Clinical and Microbiological Efficacy of Pyrophosphate Containing Toothpaste: A Double-Blinded Placebo-Controlled Randomized Clinical Trial

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
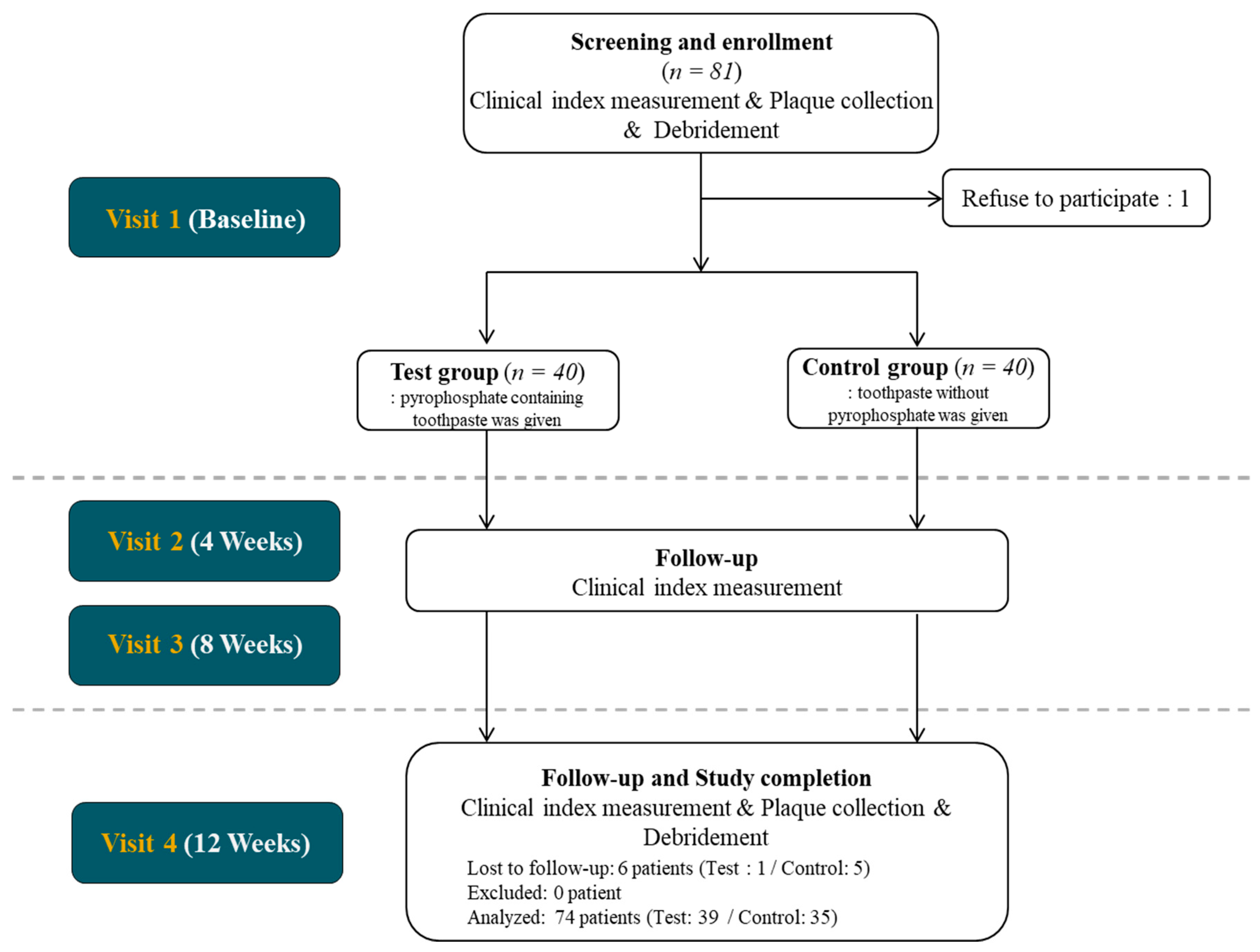
2.1. Study Design and Population
2.2. Sample Size Estimation
2.3. Randomization and Blinding
- Test group: Toothpaste containing 3.4% tetrasodium pyrophosphate was given.
- Control group: Placebo toothpaste without pyrophosphate was given.
2.4. Inclusion and Exclusion Criteria
2.5. Baseline Measurement and Follow up Measurements
2.6. Genomic DNA (gDNA) Extraction
2.7. Sample Preparation and Sequencing
2.8. Microbiome Analysis and Statistical Anaylsis
2.9. Statistical Anaylsis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Lamont, R.J. Beyond the red complex and into more complexity: The polymicrobial synergy and dysbiosis (PSD) model of periodontal disease etiology. Mol. Oral Microbiol. 2012, 27, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.S.; Griffen, A.L.; Barton, J.A.; Paster, B.J.; Moeschberger, M.L.; Leys, E.J. New bacterial species associated with chronic periodontitis. J. Dent. Res. 2003, 82, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Griffen, A.L.; Beall, C.J.; Campbell, J.H.; Firestone, N.D.; Kumar, P.S.; Yang, Z.K.; Podar, M.; Leys, E.J. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. ISME J. 2012, 6, 1176–1185. [Google Scholar] [CrossRef]
- Akcali, A.; Lang, N.P. Dental calculus: The calcified biofilm and its role in disease development. Periodontology 2000 2018, 76, 109–115. [Google Scholar] [CrossRef]
- Jepsen, S.; Deschner, J.; Braun, A.; Schwarz, F.; Eberhard, J. Calculus removal and the prevention of its formation. Periodontology 2000 2011, 55, 167–188. [Google Scholar] [CrossRef]
- Adams, D. Calculus-Inhibition Agents: A Review of Recent Clinical Trials. Adv. Dent. Res. 1995, 9, 410–418. [Google Scholar] [CrossRef]
- Fairbrother, K.J.; Heasman, P.A. Anticalculus agents. J. Clin. Periodontol. 2000, 27, 285–301. [Google Scholar] [CrossRef]
- Rustogi, K.N.; Triratana, T.; Timpawat, S.; Nakornchai, S.; Volpe, A.R. The effect of an anticalculus dentifrice on calculus formation and gingival recession in Thai children and teenagers: One-year study. Study #2. An anticalculus dentifrice containing 1.3% soluble pyrophosphate and 1.5% of a copolymer. J. Clin. Dent. 1991, 3 (Suppl. B), B31-6. [Google Scholar]
- Gaengler, P.; Kurbad, A.; Weinert, W. Evaluation of anti-calculus efficacy. An SEM method of evaluating the effectiveness of pyrophosphate dentifrice on calculus formation. J. Clin. Periodontol. 1993, 20, 144–146. [Google Scholar] [CrossRef]
- Cobb, C.M. Clinical significance of non-surgical periodontal therapy: An evidence-based perspective of scaling and root planing. J. Clin. Periodontol. 2002, 29 (Suppl. 2), 6–16. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Marco Del Castillo, A.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef] [PubMed]
- Genco, R.J.; Borgnakke, W.S. Diabetes as a potential risk for periodontitis: Association studies. Periodontology 2000 2020, 83, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, H.N.; Zhen, Z.; Pelekos, G.; Wu, M.Z.; Chen, Y.; Tonetti, M.; Tse, H.F.; Yiu, K.H.; Jin, L. A randomized controlled trial of the effects of non-surgical periodontal therapy on cardiac function assessed by echocardiography in type 2 diabetic patients. J. Clin. Periodontol. 2020, 47, 726–736. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Mallatt, M.E.; Beiswanger, B.B.; Stookey, G.K.; Swancar, J.R.; Hennon, D.K. Influence of Soluble Pyrophosphate on Calculus Formation in Adults. J. Dent. Res. 1985, 64, 1159–1162. [Google Scholar] [CrossRef]
- Gomez, A.; Espinoza, J.L.; Harkins, D.M.; Leong, P.; Saffery, R.; Bockmann, M.; Torralba, M.; Kuelbs, C.; Kodukula, R.; Inman, J.; et al. Host Genetic Control of the Oral Microbiome in Health and Disease. Cell Host Microbe 2017, 22, 269–278.E3. [Google Scholar] [CrossRef] [PubMed]
- Loe, H. The Gingival Index, the Plaque Index and the Retention Index Systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Greene, J.C.; Vermillion, J.R. The Simplified Oral Hygiene Index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef]
- Caporaso, J.G.; Kuczynski, J.; Stombaugh, J.; Bittinger, K.; Bushman, F.D.; Costello, E.K.; Fierer, N.; Pena, A.G.; Goodrich, J.K.; Gordon, J.I.; et al. QIIME allows analysis of high-throughput community sequencing data. Nat. Methods 2010, 7, 335–336. [Google Scholar] [CrossRef]
- Martin, M. Cutadapt removes adapter sequences from high-throughput sequencing reads. EMBnet. J. 2011, 17. [Google Scholar] [CrossRef]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. DADA2: High-resolution sample inference from Illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J. The role of spirochetes in periodontal disease. Adv. Dent. Res. 1988, 2, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Perez-Chaparro, P.J.; Goncalves, C.; Figueiredo, L.C.; Faveri, M.; Lobao, E.; Tamashiro, N.; Duarte, P.; Feres, M. Newly identified pathogens associated with periodontitis: A systematic review. J. Dent. Res. 2014, 93, 846–858. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.C.; Ebersole, J.L. Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: The “red complex”, a prototype polybacterial pathogenic consortium in periodontitis. Periodontology 2000 2005, 38, 72–122. [Google Scholar] [CrossRef]
- Van der Reijden, W.A.; Dellemijn-Kippuw, N.; Stijne-van Nes, A.M.; de Soet, J.J.; van Winkelhoff, A.J. Mutans streptococci in subgingival plaque of treated and untreated patients with periodontitis. J. Clin. Periodontol. 2001, 28, 686–691. [Google Scholar] [CrossRef]
- Hillman, J.D.; Socransky, S.S.; Shivers, M. The Relationships between Streptococcal Species and Periodontopathic Bacteria in Human Dental Plaque. Arch. Oral Biol. 1985, 30, 791–795. [Google Scholar] [CrossRef]
- Stingu, C.S.; Eschrich, K.; Rodloff, A.C.; Schaumann, R.; Jentsch, H. Periodontitis is associated with a loss of colonization by Streptococcus sanguinis. J. Med. Microbiol. 2008, 57, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J. Role of Streptococcus mutans in human dental decay. Microbiol. Rev. 1986, 50, 353–380. [Google Scholar] [CrossRef]
- Jiang, Q.; Liu, J.; Chen, L.; Gan, N.; Yang, D. The Oral Microbiome in the Elderly With Dental Caries and Health. Front. Cell Infect. Microbiol. 2018, 8, 442. [Google Scholar] [CrossRef]
- Kolenbrander, P.E.; Andersen, R.N.; Blehert, D.S.; Egland, P.G.; Foster, J.S.; Palmer, R.J. Communication among oral bacteria. Microbiol. Mol. Biol. Rev. 2002, 66, 486–505. [Google Scholar] [CrossRef] [PubMed]
- Signat, B.; Roques, C.; Poulet, P.; Duffaut, D. Role of Fusobacterium nucleatum in Periodontal Health and Disease. Curr. Issues Mol. Biol. 2011, 13, 25–35. [Google Scholar] [PubMed]
- Slots, J.; Genco, R.J. Black-pigmented Bacteroides species, Capnocytophaga species, and Actinobacillus actinomycetemcomitans in human periodontal disease: Virulence factors in colonization, survival, and tissue destruction. J. Dent. Res. 1984, 63, 412–421. [Google Scholar] [CrossRef]
- Heller, D.; Silva-Boghossian, C.M.; do Souto, R.M.; Colombo, A.P. Subgingival microbial profiles of generalized aggressive and chronic periodontal diseases. Arch. Oral Biol. 2012, 57, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Nonnenmacher, C.; Mutters, R.; de Jacoby, L.F. Microbiological characteristics of subgingival microbiota in adult periodontitis, localized juvenile periodontitis and rapidly progressive periodontitis subjects. Clin. Microbiol. Infect. 2001, 7, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Liljemark, W.F.; Bloomquist, C.G.; Uhl, L.A.; Schaffer, E.M.; Wolff, L.F.; Pihlstrom, B.L.; Bandt, C.L. Distribution of oral Haemophilus species in dental plaque from a large adult population. Infect. Immun. 1984, 46, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Hsu, M.T.; Sturr, G.; Curran, T.M.; Marquis, R.E. Inhibition of streptococcal growth, F-ATPase and pyrophosphatase by diphosphonates. Oral Microbiol. Immunol. 1995, 10, 47–53. [Google Scholar] [CrossRef]
- Sturr, M.G.; Marquis, R.E. Comparative acid tolerances and inhibitor sensitivities of isolated F-ATPases of oral lactic acid bacteria. Appl. Environ. Microbiol. 1992, 58, 2287–2291. [Google Scholar] [CrossRef]
- Groisman, E.A.; Hollands, K.; Kriner, M.A.; Lee, E.J.; Park, S.Y.; Pontes, M.H. Bacterial Mg2+ homeostasis, transport, and virulence. Annu. Rev. Genet. 2013, 47, 625–646. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 35) | Test (n = 39) | p Value (Control vs. Test) | |
|---|---|---|---|
| Male/Female | 14/21 | 19/20 | 0.14 |
| Age | 37.08 ± 11.08 | 33.72 ± 11.74 | 0.49 |
| Baseline (before Debridement) | 4 Weeks | 8 Weeks | 12 Weeks | p Value (4 Weeks vs. 12 Weeks) | ||
|---|---|---|---|---|---|---|
| PI | Control | 3.84 ± 1.90 | 2.50 ± 1.68 | 2.26 ± 1.61 | 2.09 ± 1.52 | 0.33 |
| Test | 3.56 ± 1.82 | 2.77 ± 2.07 | 2.32 ± 1.97 | 1.86 ± 1.46 * | 0.037 | |
| p value (Test vs. Control) | 0.35 | 0.74 | 0.87 | 0.52 | ||
| CI | Control | 1.66 ± 1.29 | 0.50 ± 0.54 | 0.61 ± 0.84 | 0.48 ± 0.38 | 0.58 |
| Test | 1.43 ± 1.25 | 0.47 ± 0.50 | 0.53 ± 0.60 | 0.47 ± 0.42 | 0.73 | |
| p value (Test vs. Control) | 0.26 | 0.90 | 0.78 | 0.70 | ||
| CI 41 | Control | 4.26 ± 1.56 | 2.40 ± 2.44 | 1.83 ± 1.92 | 2.14 ± 1.65 | 0.92 |
| Test | 4.18 ± 2.15 | 2.15 ± 2.29 | 2.10 ±2.26 | 2.33 ± 2.20 | 0.63 | |
| p value (Test vs. Control) | 0.66 | 0.75 | 0.84 | 0.98 | ||
| GI | Control | 5.43 ± 2.54 | 4.19 ± 2.34 | 4.32 ± 2.42 | 4.03 ± 2.73 | 0.92 |
| Test | 5.51 ± 2.98 | 4.30 ± 2.73 | 3.73 ± 2.64 | 3.42 ± 2.45 | 0.14 | |
| p value (Test vs. Control) | 0.83 | 0.78 | 0.42 | 0.28 | ||
| PD | Control | 2.68 ± 0.30 | 2.48 ± 0.29 | 2.53 ± 0.25 | 2.48 ± 0.27 | 0.93 |
| Test | 2.61 ± 0.32 | 2.55 ±0.29 | 2.55 ± 0.27 | 2.56 ± 0.21 | 0.67 | |
| p value (Test vs. Control) | 0.37 | 0.47 | 1.00 | 0.27 | ||
| BOP | Control | 1.77 ± 1.16 | 1.07 ± 0.83 | 1.11 ± 0.89 | 0.93 ± 0.88 | 0.40 |
| Test | 1.79 ± 1.40 | 1.23 ± 0.98 | 1.06 ± 0.98 | 0.84 ± 0.81 | 0.08 | |
| p value (Test vs. Control) | 0.93 | 0.53 | 0.51 | 0.56 |
| Baseline | 12 Weeks | |||||
|---|---|---|---|---|---|---|
| Control (%) | Test (%) | Total (%) | Control (%) | Test (%) | Total (%) | |
| Firmicutes | 33.43 | 29.03 | 31.14 | 37.00 | 41.23 *** | 39.17 |
| Proteobacteria | 37.8 | 40.04 | 38.97 | 33.63 | 28.45 *** | 30.97 |
| Actinobacteria | 18.17 | 18.57 | 18.38 | 20.70 | 22.96 | 21.86 |
| Bacteroidetes | 7.94 | 8.67 | 8.32 | 6.71 | 5.81 | 6.25 |
| Fusobacteria | 2.48 | 2.93 | 2.71 | 1.84 | 1.41 ** | 1.62 |
| Spirochaetes | 0.11 | 0.55 | 0.34 | 0.01 ** | 0.03 * | 0.02 |
| TM7 | 0.02 | 0.03 | 0.03 | 0.07 *** | 0.07 | 0.07 |
| Others | 0.05 | 0.17 | 0.11 | 0.04 | 0.04 | 0.04 |
| Baseline | 12 Weeks | |||||
|---|---|---|---|---|---|---|
| Control (%) | Test (%) | Total (%) | Control (%) | Test (%) | Total (%) | |
| Streptococcus | 30.00 | 25.65 | 27.73 | 33.15 | 31.69 ** | 35.48 |
| Lautropia | 12.37 | 12.63 | 12.51 | 8.18 | 10.62 | 8.81 |
| Actinomyces | 7.61 | 7.59 | 7.60 | 8.99 | 8.69 | 9.74 |
| Haemophilus | 7.37 | 9.42 | 8.44 | 6.08 | 6.44 ** | 4.53 |
| f_Neisseriaceae | 6.92 | 6.77 | 6.84 | 6.70 | 6.38 | 5.94 |
| Neisseria | 5.41 | 5.67 | 5.54 | 7.25 | 5.98 | 6.41 |
| Rothia | 4.8 | 4.93 | 4.87 | 4.84 | 5.23 | 5.57 |
| Corynebacterium | 4.55 | 4.98 | 4.77 | 4.46 | 4.65 | 4.53 |
| Capnocytophaga | 3.97 | 3.73 | 3.85 | 3.38 | 3.37 * | 2.91 |
| f_Propionibacteriaceae | 1.08 | 0.95 | 1.01 | 2.20 | 1.42 | 1.82 |
| Kingella | 1.35 | 1.45 | 1.40 | 1.27 | 1.37 | 1.33 |
| f_Weeksellaceae | 1.38 | 1.09 | 1.23 | 1.45 | 1.26 | 1.28 |
| Fusobacterium | 1.22 | 2.21 | 1.73 | 0.77 | 1.25 ** | 0.79 |
| Others | 11.98 | 12.93 | 12.48 | 11.28 | 11.65 | 10.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hong, I.; Lee, H.G.; Keum, H.L.; Kim, M.J.; Jung, U.-W.; Kim, K.; Kim, S.Y.; Park, T.; Kim, H.-J.; Kim, J.J.; et al. Clinical and Microbiological Efficacy of Pyrophosphate Containing Toothpaste: A Double-Blinded Placebo-Controlled Randomized Clinical Trial. Microorganisms 2020, 8, 1806. https://doi.org/10.3390/microorganisms8111806
Hong I, Lee HG, Keum HL, Kim MJ, Jung U-W, Kim K, Kim SY, Park T, Kim H-J, Kim JJ, et al. Clinical and Microbiological Efficacy of Pyrophosphate Containing Toothpaste: A Double-Blinded Placebo-Controlled Randomized Clinical Trial. Microorganisms. 2020; 8(11):1806. https://doi.org/10.3390/microorganisms8111806
Chicago/Turabian StyleHong, Inpyo, Hyun Gee Lee, Hye Lim Keum, Myong Ji Kim, Ui-Won Jung, KiJung Kim, Su Yeon Kim, Taehun Park, Hye-Jin Kim, Jin Ju Kim, and et al. 2020. "Clinical and Microbiological Efficacy of Pyrophosphate Containing Toothpaste: A Double-Blinded Placebo-Controlled Randomized Clinical Trial" Microorganisms 8, no. 11: 1806. https://doi.org/10.3390/microorganisms8111806
APA StyleHong, I., Lee, H. G., Keum, H. L., Kim, M. J., Jung, U.-W., Kim, K., Kim, S. Y., Park, T., Kim, H.-J., Kim, J. J., Sul, W. J., An, S., & Cha, J.-K. (2020). Clinical and Microbiological Efficacy of Pyrophosphate Containing Toothpaste: A Double-Blinded Placebo-Controlled Randomized Clinical Trial. Microorganisms, 8(11), 1806. https://doi.org/10.3390/microorganisms8111806