Abstract
Background/Objectives: Neisseria meningitidis is a human-specific pathogen capable of causing life-threatening illnesses. Occasionally, it is recovered from unusual sites, other than the bloodstream or the central nervous system. Herein, we describe two rare manifestations due to N. meningitidis within a year (2024) in Greece. Methods: Atypical infection due to N. meningitidis was diagnosed in two different patients: Case-1 presented with an inflammatory swelling in the mid-line of the neck, and Case-2 presented with swelling of the left knee. Both patients had high fever and no neurological signs at admission; Case-2 progressed to meningoencephalitis. Phenotypic and genotypic identifications were carried out in both cases. Results: Case-1 and Case-2 isolates were identified as follows: MenX: 18, 25-44, F5-5, ST-823; 198cc and MenB: 7-1, 1, F3-3, ST-7460; 32cc for PorA, FetA and MLST, respectively. MenX was identified for the first time in Greece and finetyping revealed rare genotypic characteristics. Both isolates were susceptible to cefotaxime, ceftriaxone and rifampicin, while Case-2 isolate expressed reduced susceptibility to penicillin and resistance to ciprofloxacin. Both patients recovered fully. Conclusions: Although uncommon, N. meningitidis may be isolated from atypical sites and specimens. Clinicians and microbiologists should remain aware that meningococcus is a potential cause of infections beyond meningitis and septicaemia.
1. Introduction
Neisseria meningitidis, also known as meningococcus, is an encapsulated, aerobic, Gram-negative diplococcus belonging to the Neisseriaceae family. It is estimated that nearly 10% of the global population carries the bacterium with no symptoms, with carriage rates reaching up to 23.7% among adolescents and young adults in developed countries [1]. Meningococcus is an obligate human pathogen, responsible for the invasive meningococcal disease (IMD) with clinical manifestations such as meningitis and/or septicaemia, which may result in high morbidity and mortality rates worldwide [2].
The pathogen is transmitted via close or lengthy contact with patients or asymptomatic carriers, through dispersion of higher respiratory and throat secretions. Diabetes mellitus, obesity, malignancies, renal disease, immunosuppression, and chronic steroid therapy are all considered as predisposing factors for IMD. However, serious disease manifestations due to N. meningitidis have also been described in the immunocompetent population or as a result of the transition from asymptomatic carriage to invasive disease [3,4].
The virulence of N. meningitidis is influenced by various factors, such as endotoxin, outer membrane adhesive proteins, iron sequestration, and capsular polysaccharide. Based on the structure and the immune response of the capsule, meningococcus may be classified in 12 serogroups: A, B, C, E, H, I, K, L, W, X, Y, Z, and 29E. The more frequently encountered serogroups responsible for IMD are A, B, C, W, X, and Y. MenB and MenC have the wider geographical distribution, whereas MenX is limited to the African sub-Saharan region. In the industrialized countries, MenB appears to be the predominant cause of endemic meningococcal disease, while MenC seems responsible for both endemic cases and sporadic epidemics [2].
IMD is manifested as acute bacterial meningitis and/or septicaemia, with symptoms and signs such as headache, fever, cervical stiffness, photophobia, severe vomiting, haemorrhagic rash, lethargy, and decreased level of consciousness [5]. At the same time, there is an increasing trend of atypical manifestations due to N. meningitidis. Reports on unusual sites of infection include the lower respiratory system [5], soft tissues [6], urogenital tract [7], gastrointestinal tract [5], eyes [8], as well as joints [5].
The aforementioned cases have been described in both adults and children, whereas the transmission route is not always clear. Two rare cases of atypical clinical manifestations caused by Neisseria meningitidis are presented. They occurred in Greece, in 2024, in two patients that lacked signs of neurological attack at the time of the diagnosis.
2. Materials and Methods
2.1. Patients
2.1.1. Case-1
An 8-year-old boy presented at the Emergency Department of a pediatric hospital in Athens in May 2024 with fever lasting 24 h, cough, rhinitis, and a single episode of vomiting. Additionally, purulent discharge was observed in the midline cervical region. According to the patient’s medical history, he had undergone surgical removal of a thyroglossal duct cyst 18 months prior to admission. Over the past three months, the boy had experienced recurrent episodes of inflammation at the surgical site, characterized by localized abscess formation, treated with oral antibiotic therapy, which first consisted of amoxicillin/clavulanic acid, followed by cefprozil.
On clinical examination upon admission, the patient was in relatively good general condition, with a temperature of 37.8 °C and a heart rate of 130 bpm. The clinical presentation included erythematous tonsils and tenderness in the cervical region, while the cervical lymph nodes were palpable and small bilaterally. Clinical examination revealed a localized inflammation in the neck area, including erythema, swelling, and purulent discharge. The neurological assessment was negative, and the purulent fluid was sent to the laboratory for further microbiological investigation.
2.1.2. Case-2
A 25-year-old male visited the Emergency Department of a tertiary general hospital of Athens in November 2024, presenting symptoms such as high fever, swelling of the left knee, and localized pain for the last nine days. The patient’s medical history was not pertinent to his medical condition, and he had no underlying diseases; furthermore, he reported to be vaccinated with MenC vaccine (Meningitec® Pfizer Inc, New York, NY, USA). With the exception of the local inflammatory signs, no other symptoms or signs were recorded, including neurological ones. According to the medical record, the patient was admitted in the Orthopaedics department, where he underwent arthrocentesis. The synovial fluid and blood cultures were sent to the Microbiology Department for further microbiological examination.
Within four hours, the patient’s clinical condition deteriorated acutely, manifesting with symptoms including sudden headache, vomiting, and pain also to the right knee. He was admitted in the Neurology Department, and an emergency lumbar puncture was performed. The cerebrospinal fluid (CSF) was sent to the Microbiology Department for further microbiological tests.
2.2. Laboratory Identification
Specimens from both the 8-year-old boy and the 25-year-old male were subjected to Gram-staining for initial assessment, followed by culture on selective and differential media to facilitate the identification of both aerobic and anaerobic bacterial pathogens. For the isolation of fastidious organisms, particularly microaerophilic bacteria, the specimens were inoculated onto chocolate agar—a nutrient-rich medium supplemented with factors V (NAD) and X (hemin)—and incubated at 37 °C in an atmosphere containing 5% CO2. In addition, specimens were cultured on Columbia CNA agar (CNA) and CDC anaerobe blood agar to support the growth of Gram-positive cocci and obligate anaerobes, respectively. Plates were incubated under appropriate atmospheric conditions: aerobic, anaerobic, and microaerophilic, depending on the suspected organisms. Identification of isolates was performed using standard microbiological techniques including colony morphology, biochemical testing, and, where appropriate, matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS), following the manufacturer’s instructions and established protocols.
Additionally, for Case-2, the BIOFIRE® FilmArray multiplex PCR system (bioMérieux, Craponne, France) was deployed for timely identification, using Blood Culture Identification 2 (BCID2) and Meningitis/Encephalitis (ME) Panels.
2.3. Phenotypic and Genotypic Characterization
Phenotypic and genotypic characterizations of the isolates were conducted at the National Meningitis Reference Laboratory. Serogroup determination was initially performed using a slide agglutination test (Remel Europe Ltd., Dartford, Kent, UK) in accordance with the manufacturer’s instructions. To confirm and further characterize the isolates, a multiplex polymerase chain reaction (PCR) assay targeting capsule-specific genes corresponding to Neisseria meningitidis serogroups A, B, C, W, and Y was employed, following previously published protocols [9].
2.4. Molecular Characterization and Finetyping
Further molecular characterization of the isolates was performed by finetyping using multilocus sequence typing (MLST), PorA, and FetA gene sequencing, as previously described [10,11]. Sequence analysis was conducted using the Neisseria database hosted at PubMLST.org (http://pubmlst.org/neisseria/) (assessed 20 May 2024 and 14 November 2024) for the two isolates respectively [12]. Sequence types (STs) were assigned based on allelic profiles and grouped into clonal complexes (ccs) according to the database definitions. PorA genotyping focused on variable regions 1 and 2 (VR1 and VR2) and was compared with reference sequences available in the PorA section of the PubMLST database (http://pubmlst.org/neisseria/PorA/) (assessed 20 May 2024 and 14 November 2024) for the two isolates respectively [12]. Similarly, the variable region of the fetA gene (FetA VR) was determined following established protocols [11] and compared with sequences in the FetA VR database (http://pubmlst.org/neisseria/FetA/), accessed on 20 May 2024 and 14 November 2024 for the two patient isolates, respectively [12].
2.5. Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed using E-test gradient strips (LI-OFILCHEM S.R.L., Roseto degli Abruzzi, Italy) in accordance with the guidelines established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST). Minimum Inhibitory Concentrations (MICs) were determined for five antimicrobial agents: penicillin, cefotaxime, ceftriaxone, rifampicin, and ciprofloxacin. Interpretation of MIC values was carried out using the EUCAST Clinical Breakpoint Tables, version 14.0, effective as of 1 January 2024 [13].
3. Results
3.1. Clinical and Laboratory Data
Both cases presented with fever and a localized swelling, each one in different body sites, with no neurological signs. Laboratory testing for Case-1 revealed leukocytosis (WBC 18,600/μL) and elevated CRP (58.3 mg/L) (Table 1). Imaging studies, including ultrasound and MRI of the neck, revealed a pathological finding: a linear contrast-enhancing lesion suggestive of a fistulous tract at the level of the hyoid bone, immediately left of the midline, with associated inflammation of the overlying subcutaneous tissue (Figure 1). The patient was diagnosed with a cervical abscess based on clinical and laboratory findings.

Table 1.
Clinical profile of the patients at admission and overall length of hospitalization.
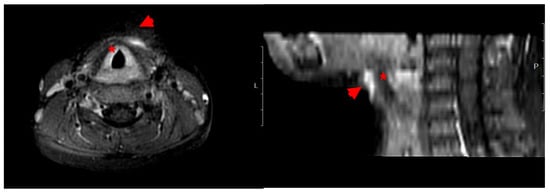
Figure 1.
Imaging (MRI). Case-1: Characteristics of the lesion in the cervical region. By the use of T2-weighted Magnetic Resonance. Axial (horizontal) view (left) and sagittal (side) view (right) of the neck. Hyperintense (bright) areas anterior to the trachea (red star) are indicated by red arrowheads suggesting a fluid collection or, abscess, or edematous tissue.
Case-2 laboratory testing upon admission revealed leukocytosis (WBC 21,760/μL) and elevated CRP (295.9 mg/L) (Table 1). Both synovial and cerebrospinal fluids were pathological; the microscopic evaluation by Gram staining revealed the presence of numerous polymorphonuclear neutrophils, along with intracellular and extracellular Gram-negative coffee-bean-like diplococci (Table 2). The blood cultures were negative after five days of incubation.
Table 2.
Microbiological characteristics of the specimens examined in both patients.
According to the basic immunological studies (C-3, C-4), both patients were immunocompetent.
3.2. Strain Identification by Conventional Methods
Upon 24 h incubation, small, round, greyish, non-haemolytic, glistening colonies with clearly defined edge were observed in both blood and chocolate agar. The isolates were oxidase-positive and displayed the characteristic pink, coffee-bean shape on Gram stain. Ultimately, both isolates were identified as Neisseria meningitidis. In Case 2, meningococcal genetic material was additionally detected directly from clinical specimens using the BioFire® FilmArray® Blood Culture Identification Panel 2 (BCID2) and the Meningitis/Encephalitis (ME) Panel (bioMérieux SA, Craponne, France).
3.3. Finetyping
Finetyping for PorA, FetA and MLST, revealed the following characteristics: MenX: 18, 25-44, F5-5, 198cc (ST-823) and MenB: 7-1, 1, F3-3, 32cc (ST-7460) for Case-1 and Case-2, respectively.
3.4. Antimicrobial Susceptibility Testing
Both isolates were susceptible to cefotaxime, ceftriaxone, and rifampicin. Reduced susceptibility to penicillin was found in the Case-2 isolate (MIC 0.19 mg/L), while it was also resistant to ciprofloxacin (MIC 0.03 mg/L), as opposed to Case-1 isolate, which was susceptible to both aforementioned antibiotics.
3.5. Antimicrobial Treatment and Outcome
Case-1 treatment included intravenous hydration and empirical antibiotic therapies by the administration of clindamycin and cefotaxime. Patient’s clinical improvement was observed before discharge, with an advice of follow up.
Case-2 was treated with ceftriaxone 2grx2 iv for 12 days and dexamethasone 8mgx4 iv for 5 days. The patient made a full recovery with no further neurological symptoms and signs.
To our knowledge, chemoprophylaxis was prescribed to the close contacts for both cases.
4. Discussion
Atypical presentations, although rare, are increasingly documented, showcasing the changing pattern of infections due to N. meningitidis. Pyelonephritis [14], conjunctivitis [15], pericarditis [16], and preseptal cellulitis [17] have been reported more recently. In France, epiglottitis [18], pneumonia, and abdominal forms associated with novel serogroups [5] increased from 2022 onwards and the overall burden of the COVID-19 pandemic is yet to be established. Specifically, to our knowledge, Case-1, is the third case reported worldwide as an unusual soft tissue manifestation due to N. meningitidis, related to previous surgical removal of a thyroglossal duct cyst. Similar clinical presentations have been documented (2008) in a pediatric patient in the USA [19] and, more recently, (2024) in a 16-year-old boy, otherwise healthy, with thyroglossal duct cyst infection in Thailand [6]. In contrast to the previous two cases, a full strain characterization is presented in Case-1 [MenX: 18, 25-44, F5-5, 198cc (ST-823)].
When compared to other serogroups, MenX is sporadically associated with invasive meningococcal disease worldwide, while it has also been detected in healthy, asymptomatic carriers (children, adolescents, and young adults) [20,21,22,23,24]. Although MenX has been previously identified in Greece [20], this is the first MenX isolate associated with an atypical presentation in our setting, susceptible to all antibiotics tested.
Although pharyngeal carriage of N. meningitidis was not assessed in the child, it is likely that the Case-1 patient was colonized with meningococcus and subsequently developed a localized infection.
Meningococcal arthritis may be manifested as a monoarticular or multiarticular infection, and the affected joints are various, namely knee [25], hip [26], ankle [27], and elbow [28]. In our study, the disease manifested as monoarthritis, and the affected joint was the knee. Knee joint infections have been reported in both children and adults, with or without positive blood cultures [25,29]. Interestingly, primary meningococcal arthritis has also been reported in the knee joint of a 30-year-old male, along with the presence of calcium oxalate crystals in the synovial fluid [30].
Case-2 presented as primary septic monoarthritis in an adult male with no neurological signs. This presentation subsequently revealed an underlying IMD with meningitis and polyarthritis. Septic arthritis is a rare but increasingly reported manifestation of N. meningitidis worldwide. Primary joint infection is rare, as arthritis usually occurs as a complication of acute meningococcal disease, secondary to invasive meningococcemia, and results directly from meningococcal bacteremia or meningitis [31,32]. In any case, bacteremia is key for the invasive infections by N. meningitidis [33]. However, in our study, the blood cultures collected at admission were negative, a finding that might be attributed to an inadequate volume of blood inoculated in the bottles.
Although unusual manifestations of N. meningitidis are rare, the most prevalent serogroups causing such presentations are MenW, which is consistently reported with atypical presentations [34], followed by MenY and MenC, and, to a lesser extent, MenB [5,35]. MenY has been indicted as responsible for arthritis in the USA [36] and Italy [37], and MenC has been identified in Romania [38].
The isolate described in this study was typed as MenB, which appears to be responsible for the majority of IMD cases [39]. This is consistent with a recent study from Italy reporting a case of primary knee septic arthritis in an 87-year-old patient, similar to Case-2 herein presented [29]. Although both the Italian and Greek cases showed similar clinical presentations, the Italian strain belonged to ST-162, cc162, whereas the Greek isolate belonged to ST-7460, cc32.
Susceptibility testing revealed that the isolate exhibited reduced susceptibility to penicillin, a finding not surprising in our setting, given that only 52% of IMD MenB isolates in Greece are susceptible to penicillin [20]. Additionally, the isolate was resistant to ciprofloxacin, an antibiotic recommended for chemoprophylaxis. This case represents the second report of ciprofloxacin-resistant Neisseria meningitidis in Greece. The first documented instance was reported in 2020 and involved two MenB isolates belonging to sequence type ST-3129, identified in a migrant camp on the Greek island of Lesbos [40]. An increasing trend of ciprofloxacin resistance has been recently observed in Europe, as well as in East and South Asia, highlighting the importance of continuous surveillance [41].
5. Conclusions
In conclusion, Neisseria meningitidis, although relatively uncommon in such presentations, can be isolated from atypical sites and clinical specimens, potentially serving as an early indicator of invasive or severe disease. For the prompt initiation of targeted therapy, it is of utmost importance to raise awareness and alertness among both clinicians and microbiologists, ensuring that N. meningitidis is considered in the differential diagnosis, even though it is classically associated with meningitis and septicaemia. Moreover, ongoing and continuous surveillance of meningococcal infections is vital for monitoring the evolving epidemiology and for developing tailored strategies and prevention efforts.
Author Contributions
Conceptualization, G.T.; methodology, K.A., G.C., A.X., S.S., C.K., A.T., L.N., F.R., M.G., N.M., D.Z., E.O., M.-K.T. and G.T.; software, A.X., S.S., M.-K.T. and G.T.; validation, K.A., A.X., S.S., C.K., A.T., D.Z., E.O., N.M. and G.T.; formal analysis, K.A., G.C., A.X., S.S. and G.T.; investigation, K.A., G.C., A.X., S.S., C.K., T.G., A.T., L.N., F.R., M.G., D.Z., E.O., N.M., M.-K.T. and G.T.; resources, K.A., G.C., A.T. and N.M.; data curation G.T.; writing—original draft preparation, K.A., G.T. and G.C.; writing—review and editing, G.T., K.A., G.C., A.X., S.S., C.K., T.G., A.T., L.N. and D.Z., E.O., M.-K.T., A.P., M.O., N.M. and M.G.; visualization, G.T.; supervision, G.T.; project administration, G.T.; funding acquisition, G.T. All authors have read and agreed to the published version of the manuscript.
Funding
The study was funded by the National Organization of Public Health (EODY) (funding number 6264/2024) in the frame of the annual financial support to the National Meningitis Reference Laboratory.
Institutional Review Board Statement
Ethical review and approval were waived for this study because depersonalized data from notifiable disease registry and laboratory findings were used.
Informed Consent Statement
Patient consent was waived due to the use of depersonalized data from a notifiable disease registry and laboratory findings.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Harrison, O.B.; Claus, H.; Jiang, Y.; Bennett, J.S.; Bratcher, H.; Jolley, K.; Corton, C.; Care, R.; Poolman, J.T.; Zollinger, W.D.; et al. Description and Nomenclature of Neisseria meningitidis Capsule Locus. Emerg. Infect. Dis. 2013, 19, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Rouphael, N.G.; Stephens, D.S. Neisseria meningitidis: Biology, microbiology, and epidemiology. Methods Mol Biol. 2012, 799, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, B.; Kittai, A.; Chang, S. Neisseria meningitidis as a cause of facial cellulitis. BMJ Case Rep. 2014, 2014, bcr2014203774. [Google Scholar] [CrossRef] [PubMed]
- Mustapha, M.M.; Marsh, J.W.; Shutt, K.A.; Schlackman, J.; Ezeonwuka, C.; Farley, M.M.; Stephens, D.S.; Wang, X.; Van Tyne, D.; Harrison, L.H. Transmission Dynamics and Microevolution of Neisseria meningitidis During Carriage and Invasive Disease in High School Students in Georgia and Maryland, 2006–2007. J. Infect. Dis. 2021, 223, 2038–2047. [Google Scholar] [CrossRef]
- Taha, S.; Deghmane, A.E.; Taha, M.K. Recent increase in atypical presentations of invasive meningococcal disease in France. BMC Infect. Dis. 2024, 24, 640. [Google Scholar] [CrossRef]
- Pinitsubsin, L.; Pongchaikul, P.; Binsirawanich, P.; Trirattanapikul, A. A rare manifestation: Neisseria meningitidis infection of thyroglossal duct cyst. Clin. Infect. Pract. 2024, 23, 100363. [Google Scholar] [CrossRef]
- Tsakalos, A.; Xirogianni, A.; Ekonomou, G.; Papandreou, A.; Prokopiou, E.; Vagiakou, E.; Tzanakaki, G. Symptomatic female genital tract infections due to Neisseria meningitidis in Athens, Greece. Diagnostics 2021, 11, 1265. [Google Scholar] [CrossRef]
- Parikh, S.R.; Campbell, H.; Mandal, S.; Ramsay, M.E.; Ladhani, S.N. Primary meningococcal conjunctivitis: Summary of evidence for the clinical and public health management of cases and close contacts. J. Infect. 2019, 79, 6. [Google Scholar] [CrossRef]
- Drakopoulou, Z.; Kesanopoulos, K.; Sioumala, M.; Tambaki, A.; Kremastinou, J.; Tzanakaki, G. Simultaneous single-tube PCR-based assay for the direct identification of the five most common meningococcal serogroups from clinical samples. FEMS Immunol. Med. Microbiol. 2008, 53, 178–182. [Google Scholar] [CrossRef]
- Russell, J.E.; Jolley, K.; Feavers, I.M.; Maiden, M.; Suker, J. PorA Variable Regions of Neisseria meningitidis. Emerg. Infect. Dis. 2004, 10, 674–678. [Google Scholar] [CrossRef]
- Maiden, M.; Bygraves, J.A.; Feil, E.; Morelli, G.; Russell, J.E.; Urwin, R.; Zhang, Q.; Zhou, J.; Zurth, K.; Caugant, D.A.; et al. Multilocus sequence typing: A portable approach to the identification of clones within populations of pathogenic microorganisms. Proc. Natl. Acad. Sci. USA 1998, 95, 3140–3145. [Google Scholar] [CrossRef]
- Jolley, K.A.; Bray, J.E.; Maiden, M.C.J. Open-access bacterial population genomics: BIGSdb software, the PubMLST.org website and their applications. Wellcome Open Res. 2018, 3, 124. [Google Scholar] [CrossRef]
- EUCAST. European Committee on Antimicrobial Susceptibility Testing. 2025. Available online: https://www.eucast.org/clinical_breakpoints (accessed on 6 July 2025).
- Hamze, H.; Press, N.; Stefanovic, A.; Ritchie, G.; Romney, M. Neisseria meningitidis pyelonephritis: A rare and unusual presentation of an established pathogen. Clin. Microbiol. Newsl. 2024, 47, 9–13. [Google Scholar] [CrossRef]
- Matsuo, Y.; Monden, Y.; Watanabe, H.; Takahashi, H.; Akeda, Y.; Akune, H.; Sasaki, K.; Ishio, D.; Yamazaki, K.; Tashiro, N.; et al. A case of primary meningococcal conjunctivitis in an older patient. J. Infect. Chemother. 2025, 31, 102702. [Google Scholar] [CrossRef] [PubMed]
- Singh, A. Meningococcal disease presenting with acute myopericarditis and concurrent acute meningitis. Emerg. Care Med. 2024, 1, 95–102. [Google Scholar] [CrossRef]
- Atay Ünal, N.; Bedir Demirdağ, T.; Tarlan, B.; Polat, M.; Tapısız, A.; Tezer, H. A Rare Cause of Preseptal Cellulitis: Neisseria meningitidis. Pediatr. Infect. Dis. J. 2024, 43, e295–e926. [Google Scholar] [CrossRef]
- Deghmane, A.E.; Taha, S.; Taha, M.K. Not Only Meningitis but Also Epiglottitis: An Emerging Clinical Presentation of Invasive Meningococcal Disease. Open Forum Infect. Dis. 2023, 11, ofad615. [Google Scholar] [CrossRef]
- Gupta, R.; Levent, F.; Healy, C.M.; Edwards, M.S. Unusual soft tissue manifestations of Neisseria meningitidis infections. Clin. Pediatr. 2008, 47, 400–403. [Google Scholar] [CrossRef]
- Spiliopoulou, I.; Xirogianni, A.; Simantirakis, S.; Tzanakaki, G. Meningococcal Antibiotic Resistance: Mo-lecular Characterization of Isolates from Patients with Invasive Meningococcal Disease (IMD) in Greece. Antibiotics 2023, 12, 1136. [Google Scholar] [CrossRef]
- Cassiolato, A.P.; Camargo, C.H.; Piccoli Cecconi, M.C.; Christakis, S.; Gonçalves, C.R.; Rodrigues Campos, K.; Takenori Higa, F.; Andrade Pereira, G.; de Moraes, C.; Silva de Lemos, A.P. Genomic characterization of inva-sive meningococcal X isolates from Brazil, 1992–2022. Int. Microbiol. 2023, 26, 611–618. [Google Scholar] [CrossRef]
- Goeders, N.; Vanneste, K.; Roosens, N.H.C.; Bogaerts, B.; Mattheus, W. Molecular and WGS-based charac-terization of invasive Neisseria meningitidis isolates collected in Belgium (2016–2022) and MenB-FHbp vaccine coverage estimation of serogroup B. Vaccine 2025, 55, 127026. [Google Scholar] [CrossRef]
- Law, D.K.; Lefebvre, B.; Gilca, R.; Deng, S.; Zhou, J.; De Wals, P.; Tsang, R.S. Characterization of invasive Neisseria meningitidis strains from Québec, Canada, during a period of increased serogroup B disease, 2009–2013: Phenotyping and genotyping with special emphasis on the non-carbohydrate protein vaccine targets. BMC Microbiol. 2015, 15, 143. [Google Scholar] [CrossRef]
- Kizil, M.C.; Kilic, O.; Ceyhan, M.; Iseri Nepesov, M.; Karbuz, A.; Kurugol, Z.; Hacimustafaoglu, M.; Celebi, S.; Dinleyici, M.; Carman, K.B.; et al. Nasopharyngeal Meningococcal Carriage among Children and Adolescents in Turkey in 2018: An Unexpected High Serogroup X Carriage. Children 2021, 8, 871. [Google Scholar] [CrossRef]
- O’Sullivan, D.; Linnane, B.; Mostyn, A.; Jonathan, N.; Lenihan, M.; O’Connell, N.H.; Dunne, C.P. Detection of Neisseria meningitidis in a paediatric patient with septic arthritis using multiplexed diagnostic PCR targeting meningitis/encephalitis (ME). Ann. Clin. Microbiol. Antimicrob. 2018, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Fidder, A.R.; de Hartog, B.; Faber, T. Child with serogroup W135 primary meningococcal septic arthritis. BMJ Case Rep. 2019, 12, e229510. [Google Scholar] [CrossRef] [PubMed]
- Boyle, C.; Howard, T.; Griffith, D.; Cowie, J. Primary meningococcal septic arthritis with multiple native joint involvement. BMJ Case Rep. 2018, 2018, bcr2017223197. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.J.; Bowen, A.C.; Hazelton, B.; O’Brien, M.; Blyth, C.C.; Campbell, A.J. Meningococcal serotype W septic arthritis: Case series in children. J. Paediatr. Child. Health 2021, 57, 1990–1994. [Google Scholar] [CrossRef]
- Longo, B.; Fazio, C.; Meini, S.; Neri, A.; Andreoli, E.; Vacca, P.; Salamone, D.; Sani, S.; Mura, M.; Bracalente, I.; et al. Primary septic arthritis of the knee caused by Neisseria meningitidis serogroup B in an elderly patient. Case report and review of the literature. Infection 2023, 51, 499–506. [Google Scholar] [CrossRef]
- Cimé-Aké, E.; Carranza-Enríquez, F.; Hurtado-Arias, J.J.; Muñoz-Castañeda, W.R.A.; Medina-Fonseca, B.; Barrera-Vargas, A.; Lizardo-Thiebaud, M.J.; Saeb-Lima, M.; Merayo-Chalico, J. Primary meningococcal septic arthritis associated with joint calcium oxalate crystals: A case report and review of the literature. Mod. Rheumatol. Case Rep. 2022, 6, 296–300. [Google Scholar] [CrossRef]
- Sarinho, J.C.; Arcadipane, M.S.; Menezes, G.T.; Duarte, D.F.; Cossermelli, W.; Aprahamian, I. Primary meningococcal polyarthritis in an adult woman. Case Rep. Med. 2015, 2015, 563672. [Google Scholar] [CrossRef]
- Masson-Behar, V.; Jacquier, H.; Richette, P.; Ziza, J.M.; Zeller, V.; Rioux, C.; Coustet, B.; Dieudé, P.; Ottaviani, S. Arthritis secondary to meningococcal disease: A case series of 7 patients. Medicine 2017, 96, e7573. [Google Scholar] [CrossRef] [PubMed]
- Vienne, P.; Ducos-Galand, M.; Guiyoule, A.; Pires, R.; Giorgini, D.; Taha, M.K.; Alonso, J.M. The role of particular strains of Neisseria meningitidis in meningococcal arthritis, pericarditis, and pneumonia. Clin. Infect. Dis. 2003, 37, 1639–1642. [Google Scholar] [CrossRef] [PubMed]
- Bertrand-Gerentes, I.; Fanchon, L.; Coste, F.; Glover, R.E.; Guiddir, T.; Taha, M.K. Range of Clinical Manifestations Caused by Invasive Meningococcal Disease Due to Serogroup W: A Systematic Review. Infect. Dis. Ther. 2023, 12, 2337–2351. [Google Scholar] [CrossRef] [PubMed]
- Gyamfi-Brobbey, G.; Clark, S.A.; Campbell, H.; Lekshmi, A.; Ribeiro, S.; Walker, A.; Mensah, A.; Willerton, L.; Walsh, L.; Lucidarme, J.; et al. An analysis of Neisseria meningitidis strains causing meningococcal septic arthritis in England and Wales: 2010–2020. J. Infect. 2022, 85, 390–396. [Google Scholar] [CrossRef]
- Yee, N.M.; Katz, M.; Neu, H.C. Meningitis, pneumonitis, and arthritis caused by Neisseria meningitidis group Y. JAMA 1975, 232, 1354–1355. [Google Scholar] [CrossRef] [PubMed]
- Ricci, S.; Montemaggi, A.; Nieddu, F.; Serranti, D.; Indolfi, G.; Moriondo, M.; Azzari, C. Is primary meningococcal arthritis in children more frequent than we expect? Two pediatric case reports revealed by molecular test. BMC Infect. Dis. 2018, 18, 703. [Google Scholar] [CrossRef]
- Straticiuc, S.; Ignat, A.; Hanganu, E.; Lupu, V.V.; Ciubara, A.B.; Cretu, R. Neisseria meningitidis Serogroup C Causing Primary Arthritis in a Child: Case Report. Medicine 2016, 95, e2745. [Google Scholar] [CrossRef]
- Scholz, S.; Koerber, F.; Meszaros, K.; Fassbender, R.M.; Ultsch, B.; Welte, R.R.; Greiner, W. The cost-of-illness for invasive meningococcal disease caused by serogroup B Neisseria meningitidis (MenB) in Germany. Vaccine 2019, 37, 1692–1701. [Google Scholar] [CrossRef]
- Tzanakaki, G.; Georgakopoulou, T.; Xirogianni, A.; Papandreou, A.; Deghmane, A.E.; Magaziotou, I.; Taha, M.K. First report of meningococcal ciprofloxacin resistance in Greece due to invasive isolates of the sequence type ST-3129. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 2467–2470. [Google Scholar] [CrossRef]
- Deghmane, A.E.; Taha, S.; Taha, M.K. Meningococcal resistance to ciprofloxacin is not rare anymore. J. Antimicrob Chemother. 2025, 80, 311–313. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).