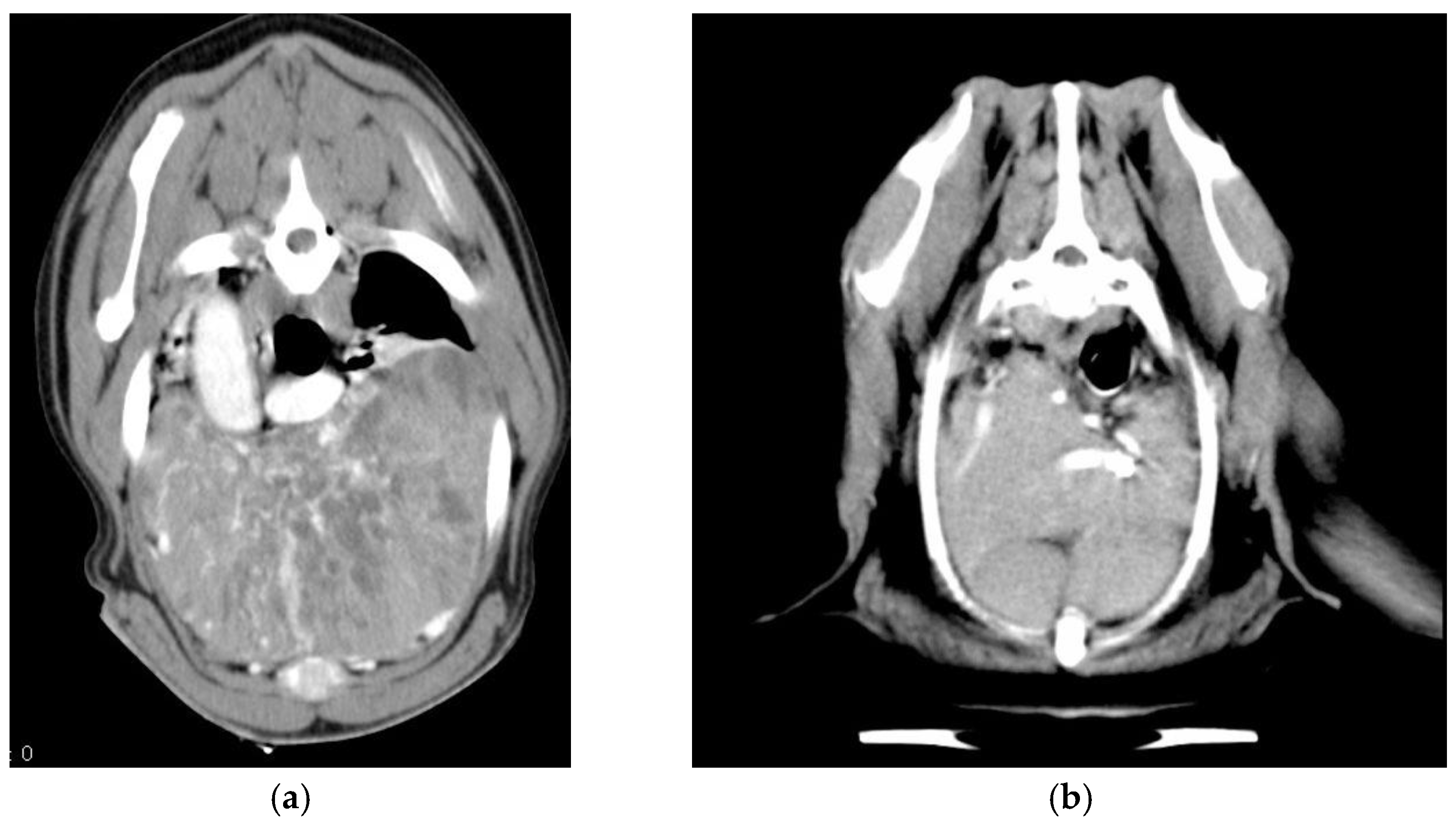
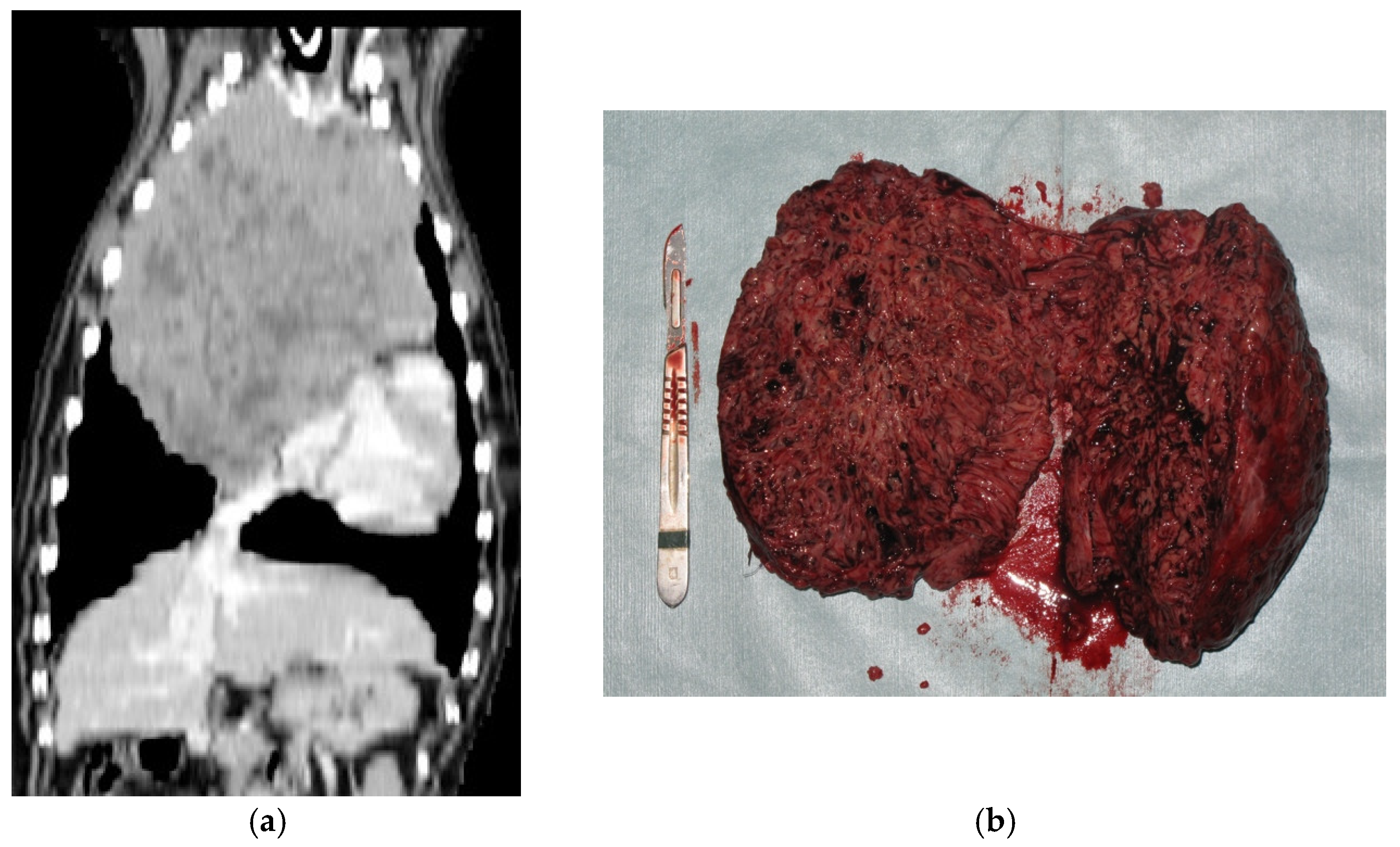
- Diagnostics: contrast-enhanced CT of the thorax without an angiogram was performed and available in 18 dogs; in older cases, medical records only reported three-view thoracic radiographs and thoracic ultrasounds for guidance in FNA of the mediastinal mass.
- Paraneoplastic syndromes: MG was diagnosed in two dogs (7.1%) before tumor removal and in three dogs (10.7%) after tumor excision, one of which was in the form of the focal megaesophagus; MG was confirmed by AchR antibody titers in four dogs and was presumed on the basis of the Tensilon test in one dog. The syndrome was resolved after surgery in one case and persisted in the other one. Pyridostigmine was administered to the animals in the generalized form. Hypercalcemia was diagnosed in two dogs (7.1%), both of which were affected by a thymic carcinoma, and one of which developed postoperative hypocalcemia that was resolved with symptomatic treatment after 15 days of hospitalization. The other dog presented with a large mediastinal mass and clinical signs of hypercalcemia, which was treated medically by the referring veterinarian with furosemide for 3 months before surgery was accepted by the owners. The syndrome was resolved after surgery, and it recurred at the time of tumor recurrence. Parathyroid hormone-related peptide (PTH-rp) was not evaluated in either animal.One dog was first seen for severe immune-mediated anemia that was treated by immunosuppressive doses of prednisone and cyclophosphamide and did not recur after extirpation of the tumor. The final diagnosis was thymoma, but the tumor recurred after 366 days and the dog was lost to follow up at that time.
- Five dogs (17.8%) had a concurrent tumor or developed one in the course of their life: one brochioloalveolar carcinoma, one lung squamous cell carcinoma, one squamous cell carcinoma of the digit, one cutaneous hemangiosarcoma, and one solid carcinoma of the frontal sinus. Brochioloalveolar carcinoma was the cause of death in one dog.
3.2. Therapy
- Neoadjuvant and adjuvant treatments: chemotherapy was administered to seven dogs (25%), five postoperatively and two before surgery. The dog affected by immune-mediated anemia received cyclophosphamide (200 mg/m2/week) and prednisone (starting from 2 mg/kg/day for 1 week, tapering the dose in the following weeks) before surgery, which partially resolved the anemia. The other dog had an erroneous first diagnosis of lymphoma; therefore, a COP protocol (cyclophosphamide, vincristine, and prednisone) was started by the referring veterinarian, without success.The dog with hypercalcemia and thymic carcinoma received carboplatin (300 mg/m2) at the time of tumor recurrence, 60 days after surgery. A partial response was achieved, and the hypercalcemia was resolved. He is currently under treatment at the time of writing, but a complete response was not achieved, and the owners refused RT.
3.3. Histopathology Reports
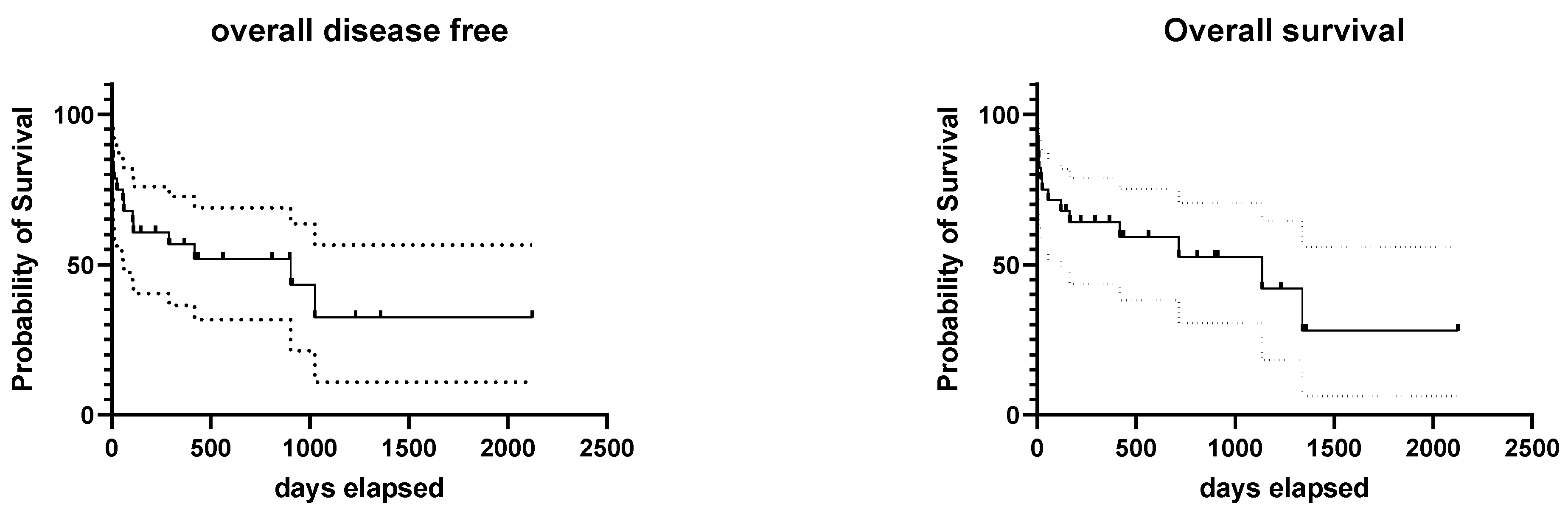
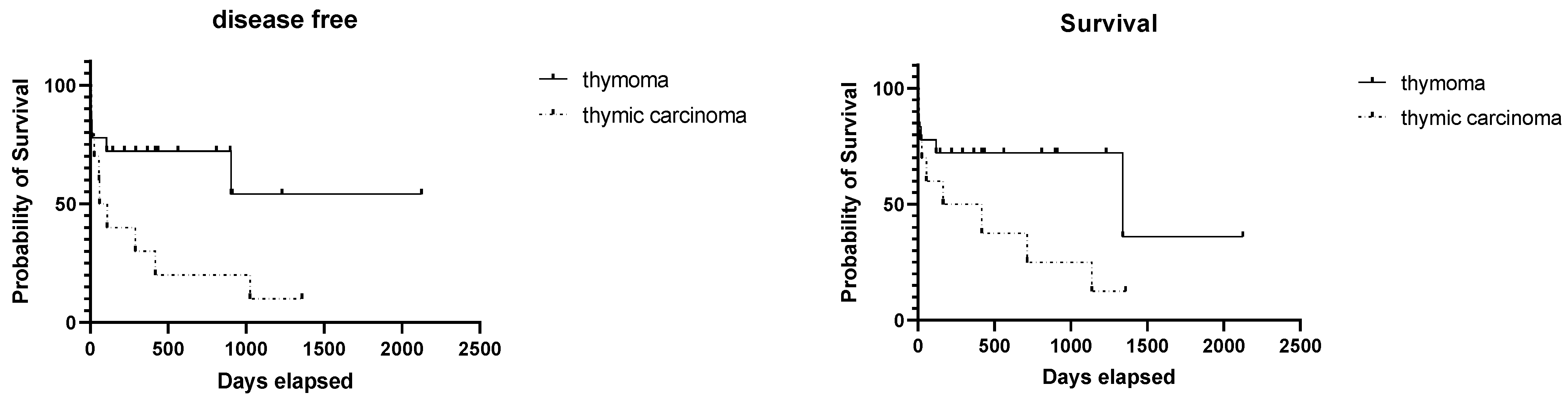
3.4. Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- de Mello Souza, C.H. Section B: Thymoma. In Withrow and McEwen’s Small Animal Clinical Oncology; Elsevier: Maryland Heights, MO, USA, 2020; pp. 778–781. ISBN 978-0-323-59496-7. [Google Scholar]
- Day, M.J. Review of Thymic Pathology in 30 Cats and 36 Dogs. J. Small Anim. Pract. 1997, 38, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Bernard, C.; Frih, H.; Pasquet, F.; Kerever, S.; Jamilloux, Y.; Tronc, F.; Guibert, B.; Isaac, S.; Devouassoux, M.; Chalabreysse, L.; et al. Thymoma Associated with Autoimmune Diseases: 85 Cases and Literature Review. Autoimmun. Rev. 2016, 15, 82–92. [Google Scholar] [CrossRef]
- Scorsetti, M.; Leo, F.; Trama, A.; D’Angelillo, R.; Serpico, D.; Macerelli, M.; Zucali, P.; Gatta, G.; Garassino, M.C. Thymoma and Thymic Carcinomas. Crit. Rev. Oncol. Hematol. 2016, 99, 332–350. [Google Scholar] [CrossRef]
- Lana, S.; Plaza, S.; Hampe, K.; Burnett, R.; Avery, A.C. Diagnosis of Mediastinal Masses in Dogs by Flow Cytometry. J. Vet. Intern. Med. 2006, 20, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- Pintore, L.; Bertazzolo, W.; Bonfanti, U.; Gelain, M.E.; Bottero, E. Cytological and Histological Correlation in Diagnosing Feline and Canine Mediastinal Masses. J. Small Anim. Pract. 2014, 55, 28–32. [Google Scholar] [CrossRef]
- Von Stade, L.; Randall, E.K.; Rao, S.; Marolf, A.J. CT Imaging Features of Canine Thymomas. Vet. Radiol. Ultrasound 2019, 60, 659–667. [Google Scholar] [CrossRef] [Green Version]
- Robat, C.S.; Cesario, L.; Gaeta, R.; Miller, M.; Schrempp, D.; Chun, R. Clinical Features, Treatment Options, and Outcome in Dogs with Thymoma: 116 Cases (1999–2010). J. Am. Vet. Med. Assoc. 2013, 243, 1448–1454. [Google Scholar] [CrossRef]
- Yale, A.D.; Priestnall, S.L.; Pittaway, R.; Taylor, A.J. Thymic Epithelial Tumours in 51 Dogs: Histopathologic and Clinicopathologic Findings. Vet. Comp. Oncol. 2021, vco.12705. [Google Scholar] [CrossRef] [PubMed]
- Garneau, M.S.; Price, L.L.; Withrow, S.J.; Boston, S.E.; Ewing, P.J.; McClaran, J.K.; Liptak, J.M.; Berg, J. Perioperative Mortality and Long-Term Survival in 80 Dogs and 32 Cats Undergoing Excision of Thymic Epithelial Tumors: Thymic Epithelial Tumor Survival. Vet. Surg. 2015, 44, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Zitz, J.C.; Birchard, S.J.; Couto, G.C.; Samii, V.F.; Weisbrode, S.E.; Young, G.S. Results of Excision of Thymoma in Cats and Dogs: 20 Cases (1984–2005). J. Am. Vet. Med. Assoc. 2008, 232, 1186–1192. [Google Scholar] [CrossRef]
- Tomaszek, S.; Wigle, D.A.; Keshavjee, S.; Fischer, S. Thymomas: Review of Current Clinical Practice. Ann. Thorac. Surg. 2009, 87, 1973–1980. [Google Scholar] [CrossRef] [Green Version]
- Burgess, K.E.; DeRegis, C.J.; Brown, F.S.; Keating, J.H. Histologic and Immunohistochemical Characterization of Thymic Epithelial Tumours in the Dog: Histologic Characterization of Canine Thymomas. Vet. Comp. Oncol. 2016, 14, 113–121. [Google Scholar] [CrossRef]
- Masaoka, A.; Monden, Y. Follow-up Study of Thymomas with Special Reference to Their Clinical Stages. Cancer 1981, 48, 2485–2492. [Google Scholar] [CrossRef]
- Marx, A.; Ströbel, P.; Badve, S.S.; Chalabreysse, L.; Chan, J.K.C.; Chen, G.; de Leval, L.; Detterbeck, F.; Girard, N.; Huang, J.; et al. ITMIG Consensus Statement on the Use of the WHO Histological Classification of Thymoma and Thymic Carcinoma: Refined Definitions, Histological Criteria, and Reporting. J. Thorac. Oncol. 2014, 9, 596–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brückner, M.; Henrich, M. Giant Thymoma with Benign Central Cystic Lesions in a 1-Year-Old Pug. J. Am. Anim. Hosp. Assoc. 2019, 55, e556-01. [Google Scholar] [CrossRef]
- Reeve, E.J.; Mapletoft, E.K.; Schiborra, F.; Maddox, T.W.; Lamb, C.R.; Warren-Smith, C.M.R. Mediastinal Lymphoma in Dogs Is Homogeneous Compared to Thymic Epithelial Neoplasia and Is More Likely to Envelop the Cranial Vena Cava in CT Images. Vet. Radiol. Ultrasound 2020, 61, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Liptak, J.M.; Kamstock, D.A.; Dernell, W.S.; Ehrhart, E.J.; Rizzo, S.A.; Withrow, S.J. Cranial Mediastinal Carcinomas in Nine Dogs. Vet. Comp. Oncol. 2008, 6, 19–30. [Google Scholar] [CrossRef]
- Morini, M.; Bettini, G.; Diana, A.; Spadari, A.; Casadio Tozzi, A.; Santi, M.; Romagnoli, N.; Scarpa, F.; Mandrioli, L. Thymofibrolipoma in Two Dogs. J. Comp. Pathol. 2009, 141, 74–77. [Google Scholar] [CrossRef]
- Ramírez, G.A.; Spattini, G.; Altimira, J.; García, B.; Vilafranca, M. Clinical and Histopathological Features of a Thymolipoma in a Dog. J. Vet. Diagn. Investig. 2008, 20, 360–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobias, J.R.; Cullen, J.M. Thymofibrolipoma in a Labrador Retriever. Vet. Pathol. 2014, 51, 816–819. [Google Scholar] [CrossRef] [Green Version]
- Reichle, J.K.; Wisner, E.R. Non-Cardiac Thoracic Ultrasound in 75 Feline and Canine Paitents. Vet. Radiol. Ultrasound 2000, 41, 154–162. [Google Scholar] [CrossRef] [PubMed]
- Patterson, M.M.E.; Marolf, A.J. Sonographic Characteristics of Thymoma Compared with Mediastinal Lymphoma. J. Am. Anim. Hosp. Assoc. 2014, 50, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, W.; Kyles, A.; Samii, V.; Hardie, E.; Kass, P.; Gregory, C. Computed Tomographic Assessment of Vascular Invasion and Resectability of Mediastinal Masses in Dogs and a Cat. N. Z. Vet. J. 2008, 56, 330–333. [Google Scholar] [CrossRef] [PubMed]
- Rick, T.; Kleiter, M.; Schwendenwein, I.; Ludewig, E.; Reifinger, M.; Hittmair, K.M. Contrast-Enhanced Ultrasonography Characteristics of Intrathoracic Mass Lesions in 36 Dogs and 24 Cats. Vet. Radiol. Ultrasound 2019, 60, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Burton, A.G.; Borjesson, D.L.; Vernau, W. Thymoma-Associated Lymphocytosis in a Dog. Vet. Clin. Pathol. 2014, 43, 584–588. [Google Scholar] [CrossRef]
- Wikander, Y.M.; Knights, K.; Coffee, C.; Vernau, W.; Biller, D.S.; Higginbotham, M.L.; Springer, N.L. CD4 and CD8 Double-Negative Immunophenotype of Thymoma-Associated Lymphocytes in a Dog. J. Vet. Diagn. Investig. 2020, 32, 918–922. [Google Scholar] [CrossRef]
- Suster, S.; Moran, C.A. Thymoma, Atypical Thymoma, and Thymic Carcinoma: A Novel Conceptual Approach to the Classification of Thymic Epithelial Neoplasms. Am. J. Clin. Pathol. 1999, 111, 826–833. [Google Scholar] [CrossRef]
- Bergman, P.J. Paraneoplastic Hypercalcemia. Top. Companion Anim. Med. 2012, 27, 156–158. [Google Scholar] [CrossRef]
- Foley, P.; Shaw, D.; Runyon, C.; McConkey, S.; Ikede, B. Serum Parathyroid Hormone-Related Protein Concentration in a Dog with a Thymoma and Persistent Hypercalcemia. Can. Vet. J. 2000, 41, 867–870. [Google Scholar]
- Batlivala, T.P.; Bacon, N.J.; Avery, A.C.; Barabas, K.; Gunn-Christie, R.G.; Conway, J.; Avery, P.R. Paraneoplastic T Cell Lymphocytosis Associated with a Thymoma in a Dog. J. Small Anim. Pract. 2010, 51, 491–494. [Google Scholar] [CrossRef] [PubMed]
- Tepper, L.C.; Spiegel, I.B.; Davis, G.J. Diagnosis of Erythema Multiforme Associated with Thymoma in a Dog and Treated with Thymectomy. J. Am. Anim. Hosp. Assoc. 2011, 47, e19–e25. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Wright, J.; WR, B., Jr.; LaRue, S.; Fineman, L.; Hogge, G.; Kitchell, B.; Hohenhaus, A.; Burk, R.; Dhaliwal, R.; et al. Radiation Therapy in the Treatment of Canine and Feline Thymomas: A Retrospective Study (1985–1999). J. Am. Anim. Hosp. Assoc. 2001, 37, 489–496. [Google Scholar] [CrossRef]
- Mignan, T.; Targett, M.; Lowrie, M. Classification of Myasthenia Gravis and Congenital Myasthenic Syndromes in Dogs and Cats. J. Vet. Intern. Med. 2020, 34, 1707–1717. [Google Scholar] [CrossRef]
- MacIver, M.A.; Case, J.B.; Monnet, E.L.; Hunt, G.B.; Mayhew, P.D.; Oblak, M.L.; Runge, J.J.; Singh, A.; Smeak, D.D.; Steffey, M.A.; et al. Video-Assisted Extirpation of Cranial Mediastinal Masses in Dogs: 18 Cases (2009–2014). J. Am. Vet. Med. Assoc. 2017, 250, 1283–1290. [Google Scholar] [CrossRef]
- Wiles, V.; Haddad, J.; Leibman, N.; Avery, A.C.; Hughes, K.L. Metastatic Thymoma in the Liver of a Dog. J. Vet. Diagn. Investig. 2018, 30, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Rohrer Bley, C.; Meier, V.; Schneider, U. Dosimetric Benefit of Adaptive Radiotherapy in the Neoadjuvant Management of Canine and Feline Thymoma-An Exploratory Case Series. Vet. Comp. Oncol. 2018, 16, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Goto, S.; Murakami, M.; Kawabe, M.; Iwasaki, R.; Heishima, K.; Sakai, H.; Mori, T. Hypofractionated Radiation Therapy in the Treatment of Canine Thymoma: Retrospective Study of Eight Cases. Vet. Radiol. Ultrasound 2017, 58, 613–620. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Yamazaki, H.; Tanaka, M.; Kaneguchi, A.; Tanaka, T.; Akiyoshi, H.; Noguchi, S. Radiotherapy-Induced Tumor Lysis Syndrome in a Dog with Thymoma. J. Vet. Med. Sci. 2021, 83, 1290–1294. [Google Scholar] [CrossRef]
- Berghmans, T.; Durieux, V.; Holbrechts, S.; Jungels, C.; Lafitte, J.-J.; Meert, A.-P.; Moretti, L.; Ocak, S.; Roelandts, M.; Girard, N. Systemic Treatments for Thymoma and Thymic Carcinoma: A Systematic Review. Lung Cancer 2018, 126, 25–31. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stage | Description |
|---|---|
| I | Completely encapsulated |
| II | Invades the capsule, either microscopically or macroscopically |
| III | Invades the neighboring organs, with or without great vessel involvement |
| IV | Metastatic, either locally on the thoracic mesothelium or distantly |
| Stage | N. of Cases | Median Survival (Days) | Alive | Dead from the Tumor | Lost to Follow-Up/Dead from Unrelated Causes |
|---|---|---|---|---|---|
| I | 8 | 1732 | 2 | 1 | 4 |
| II | 7 | n.r. | 1 | 3 | 3 |
| III | 10 | 291 | 2 | 8 | 0 |
| IV | 0 | - | - | - | - |
| Case # | Breed | CT | Paraneoplastic HC 1/MG 2 | Masaoka Stage | Histotype | Recurrence (R) Metastasis (M) | DF 3 (Days) | OS 4 (Days) | Status |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Mix | no | n.d. 5 | Thymoma | 898 | 898 | Dead * 6 | ||
| 2 | Mix | no | III | Invasive thymoma | 0 | 0 | Dead | ||
| 3 | Mix | no | I | Thymoma | R | 366 | 366 | LFU | |
| 4 | Rottweiler | yes | n.d. | Thymoma | 8 | 8 | Dead | ||
| 5 | Mix | no | II | Thymoma | R | 105 | 120 | Dead | |
| 6 | Rottweiler | no | I | Thymoma | 912 | 912 | Dead * | ||
| 7 | Labrador retriever | no | MG | I | Thymoma | R | 903 | 1340 | Dead |
| 8 | Alsatian (German shepherd) | no | III | Thymoma | M | 12 | 20 | Dead | |
| 9 | Fox terrier | no | I | Thymoma | 562 | 562 | LFU | ||
| 10 | Mix | Yes | HC | II | Thymic k 7 | 1358 | 1358 | LFU | |
| 11 | Mix | Yes | III | Thymic k | R | 417 | 417 | Dead | |
| 12 | Shi-tzu | No | III | Thymoma | 0 | 0 | Dead | ||
| 13 | Mix | Yes | II | Thymic k | 7 | 7 | Dead | ||
| 14 | Mix | Yes | I | Thymoma | 1231 | 1231 | LFU | ||
| 15 | Mix | Yes | MG | n.d. | Thymic k | 56 | 56 | Dead | |
| 16 | Akita Inu | Yes | I | Thymoma | 2124 | 2124 | Dead * | ||
| 17 | Beagle | Yes | MG | III | Thymic k | R | 1025 | 1137 | Dead |
| 18 | Labrador retriever | Yes | III | Thymic k | R/M | 289 | 714 | Dead | |
| 19 | Golden retriever | Yes | II | Thymoma | 435 | 435 | LFU | ||
| 20 | Mix | Yes | II | Thymic k | 25 | 25 | Dead | ||
| 21 | Fox terrier | Yes | II | Thymoma | 809 | 809 | Alive | ||
| 22 | Lagotto | Yes | I | Thymoma | 417 | 417 | Alive | ||
| 23 | American Staffordshire terrier | No | MG | II | Atypical thymoma | 220 | 220 | LFU | |
| 24 | Yorkshire terrier | Yes | III | Thymoma | 293 | 293 | Alive | ||
| 25 | Doberman pinscher | Yes | MG | I | Thymoma | 145 | 145 | Alive | |
| 26 | Rottweiler | Yes | HC | III | Thymic k | R | 60 | 167 | Alive |
| 27 | Mix | Yes | III | Thymic k | 7 | 7 | Dead | ||
| 28 | Mix | Yes | III | Thymic k | R | 109 | 165 | Dead |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martano, M.; Buracco, P.; Morello, E.M. Canine Epithelial Thymic Tumors: Outcome in 28 Dogs Treated by Surgery. Animals 2021, 11, 3444. https://doi.org/10.3390/ani11123444
Martano M, Buracco P, Morello EM. Canine Epithelial Thymic Tumors: Outcome in 28 Dogs Treated by Surgery. Animals. 2021; 11(12):3444. https://doi.org/10.3390/ani11123444
Chicago/Turabian StyleMartano, Marina, Paolo Buracco, and Emanuela Maria Morello. 2021. "Canine Epithelial Thymic Tumors: Outcome in 28 Dogs Treated by Surgery" Animals 11, no. 12: 3444. https://doi.org/10.3390/ani11123444
APA StyleMartano, M., Buracco, P., & Morello, E. M. (2021). Canine Epithelial Thymic Tumors: Outcome in 28 Dogs Treated by Surgery. Animals, 11(12), 3444. https://doi.org/10.3390/ani11123444