Recovery of Vaginal Microbiota after Standard Treatment for Bacterial Vaginosis Infection: An Observational Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
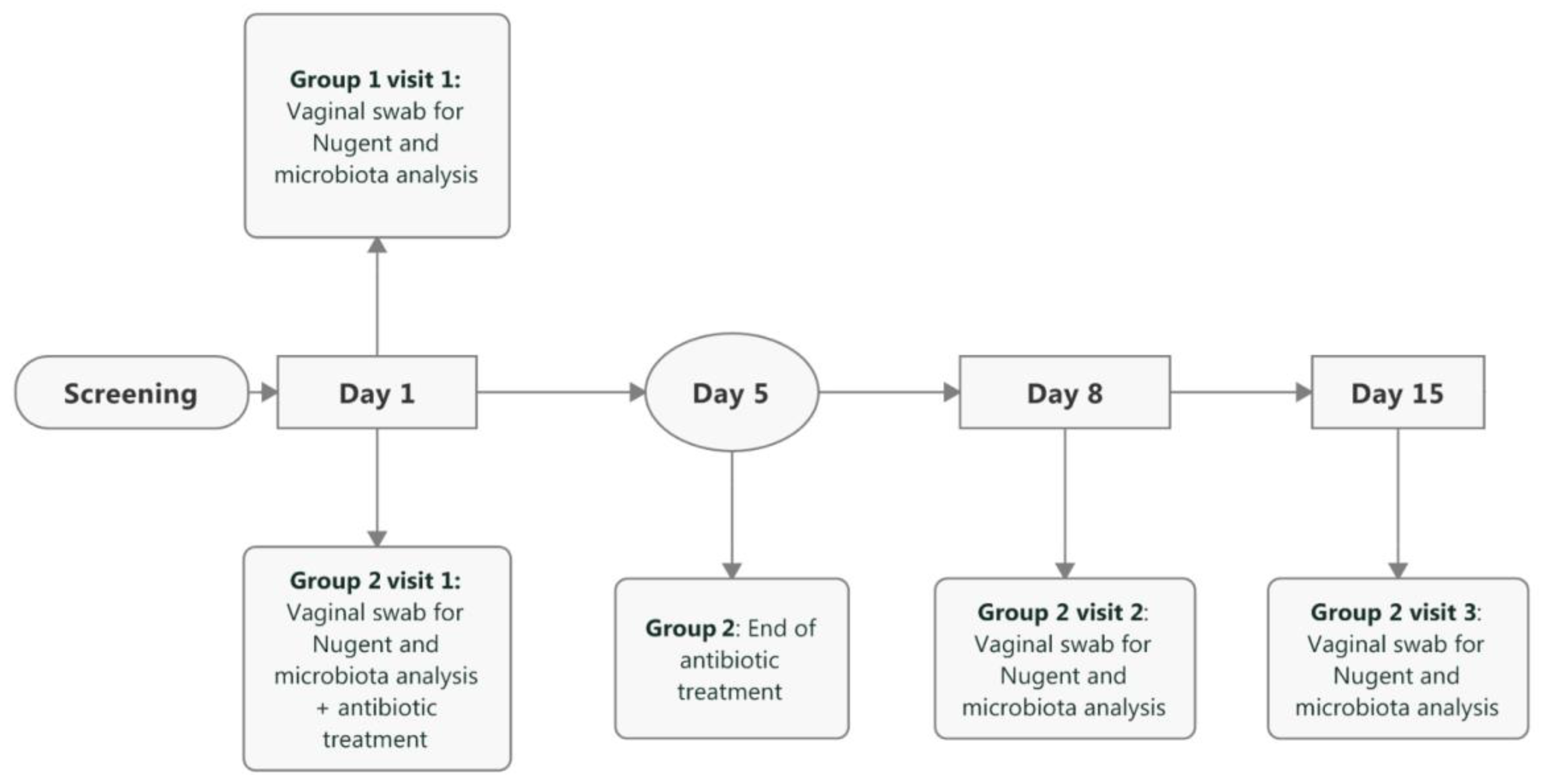
2.1. Study Design
2.2. Outcomes
2.3. Sample Collection
2.4. Nugent Score
2.5. Vaginal Microbiota Sample Processing and Analysis
2.5.1. DNA Extraction
2.5.2. Vaginal Microbiota Sequencing and Data Analysis
3. Results
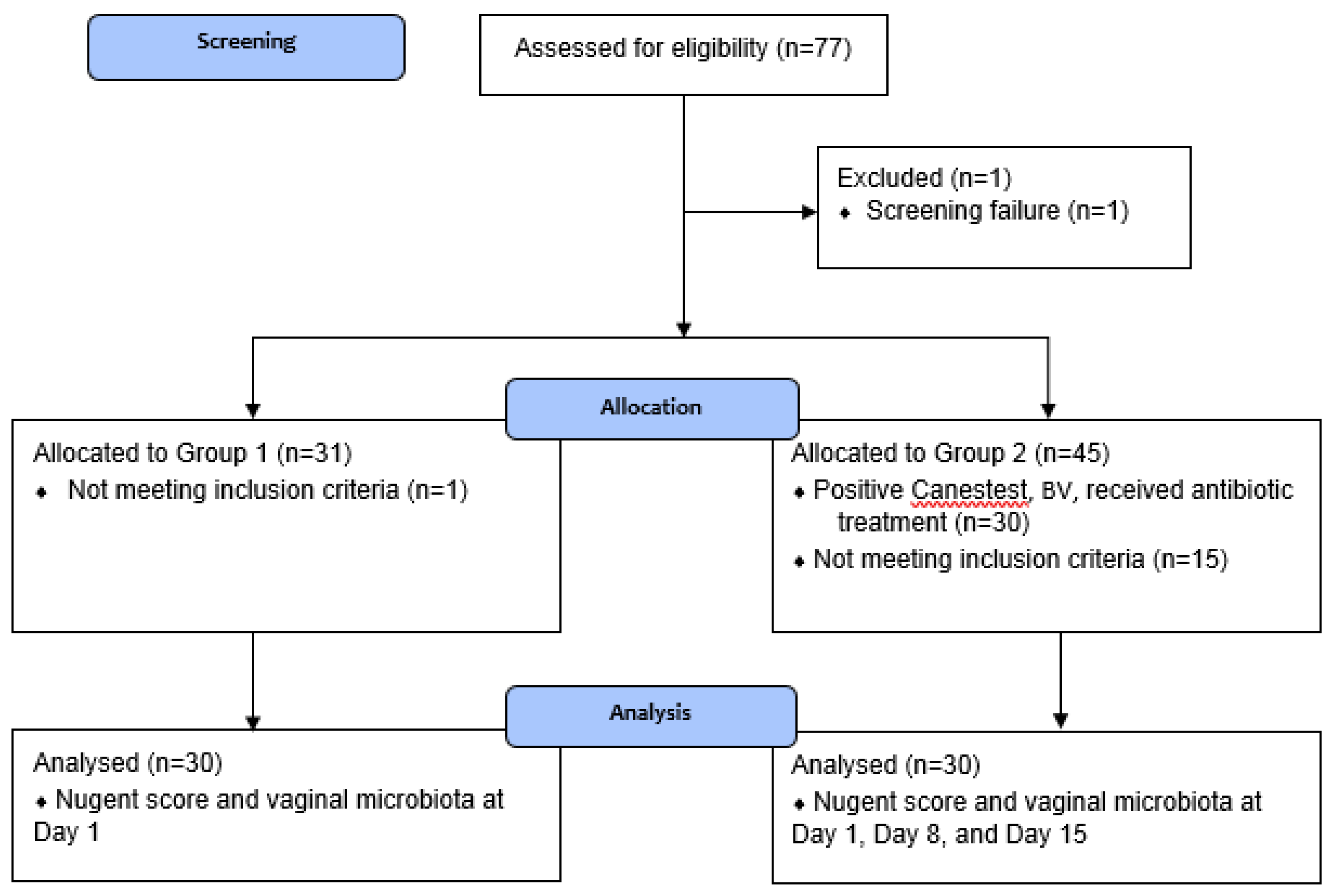
3.1. Participant Flow
3.2. Nugent Score Evaluation
3.3. Vaginal Microbiota Evaluation
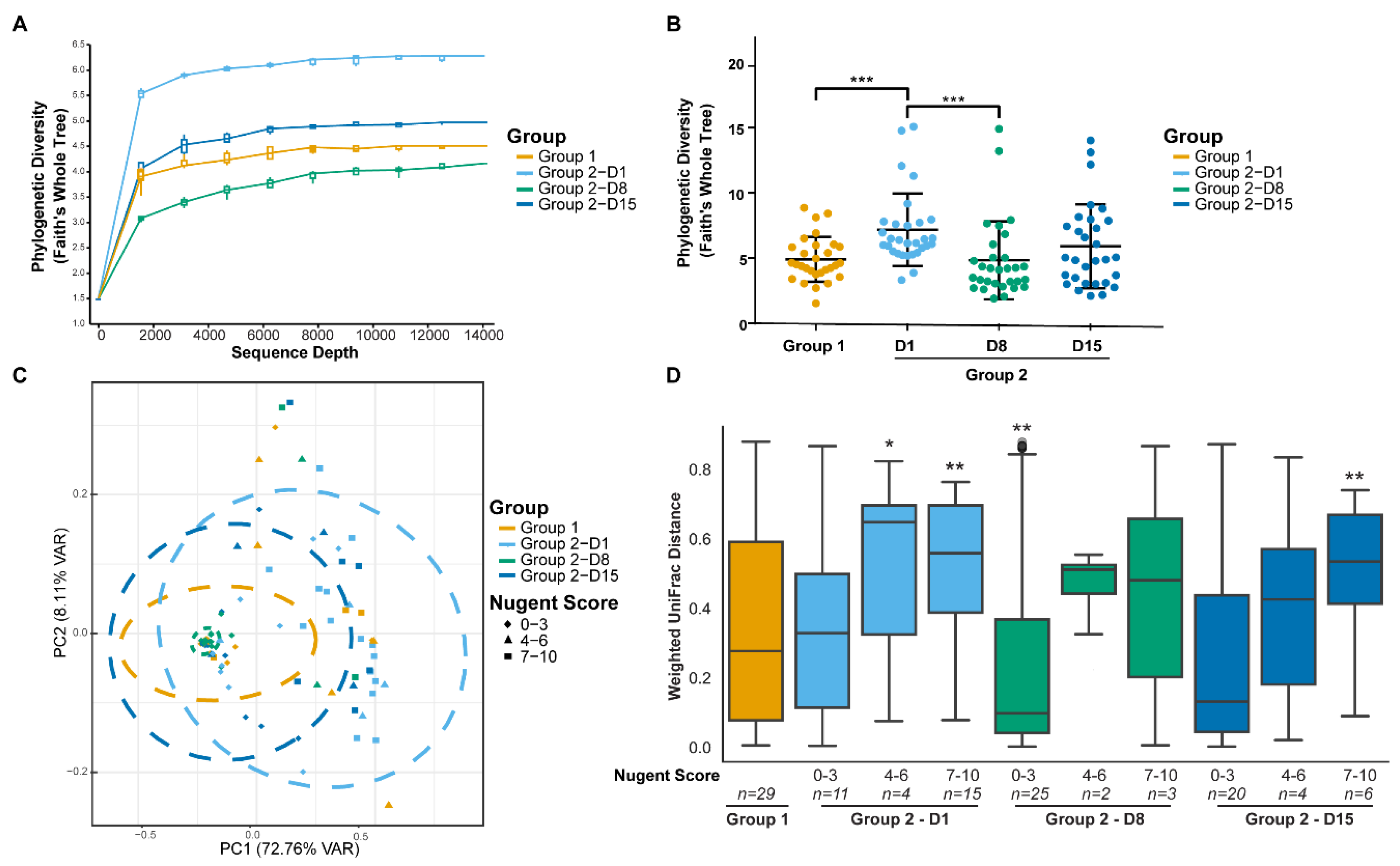
3.3.1. Diversity
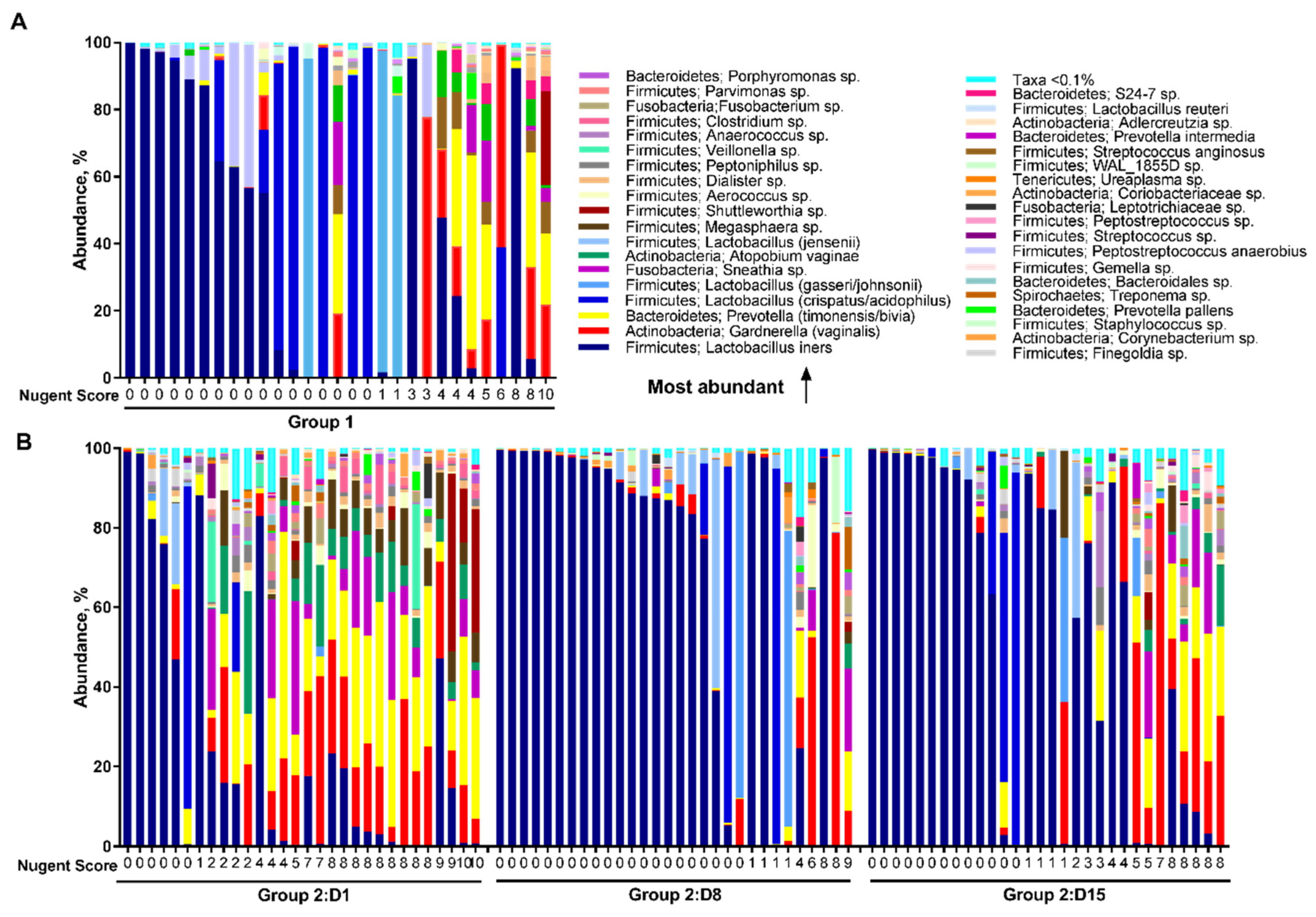
3.3.2. Relative Abundance
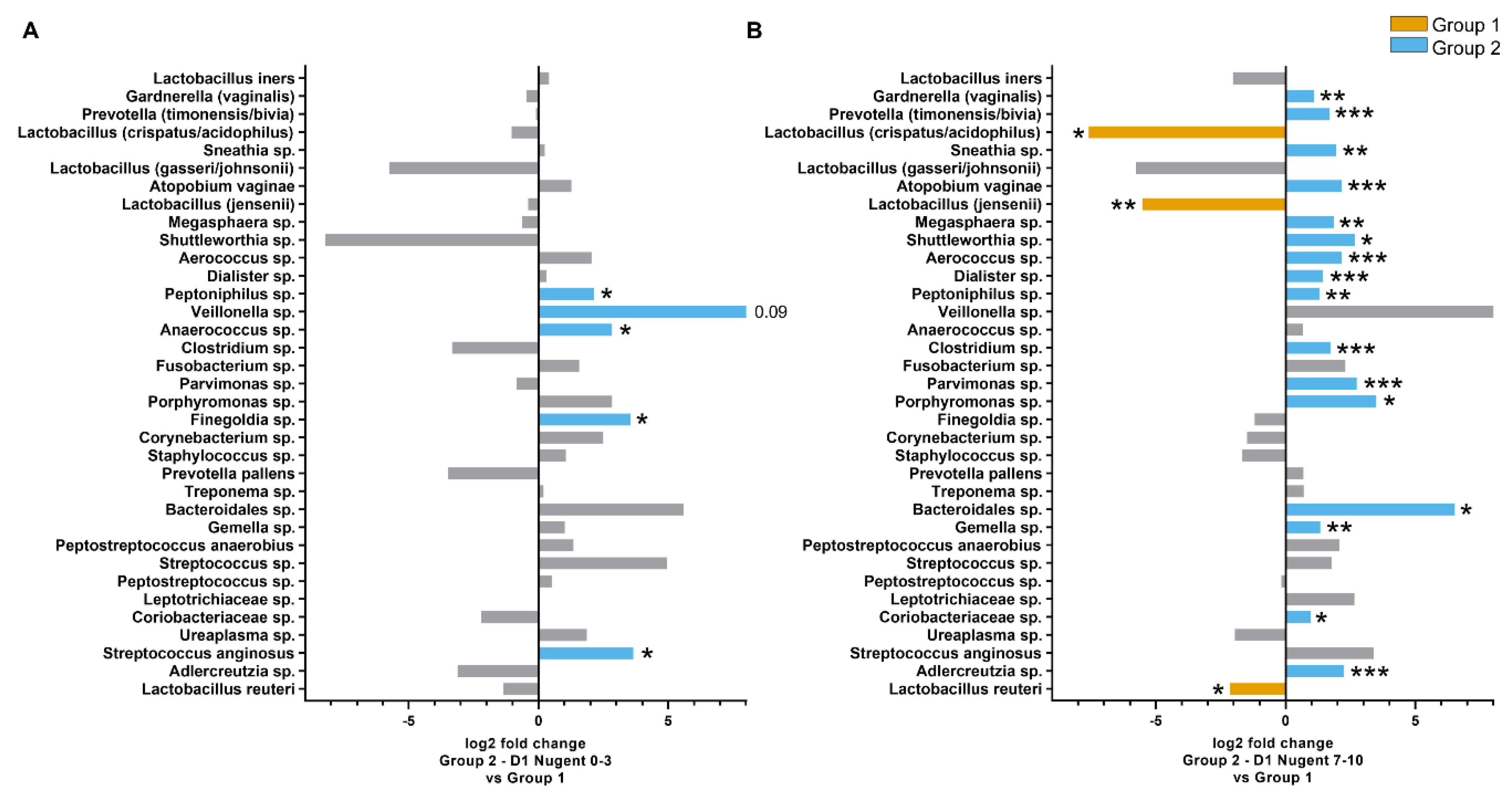
3.3.3. Nugent Score Subgroups within Group 2
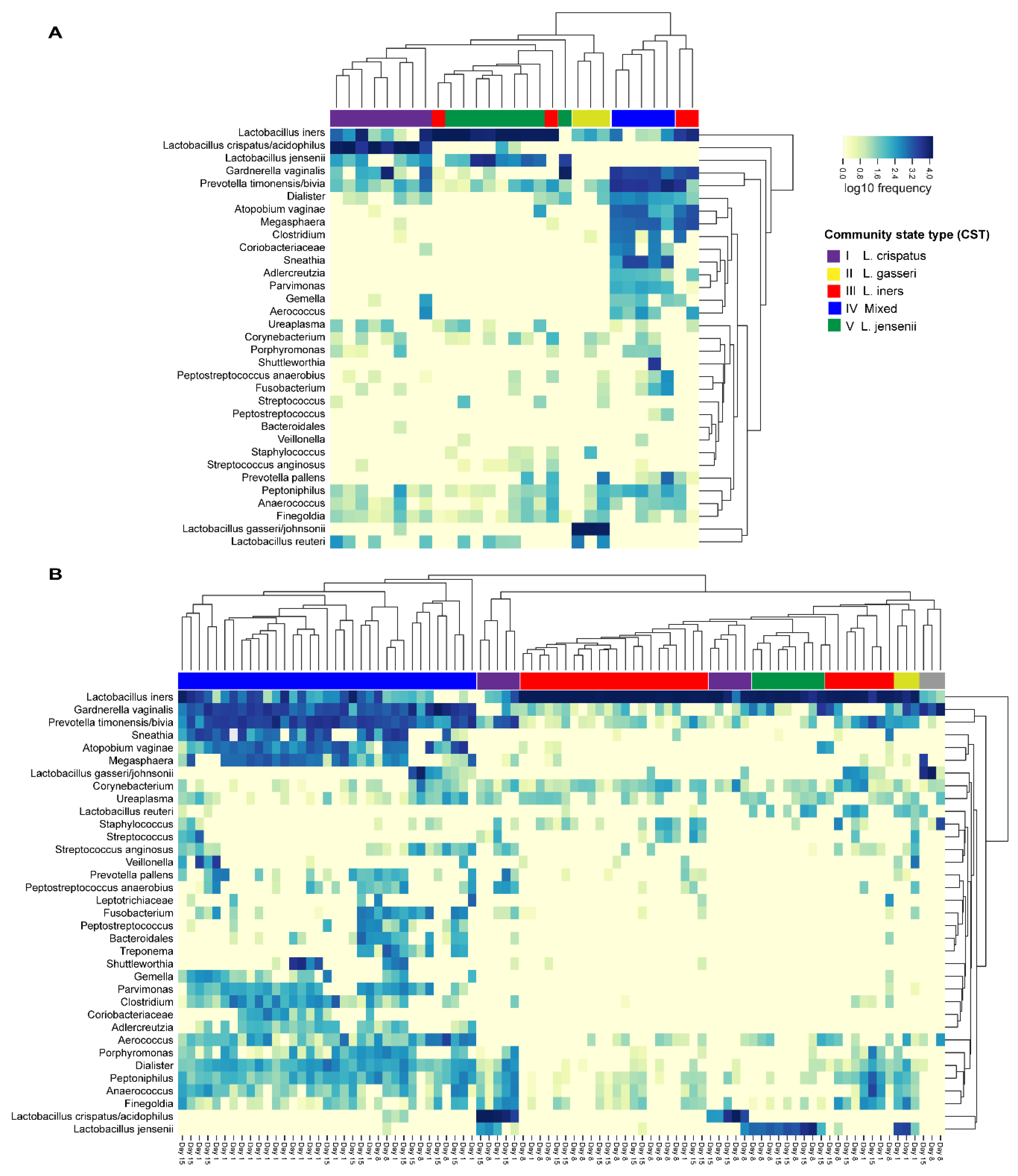
3.3.4. Community State Types
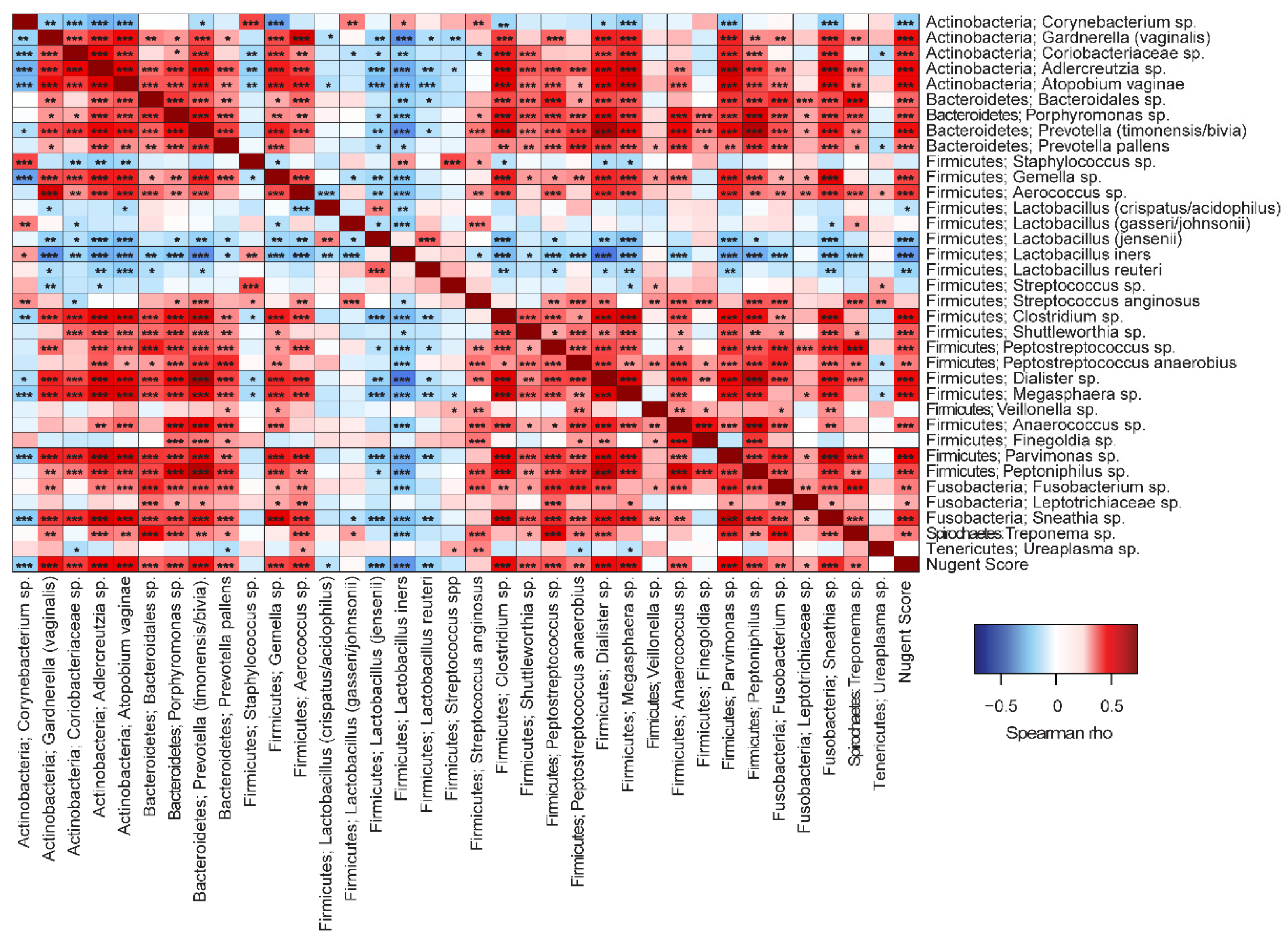
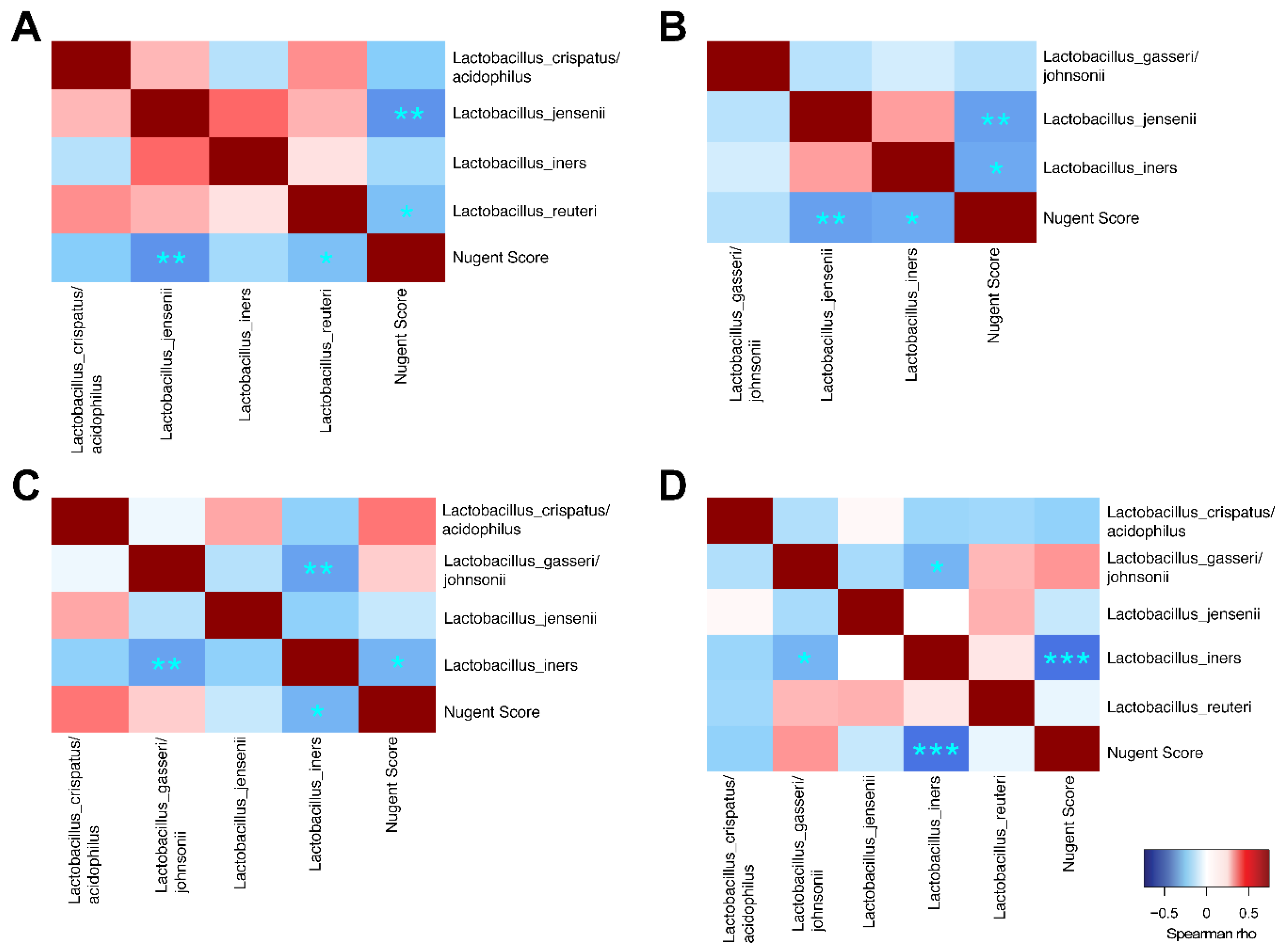
3.3.5. Correlations to Nugent Score and Taxa
3.4. Safety
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Smith, S.B.; Ravel, J. The vaginal microbiota, host defence and reproductive physiology. J. Physiol. 2017, 595, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Petrova, M.I.; Reid, G.; Vaneechoutte, M.; Lebeer, S. Lactobacillus iners: Friend or Foe? Trends Microbiol. 2017, 25, 182–191. [Google Scholar] [CrossRef] [PubMed]
- Machado, A.; Cerca, N. Influence of Biofilm Formation by Gardnerella vaginalis and Other Anaerobes on Bacterial Vaginosis. J. Infect. Dis. 2015, 212, 1856–1861. [Google Scholar] [CrossRef]
- Oduyebo, O.O.; Anorlu, R.I.; Ogunsola, F.T. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst. Rev. 2009, 8, CD006055. [Google Scholar] [CrossRef] [PubMed]
- Menard, J.-P. Antibacterial treatment of bacterial vaginosis: Current and emerging therapies. Int. J. Women’s Health 2011, 3, 295–305. [Google Scholar] [CrossRef]
- Bradshaw, C.S.; Sobel, J. Current Treatment of Bacterial Vaginosis—Limitations and Need for Innovation. J. Infect. Dis. 2016, 214 (Suppl. S1), S14–S20. [Google Scholar] [CrossRef] [PubMed]
- Lambert, J.A.; John, S.; Sobel, J.D.; Akins, R.A. Longitudinal analysis of vaginal microbiome dynamics in women with recurrent bacterial vaginosis: Recognition of the conversion process. PLoS ONE 2013, 8, e82599. [Google Scholar] [CrossRef]
- Mayer, B.T.; Srinivasan, S.; Fiedler, T.L.; Marrazzo, J.M.; Fredricks, D.N.; Schiffer, J.T. Rapid and Profound Shifts in the Vaginal Microbiota Following Antibiotic Treatment for Bacterial Vaginosis. J. Infect. Dis. 2015, 212, 793–802. [Google Scholar] [CrossRef]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef]
- Caporaso, J.G.; Lauber, C.L.; Walters, W.A.; Berg-Lyons, D.; Huntley, J.; Fierer, N. Ultra-high-throughput microbial community analysis on the Illumina HiSeq and MiSeq platforms. ISME J. 2012, 6, 1621–1624. [Google Scholar] [CrossRef]
- Raza, G.S.; Putaala, H.; Hibberd, A.A.; Alhoniemi, E.; Tiihonen, K.; Mäkelä, K.A. Polydextrose changes the gut microbiome and attenuates fasting triglyceride and cholesterol levels in Western diet fed mice. Sci. Rep. 2017, 7, 5294. [Google Scholar] [CrossRef] [PubMed]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Bokulich, N.A.; Kaehler, B.D.; Rideout, J.R.; Dillon, M.; Bolyen, E.; Knight, R. Optimizing taxonomic classification of marker-gene amplicon sequences with QIIME 2′s q2-feature-classifier plugin. Microbiome 2018, 6, 90. [Google Scholar] [CrossRef] [PubMed]
- Katoh, K.; Standley, D.M. MAFFT multiple sequence alignment software version 7: Improvements in performance and usability. Mol. Biol. Evol. 2013, 30, 772–780. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Yoon, S.H.; Ha, S.M.; Kwon, S.; Lim, J.; Kim, Y.; Seo, H. Introducing EzBioCloud: A taxonomically united database of 16S rRNA gene sequences and whole-genome assemblies. Int. J. Syst. Evol. Microbiol. 2017, 67, 1613–1617. [Google Scholar] [CrossRef]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B (Methodol.) 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Faith, D.P. Conservation evaluation and phylogenetic diversity. Biol. Conserv. 1992, 61, 1–10. [Google Scholar] [CrossRef]
- Lozupone, C.; Knight, R. UniFrac: A new phylogenetic method for comparing microbial communities. Appl. Environ. Microbiol. 2005, 71, 8228–8235. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008; Available online: http://www.R-project.org (accessed on 20 April 2018).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2009; Available online: http://CRAN.R-project.org/package=ggplot2 (accessed on 20 April 2018).
- Harrell, F.E., Jr.; Dupont, C. Hmisc: Harrell Miscellaneous. R Package Version 4.0-3. 2017. Available online: http://CRAN.R-project.org/package=Hmisc (accessed on 20 April 2018).
- Warnes, G.R.; Bolker, B.; Bonebakker, L.; Gentleman, R.; Liaw, W.H.A.; Lumley, T. Gplots: Various R Programming Tools for Plotting Data. 2012. Available online: http://CRAN.R-project.org/package=gplots (accessed on 20 April 2018).
- Deng, Z.L.; Gottschick, C.; Bhuju, S.; Masur, C.; Abels, C.; Wagner-Dobler, I. Metatranscriptome Analysis of the Vaginal Microbiota Reveals Potential Mechanisms for Protection against Metronidazole in Bacterial Vaginosis. mSphere 2018, 3. [Google Scholar] [CrossRef] [PubMed]
- Macklaim, J.M.; Clemente, J.C.; Knight, R.; Gloor, G.B.; Reid, G. Changes in vaginal microbiota following antimicrobial and probiotic therapy. Microb. Ecol. Health Dis. 2015, 26, 27799. [Google Scholar] [CrossRef] [PubMed]
- Xiao, B.; Niu, X.; Han, N.; Wang, B.; Du, P.; Na, R. Predictive value of the composition of the vaginal microbiota in bacterial vaginosis, a dynamic study to identify recurrence-related flora. Sci. Rep. 2016, 6, 26674. [Google Scholar] [CrossRef] [PubMed]
- Fredricks, D.N.; Fiedler, T.L.; Marrazzo, J.M. Molecular identification of bacteria associated with bacterial vaginosis. N. Engl. J. Med. 2005, 353, 1899–1911. [Google Scholar] [CrossRef]
- Onderdonk, A.B.; Delaney, M.L.; Fichorova, R.N. The Human Microbiome during Bacterial Vaginosis. Clin. Microbiol. Rev. 2016, 29, 223–238. [Google Scholar] [CrossRef]
- Tao, Z.; Zhang, L.; Zhang, Q.; Lv, T.; Chen, R.; Wang, L.; Huang, Z.; Hu, L.; Liao, Q. The Pathogenesis of Streptococcus anginosus in Aerobic Vaginitis. Infect. Drug Resist. 2019, 12, 3745–3754. [Google Scholar] [CrossRef]
- Martin, D.H. The microbiota of the vagina and its influence on women’s health and disease. Am. J. Med. Sci. 2012, 343, 2–9. [Google Scholar] [CrossRef]
- van de Wijgert, J.H.; Borgdorff, H.; Verhelst, R.; Crucitti, T.; Francis, S.; Verstraelen, H. The vaginal microbiota: What have we learned after a decade of molecular characterization? PLoS ONE 2014, 9, e105998. [Google Scholar] [CrossRef]
- Virtanen, S.; Rantsi, T.; Virtanen, A.; Kervinen, K.; Nieminen, P.; Kalliala, I. Vaginal Microbiota Composition Correlates between Pap Smear Microscopy and Next Generation Sequencing and Associates to Socioeconomic Status. Sci. Rep. 2019, 9, 7750. [Google Scholar] [CrossRef]
- Vaneechoutte, M. Lactobacillus iners. The unusual suspect. Res. Microbiol. 2017, 168, 826–836. [Google Scholar] [CrossRef]
- Srinivasan, S.; Liu, C.; Mitchell, C.M.; Fiedler, T.L.; Thomas, K.K.; Agnew, K.J. Temporal variability of human vaginal bacteria and relationship with bacterial vaginosis. PLoS ONE 2010, 5, e10197. [Google Scholar] [CrossRef]
- Verstraelen, H.; Verhelst, R.; Claeys, G.; De Backer, E.; Temmerman, M.; Vaneechoutte, M. Longitudinal analysis of the vaginal microflora in pregnancy suggests that L. crispatus promotes the stability of the normal vaginal microflora and that L. gasseri and/or L. iners are more conducive to the occurrence of abnormal vaginal microflora. BMC Microbiol. 2009, 9, 116. [Google Scholar] [CrossRef]
- Witkin, S.; Linhares, I. Why do lactobacilli dominate the human vaginal microbiota? BJOG 2017, 124, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Witkin, S.S.; Mendes-Soares, H.; Linhares, I.M.; Jayaram, A.; Ledger, W.J.; Forney, L.J. Influence of vaginal bacteria and D- and L-lactic acid isomers on vaginal extracellular matrix metalloproteinase inducer: Implications for protection against upper genital tract infections. mBio 2013, 4, e00460-13. [Google Scholar] [CrossRef]
- McKinnon, L.R.; Achilles, S.L.; Bradshaw, C.S.; Burgener, A.; Crucitti, T.; Fredricks, D.N. The Evolving Facets of Bacterial Vaginosis: Implications for HIV Transmission. AIDS Res. Hum. Retroviruses 2019, 35, 219–228. [Google Scholar] [CrossRef] [PubMed]
- De Backer, E.; Verhelst, R.; Verstraelen, H.; Alqumber, M.A.; Burton, J.P.; Tagg, J.R. Quantitative determination by real-time PCR of four vaginal Lactobacillus species, Gardnerella vaginalis and Atopobium vaginae indicates an inverse relationship between L. gasseri and L. iners. BMC Microbiol. 2007, 7, 115. [Google Scholar] [CrossRef]
- Donders, G.G.G.; Gonzaga, A.; Marconi, C.; Donders, F.; Michiels, T.; Eggermont, N. Increased vaginal pH in Ugandan women: What does it indicate? Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1297–1303. [Google Scholar] [CrossRef][Green Version]
- Fettweis, J.M.; Brooks, J.P.; Serrano, M.G.; Sheth, N.U.; Girerd, P.H.; Edwards, D.J. Differences in vaginal microbiome in African American women versus women of European ancestry. Microbiology 2014, 160 Pt 10, 2272–2282. [Google Scholar] [CrossRef]
- Ravel, J.; Gajer, P.; Abdo, Z.; Schneider, G.M.; Koenig, S.S.K.; McCulle, S.L. Vaginal microbiome of reproductive-age women. Proc. Natl. Acad. Sci. USA 2011, 108 (Suppl. S1), 4680–4687. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nugent Score | Group 1 Canestest Negative | Group 2 Canestest Positive | ||
|---|---|---|---|---|
| Day 1 | Day 1 | Day 8 | Day 15 | |
| 0–3 | 21 | 11 | 25 | 20 |
| 4–6 | 6 | 4 | 2 | 4 |
| >7 | 3 | 15 | 3 | 6 |
| Total | 30 | 30 | 30 | 30 |
| Relative Abundance (%), Mean ± SD | p-Value (FDR adj.) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Taxon | Group 1 | Group 2 | |||||||
| n = 29 | Day 1 n = 30 | Day 8 n = 30 | Day 15 n = 30 | Group 1 vs. Group 2 Day 1 | Group 1 vs. Group 2 Day 8 | Group 2 Day 1 vs. Day 8 | Group 2 Day 8 vs. Day 15 | Group 2 Day 1 vs. Day 15 | |
| Actinobacteria | |||||||||
| Adlercreutzia sp. | 0.1 ± 0.2 | 0.3 ± 0.4 | 0.01 ± 0.03 | 0.1 ± 0.2 | 0.018 | <0.001 | 0.008 | ||
| Atopobium vaginae | 1.8 ± 3.9 | 5.9 ± 7.4 | 0.2 ± 1.2 | 1.2 ± 3.0 | 0.018 | <0.001 | 0.011 | ||
| Coriobacteriaceae sp. | 0.5 ± 1.4 | 0.5 ± 1.2 | 0.00 ± 0.00 | 0.01 ± 0.01 | 0.001 | 0.008 | |||
| Corynebacterium sp. | 0.1 ± 0.1 | 0.2 ± 0.7 | 0.7 ± 1.4 | 0.1 ± 0.1 | 0.001 | <0.001 | |||
| Gardnerella vaginalis | 9.6 ± 18.6 | 14.6 ± 11.7 | 6.1 ± 16.9 | 11.5 ± 20.0 | 0.018 | 0.002 | |||
| Bacteroidetes | |||||||||
| Bacteroidales sp. | 0.002 ± 0.01 | 0.2 ± 0.6 | 0.2 ± 0.6 | 0.3 ± 1.5 | 0.018 | ||||
| Porphyromonas sp. | 0.1 ± 0.1 | 0.6 ± 0.9 | 0.3 ± 1.0 | 0.4 ± 1.0 | 0.018 | 0.001 | 0.035 | ||
| Prevotella pallens | 0.5 ± 1.7 | 0.5 ± 1.3 | 0.1 ± 0.3 | 0.3 ± 1.0 | 0.008 | 0.035 | |||
| Prevotella (timonensis/bivia) | 7.6 ± 15.0 | 18.0 ± 14.9 | 1.4 ± 4.0 | 6.7 ± 9.9 | 0.003 | 0.049 | <0.001 | 0.007 | |
| Firmicutes | |||||||||
| Aerococcus sp. | 0.3 ± 0.8 | 1.1 ± 1.9 | 1.0 ± 3.8 | 0.4 ± 1.0 | 0.003 | ||||
| Anaerococcus sp. | 0.2 ± 0.3 | 0.6 ± 1.0 | 0.02 ± 0.1 | 1.2 ± 3.5 | 0.025 | 0.001 | <0.001 | <0.001 | |
| Clostridium sp. | 0.8 ± 2.0 | 1.6 ± 2.5 | 0.03 ± 0.1 | 0.1 ± 0.3 | 0.013 | <0.001 | 0.008 | ||
| Dialister sp. | 0.6 ± 1.2 | 1.2 ± 1.0 | 0.1 ± 0.4 | 0.8 ± 1.6 | 0.004 | <0.001 | 0.011 | ||
| Finegoldia sp. | 0.1 ± 0.2 | 0.6 ± 1.2 | 0.1 ± 0.5 | 0.5 ± 0.8 | <0.001 | <0.001 | <0.001 | ||
| Gemella sp. | 0.1 ± 0.3 | 0.3 ± 0.6 | 0.01 ± 0.5 | 0.4 ± 1.1 | 0.002 | ||||
| Lactobacillus (crispatus/acidophilus) | 19.2 ± 36.0 | 3.5 ± 15.2 | 6.8 ± 23.4 | 6.5 ± 20.9 | 0.042 | ||||
| Lactobacillus iners | 37.5 ± 41.3 | 25.8 ± 34.2 | 67.8 ± 41.0 | 55.6 ± 41.5 | 0.049 | 0.003 | |||
| Lactobacillus (jensenii) | 4.6 ± 10.6 | 1.3 ± 4.8 | 3.4 ± 10.7 | 2.2 ± 7.6 | 0.018 | ||||
| Megasphaera sp. | 2.0 ± 4.2 | 4.5 ± 4.8 | 0.1 ± 0.6 | 1.3 ± 4.4 | 0.018 | <0.001 | 0.008 | ||
| Parvimonas sp. | 0.2 ± 0.4 | 0.9 ± 1.0 | 0.1 ± 0.3 | 0.3 ± 0.9 | 0.004 | <0.001 | <0.001 | 0.009 | |
| Peptoniphilus sp. | 0.3 ± 0.5 | 1.0 ± 1.1 | 0.2 ± 0.8 | 0.8 ± 1.8 | 0.003 | 0.049 | <0.001 | 0.024 | 0.016 |
| Peptostreptococcus anaerobius | 0.1 ± 0.5 | 0.4 ± 0.8 | 0.02 ± 0.1 | 0.2 ± 0.7 | <0.001 | ||||
| Fusobacteria | |||||||||
| Fusobacterium sp. | 0.1 ± 0.5 | 0.6 ± 1.5 | 0.2 ± 0.8 | 0.4 ± 1.3 | 0.046 | ||||
| Sneathia sp. | 2.0 ± 5.3 | 6.8 ± 10.3 | 1.2 ± 4.2 | 2.5 ± 6.3 | 0.018 | 0.011 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehtoranta, L.; Hibberd, A.A.; Reimari, J.; Junnila, J.; Yeung, N.; Maukonen, J.; Crawford, G.; Ouwehand, A.C. Recovery of Vaginal Microbiota after Standard Treatment for Bacterial Vaginosis Infection: An Observational Study. Microorganisms 2020, 8, 875. https://doi.org/10.3390/microorganisms8060875
Lehtoranta L, Hibberd AA, Reimari J, Junnila J, Yeung N, Maukonen J, Crawford G, Ouwehand AC. Recovery of Vaginal Microbiota after Standard Treatment for Bacterial Vaginosis Infection: An Observational Study. Microorganisms. 2020; 8(6):875. https://doi.org/10.3390/microorganisms8060875
Chicago/Turabian StyleLehtoranta, Liisa, Ashley A. Hibberd, Jenni Reimari, Jouni Junnila, Nicolas Yeung, Johanna Maukonen, Gordon Crawford, and Arthur C. Ouwehand. 2020. "Recovery of Vaginal Microbiota after Standard Treatment for Bacterial Vaginosis Infection: An Observational Study" Microorganisms 8, no. 6: 875. https://doi.org/10.3390/microorganisms8060875
APA StyleLehtoranta, L., Hibberd, A. A., Reimari, J., Junnila, J., Yeung, N., Maukonen, J., Crawford, G., & Ouwehand, A. C. (2020). Recovery of Vaginal Microbiota after Standard Treatment for Bacterial Vaginosis Infection: An Observational Study. Microorganisms, 8(6), 875. https://doi.org/10.3390/microorganisms8060875