
Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections

Abstract
:1. Introduction
2. Materials and Methods

{kind=link}
{kind=link}
{kind=link}
| Time Frame | Supplements/Nutritional Support | Indication |
|---|---|---|
| Prior to Beginning DDDCT | Biofilm agents: take cinnamon/clove/oregano oil one twice a day (Doctor Inspired Formulations, Hopkinton Drug Compounding Pharmacy, Hopkinton, MA, USA), Biocidin 2 sprays twice a day (Biocidin Botanicals, Aptos, CA, USA), Stevia 15 drops twice a day (NutraMedix, Jupiter, FL, USA) and peppermint oil capsules one twice a day (Infuserve America Compounding Pharmacy, St. Petersburg, FL, USA). If you have had severe/resistant symptoms, speak to your provider about adding on Argentyn 23, 1 teaspoon twice a day (Natural Immunogenics, Sarasota, FL, USA) during the last month of the protocol with or without EDTA suppositories (Detoxamine, Draper, UT, USA) the last week of the protocol for extra biofilm support [137,143]. | Biofilm support |
| Probiotics: Orthobiotic (Ortho Molecular Products, Woodstock, IL, USA), Saccharomyces boulardii (Ortho Molecular Products, Woodstock, IL, USA), Theralac (Master Supplements, Victoria, MN, USA) are all taken twice a day first thing in the morning and last thing before bed, along with ½ a packet of Probiomax 350 billion (Xymogen, Orlando, FL, USA) once a day (this can be used twice a day if there are any loose stools). | Microbiome support | |
| Detoxification/Inflammatory Support: N-Acetyl Cysteine (NAC) 600 mg twice a day (Xymogen, Orlando, FL, USA), glutathione 4 capsules (250 mg each) twice a day (Ortho Molecular Products; or Essential Pro Glutathione, Wellness Pharmacy, Birmingham, AL, USA), Alamax (alpha lipoic acid, Xymogen) 600 mg, one twice a day, curcuplex (Xymogen) 500 mg, one twice a day, sulforaphane glucosinolate (Oncoplex ES, Xymogen) 100 mg, one twice a day, vitamin C 1–2 g twice a day (Xymogen), vitamin E 300 IUs twice a day (Designs for Health, Suffield, CT, USA), NADH (ENADA Nutraceuticals, Las Vegas, NV, USA) 5 mg twice a day; please keep Alka-Seltzer gold or sodium HCO3 (bicarbonate) at home which can be used as needed for temporary increases in underlying Lyme disease symptoms, i.e., severe Herxheimer reactions [130], which is used with 2 g of glutathione all at once, up to three times daily until the Herxheimer reaction resolves [50,144]. You can also use up to 2000 mg of glutathione 3× per day if there are symptoms of methemoglobinemia [118] (blue hands, blue lips, headaches, fatigue, shortness of breath) although the symptoms would be unusual using higher dose methylene blue at a dose of 300 mg twice a day, as it helps keep down significantly elevated methemoglobin levels. | Detoxification/ Inflammatory Support | |
| Weeks 1–4 of DDDCT (slowly increasing dapsone from 25 mg per day to 100 mg per day) | Continue biofilm, microbiome and detoxification/inflammatory support listed above. Add Folic acid support once starting dapsone: two tablets of L-methyl folate 15 mg each, twice a day month one (weeks 1–4), for a total of 60 mg of L-methyl folate per day (Xymogen, Folafy-ER). Folic acid supplementation can be taken at the same time as all antibiotics, twice a day, after breakfast and dinner, with a full stomach. Probiotics should be taken away from antibiotics, i.e., first thing upon awakening, and last thing at night before bedtime. Add B12 support (Methyl protect, one a day, Xymogen) and over the counter (OTC) iron (Fe), between 45–325 mg per day (at lunch, away from antibiotics). Any mineral supplements (magnesium, calcium, zinc, iron, copper, etc.) should be taken at least one hour away from antibiotics to avoid interfering with absorption of tetracyclines. | Addition of Folic acid, B12 and iron helps reduce dapsone induced anemia |
| Week 5–8 DDDCT (100 mg BID) | Continue biofilm, microbiome and detoxification/inflammatory support listed above. Continue B12 and iron support, as listed above. Folic acid dosing doubles on DDDCT: use 4 tablets of L-methyl folate 15 mg each, twice a day, for a total dose of 60 mg of L-methyl folate twice a day (120 mg total). Keep Alka-Seltzer gold or sodium HCO3 (bicarbonate) at home which can be used as needed for temporary increases in underlying Lyme disease symptoms, i.e., severe Herxheimer reactions [130], which is used with 2 g of glutathione all at once, up to three times daily until the Herxheimer reaction resolves [50,144]. You can also use up to 2000 mg of glutathione 3× per day if there are symptoms of methemoglobinemia [118] (blue hands, blue lips, headaches, fatigue, shortness of breath) although the symptoms would be unusual using higher dose methylene blue. | Antioxidant support to help lower methemoglobin levels, along with biofilm, microbiome, and detoxification/inflammatory support. Extra folic acid helps reduce dapsone induced anemia |
| Week 9 (HDDCT) | Continue biofilm, microbiome and detoxification/inflammatory support listed above. Continue folic acid, B12 and iron support, as listed above. Depending on laboratory results week 9, adjust glutathione doses and/or folic acid dosing. This will be based on levels of anemia, and methemoglobin levels. L-methyl folate doses can be increased to 5–6 tablets twice a day week 9 if needed for any increases in anemia from higher dose dapsone. Glutathione dosing can increase to 2000 mg TID, if there are any increases in methemoglobin despite methylene blue dosing at 300 mg PO BID. | Biofilm, microbiome, inflammatory, detoxification, hematological support |
| Weeks 10–14 (first month off dapsone) | Continue biofilm, microbiome and detoxification/inflammatory support listed above. Continue folic acid, B12 and iron support, as above. Folic acid doses for L-methyl folate may be slowly decreased from 4–5 twice a day (by week 11) to 3 twice a day (week 12) to 2 twice a day (weeks 13–14, i.e., 60 mg of L-methyl folate per day) depending on the CBC and rapidity of reversal of anemia off dapsone. Individualized dosing for folic acid will depend on the level of anemia; a follow-up CBC and CMP with haptoglobin levels should be done 5–7 days post dapsone combination therapy, especially if any sudden unexpected drops in hemoglobin levels were noted the week on HDDCT (week 9), and/or if any other significant hematological abnormalities were noted. If a CBC and CMP are stable one week post dapsone, repeat laboratory testing week 2–3 weeks later to adjust folic acid dosing. Add a one month mitochondrial regeneration program weeks 10–14: This includes: ATP 360, 3 capsules once a day (Researched Nutritionals), ENADA (NADH) one twice a day; carnitex (Xymogen) two twice a day (not for those with alpha gal allergy), CoQ Power 400 mg twice a day (Researched Nutritionals), Cardio Ribose (Researched Nutritionals), one scoop twice a day, along with Mitoprime (Xymogen) one a day, and Mito NR (Designs for Health, Suffield, CT, USA) two a day. Mitochondrial support has been shown to be helpful in certain patients with a chronic, fatiguing illness. You can stop the mitochondrial supplements after one month post high dose dapsone combination therapy. | Continue to replace healthy GI bacteria with microbiome support 1 month post DDDCT and HDDCT. Continue antioxidant and anti-inflammatory support post DDDCT and HDDCT Mitochondrial support can reverse potential mitochondrial damage from high levels of free radicals/oxidative stress during therapy |
| Weeks 15–19 (2nd month post DDDCT and HDDCT | Lower biofilm support to once a day; Lower microbiome support to once a day. B12 and iron supplementation may be stopped if no deficiencies noted. Antioxidant/anti-inflammatory support with NAC, alpha lipoic acid, glutathione, Curcuplex and sulforaphane glucosinolate (Oncoplex ES) may be continued if ongoing sources of inflammation are present, including but not limited to ongoing infections, environmental toxins (mold, heavy metals), or if needing COVID support. Folic acid dosing is based on the rapidity of reversal of the CBC off dapsone. Patients may require staying on a lower dose of L-methyl folate (15 mg BID) depending on the CBC. |
Medication Regimen for DDDCT and HDDCT
| Time Frame | Medication | Nutritional Support | Laboratory/EKG |
|---|---|---|---|
| Prior to beginning DDDCT | Add medications gradually to ensure GI tolerance. For example, start with Plaquenil (hydroxychloroquine) 200 mg twice a day after meals, Nystatin 500,000 U tablets twice a day, and minocycline (or doxycycline) 100 mg twice a day. Lower-dose minocycline or doxycycline (50 mg twice a day) can be initiated if there is a history of GI intolerance to tetracyclines. If there is no issue with GI tolerance in an adult patient, add rifampin (300 mg BID). Rifabutin 150 mg PO BID may be substituted for rifampin if you are intolerant to rifampin. After several days, then add pyrazinamide (which is dosed by body weight): up to 55 kg = 1000 mg once a day (2 pills of 500 mg once a day); 56–75 kg = 1500 mg once a day (3 pills once a day); over 76–90 kg = 2000 mg once a day (4 pills once a day). The 8-week DDDCT protocol starts when all antibiotics are on board and tolerated (which may add an extra week to the protocol). Rifampin may affect medication levels. Perform a drug interaction check. Adjust doses | See Table 1 regarding doses of biofilm agents, probiotics, detoxification, and inflammatory support. | Patients should be G6PD positive without B12, folate, or iron deficiency before starting dapsone EKG should be normal |
| Week 1 | Plaquenil 200 mg PO BID, doxy (or minocycline) 100 mg PO BID, rifampin 300 mg PO BID, Nystatin 500,000 U tablets, 2 PO BID. Start dapsone 25 mg one PO QD, taken at the same time as the other antibiotics. Add folic acid support: Leucovorin (folinic acid) 25 mg two twice a day (50 mg twice a day) along with 15 mg of L-methyl folate, 2 twice a day. See Table 1 for details. | Add Folic acid support once starting dapsone. | |
| Week 2 | Same doses of the above medication, but increase dapsone to 25 mg PO BID (50 mg/day). Clotrimazole (Mycelex) troches (10 mg QID prn) may be used at any time during the protocol if, despite a strict sugar-free/yeast-free diet, any signs of yeast/Candida arise on the tongue. | See Table 1 | |
| Week 3 | Same doses of the above medication; increase dapsone to 50 mg in the am, 25 mg in the pm for a total of 75 mg per day. | See Table 1 | CBC, CMP is ordered at the end of week 3 with a baseline MetHb |
| Week 4 | Same doses of the above medication; increase dapsone to 50 mg in the morning and 50 mg in the afternoon for a total of 100 mg of dapsone per day. Order 100 mg of dapsone tablets from the pharmacy for week 5 (90 tablets) and renew all of the above medications. Start methylene blue 50 mg twice a day week 4. This is taken with high-dose antioxidants to help reverse methemoglobin levels. See Table 1. This would include 1000 to 2000 mg of glutathione twice a day, vitamin C 1–2 g twice a day, vitamin E 300 IU twice a day, and NADH 5 mg twice a day. Consider starting cimetidine 400 mg twice a day if there has been a history of any significantly elevated methemoglobin levels proceeding into month two. If cimetidine is required due to elevated methemoglobin levels, lower Plaquenil (hydroxychloroquine) once a day and check drug interactions for potential medication interactions. If any significant Herxheimer reactions occur at 100 mg of dapsone that do not resolve with alkalizing and high dose glutathione, or if there is any evidence of unexpected anemia (greater than a 2–3 g drop in hemoglobin) with unexpected rises in methemoglobin (greater than 5%) proceeding into week 4, the dose of dapsone can be temporarily held for a week, increasing Leucovorin to 4 tablets twice a day (100 mg PO BID) with 4, 15 mg L-methyl folate twice a day (60 mg PO BID) until the anemia improves and/or the methemoglobin level decreases. Then restart dapsone at 100 mg per day. | See Table 1 for nutritional support. | |
| Week 5 | Take dapsone 100 mg, 1 dose twice a day (this is officially the start of one month of double-dose dapsone). Add 250 mg of azithromycin (Zithromax) twice a day with a full stomach. Clarithromycin (Biaxin) can alternatively be used as a macrolide instead of Zithromax if insurance coverage requires a different medication. Increase Leucovorin to 25 mg, 4 tablets PO BID (100 mg BID) with 15 mg of L-methyl folate, and 4 tablets PO BID (60 mg BID) for a total dose of 320 mg of folic acid. Increase methylene blue (MB) to 100 mg PO BID × 3 days, then increase MB to 150 mg PO BID. The total dose of MB at the end of week 5 is 300 mg per day. All other medications and nutritional supplements remain the same. Check an EKG and rule out QT prolongation on hydroxychloroquine and azithromycin with one dose of 8 mg of ondansetron (Zofran). If the EKG is stable, you may use ondansetron Q 8 h prn for nausea. Use phenazopyridine (Pyridium) 200 mg PO TID prn for any urinary burning/discomfort on MB. | See Table 1 for nutritional support | CBC, CMP, MetHb, haptoglobin end of week 5 & q week. Check hormones (thyroids, etc.) on rifampin and adjust prn. EKG |
| Week 6 | Increase methylene blue to 200 mg PO BID. All other medications remain the same. May increase methylene blue to 250 mg PO BID if methemoglobin level is >5% despite using antioxidants in Table 1. May add cimetidine if needed for elevated MetHb | See Table 1 | CBC, CMP, MetHb, haptoglobin |
| Week 7 | Increase methylene blue to 250 mg PO BID. All other medications remain the same. May increase methylene blue to 300 mg PO BID if methemoglobin level is >5%. If CBC, CMP, MetHb is stable, continue protocol. May hold dapsone temporarily if any unexpected drops in hemoglobin from baseline (average drop in Hb is 3.5–4 g on DDDCT, which is to be expected). | See Table 1 | CBC, CMP, MetHb, haptoglobin Follow BP QD on MB |
| Week 8 | Increase methylene blue to 300 mg PO BID. This is the final dose adjustment for MB. All other medications remain the same. Dapsone may cause low-grade hemolysis, but if CBC, CMP, and MetHb are stable, continue the protocol. In rare cases, higher doses of MB may result in increased hemolysis. Hold dapsone, increase folic acid dosing, and lower MB to 200 mg PO BID if any unexpected drops in Hb result. | See Table 1 | CBC, CMP, MetHb, haptoglobin |
| Week 9 (HDDCT) | Increase dapsone to 200 mg PO BID for 4 days in a row if treating CLD without evidence of co-infections such as Bartonella, or increase dapsone to 200 mg PO BID × 6 days in a row if treating Bartonella. This is a high-dose dapsone combination therapy. All other medications remain the same. Use ondansetron (Zofran) 8 mg q 8 h prn for any nausea/vomiting. Check labs after 3 and 5 days on HDDCT and adjust dosing based on symptoms and laboratory results. Stop dapsone if the hemoglobin level is >20% and if there is an unexpected drop in hemoglobin > 1–2 g from the prior CBC, hold dapsone, increase folic acid dosing, and lower the MB to 200 mg PO BID. | See Table 1 | CBC, CMP, MetHb, and haptoglobin on days 3 and 5 of HDDCT Follow BP QD on MB |
| Week 10, First week off HDDCT | Stop all antibiotics including tetracyclines (doxycycline or minocycline), rifampin (or rifabutin), pyrazinamide, azithromycin (or clarithromycin), and hydroxychloroquine (Plaquenil). Remain on same doses of Nystatin, Leucovorin, L-methyl folate, all probiotics, biofilm support, and nutritional support. Taper MB. First day off dapsone take 300 mg PO BID, then decrease MB to 200 mg BID for 2 days, 100 mg BID for 2 days, 50 mg PO BID for 2 days, and then stop methylene blue. | See Table 1 Add mitochondrial support | CBC, CMP, MetHb, haptoglobin 4 days post-HDDCT |
| Week 11 | Increase folic acid dosing prn if any unexpected decreases in hemoglobin occur. For example, may increase Leucovorin and L-methyl folate by 1–2 tabs BID for 1 week | See Table 1 | Repeat CBC if unexpected decrease in Hb |
| Week 12 | Decrease folic acid dosing if CBC is stable | See Table 1 | |
| Week 13 | Decrease folic acid dosing if CBC is stable | See Table 1 | CBC, CMP |
| Weeks 14–18, 2nd mo. | Continue to decrease folic acid and nutritional support. If the patient is in remission, no further pulses of HDDCT are required. If Bartonella is still active, consider a 2 week HDDCT pulse (14 days), i.e., Protocol 2, q 6–8 weeks once labs return to normal | See Table 1 | CBC, CMP end of month 2 |
| Time Frame | Medication | Nutritional Support | Laboratory/EKG |
|---|---|---|---|
| Week 1 | Beginning on a Monday, start with Plaquenil (hydroxychloroquine) 200 mg twice a day, minocycline 100 mg twice a day (or doxycycline 100 mg PO BID), Nystatin 500,000 units, two twice a day, and after two days add rifampin (Wednesday), 300 mg twice a day; then after one day (Thursday), add pyrazinamide (PZA) 500 mg tabs, 2–4 once a day (the dose is dependent on body weight (see Table 2); then after one more day (Friday), add azithromycin (Zithromax) 250 mg twice a day. All antibiotics are taken on a full stomach after breakfast and dinner. The methylene blue dosage for week one of this protocol is 50 mg twice a day × 2 days (Monday, Tuesday), then 100 mg twice a day for 2 days (Wednesday, Thursday), then 200 mg twice a day for 3 days (400 mg by days 6–7). At the end of week one, the patient will therefore be on Plaquenil, minocycline (or doxycycline), rifampin (or rifabutin), PZA, Zithromax, Nystatin, and methylene blue. See Table 1 for nutritional support with biofilm agents, probiotics, detoxification, and inflammatory support. Follow a low-histamine diet as per Protocol 1. All psychiatric medications that can interact with methylene blue (MB) must be stopped at least one week before using MB and several weeks afterwards to avoid potential side effects. | See Table 1 | CBC, CMP, and Methemoglobin levels should be normal before starting HDDCT EKG should be WNL; check QT intervals on Plaquenil, azithromycin + ondansetron if not previously conducted |
| Week 2 | Dapsone starts week two, and day 8, is added at a dose of 100 mg twice a day for 1 day (double dose dapsone). This will be taken with Leucovorin 25 mg, 4, twice a day, with L-methyl folate 15 mg (Folafy-ER) 4 twice a day along with all antibiotics and nutritional supplements from week 1. Rifampin will be increased to double dose (300 mg, 2 twice a day) at the beginning of week 2 if liver functions are WNL. For a 4 day HDDCT pulse, days 9–12 you will take high dose dapsone × 4 days (200 mg twice a day). This is primarily for those with CLD/PTLDS without associated co-infections (i.e., Bartonella). For a 6-day HDDCT pulse, i.e., for those with active intracellular co-infections (e.g., Bartonella), take high-dose dapsone (200 mg twice a day) for 6 days, days 9–14, with the same doses of folic acid. The last week, days 8–14, the methylene blue dose is increased to 300 mg twice a day once starting dapsone and continued at that dosage for as long as the patient remains on HDDCT. For those needing phenazopyridine (Pyridium) to decrease urinary tract discomfort, it can be prescribed at a dose of 200 mg three times a day while on methylene blue. Ondansetron 4–8 mg Q8 prn may be used prn for nausea and/or vomiting if QT intervals are WNL | See Table 1 | CBC, CMP, Methemoglobin, and haptoglobin levels are drawn on day 10 and day 12 to rule out any significant hematological and/or laboratory changes |
| Week 3 | Stop all antibiotics including tetracyclines (doxycycline or minocycline), rifampin (or rifabutin), pyrazinamide, azithromycin (or clarithromycin), and hydroxychloroquine. Remain on same doses of Nystatin, Leucovorin, L-methyl folate, all probiotics, biofilm support and nutritional support. Increase folic acid dosing prn if any unexpected decreases in hemoglobin occur post high dose dapsone, weeks 3–4. For example, may increase Leucovorin and L-methyl folate by 1–2 tabs BID for 1 week, then begin a slow taper off folic acid based on the results of the CBC. Taper MB. First day off dapsone take 300 mg PO BID, then decrease MB to 200 mg BID for 2 days, 100 mg BID for 2 days, 50 mg PO BID for 2 days, and then stop methylene blue. Start mitochondrial support. | See Table 1 | Repeat CBC, CMP, Methb and haptoglobin levels on days 17–18, 3–4 days post dapsone |
| Week 4 | Continue with a mitochondrial regeneration protocol post-treatment for a total of 4 weeks (weeks 3–7). ATP 360, 3 a day (Researched Nutritionals), ENADA, one a day; carnitex, 2 twice a day (Xymogen, not for those with alpha-gal allergy); CoQ Power, 2 times a day (Researched Nutritionals); Cardio Ribose, one scoop twice a day; along with Mitoprime (Xymogen), 1 a day; and Mito NR (Designs for Health), 2 a day. Mitochondrial support has been shown to be helpful in some patients with chronic, fatiguing illnesses. Stop the mitochondrial supplements after one month of high-dose dapsone combination therapy. Continue to slowly taper folic acid dosing if the CBC is stable. | See Table 1 | |
| Weeks 5–6 | Finish the mitochondrial regeneration protocol. Continue to taper folic acid. Continued folic acid support will depend on the CBC 3 weeks post-HDDCT. Taper biofilm agents, probiotics, detoxification/inflammatory support as per Table 1 post-dapsone. | See Table 1 | Repeat CBC, CMP 3 weeks post HDDCT |
3. Results
| Patient | M/F | Age | # Courses of DDDCT | # Courses of HDDCT × 4 Days | # Courses of HDDCT × 5–7 Days | Bart FISH + | Bart + Spp., Striae VEGF | Bab FISH + | Bab + spp. | Full Remission # Months | >30% Impr | 21–30% Impr | 11–20% Impr | 10–19% Impr | 0–9% Impr | No C Hange | MSIDS Variables Potentially Affecting Treatment Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 18 | 1 | 0 | 1 (6 d) | Yes | Bh | No | N/A | >3 mo | N/A | N/A | N/A | N/A | N/A | N/A | CVID, POTS, Mold |
| 2 | F | 23 | 1 | 0 | 1 (5 d) | No | Bq | No | N/A | >8 mo | N/A | N/A | N/A | N/A | N/A | N/A | MCAS Leaky Gut |
| 3 | M | 54 | 1 | 0 | 2 (5 d) | Yes | ? spp | No | N/A | >4 mo | N/A | N/A | N/A | N/A | N/A | N/A | BMD, TBRF Mitochondr EM+ |
| 4 | F | 35 | 1 | 5 | 1 (7 d) | No | Yes, Bv, striae | No | Bd | >3 mo | N/A | N/A | N/A | N/A | N/A | N/A | Bd, Anapl, COVID, HSV, Mold, Phase III adrenals, PTSD |
| 5 | M | 41 | 1 | 1 | 0 | No | No | No | No | >6 mo | N/A | N/A | N/A | N/A | N/A | N/A | EM + 21 yrs prior, Insomnia, COVID, Hypoglyc |
| 6 | M | 59 | 1 | 1 | 0 | No | No | No | Bm | >11 mo | N/A | N/A | N/A | N/A | N/A | N/A | Phase II adrenals, COVID |
| 7 | F | 51 | 1 | 1 | 0 | No | No | No | Bm | >22 mo | N/A | N/A | N/A | N/A | N/A | N/A | COVID, Mold, Vasculitis |
| 8 | M | 63 | 1 | 0 | 1 (6 d) | No | Yes, Be | No | N/A | 1 mo | N/A | N/A | N/A | N/A | N/A | N/A | COVID, EBV PCR + Mold, Low T, CVID, Sick × 22 y, Poss EM |
| 9 | M | 53 | 3 | 0 | 1 (6 d) | No | Yes, Be | No | ? | 1 mo | N/A | N/A | N/A | N/A | N/A | N/A | TBRF, Mycopl PCR +, OSA, Phase II Adrenal, Inflamm, sick for 31 y |
| 10 | F | 22 | 1 | 3 Bart pseudo seizures stopped | 1 (6 d) | Yes | Yes, Bq | No | N/A | 2 mo, relapsed during menses × sev d, then felt well | N/A | N/A | N/A | N/A | N/A | N/A | Low GSH, Phase III Adrenal, POTS |
| 11 | F | 31 | 0 Did low dose DDS for mo’s + 100 mg for 2 week | 0 | 1 (4½–5 days) | Yes | Yes Bh, Be | No | BmBd | No | Y, >60% | N/A | N/A | N/A | N/A | N/A | Bd 1:640 +, Bm 1:160 + Phase III adrenal, severe PTSD, Candida, POTS, CVID |
| 12 | M | 22 | 1 | 1 | 0 | No | Yes, Bh, Be, Bv | No | Bm Bd | No | Y, 50% | N/A | N/A | N/A | N/A | N/A | Bm, Bd, Phase III adrenal |
| 13 | M | 45 | 1 | 2 | 0 | No | Yes, Bh, Striae | Yes | BmBd | No? (Cognitive symptoms lingering, but OSA) | Y, >70% | N/A | N/A | N/A | N/A | N/A | OSA, Food Sensitivity, Insulin R, Low T, NASH |
| 14 | F | 60 | 2 | 0 | 1 (6–7 days) Best protocol in 13 yrs | No | Yes, Bh, Be, Bv, ↑ VEGF | No | Bm | No | Y, >60% | N/A | N/A | N/A | N/A | N/A | Bm 1:320 + Mold, PTSD, Phase II Adrenal, POTS, Bart granuloma ↓ size post HDDCT |
| 15 | M | 33 | 1 | 0 | 1 (7 days) | Yes | Yes, Bh, Bq, Be, Bv | Yes | Bm Bd Bo | No | Y 60% | N/A | N/A | N/A | N/A | N/A | Mold, COVID, EBV PCR +. Insomnia, Detox |
| 16 | F | 52 | 1 | 0 | 1 (6 days) | No | Yes, Bart spp. + ↑ VEGF | No | No | No | Y >60% | N/A | N/A | N/A | N/A | N/A | Anaplasma PCR +, COVID, Phase III adrenal, Detox |
| 17 | M | 48 | 1 | 1 All Sx ↓ except PNP | 0 | Yes | Bh, Bq, Bv | Yes | Bd Bo | No | Y >50% | N/A | N/A | N/A | N/A | N/A | Bb, Bab, Bart FISH + PTSD, Microbiome Abn, Insomnia |
| 18 | M | 64 | 1 | 2 | 0 | Yes | Bq Bv | Yes | ? | Physical sx > 18 mo in remission; Cognitive relapse + ? secondary TBD | N/A | N/A | N/A | N/A | N/A | N/A | Elevated Hg blood, Detox, Moderate OSA, Phase 3 Adrenal, hypoglyc, Low B12 |
| 19 | M | 32 | 1 | 0 Did > 1 yr. 100 mg DDSCT | 1 (6 days) but no M.B., due to psych meds. | Yes | Bart genus +, Striae | No | No | No But ↓ psychosis↓ hallucin’s Post HDDCT | Y >30% | N/A | N/A | N/A | N/A | N/A | PTSD, Detox, Mitochond, Insomnia, Vit Def |
| 20 | M | 41 | 1 Bart Striae ↑ 1 year later | 1 | 0 | No | Bh, Striae, ↑ VEGF | No | Bm | No But most Sx gone × 21 mo’s, (f) at 95% N except sl cognitive dysfunction | Y >45% | N/A | N/A | N/A | N/A | N/A | COVID, Heavy metals, Phase II adrenal, CVA × 2, Hx PFO |
| 21 | F | 19 | 3 | 3 Last course w MB 300 BID, ↑ improv | 0 | No | Bh, Bq, ↑ VEGF | No | Bd | No, but for the 1st time in years, had sustained improv, including paralysis | Y > 15% | N/A | N/A | N/A | N/A | N/A | Babesia ++ Severe POTS, EDS, Phase III adrenal, AI IVIG/SQIG, Leaky gut, MCAS, Immune dys(f) |
| 22 | M | 34 | 1 | 4 | 0 | Yes | Bart genus | No | Bd | No | Y 30% | N/A | N/A | N/A | N/A | N/A | Mold +++ Babesia ++ CVID (not yet on IVIG), low T, NASH, insomnia |
| 23 | M | 33 | 1 | 0 | 2 (7 days) | Yes | Bh, Bq, Bk, Bbac Striae | No | Bm Bd, B div | No | N/A | N/A | Y 15% | N/A | N/A | N/A | Bab ++ Mold +++ POTS MCAS CIDP COVID w/EBV PCR+ S/P EM |
| 24 | F | 45 | 2 | 3 Lower dose MB used | 1 (6 d) Dapsone helped ↓ Morgellon’s lesions | Yes | Bh | Yes | ? | No | No | No | No | Y, 15% | N/A | N/A | Morgellons CVID Hypopit:, Phase III adrenal, hypothy, ↓ sex hormones, PTSD, insomnia +++ POTS, Mitochondr dysfunction Inflamm ↑ Vit/min def AI dx with HELLP Syndrome |
| 25 | M | 32 | 1 (only did 2 weeks) | 1 Lower dose MB used (150 mg BID) | 0 | No | No | Yes | Bd | No | No | No | No | No | Y, 5% | N/A | Mold Babesia ++ PTSD Phase II Adrenal. States (f) at 90% N |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Lyme Disease Data and Surveillance|CDC. Available online: https://www.cdc.gov/lyme/datasurveillance/index.html (accessed on 23 May 2023).
- Dong, Y.; Zhou, G.; Cao, W.; Xu, X.; Zhang, Y.; Ji, Z.; Yang, J.; Chen, J.; Liu, M.; Fan, Y.; et al. Global Seroprevalence and Sociodemographic Characteristics of Borrelia burgdorferi Sensu Lato in Human Populations: A Systematic Review and Meta-Analysis. BMJ Glob. Health 2022, 7, e007744. [Google Scholar] [CrossRef] [PubMed]
- Ursinus, J.; Vrijmoeth, H.D.; Harms, M.G.; Tulen, A.D.; Knoop, H.; Gauw, S.A.; Zomer, T.P.; Wong, A.; Friesema, I.H.M.; Vermeeren, Y.M.; et al. Prevalence of Persistent Symptoms after Treatment for Lyme Borreliosis: A Prospective Observational Cohort Study. Lancet Reg. Health Eur. 2021, 6, 100142. [Google Scholar] [CrossRef] [PubMed]
- Aucott, J.N.; Rebman, A.W.; Crowder, L.A.; Kortte, K.B. Post-Treatment Lyme Disease Syndrome Symptomatology and the Impact on Life Functioning: Is There Something Here? Qual. Life Res. 2013, 22, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Mac, S.; Bahia, S.; Simbulan, F.; Pullenayegum, E.M.; Evans, G.A.; Patel, S.N.; Sander, B. Long-Term Sequelae and Health-Related Quality of Life Associated with Lyme Disease: A Systematic Review. Clin. Infect. Dis. 2020, 71, 440–452. [Google Scholar] [CrossRef] [PubMed]
- DeLong, A.; Hsu, M.; Kotsoris, H. Estimation of Cumulative Number of Post-Treatment Lyme Disease Cases in the US, 2016 and 2020. BMC Public Health 2019, 19, 352. [Google Scholar] [CrossRef] [PubMed]
- Burn, L.; Tran, T.M.P.; Pilz, A.; Vyse, A.; Fletcher, M.A.; Angulo, F.J.; Gessner, B.D.; Moïsi, J.C.; Jodar, L.; Stark, J.H. Incidence of Lyme Borreliosis in Europe from National Surveillance Systems (2005–2020). Vector Borne Zoonotic Dis. 2023, 23, 156–171. [Google Scholar] [CrossRef]
- Hook, S.A.; Jeon, S.; Niesobecki, S.A.; Hansen, A.P.; Meek, J.I.; Bjork, J.K.H.; Dorr, F.M.; Rutz, H.J.; Feldman, K.A.; White, J.L.; et al. Economic Burden of Reported Lyme Disease in High-Incidence Areas, United States, 2014–2016. Emerg. Infect. Dis. 2022, 28, 1170–1179. [Google Scholar] [CrossRef]
- Willems, R.; Verhaeghe, N.; Perronne, C.; Borgermans, L.; Annemans, L. Cost of Illness in Patients with Post-Treatment Lyme Disease Syndrome in Belgium. Eur. J. Public Health 2023, 33, 668–674. [Google Scholar] [CrossRef]
- Mojahed, N.; Mohammadkhani, M.A.; Mohamadkhani, A. Climate Crises and Developing Vector-Borne Diseases: A Narrative Review. Iran. J. Public Health 2022, 51, 2664–2673. [Google Scholar] [CrossRef]
- Leibovici, D.G.; Bylund, H.; Björkman, C.; Tokarevich, N.; Thierfelder, T.; Evengård, B.; Quegan, S. Associating Land Cover Changes with Patterns of Incidences of Climate-Sensitive Infections: An Example on Tick-Borne Diseases in the Nordic Area. Int. J. Environ. Res. Public Health 2021, 18, 10963. [Google Scholar] [CrossRef]
- El-Sayed, A.; Kamel, M. Climatic Changes and Their Role in Emergence and Re-Emergence of Diseases. Environ. Sci. Pollut Res. Int. 2020, 27, 22336–22352. [Google Scholar] [CrossRef]
- Hammond, T.T.; Hendrickson, C.I.; Maxwell, T.L.; Petrosky, A.L.; Palme, R.; Pigage, J.C.; Pigage, H.K. Host Biology and Environmental Variables Differentially Predict Flea Abundances for Two Rodent Hosts in a Plague-Relevant System. Int. J. Parasitol. Parasites Wildl. 2019, 9, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Breitschwerdt, E.B. Bartonellosis, One Health and All Creatures Great and Small. Vet. Derm. 2017, 28, 111–121. [Google Scholar] [CrossRef]
- Rebman, A.W.; Aucott, J.N. Post-Treatment Lyme Disease as a Model for Persistent Symptoms in Lyme Disease. Front. Med. 2020, 7, 57. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.H.; Shapiro, E.D.; Soffer, G.K. A Review of Post-Treatment Lyme Disease Syndrome and Chronic Lyme Disease for the Practicing Immunologist. Clin. Rev. Allergy Immunol. 2022, 62, 264–271. [Google Scholar] [CrossRef]
- Lantos, P.M.; Wormser, G.P. Chronic Coinfections in Patients Diagnosed with Chronic Lyme Disease: A Systematic Review. Am. J. Med. 2014, 127, 1105–1110. [Google Scholar] [CrossRef]
- Krause, P.J.; Telford, S.R.; Spielman, A.; Sikand, V.; Ryan, R.; Christianson, D.; Burke, G.; Brassard, P.; Pollack, R.; Peck, J.; et al. Concurrent Lyme Disease and Babesiosis. Evidence for Increased Severity and Duration of Illness. JAMA 1996, 275, 1657–1660. [Google Scholar] [CrossRef]
- Berghoff, W. Chronic Lyme Disease and Co-Infections: Differential Diagnosis. Open Neurol. J. 2012, 6, 158–178. [Google Scholar] [CrossRef]
- Hodzic, E.; Imai, D.; Feng, S.; Barthold, S.W. Resurgence of Persisting Non-Cultivable Borrelia burgdorferi Following Antibiotic Treatment in Mice. PLoS ONE 2014, 9, e86907. [Google Scholar] [CrossRef] [PubMed]
- Straubinger, R.K.; Summers, B.A.; Chang, Y.F.; Appel, M.J. Persistence of Borrelia burgdorferi in Experimentally Infected Dogs after Antibiotic Treatment. J. Clin. Microbiol. 1997, 35, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Embers, M.E.; Barthold, S.W.; Borda, J.T.; Bowers, L.; Doyle, L.; Hodzic, E.; Jacobs, M.B.; Hasenkampf, N.R.; Martin, D.S.; Narasimhan, S.; et al. Persistence of Borrelia burgdorferi in Rhesus Macaques Following Antibiotic Treatment of Disseminated Infection. PLoS ONE 2012, 7, e29914. [Google Scholar] [CrossRef]
- Sapi, E.; Kasliwala, R.S.; Ismail, H.; Torres, J.P.; Oldakowski, M.; Markland, S.; Gaur, G.; Melillo, A.; Eisendle, K.; Liegner, K.B.; et al. The Long-Term Persistence of Borrelia burgdorferi Antigens and DNA in the Tissues of a Patient with Lyme Disease. Antibiotics 2019, 8, 183. [Google Scholar] [CrossRef] [PubMed]
- Middelveen, M.J.; Sapi, E.; Burke, J.; Filush, K.R.; Franco, A.; Fesler, M.C.; Stricker, R.B. Persistent Borrelia Infection in Patients with Ongoing Symptoms of Lyme Disease. Healthcare 2018, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Terkawi, M.A.; Cao, S.; Herbas, M.S.; Nishimura, M.; Li, Y.; Moumouni, P.F.A.; Pyarokhil, A.H.; Kondoh, D.; Kitamura, N.; Nishikawa, Y.; et al. Macrophages Are the Determinant of Resistance to and Outcome of Nonlethal Babesia microti Infection in Mice. Infect. Immun. 2014, 83, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Schetters, T. Mechanisms Involved in the Persistence of Babesia Canis Infection in Dogs. Pathogens 2019, 8, 94. [Google Scholar] [CrossRef]
- Suarez, C.E.; Alzan, H.F.; Silva, M.G.; Rathinasamy, V.; Poole, W.A.; Cooke, B.M. Unravelling the Cellular and Molecular Pathogenesis of Bovine Babesiosis: Is the Sky the Limit? Int. J. Parasitol. 2019, 49, 183–197. [Google Scholar] [CrossRef]
- Bloch, E.M.; Kumar, S.; Krause, P.J. Persistence of Babesia microti Infection in Humans. Pathogens 2019, 8, 102. [Google Scholar] [CrossRef]
- Harms, A.; Dehio, C. Intruders below the Radar: Molecular Pathogenesis of Bartonella spp. Clin. Microbiol. Rev. 2012, 25, 42–78. [Google Scholar] [CrossRef]
- Breitschwerdt, E.B.; Kordick, D.L. Bartonella Infection in Animals: Carriership, Reservoir Potential, Pathogenicity, and Zoonotic Potential for Human Infection. Clin. Microbiol. Rev. 2000, 13, 428–438. [Google Scholar] [CrossRef]
- Krause, P.J.; McKay, K.; Thompson, C.A.; Sikand, V.K.; Lentz, R.; Lepore, T.; Closter, L.; Christianson, D.; Telford, S.R.; Persing, D.; et al. Disease-Specific Diagnosis of Coinfecting Tickborne Zoonoses: Babesiosis, Human Granulocytic Ehrlichiosis, and Lyme Disease. Clin. Infect. Dis. 2002, 34, 1184–1191. [Google Scholar] [CrossRef]
- Steere, A.C.; McHugh, G.; Suarez, C.; Hoitt, J.; Damle, N.; Sikand, V.K. Prospective Study of Coinfection in Patients with Erythema Migrans. Clin. Infect. Dis. 2003, 36, 1078–1081. [Google Scholar] [CrossRef]
- Bloch, E.M.; Zhu, X.; Krause, P.J.; Patel, E.U.; Grabowski, M.K.; Goel, R.; Auwaerter, P.G.; Tobian, A.A.R. Comparing the Epidemiology and Health Burden of Lyme Disease and Babesiosis Hospitalizations in the United States. Open Forum Infect. Dis. 2022, 9, ofac597. [Google Scholar] [CrossRef]
- Stricker, R.B.; Burrascano, J.J.; Harris, N.S.; Horowitz, R.; Johnson, L.; Smith, P.V.; Phillips, S.E. Coinfection with Borrelia burgdorferi and Babesia microti: Bad or Worse? J. Infect. Dis. 2006, 193, 901–902. [Google Scholar] [CrossRef] [PubMed]
- Eskow, E.; Rao, R.-V.S.; Mordechai, E. Concurrent Infection of the Central Nervous System by Borrelia burgdorferi and Bartonella henselae: Evidence for a Novel Tick-Borne Disease Complex. Arch. Neurol. 2001, 58, 1357–1363. [Google Scholar] [CrossRef]
- Cheslock, M.A.; Embers, M.E. Human Bartonellosis: An Underappreciated Public Health Problem? Trop. Med. Infect. Dis. 2019, 4, 69. [Google Scholar] [CrossRef] [PubMed]
- Stricker, R.B.; Fesler, M.C. Chronic Lyme Disease: A Working Case Definition. Am. J. Infect. Dis. 2018, 14, 1–44. [Google Scholar] [CrossRef]
- Shor, S.; Green, C.; Szantyr, B.; Phillips, S.; Liegner, K.; Burrascano, J.; Bransfield, R.; Maloney, E.L. Chronic Lyme Disease: An Evidence-Based Definition by the ILADS Working Group. Antibiotics 2019, 8, 269. [Google Scholar] [CrossRef]
- Anderson, C.; Brissette, C.A. The Brilliance of Borrelia: Mechanisms of Host Immune Evasion by Lyme Disease-Causing Spirochetes. Pathogens 2021, 10, 281. [Google Scholar] [CrossRef]
- Caine, J.A.; Lin, Y.-P.; Kessler, J.R.; Sato, H.; Leong, J.M.; Coburn, J. Borrelia burgdorferi Outer Surface Protein C (OspC) Binds Complement Component C4b and Confers Bloodstream Survival. Cell Microbiol. 2017, 19, e12786. [Google Scholar] [CrossRef]
- Coburn, J.; Garcia, B.; Hu, L.T.; Jewett, M.W.; Kraiczy, P.; Norris, S.J.; Skare, J. Lyme Disease Pathogenesis. Curr. Issues Mol. Biol. 2021, 42, 473–518. [Google Scholar] [CrossRef]
- Lochhead, R.B.; Strle, K.; Arvikar, S.L.; Weis, J.J.; Steere, A.C. Lyme Arthritis: Linking Infection, Inflammation and Autoimmunity. Nat. Rev. Rheumatol. 2021, 17, 449–461. [Google Scholar] [CrossRef]
- Jutras, B.L.; Lochhead, R.B.; Kloos, Z.A.; Biboy, J.; Strle, K.; Booth, C.J.; Govers, S.K.; Gray, J.; Schumann, P.; Vollmer, W.; et al. Borrelia burgdorferi Peptidoglycan Is a Persistent Antigen in Patients with Lyme Arthritis. Proc. Natl. Acad. Sci. USA 2019, 116, 13498–13507. [Google Scholar] [CrossRef]
- Girschick, H.J.; Huppertz, H.I.; Rüssmann, H.; Krenn, V.; Karch, H. Intracellular Persistence of Borrelia burgdorferi in Human Synovial Cells. Rheumatol. Int. 1996, 16, 125–132. [Google Scholar] [CrossRef]
- Karvonen, K.; Nykky, J.; Marjomäki, V.; Gilbert, L. Distinctive Evasion Mechanisms to Allow Persistence of Borrelia burgdorferi in Different Human Cell Lines. Front. Microbiol. 2021, 12, 711291. [Google Scholar] [CrossRef]
- Georgilis, K.; Peacocke, M.; Klempner, M.S. Fibroblasts Protect the Lyme Disease Spirochete, Borrelia burgdorferi, from Ceftriaxone In Vitro. J. Infect. Dis. 1992, 166, 440–444. [Google Scholar] [CrossRef]
- Livengood, J.A.; Gilmore, R.D. Invasion of Human Neuronal and Glial Cells by an Infectious Strain of Borrelia burgdorferi. Microbes Infect. 2006, 8, 2832–2840. [Google Scholar] [CrossRef] [PubMed]
- Crossland, N.A.; Alvarez, X.; Embers, M.E. Late Disseminated Lyme Disease: Associated Pathology and Spirochete Persistence Posttreatment in Rhesus Macaques. Am. J. Pathol. 2018, 188, 672–682. [Google Scholar] [CrossRef]
- Bobe, J.R.; Jutras, B.L.; Horn, E.J.; Embers, M.E.; Bailey, A.; Moritz, R.L.; Zhang, Y.; Soloski, M.J.; Ostfeld, R.S.; Marconi, R.T.; et al. Recent Progress in Lyme Disease and Remaining Challenges. Front. Med. 2021, 18, 666554. [Google Scholar] [CrossRef]
- Horowitz, R.I.; Freeman, P.R. Precision Medicine: The Role of the MSIDS Model in Defining, Diagnosing, and Treating Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome and Other Chronic Illness: Part 2. Healthcare 2018, 6, 129. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, R.I.; Freeman, P.R. Precision Medicine: Retrospective Chart Review and Data Analysis of 200 Patients on Dapsone Combination Therapy for Chronic Lyme Disease/Post-Treatment Lyme Disease Syndrome: Part 1. Int. J. Gen. Med. 2019, 12, 101–119. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.H.; Kim, W.-U. Dysregulation of Gut Microbiota and Chronic Inflammatory Disease: From Epithelial Defense to Host Immunity. Exp. Mol. Med. 2017, 49, e337. [Google Scholar] [CrossRef]
- Morrissette, M.; Pitt, N.; González, A.; Strandwitz, P.; Caboni, M.; Rebman, A.W.; Knight, R.; D’Onofrio, A.; Aucott, J.N.; Soloski, M.J.; et al. A Distinct Microbiome Signature in Posttreatment Lyme Disease Patients. mBio 2020, 11, e02310-20. [Google Scholar] [CrossRef] [PubMed]
- Aleman, R.S.; Moncada, M.; Aryana, K.J. Leaky Gut and the Ingredients That Help Treat It: A Review. Molecules 2023, 28, 619. [Google Scholar] [CrossRef] [PubMed]
- Talkington, J.; Nickell, S.P. Borrelia burgdorferi Spirochetes Induce Mast Cell Activation and Cytokine Release. Infect. Immun. 1999, 67, 1107–1115. [Google Scholar] [CrossRef]
- Alexander, W. 2012 Integrative Healthcare Symposium. Pharm. Ther. 2012, 37, 247–249. [Google Scholar]
- Hope, J. A Review of the Mechanism of Injury and Treatment Approaches for Illness Resulting from Exposure to Water-Damaged Buildings, Mold, and Mycotoxins. Sci. World J. 2013, 2013, 767482. [Google Scholar] [CrossRef]
- Wessels, I.; Maywald, M.; Rink, L. Zinc as a Gatekeeper of Immune Function. Nutrients 2017, 9, 1286. [Google Scholar] [CrossRef]
- Staff, N.P.; Windebank, A.J. Peripheral Neuropathy Due to Vitamin Deficiency, Toxins, and Medications. Continuum 2014, 20, 1293–1306. [Google Scholar] [CrossRef] [PubMed]
- Motamedi, V.; Kanefsky, R.; Matsangas, P.; Mithani, S.; Jeromin, A.; Brock, M.S.; Mysliwiec, V.; Gill, J. Elevated Tau and Interleukin-6 Concentrations in Adults with Obstructive Sleep Apnea. Sleep Med. 2018, 43, 71–76. [Google Scholar] [CrossRef]
- Weinstein, E.R.; Rebman, A.W.; Aucott, J.N.; Johnson-Greene, D.; Bechtold, K.T. Sleep Quality in Well-Defined Lyme Disease: A Clinical Cohort Study in Maryland. Sleep 2018, 41. [Google Scholar] [CrossRef]
- Peacock, B.N.; Gherezghiher, T.B.; Hilario, J.D.; Kellermann, G.H. New Insights into Lyme Disease. Redox Biol. 2015, 5, 66–70. [Google Scholar] [CrossRef]
- Bransfield, R.C. The Psychoimmunology of Lyme/Tick-Borne Diseases and Its Association with Neuropsychiatric Symptoms. Open Neurol. J. 2012, 6, 88–93. [Google Scholar] [CrossRef]
- Perkins, C.M.P.; Shumway, C.N.; Jackson, M.W.L. Lyme Neuroborreliosis Presenting as the Syndrome of Inappropriate Antidiuretic Hormone Secretion. Med. Gen. Med. 2006, 8, 71. [Google Scholar]
- Kanjwal, K.; Karabin, B.; Kanjwal, Y.; Grubb, B.P. Postural Orthostatic Tachycardia Syndrome Following Lyme Disease. Cardiol. J. 2011, 18, 63–66. [Google Scholar]
- Yehudina, Y.; Trypilka, S. Lyme Borreliosis as a Trigger for Autoimmune Disease. Cureus 2021, 13, e18648. [Google Scholar] [CrossRef]
- Bransfield, R.C. Neuropsychiatric Lyme Borreliosis: An Overview with a Focus on a Specialty Psychiatrist’s Clinical Practice. Healthcare 2018, 6, 104. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, H.W.; Dworkin, B.; Forseter, G.; Nadelman, R.B.; Connolly, C.; Luciano, B.B.; Nowakowski, J.; O’Brien, T.A.; Calmann, M.; Wormser, G.P. Liver Function in Early Lyme Disease. Hepatology 1996, 23, 1412–1417. [Google Scholar] [CrossRef]
- Budzáková, M.; Trna, J. Gastrointestinal and Hepatic Symptoms of Tickborne Diseases. Vnitr. Lek. 2020, 66, 232–235. [Google Scholar] [CrossRef]
- Horowitz, R.; Horowitz, R.I. Why Can’t I Get Better?: Solving the Mystery of Lyme and Chronic Disease; Macmillan: London, UK, 2013; ISBN 978-1-250-01940-0. [Google Scholar]
- Horowitz, R. How Can. I Get Better?: An Action Plan. for Treating Resistant Lyme & Chronic Disease; St. Martin’s Publishing Group: New York, NY, USA, 2017; ISBN 978-1-250-11144-9. [Google Scholar]
- Feng, J.; Shi, W.; Zhang, S.; Zhang, Y. Persister Mechanisms in Borrelia burgdorferi: Implications for Improved Intervention. Emerg. Microbes Infect. 2015, 4, e51. [Google Scholar] [CrossRef]
- Sapi, E.; Bastian, S.L.; Mpoy, C.M.; Scott, S.; Rattelle, A.; Pabbati, N.; Poruri, A.; Burugu, D.; Theophilus, P.A.S.; Pham, T.V.; et al. Characterization of Biofilm Formation by Borrelia burgdorferi in Vitro. PLoS ONE 2012, 7, e48277. [Google Scholar] [CrossRef] [PubMed]
- Pothineni, V.R.; Wagh, D.; Babar, M.M.; Inayathullah, M.; Solow-Cordero, D.; Kim, K.-M.; Samineni, A.V.; Parekh, M.B.; Tayebi, L.; Rajadas, J. Identification of New Drug Candidates against Borrelia burgdorferi Using High-Throughput Screening. Drug Des. Dev. 2016, 10, 1307–1322. [Google Scholar] [CrossRef]
- Sharma, B.; Brown, A.V.; Matluck, N.E.; Hu, L.T.; Lewis, K. Borrelia burgdorferi, the Causative Agent of Lyme Disease, Forms Drug-Tolerant Persister Cells. Antimicrob. Agents Chemother. 2015, 59, 4616–4624. [Google Scholar] [CrossRef]
- Feng, J.; Zhang, S.; Shi, W.; Zhang, Y. Ceftriaxone Pulse Dosing Fails to Eradicate Biofilm-like Microcolony B. burgdorferi Persisters Which Are Sterilized by Daptomycin/Doxycycline/Cefuroxime without Pulse Dosing. Front. Microbiol. 2016, 7, 1744. [Google Scholar] [CrossRef]
- Feng, J.; Li, T.; Yee, R.; Yuan, Y.; Bai, C.; Cai, M.; Shi, W.; Embers, M.; Brayton, C.; Saeki, H.; et al. Stationary Phase Persister/Biofilm Microcolony of Borrelia burgdorferi Causes More Severe Disease in a Mouse Model of Lyme Arthritis: Implications for Understanding Persistence, Post-Treatment Lyme Disease Syndrome (PTLDS), and Treatment Failure. Discov. Med. 2019, 27, 125–138. [Google Scholar]
- Liang, F.T.; Yan, J.; Mbow, M.L.; Sviat, S.L.; Gilmore, R.D.; Mamula, M.; Fikrig, E. Borrelia burgdorferi Changes Its Surface Antigenic Expression in Response to Host Immune Responses. Infect. Immun. 2004, 72, 5759–5767. [Google Scholar] [CrossRef] [PubMed]
- Berndtson, K. Review of Evidence for Immune Evasion and Persistent Infection in Lyme Disease. Int. J. Gen. Med. 2013, 6, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Bamm, V.V.; Ko, J.T.; Mainprize, I.L.; Sanderson, V.P.; Wills, M.K.B. Lyme Disease Frontiers: Reconciling Borrelia Biology and Clinical Conundrums. Pathogens 2019, 8, 299. [Google Scholar] [CrossRef]
- Hastey, C.J.; Elsner, R.A.; Barthold, S.W.; Baumgarth, N. Delays and Diversions Mark the Development of B Cell Responses to Borrelia burgdorferi Infection. J. Immunol. 2012, 188, 5612–5622. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Sturrock, A.; Weis, J.J. Intracellular Localization of Borrelia burgdorferi within Human Endothelial Cells. Infect. Immun. 1991, 59, 671–678. [Google Scholar] [CrossRef]
- Montgomery, R.R.; Malawista, S.E. Entry of Borrelia burgdorferi into Macrophages Is End-on and Leads to Degradation in Lysosomes. Infect. Immun. 1996, 64, 2867–2872. [Google Scholar] [CrossRef]
- Klempner, M.S.; Noring, R.; Rogers, R.A. Invasion of Human Skin Fibroblasts by the Lyme Disease Spirochete, Borrelia burgdorferi. J. Infect. Dis. 1993, 167, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Meriläinen, L.; Herranen, A.; Schwarzbach, A.; Gilbert, L. Morphological and Biochemical Features of Borrelia burgdorferi Pleomorphic Forms. Microbiology 2015, 161, 516–527. [Google Scholar] [CrossRef]
- Vancová, M.; Rudenko, N.; Vaněček, J.; Golovchenko, M.; Strnad, M.; Rego, R.O.M.; Tichá, L.; Grubhoffer, L.; Nebesářová, J. Pleomorphism and Viability of the Lyme Disease Pathogen Borrelia burgdorferi Exposed to Physiological Stress Conditions: A Correlative Cryo-Fluorescence and Cryo-Scanning Electron Microscopy Study. Front. Microbiol. 2017, 8, 596. [Google Scholar] [CrossRef]
- Miklossy, J.; Kasas, S.; Zurn, A.D.; McCall, S.; Yu, S.; McGeer, P.L. Persisting Atypical and Cystic Forms of Borrelia burgdorferi and Local Inflammation in Lyme Neuroborreliosis. J. Neuroinflamm. 2008, 5, 40. [Google Scholar] [CrossRef] [PubMed]
- Brorson, Ø.; Brorson, S.-H.; Scythes, J.; MacAllister, J.; Wier, A.; Margulis, L. Destruction of Spirochete Borrelia burgdorferi Round-Body Propagules (RBs) by the Antibiotic Tigecycline. Proc. Natl. Acad. Sci. USA 2009, 106, 18656–18661. [Google Scholar] [CrossRef]
- Stevenson, B.; von Lackum, K.; Wattier, R.L.; McAlister, J.D.; Miller, J.C.; Babb, K. Quorum Sensing by the Lyme Disease Spirochete. Microbes Infect. 2003, 5, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Rudenko, N.; Golovchenko, M.; Kybicova, K.; Vancova, M. Metamorphoses of Lyme Disease Spirochetes: Phenomenon of Borrelia Persisters. Parasites Vectors 2019, 12, 237. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, E.G.; Cavallo, I.; Bordignon, V.; D’Agosto, G.; Pontone, M.; Trento, E.; Gallo, M.T.; Prignano, G.; Pimpinelli, F.; Toma, L.; et al. The Emerging Role of Microbial Biofilm in Lyme Neuroborreliosis. Front. Neurol. 2018, 9, 1048. [Google Scholar] [CrossRef]
- Hall-Stoodley, L.; Stoodley, P. Evolving Concepts in Biofilm Infections. Cell. Microbiol. 2009, 11, 1034–1043. [Google Scholar] [CrossRef]
- Lewis, K. Persister Cells, Dormancy and Infectious Disease. Nat. Rev. Microbiol. 2007, 5, 48–56. [Google Scholar] [CrossRef]
- Pothineni, V.R.; Wagh, D.; Babar, M.M.; Inayathullah, M.; Watts, R.E.; Kim, K.-M.; Parekh, M.B.; Gurjarpadhye, A.A.; Solow-Cordero, D.; Tayebi, L.; et al. Screening of NCI-DTP Library to Identify New Drug Candidates for Borrelia burgdorferi. J. Antibiot. 2017, 70, 308–312. [Google Scholar] [CrossRef]
- Horowitz, R.I.; Murali, K.; Gaur, G.; Freeman, P.R.; Sapi, E. Effect of Dapsone Alone and in Combination with Intracellular Antibiotics against the Biofilm Form of B. burgdorferi. BMC Res. Notes 2020, 13, 455. [Google Scholar] [CrossRef]
- Liegner, K.B. Disulfiram (Tetraethylthiuram Disulfide) in the Treatment of Lyme Disease and Babesiosis: Report of Experience in Three Cases. Antibiotics 2019, 8, 72. [Google Scholar] [CrossRef]
- Gao, J.; Gong, Z.; Montesano, D.; Glazer, E.; Liegner, K. “Repurposing” Disulfiram in the Treatment of Lyme Disease and Babesiosis: Retrospective Review of First 3 Years’ Experience in One Medical Practice. Antibiotics 2020, 9, 868. [Google Scholar] [CrossRef]
- Li, T.; Feng, J.; Xiao, S.; Shi, W.; Sullivan, D.; Zhang, Y. Identification of FDA-Approved Drugs with Activity against Stationary Phase Bartonella henselae. Antibiotics 2019, 8, 50. [Google Scholar] [CrossRef]
- Chomel, B.B.; Kasten, R.W.; Sykes, J.E.; Boulouis, H.-J.; Breitschwerdt, E.B. Clinical Impact of Persistent Bartonella Bacteremia in Humans and Animals. Ann. N. Y. Acad. Sci. 2003, 990, 267–278. [Google Scholar] [CrossRef]
- Breitschwerdt, E.B.; Maggi, R.G.; Duncan, A.W.; Nicholson, W.L.; Hegarty, B.C.; Woods, C.W. Bartonella Species in Blood of Immunocompetent Persons with Animal and Arthropod Contact. Emerg. Infect. Dis. 2007, 13, 938–941. [Google Scholar] [CrossRef]
- Zheng, X.; Ma, X.; Li, T.; Shi, W.; Zhang, Y. Effect of Different Drugs and Drug Combinations on Killing Stationary Phase and Biofilms Recovered Cells of Bartonella henselae in Vitro. BMC Microbiol. 2020, 20, 87. [Google Scholar] [CrossRef]
- Horowitz, R.I.; Freeman, P.R. Efficacy of Double-Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post-Treatment Lyme Disease Syndrome (PTLDS) and Associated Co-Infections: A Report of Three Cases and Retrospective Chart Review. Antibiotics 2020, 9, 725. [Google Scholar] [CrossRef]
- Horowitz, R.I.; Freeman, P.R. Efficacy of Short-Term High Dose Pulsed Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post-Treatment Lyme Disease Syndrome (PTLDS) and Associated Co-Infections: A Report of Three Cases and Literature Review. Antibiotics 2022, 11, 912. [Google Scholar] [CrossRef]
- Horowitz, R.I.; Freeman, P.R. The Use of Dapsone as a Novel “Persister” Drug in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome. J. Clin. Exp. Derm. Res. 2016, 7, 3. [Google Scholar] [CrossRef]
- Horowitz, R.I.; Freeman, P.R. Are Mycobacterium Drugs Effective for Treatment Resistant Lyme Disease, TickBorne Co-Infections, and Autoimmune Disease? JSM Arthritis 2016, 1, 1008. [Google Scholar]
- Bistas, E.; Sanghavi, D. Methylene Blue; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Feng, J.; Weitner, M.; Shi, W.; Zhang, S.; Sullivan, D.; Zhang, Y. Identification of Additional Anti-Persister Activity against Borrelia burgdorferi from an FDA Drug Library. Antibiotics 2015, 4, 397–410. [Google Scholar] [CrossRef]
- Feng, J.; Zhang, S.; Shi, W.; Zhang, Y. Activity of Sulfa Drugs and Their Combinations against Stationary Phase B. burgdorferi In Vitro. Antibiotics 2017, 6, 10. [Google Scholar] [CrossRef]
- Esbenshade, A.J.; Ho, R.H.; Shintani, A.; Zhao, Z.; Smith, L.-A.; Friedman, D.L. Dapsone-Induced Methemoglobinemia: A Dose-Related Occurrence? Cancer 2011, 117, 3485–3492. [Google Scholar] [CrossRef]
- Kurien, G.; Jamil, R.T.; Preuss, C.V. Dapsone; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kowal, K.; Weinstein, A. Western Blot Band Intensity Analysis. Application to the Diagnosis of Lyme Arthritis. Arthritis Rheum. 1994, 37, 1206–1211. [Google Scholar] [CrossRef]
- Branda, J.A.; Steere, A.C. Laboratory Diagnosis of Lyme Borreliosis. Clin. Microbiol. Rev. 2021, 34, e00018-19. [Google Scholar] [CrossRef]
- Kabir, H.; Lakshmanan, R.; Gopinath, S.; Bhonagiri, D. Dapsone-induced Methemoglobinemia—A Case Report. Clin. Case Rep. 2021, 9, e04054. [Google Scholar] [CrossRef]
- Farzam, K.; Tivakaran, V.S. QT Prolonging Drugs; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Horowitz, R.I.; Freeman, P.R.; Bruzzese, J. Efficacy of Glutathione Therapy in Relieving Dyspnea Associated with COVID-19 Pneumonia: A Report of 2 Cases. Respir. Med. Case Rep. 2020, 30, 101063. [Google Scholar] [CrossRef]
- Houghton, C.A.; Fassett, R.G.; Coombes, J.S. Sulforaphane and Other Nutrigenomic Nrf2 Activators: Can the Clinician’s Expectation Be Matched by the Reality? Oxid Med. Cell Longev. 2016, 2016, 7857186. [Google Scholar] [CrossRef]
- Moratilla-Rivera, I.; Sánchez, M.; Valdés-González, J.A.; Gómez-Serranillos, M.P. Natural Products as Modulators of Nrf2 Signaling Pathway in Neuroprotection. Int. J. Mol. Sci. 2023, 24, 3748. [Google Scholar] [CrossRef]
- Stratton, L.P.; Rudolph, A.S.; Knoll, W.K.; Bayne, S.; Farmer, M.C. The Reduction of Methemoglobin Levels by Antioxidants. Hemoglobin 1988, 12, 353–368. [Google Scholar] [CrossRef] [PubMed]
- Atyabi, N.; Yasini, S.P.; Jalali, S.M.; Shaygan, H. Antioxidant Effect of Different Vitamins on Methemoglobin Production: An in Vitro Study. Vet. Res. Forum 2012, 3, 97–101. [Google Scholar] [PubMed]
- Coleman, M.; Rhodes, L.; Scott, A.; Verbov, J.; Friedmann, P.; Breckenridge, A.; Park, B. The Use of Cimetidine to Reduce Dapsone-Dependent Methaemoglobinaemia in Dermatitis Herpetiformis Patients. Br. J. Clin. Pharmacol. 1992, 34, 244–249. [Google Scholar] [CrossRef]
- Coleman, M.; Scott, A.; Breckenridge, A.; Park, B. The Use of Cimetidine as a Selective Inhibitor of Dapsone N- Hydroxylation in Man. Br. J. Clin. Pharmacol. 1990, 30, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Gristan, Y.D.; Moosavi, L. Folinic Acid; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Mcfarland, L. Meta-Analysis of Probiotics for the Prevention of Antibiotic Associated Diarrhea and the Treatment of Clostridium Difficile Disease. Am. J. Gastroenterol. 2006, 101, 812–822. [Google Scholar] [CrossRef]
- Kopacz, K.; Phadtare, S. Probiotics for the Prevention of Antibiotic-Associated Diarrhea. Healthcare 2022, 10, 1450. [Google Scholar] [CrossRef]
- Gillman, P.K. CNS Toxicity Involving Methylene Blue: The Exemplar for Understanding and Predicting Drug Interactions That Precipitate Serotonin Toxicity. J. Psychopharmacol. 2011, 25, 429–436. [Google Scholar] [CrossRef]
- Edinoff, A.N.; Swinford, C.R.; Odisho, A.S.; Burroughs, C.R.; Stark, C.W.; Raslan, W.A.; Cornett, E.M.; Kaye, A.M.; Kaye, A.D. Clinically Relevant Drug Interactions with Monoamine Oxidase Inhibitors. Health Psychol. Res. 2000, 10, 39576. [Google Scholar] [CrossRef]
- Garcia, E.; Santos, C. Monoamine Oxidase Inhibitor Toxicity; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Mehta, P.; Leslie, S.W.; Reddivari, A.K.R. Dysuria; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Tran, A.T.; Rison, R.A.; Beydoun, S.R. Disulfiram Neuropathy: Two Case Reports. J. Med. Case Rep. 2016, 10, 72. [Google Scholar] [CrossRef] [PubMed]
- Butler, T. The Jarisch-Herxheimer Reaction after Antibiotic Treatment of Spirochetal Infections: A Review of Recent Cases and Our Understanding of Pathogenesis. Am. J. Trop. Med. Hyg. 2017, 96, 46–52. [Google Scholar] [CrossRef]
- Stokes, M.; Abdijadid, S. Disulfiram; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Shutter, M.C.; Akhondi, H. Tetracycline; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Theophilus, P.A.S.; Victoria, M.J.; Socarras, K.M.; Filush, K.R.; Gupta, K.; Luecke, D.F.; Sapi, E. Effectiveness of Stevia Rebaudiana Whole Leaf Extract Against the Various Morphological Forms of Borrelia burgdorferi in Vitro. Eur. J. Microbiol. Immunol. (Bp) 2015, 5, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Karvonen, K.; Gilbert, L. Effective Killing of Borrelia burgdorferi in Vitro with Novel Herbal Compounds. Gen. Med. Open 2018, 2, 1–4. [Google Scholar] [CrossRef]
- Feng, J.; Shi, W.; Miklossy, J.; Tauxe, G.M.; McMeniman, C.J.; Zhang, Y. Identification of Essential Oils with Strong Activity against Stationary Phase Borrelia burgdorferi. Antibiotics 2018, 7, 89. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, W.; Ali, Q.; Ahmed, S. Microscopic Visualization of the Antibiofilm Potential of Essential Oils against Staphylococcus aureus and Klebsiella pneumoniae. Microsc. Res. Tech. 2022, 85, 3921–3931. [Google Scholar] [CrossRef]
- Percival, S.L.; Salisbury, A.-M. The Efficacy of Tetrasodium EDTA on Biofilms. In Advances in Microbiology, Infectious Diseases and Public Health: Volume 9; Donelli, G., Ed.; Advances in Experimental Medicine and Biology; Springer International Publishing: Cham, Switzerland, 2018; pp. 101–110. ISBN 978-3-319-79017-6. [Google Scholar]
- Bruna, T.; Maldonado-Bravo, F.; Jara, P.; Caro, N. Silver Nanoparticles and Their Antibacterial Applications. Int. J. Mol. Sci. 2021, 22, 7202. [Google Scholar] [CrossRef] [PubMed]
- Krislee, A.; Fadly, C.; Nugrahaningsih, D.A.A.; Nuryastuti, T.; Nitbani, F.O.; Jumina; Sholikhah, E.N. The 1-Monolaurin Inhibit Growth and Eradicate the Biofilm Formed by Clinical Isolates of Staphylococcus epidermidis. BMC Proc. 2019, 13, 19. [Google Scholar] [CrossRef]
- Katsipis, G.; Pantazaki, A.A. Serrapeptase Impairs Biofilm, Wall, and Phospho-Homeostasis of Resistant and Susceptible Staphylococcus aureus. Appl. Microbiol. Biotechnol. 2023, 107, 1373–1389. [Google Scholar] [CrossRef]
- Goc, A.; Rath, M. The Anti-Borreliae Efficacy of Phytochemicals and Micronutrients: An Update. Adv. Infect. Dis. 2016, 3, 75–82. [Google Scholar] [CrossRef]
- Brorson, O.; Brorson, S. An in Vitro Study of the Susceptibility of Mobile and Cystic Forms of Borrelia burgdorferi to Hydroxychloroquine. Int. Microbiol. Off. J. Span. Soc. Microbiol. 2002, 5, 25–31. [Google Scholar] [CrossRef]
- Liu, F.; Hansra, S.; Crockford, G.; Köster, W.; Allan, B.J.; Blondeau, J.M.; Lainesse, C.; White, A.P. Tetrasodium EDTA Is Effective at Eradicating Biofilms Formed by Clinically Relevant Microorganisms from Patients’ Central Venous Catheters. mSphere 2018, 3, e00525-18. [Google Scholar] [CrossRef]
- Wu, G.; Lupton, J.R.; Turner, N.D.; Fang, Y.-Z.; Yang, S. Glutathione Metabolism and Its Implications for Health. J. Nutr. 2004, 134, 489–492. [Google Scholar] [CrossRef]
- Agrawal, S. Methylene Blue Dye|Uses & Side Effects; Macsen Labs: Udaipur, India, 2021. [Google Scholar]
- Griddine, A.; Bush, J.S. Ondansetron; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Krause, P.J.; Lepore, T.; Sikand, V.K.; Gadbaw, J.; Burke, G.; Telford, S.R.; Brassard, P.; Pearl, D.; Azlanzadeh, J.; Christianson, D.; et al. Atovaquone and Azithromycin for the Treatment of Babesiosis. N. Engl. J. Med. 2000, 343, 1454–1458. [Google Scholar] [CrossRef]
- Weiss, L.M. Babesiosis in Humans: A Treatment Review. Expert Opin. Pharmacother. 2002, 3, 1109–1115. [Google Scholar] [CrossRef]
- Vyas, J.M.; Telford, S.R.; Robbins, G.K. Treatment of Refractory Babesia microti Infection with Atovaquone-Proguanil in an HIV-Infected Patient: Case Report. Clin. Infect. Dis. 2007, 45, 1588–1590. [Google Scholar] [CrossRef]
- Marcos, L.A.; Leung, A.; Kirkman, L.; Wormser, G.P. Use of Tafenoquine to Treat a Patient with Relapsing Babesiosis with Clinical and Molecular Evidence of Resistance to Azithromycin and Atovaquone. IDCases 2022, 27, e01460. [Google Scholar] [CrossRef] [PubMed]
- Batiha, G.E.-S.; Beshbishy, A.M.; Tayebwa, D.S.; Adeyemi, O.S.; Yokoyama, N.; Igarashi, I. Evaluation of the Inhibitory Effect of Ivermectin on the Growth of Babesia and Theileria parasites in Vitro and in Vivo. Trop. Med. Health 2019, 47, 42. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, A.; Matsuu, A.; Matsuyama, K.; Hikasa, Y. The Efficacy of Artemisinin, Artemether, and Lumefantrine against Babesia Gibsoni in Vitro. Parasitol. Int. 2015, 64, 190–193. [Google Scholar] [CrossRef]
- Munkhjargal, T.; AbouLaila, M.; Terkawi, M.A.; Sivakumar, T.; Ichikawa, M.; Davaasuren, B.; Nyamjargal, T.; Yokoyama, N.; Igarashi, I. Inhibitory Effects of Pepstatin A and Mefloquine on the Growth of Babesia Parasites. Am. J. Trop. Med. Hyg. 2012, 87, 681–688. [Google Scholar] [CrossRef]
- Puri, B.K.; Hakkarainen-Smith, J.S.; Monro, J.A. The Effect of Artesunate on Short-Term Memory in Lyme Borreliosis. Med. Hypotheses 2017, 105, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Batiha, G.E.-S.; Beshbishy, A.M.; Alkazmi, L.M.; Nadwa, E.H.; Rashwan, E.K.; Yokoyama, N.; Igarashi, I. In Vitro and in Vivo Growth Inhibitory Activities of Cryptolepine Hydrate against Several Babesia Species and Theileria equi. PLoS Negl. Trop. Dis. 2020, 14, e0008489. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Alvarez-Manzo, H.; Leone, J.; Schweig, S.; Zhang, Y. Botanical Medicines Cryptolepis sanguinolenta, Artemisia annua, Scutellaria baicalensis, Polygonum cuspidatum, and Alchornea cordifolia Demonstrate Inhibitory Activity against Babesia duncani. Front. Cell Infect. Microbiol. 2021, 11, 624745. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Shapiro, M.; Janicki, S.; Mankoff, J.; Stricker, R.B. Does Biological Sex Matter in Lyme Disease? The Need for Sex-Disaggregated Data in Persistent Illness. IJGM 2023, 16, 2557–2571. [Google Scholar] [CrossRef]
- Scheckelhoff, M.R.; Telford, S.R.; Wesley, M.; Hu, L.T. Borrelia burgdorferi Intercepts Host Hormonal Signals to Regulate Expression of Outer Surface Protein A. Proc. Natl. Acad. Sci. USA 2007, 104, 7247–7252. [Google Scholar] [CrossRef]
- Tjernberg, I.; Carlsson, M.; Ernerudh, J.; Eliasson, I.; Forsberg, P. Mapping of Hormones and Cortisol Responses in Patients after Lyme Neuroborreliosis. BMC Infect. Dis. 2010, 10, 20. [Google Scholar] [CrossRef] [PubMed]
- Wiffen, P.J.; Derry, S.; Bell, R.F.; Rice, A.S.; Tölle, T.R.; Phillips, T.; Moore, R.A. Gabapentin for Chronic Neuropathic Pain in Adults. Cochrane Database Syst. Rev. 2017, 6, CD007938. [Google Scholar] [CrossRef]
- Moore, R.A.; Derry, S.; Aldington, D.; Cole, P.; Wiffen, P.J. Amitriptyline for Neuropathic Pain in Adults. Cochrane Database Syst. Rev. 2015, 2015, CD008242. [Google Scholar] [CrossRef]
- Derry, S.; Bell, R.F.; Straube, S.; Wiffen, P.J.; Aldington, D.; Moore, R.A. Pregabalin for Neuropathic Pain in Adults. Cochrane Database Syst. Rev. 2019, 2019, CD007076. [Google Scholar] [CrossRef]
- Duloxetine for Treating Painful Neuropathy, Chronic Pain or Fibromyalgia. Available online: https://www.cochrane.org/CD007115/NEUROMUSC_duloxetine-treating-painful-neuropathy-chronic-pain-or-fibromyalgia (accessed on 23 June 2023).
- Freitas, J.; Santos, R.; Azevedo, E.; Costa, O.; Carvalho, M.; de Freitas, A.F. Clinical Improvement in Patients with Orthostatic Intolerance after Treatment with Bisoprolol and Fludrocortisone. Clin. Auton. Res. 2000, 10, 293–299. [Google Scholar] [CrossRef]
- Ross, A.J.; Ocon, A.J.; Medow, M.S.; Stewart, J.M. A Double-Blind Placebo-Controlled Cross-over Study of the Vascular Effects of Midodrine in Neuropathic Compared with Hyperadrenergic Postural Tachycardia Syndrome. Clin. Sci. 2014, 126, 289–296. [Google Scholar] [CrossRef]
- Ruzieh, M.; Dasa, O.; Pacenta, A.; Karabin, B.; Grubb, B. Droxidopa in the Treatment of Postural Orthostatic Tachycardia Syndrome. Am. J. 2017, 24, e157–e161. [Google Scholar] [CrossRef]
- Deng, X.; Zhang, Y.; Liao, Y.; Du, J. Efficacy of β-Blockers on Postural Tachycardia Syndrome in Children and Adolescents: A Systematic Review and Meta-Analysis. Front. Pediatr. 2019, 7, 460. [Google Scholar] [CrossRef]
- Tahir, F.; Bin Arif, T.; Majid, Z.; Ahmed, J.; Khalid, M. Ivabradine in Postural Orthostatic Tachycardia Syndrome: A Review of the Literature. Cureus 2020, 12, e7868. [Google Scholar] [CrossRef] [PubMed]
- Maurin, M. Francisella Tularensis, Tularemia and Serological Diagnosis. Front. Cell Infect. Microbiol. 2020, 10, 512090. [Google Scholar] [CrossRef] [PubMed]
- Corbel, M.J.; Stuart, F.A.; Brewer, R.A. Observations on Serological Cross-Reactions between Smooth Brucella Species and Organisms of Other Genera. Dev. Biol. Stand. 1984, 56, 341–348. [Google Scholar]
- Gatti, G.; Merighi, M.; Hossein, J.; Travaini, S.; Casazza, R.; Karlsson, M.; Cruciani, M.; Bassetti, D. Population Pharmacokinetics of Dapsone Administered Biweekly to Human Immunodeficiency Virus-Infected Patients. Antimicrob. Agents Chemother. 1996, 40, 2743–2748. [Google Scholar] [CrossRef] [PubMed]
- Burke, P.; Jahangir, K.; Kolber, M.R. Dapsone-Induced Methemoglobinemia. Can. Fam. Physician 2013, 59, 958–961. [Google Scholar] [PubMed]
- Rehman, H.U. Methemoglobinemia. West. J. Med. 2001, 175, 193–196. [Google Scholar] [CrossRef]
- Billett, H.H. Hemoglobin and Hematocrit. In Clinical Methods: The History, Physical, and Laboratory Examinations; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, UK, 1990; ISBN 978-0-409-90077-4. [Google Scholar]
- Maner, B.S.; Moosavi, L. Mean Corpuscular Volume; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Seydel, J.K.; Richter, M.; Wempe, E. Mechanism of Action of the Folate Blocker Diaminodiphenylsulfone (Dapsone, DDS) Studied in E. Coli Cell-Free Enzyme Extracts in Comparison to Sulfonamides (SA). Int. J. Lepr. Other Mycobact. Dis. 1980, 48, 18–29. [Google Scholar]
- Khalid, F.; Mahendraker, N.; Tonismae, T. HELLP Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Chandler, C.M.; Reid, M.C.; Cherian, S.; Sabath, D.E.; Edlefsen, K.L. Comparison of Blood Counts and Markers of Inflammation and Coagulation in Patients with and without COVID-19 Presenting to the Emergency Department in Seattle, WA. Am. J. Clin. Pathol. 2021, 156, 185–197. [Google Scholar] [CrossRef]
- Tishkowski, K.; Gupta, V. Erythrocyte Sedimentation Rate; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Nehring, S.M.; Goyal, A.; Patel, B.C. C Reactive Protein; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Jinna, S.; Khandhar, P.B. Thrombocytopenia; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Al-Gwaiz, L.A.; Babay, H.H. The Diagnostic Value of Absolute Neutrophil Count, Band Count and Morphologic Changes of Neutrophils in Predicting Bacterial Infections. Med. Princ. Pract. 2007, 16, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Tahir, N.; Zahra, F. Neutrophilia; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Honda, T.; Uehara, T.; Matsumoto, G.; Arai, S.; Sugano, M. Neutrophil Left Shift and White Blood Cell Count as Markers of Bacterial Infection. Clin. Chim. Acta 2016, 457, 46–53. [Google Scholar] [CrossRef]
- Lowe, D.; Sanvictores, T.; Zubair, M.; John, S. Alkaline Phosphatase; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Lala, V.; Zubair, M.; Minter, D.A. Liver Function Tests; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Riancho, J.A. Diagnostic Approach to Patients with Low Serum Alkaline Phosphatase. Calcif. Tissue Int. 2023, 112, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Thoguluva Chandrasekar, V.; Faust, T.W.; John, S. Gilbert Syndrome; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Ahmed, Z.; Ur Rehman, A.; Awais, A.; Hanan, A.; Ahmad, S. Lyme Disease and Severe Hyperbilirubinemia: A Rare Presentation of Lyme Disease. Cureus 2020, 12, e8363. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Wilcox, S.; Mankoff, J.; Stricker, R.B. Severity of Chronic Lyme Disease Compared to Other Chronic Conditions: A Quality of Life Survey. PeerJ 2014, 2, e322. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and Risk Factors for Long COVID in Non-Hospitalized Adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- Garg, M.; Maralakunte, M.; Garg, S.; Dhooria, S.; Sehgal, I.; Bhalla, A.S.; Vijayvergiya, R.; Grover, S.; Bhatia, V.; Jagia, P.; et al. The Conundrum of ‘Long-COVID-19ʹ: A Narrative Review. Int. J. Gen. Med. 2021, 14, 2491–2506. [Google Scholar] [CrossRef]
- Kobusiak-Prokopowicz, M.; Fułek, K.; Fułek, M.; Kaaz, K.; Mysiak, A.; Kurpas, D.; Beszłej, J.A.; Brzecka, A.; Leszek, J. Cardiovascular, Pulmonary, and Neuropsychiatric Short- and Long-Term Complications of COVID-19. Cells 2022, 11, 3882. [Google Scholar] [CrossRef]
- Citera, M.; Freeman, P.R.; Horowitz, R.I. Empirical Validation of the Horowitz Multiple Systemic Infectious Disease Syndrome Questionnaire for Suspected Lyme Disease. Int. J. Gen. Med. 2017, 10, 249–273. [Google Scholar] [CrossRef]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Paxlovid in Reducing Severe Coronavirus Disease 2019 and Mortality in High-Risk Patients. Clin. Infect. Dis. 2023, 76, e342–e349. [Google Scholar] [CrossRef]
- Cameron, D.J.; McWhinney, S.R. Consequences of Contracting COVID-19 or Taking the COVID-19 Vaccine for Individuals with a History of Lyme Disease. Antibiotics 2023, 12, 493. [Google Scholar] [CrossRef] [PubMed]
- Farouk, A.; Salman, S. Dapsone and Doxycycline Could Be Potential Treatment Modalities for COVID-19. Med. Hypotheses 2020, 140, 109768. [Google Scholar] [CrossRef] [PubMed]
- Debol, S.M.; Herron, M.J.; Nelson, R.D. Anti-Inflammatory Action of Dapsone: Inhibition of Neutrophil Adherence Is Associated with Inhibition of Chemoattractant-Induced Signal Transduction. J. Leukoc. Biol. 1997, 62, 827–836. [Google Scholar] [CrossRef]
- Al-kuraishy, H.M.; Al-Gareeb, A.I.; Elekhnawy, E.; Alexiou, A.; Batiha, G.E. The Potential Effect of Dapsone on the Inflammatory Reactions in COVID-19: Staggering View. Comb. Chem. High. Throughput Screen. 2023, 26, 1–5. [Google Scholar]
- Kanwar, B.; Lee, C.J.; Lee, J.-H. Specific Treatment Exists for SARS-CoV-2 ARDS. Vaccines 2021, 9, 635. [Google Scholar] [CrossRef]
- Kanwar, B.A.; Khattak, A.; Balentine, J.; Lee, J.H.; Kast, R.E. Benefits of Using Dapsone in Patients Hospitalized with COVID-19. Vaccines 2022, 10, 195. [Google Scholar] [CrossRef]
- Rhodes, L.E.; Tingle, M.D.; Park, B.K.; Chu, P.; Verbov, J.L.; Friedmann, P.S. Cimetidine Improves the Therapeutic/Toxic Ratio of Dapsone in Patients on Chronic Dapsone Therapy. Br. J. Derm. 1995, 132, 257–262. [Google Scholar] [CrossRef]
- Lee, J.H.; Kanwar, B.; Lee, C.J.; Sergi, C.; Coleman, M.D. Dapsone Is an Anticatalysis for Alzheimer’s Disease Exacerbation. iScience 2022, 25, 104274. [Google Scholar] [CrossRef] [PubMed]
- Miklossy, J.; Khalili, K.; Gern, L.; Ericson, R.L.; Darekar, P.; Bolle, L.; Hurlimann, J.; Paster, B.J. Borrelia burgdorferi Persists in the Brain in Chronic Lyme Neuroborreliosis and May Be Associated with Alzheimer Disease. J. Alzheimers Dis. 2004, 6, 639–649, discussion 673–681. [Google Scholar] [CrossRef]
- Miklossy, J. Chronic Inflammation and Amyloidogenesis in Alzheimer’s Disease—Role of Spirochetes. J. Alzheimers Dis. 2008, 13, 381–391. [Google Scholar] [CrossRef]
- Miklossy, J. Chronic or Late Lyme Neuroborreliosis: Analysis of Evidence Compared to Chronic or Late Neurosyphilis. Open Neurol. J. 2012, 6, 146–157. [Google Scholar] [CrossRef]
- Kristoferitsch, W.; Aboulenein-Djamshidian, F.; Jecel, J.; Rauschka, H.; Rainer, M.; Stanek, G.; Fischer, P. Secondary Dementia Due to Lyme Neuroborreliosis. Wien. Klin. Wochenschr. 2018, 130, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Senejani, A.G.; Maghsoudlou, J.; El-Zohiry, D.; Gaur, G.; Wawrzeniak, K.; Caravaglia, C.; Khatri, V.A.; MacDonald, A.; Sapi, E. Borrelia burgdorferi Co-Localizing with Amyloid Markers in Alzheimer’s Disease Brain Tissues. J. Alzheimers Dis. 2022, 85, 889–903. [Google Scholar] [CrossRef]
- Buonsenso, D.; Piazza, M.; Boner, A.L.; Bellanti, J.A. Long COVID: A Proposed Hypothesis-Driven Model of Viral Persistence for the Pathophysiology of the Syndrome. Allergy Asthma Proc. 2022, 43, 187–193. [Google Scholar] [CrossRef]
- Chen, B.; Julg, B.; Mohandas, S.; Bradfute, S.B. RECOVER Mechanistic Pathways Task Force Viral Persistence, Reactivation, and Mechanisms of Long COVID. eLife 2023, 12, e86015. [Google Scholar] [CrossRef]
- Rojas, M.; Rodríguez, Y.; Acosta-Ampudia, Y.; Monsalve, D.M.; Zhu, C.; Li, Q.-Z.; Ramírez-Santana, C.; Anaya, J.-M. Autoimmunity Is a Hallmark of Post-COVID Syndrome. J. Transl. Med. 2022, 20, 129. [Google Scholar] [CrossRef]
- Pozzi, A. COVID-19 and Mitochondrial Non-Coding RNAs: New Insights from Published Data. Front. Physiol. 2021, 12, 805005. [Google Scholar] [CrossRef] [PubMed]
- Nunn, A.V.W.; Guy, G.W.; Brysch, W.; Bell, J.D. Understanding Long COVID; Mitochondrial Health and Adaptation-Old Pathways, New Problems. Biomedicines 2022, 10, 3113. [Google Scholar] [CrossRef]
- Raj, S.R.; Arnold, A.C.; Barboi, A.; Claydon, V.E.; Limberg, J.K.; Lucci, V.-E.M.; Numan, M.; Peltier, A.; Snapper, H.; Vernino, S.; et al. Long-COVID Postural Tachycardia Syndrome: An American Autonomic Society Statement. Clin. Auton. Res. 2021, 31, 365–368. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major Findings, Mechanisms and Recommendations. Nat. Rev. Microbiol. 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Mohandas, S.; Jagannathan, P.; Henrich, T.J.; Sherif, Z.A.; Bime, C.; Quinlan, E.; Portman, M.A.; Gennaro, M.; Rehman, J. RECOVER Mechanistic Pathways Task Force Immune Mechanisms Underlying COVID-19 Pathology and Post-Acute Sequelae of SARS-CoV-2 Infection (PASC). eLife 2023, 12, e86014. [Google Scholar] [CrossRef] [PubMed]
- Caskey, J.R.; Embers, M.E. Persister Development by Borrelia burgdorferi Populations In Vitro. Antimicrob. Agents Chemother. 2015, 59, 6288–6295. [Google Scholar] [CrossRef] [PubMed]
- Cabello, F.C.; Embers, M.E.; Newman, S.A.; Godfrey, H.P. Borreliella Burgdorferi Antimicrobial-Tolerant Persistence in Lyme Disease and Posttreatment Lyme Disease Syndromes. mBio 2022, 13, e0344021. [Google Scholar] [CrossRef] [PubMed]
- Gindl, A.; Schötta, A.; Berent, S.; Markowicz, M.; Stockinger, H.; Thalhammer, F.; Stary, G.; Strobl, J. Persistent Lyme Disease with Cutaneous Borrelia Biofilm Formation. Br. J. Derm. 2022, 186, 1041–1043. [Google Scholar] [CrossRef] [PubMed]
- Preac-Mursic, V.; Weber, K.; Pfister, H.W.; Wilske, B.; Gross, B.; Baumann, A.; Prokop, J. Survival of Borrelia burgdorferi in Antibiotically Treated Patients with Lyme Borreliosis. Infection 1989, 17, 355–359. [Google Scholar] [CrossRef]
- Bayer, M.E.; Zhang, L.; Bayer, M.H. Borrelia burgdorferi DNA in the Urine of Treated Patients with Chronic Lyme Disease Symptoms. A PCR Study of 97 Cases. Infection 1996, 24, 347–353. [Google Scholar] [CrossRef]
- Donta, S.T. Tetracycline Therapy for Chronic Lyme Disease. Clin. Infect. Dis. 1997, 25 (Suppl. S1), S52–S56. [Google Scholar] [CrossRef]
- Bradley, J.F.; Johnson, R.C.; Goodman, J.L. The Persistence of Spirochetal Nucleic Acids in Active Lyme Arthritis. Ann. Intern. Med. 1994, 120, 487–489. [Google Scholar] [CrossRef]
- Battafarano, D.F.; Combs, J.A.; Enzenauer, R.J.; Fitzpatrick, J.E. Chronic Septic Arthritis Caused by Borrelia burgdorferi. Clin. Orthop Relat Res. 1993, 297, 238–241. [Google Scholar] [CrossRef]
- Häupl, T.; Hahn, G.; Rittig, M.; Krause, A.; Schoerner, C.; Schönherr, U.; Kalden, J.R.; Burmester, G.R. Persistence of Borrelia burgdorferi in Ligamentous Tissue from a Patient with Chronic Lyme Borreliosis. Arthritis. Rheum. 1993, 36, 1621–1626. [Google Scholar] [CrossRef]
- Fraser, D.D.; Kong, L.I.; Miller, F.W. Molecular Detection of Persistent Borrelia burgdorferi in a Man with Dermatomyositis. Clin. Exp. Rheumatol. 1992, 10, 387–390. [Google Scholar]
- Aberer, E.; Koszik, F.; Silberer, M. Why Is Chronic Lyme Borreliosis Chronic? Clin. Infect. Dis. 1997, 25 (Suppl. S1), S64–S70. [Google Scholar] [CrossRef] [PubMed]
- Karma, A.; Stenborg, T.; Summanen, P.; Immonen, I.; Mikkilä, H.; Seppälä, I. Long-Term Follow-up of Chronic Lyme Neuroretinitis. Retina 1996, 16, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Keller, T.L.; Halperin, J.J.; Whitman, M. PCR Detection of Borrelia burgdorferi DNA in Cerebrospinal Fluid of Lyme Neuroborreliosis Patients. Neurology 1992, 42, 32–42. [Google Scholar] [CrossRef]
- Diringer, M.N.; Halperin, J.J.; Dattwyler, R.J. Lyme Meningoencephalitis: Report of a Severe, Penicillin-Resistant Case. Arthritis. Rheum. 1987, 30, 705–708. [Google Scholar] [PubMed]
- Preac Mursic, V.; Patsouris, E.; Wilske, B.; Reinhardt, S.; Gross, B.; Mehraein, P. Persistence of Borrelia burgdorferi and Histopathological Alterations in Experimentally Infected Animals. A Comparison with Histopathological Findings in Human Lyme Disease. Infection 1990, 18, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Straubinger, R.K. PCR-Based Quantification of Borrelia burgdorferi Organisms in Canine Tissues over a 500-Day Postinfection Period. J. Clin. Microbiol. 2000, 38, 2191–2199. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-F.; Ku, Y.-W.; Chang, C.-F.; Chang, C.-D.; McDonough, S.P.; Divers, T.; Pough, M.; Torres, A. Antibiotic Treatment of Experimentally Borrelia burgdorferi-Infected Ponies. Vet. Microbiol. 2005, 107, 285–294. [Google Scholar] [CrossRef]
- Embers, M.E.; Hasenkampf, N.R.; Jacobs, M.B.; Tardo, A.C.; Doyle-Meyers, L.A.; Philipp, M.T.; Hodzic, E. Variable Manifestations, Diverse Seroreactivity and Post-Treatment Persistence in Non-Human Primates Exposed to Borrelia burgdorferi by Tick Feeding. PLoS ONE 2017, 12, e0189071. [Google Scholar] [CrossRef]
- Marques, A.; Telford, S.R.; Turk, S.-P.; Chung, E.; Williams, C.; Dardick, K.; Krause, P.J.; Brandeburg, C.; Crowder, C.D.; Carolan, H.E.; et al. Xenodiagnosis to Detect Borrelia burgdorferi Infection: A First-in-Human Study. Clin. Infect. Dis. 2014, 58, 937–945. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Manzo, H.S.; Zhang, Y.; Shi, W.; Zhang, Y. Evaluation of Disulfiram Drug Combinations and Identification of Other More Effective Combinations against Stationary Phase Borrelia burgdorferi. Antibiotics 2020, 9, 542. [Google Scholar] [CrossRef] [PubMed]
- Alruwaili, Y.; Jacobs, M.B.; Hasenkampf, N.R.; Tardo, A.C.; McDaniel, C.E.; Embers, M.E. Superior Efficacy of Combination Antibiotic Therapy versus Monotherapy in a Mouse Model of Lyme Disease. bioRxiv 2023. [Google Scholar] [CrossRef]
- Okaro, U.; Addisu, A.; Casanas, B.; Anderson, B. Bartonella Species, an Emerging Cause of Blood-Culture-Negative Endocarditis. Clin. Microbiol. Rev. 2017, 30, 709–746. [Google Scholar] [CrossRef]
- Okaro, U.; Green, R.; Mohapatra, S.; Anderson, B. The Trimeric Autotransporter Adhesin BadA Is Required for in Vitro Biofilm Formation by Bartonella henselae. NPJ Biofilms Microbiomes 2019, 5, 10. [Google Scholar] [CrossRef]
- Tucker, D.; Lu, Y.; Zhang, Q. From Mitochondrial Function to Neuroprotection—An Emerging Role for Methylene Blue. Mol. Neurobiol. 2018, 55, 5137–5153. [Google Scholar] [CrossRef]
- Zhang, Y. Persisters, Persistent Infections and the Yin–Yang Model. Emerg. Microbes Infect. 2014, 3, e3. [Google Scholar] [CrossRef]
- Dhanya, N.B.; Rai, R.; Srinivas, C.R. Histamine 2 Blocker Potentiates the Effects of Histamine 1 Blocker in Suppressing Histamine-Induced Wheal. Indian J. Derm. Venereol. Leprol. 2008, 74, 475–477. [Google Scholar] [CrossRef]
- Wozel, G.; Blasum, C. Dapsone in Dermatology and Beyond. Arch. Derm. Res. 2014, 306, 103–124. [Google Scholar] [CrossRef] [PubMed]
- Piette, E.W.; Werth, V.P. Dapsone in the Management of the Autoimmune Bullous Diseases. Derm. Clin. 2011, 29, 561–564. [Google Scholar] [CrossRef]
- Liang, S.E.; Hoffmann, R.; Peterson, E.; Soter, N.A. Use of Dapsone in the Treatment of Chronic Idiopathic and Autoimmune Urticaria. JAMA Derm. 2019, 155, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Rabah, H.; Chukkalore, D.; El-Charabaty, E.; Mobarakai, N. Babesiosis and the Human Immune System. IDCases 2021, 27, e01368. [Google Scholar] [CrossRef]
- Djokic, V.; Primus, S.; Akoolo, L.; Chakraborti, M.; Parveen, N. Age-Related Differential Stimulation of Immune Response by Babesia microti and Borrelia burgdorferi during Acute Phase of Infection Affects Disease Severity. Front. Immunol. 2018, 9, 2891. [Google Scholar] [CrossRef] [PubMed]
- Mozayeni, B.R.; Maggi, R.G.; Bradley, J.M.; Breitschwerdt, E.B. Rheumatological Presentation of Bartonella koehlerae and Bartonella henselae Bacteremias: A Case Report. Medicine 2018, 97, e0465. [Google Scholar] [CrossRef] [PubMed]
- Maggi, R.G.; Mozayeni, B.R.; Pultorak, E.L.; Hegarty, B.C.; Bradley, J.M.; Correa, M.; Breitschwerdt, E.B. Bartonella spp. Bacteremia and Rheumatic Symptoms in Patients from Lyme Disease–Endemic Region. Emerg. Infect. Dis. 2012, 18, 783–791. [Google Scholar] [CrossRef]
- Mada, P.K.; Zulfiqar, H.; Joel Chandranesan, A.S. Bartonellosis; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Beydon, M.; Rodriguez, C.; Karras, A.; Cez, A.; Rafat, C.; Jourde-Chiche, N.; Fain, O.; Philipponnet, C.; Puéchal, X.; Dossier, A.; et al. Bartonella and Coxiella Infections Presenting as Systemic Vasculitis: Case Series and Review of Literature. Rheumatology 2022, 61, 2609–2618. [Google Scholar] [CrossRef]
- Iannace, C.; Lo Conte, D.; Di Libero, L.; Varricchio, A.; Testa, A.; Vigorito, R.; Gagliardi, G.; Lepore, M.; Caracciolo, F. Cat Scratch Disease Presenting as Breast Cancer: A Report of an Unusual Case. Case Rep. Oncol. Med. 2013, 2013, 507504. [Google Scholar] [CrossRef]
- Marques, L.C.; Pincerato, K.; Yoshimura, A.A.; Andrade, F.E.M.; Barros, A.C.S.D.D. Cat Scratch Disease Presenting as Axillary Lymphadenopathy and a Palpable Benign Mammary Nodule Mimicking a Carcinoma. Rev. Soc. Bras. Med. Trop. 2018, 51, 247–248. [Google Scholar] [CrossRef]
- Markaki, S.; Sotiropoulou, M.; Papaspirou, P.; Lazaris, D. Cat-Scratch Disease Presenting as a Solitary Tumour in the Breast: Report of Three Cases. Eur. J. Obs. Gynecol. Reprod. Biol. 2003, 106, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Ericson, M.E.; Breitschwerdt, E.B.; Reicherter, P.; Maxwell, C.; Maggi, R.G.; Melvin, R.G.; Maluki, A.H.; Bradley, J.M.; Miller, J.C.; Simmons, G.E.; et al. Bartonella henselae Detected in Malignant Melanoma, a Preliminary Study. Pathogens 2021, 10, 326. [Google Scholar] [CrossRef]
- Breitschwerdt, E.B.; Bradley, J.M.; Maggi, R.G.; Lashnits, E.; Reicherter, P. Bartonella Associated Cutaneous Lesions (BACL) in People with Neuropsychiatric Symptoms. Pathogens 2020, 9, 1023. [Google Scholar] [CrossRef]
- Lins, K.D.A.; Drummond, M.R.; Velho, P.E.N.F. Cutaneous Manifestations of Bartonellosis. An. Bras. Derm. 2019, 94, 594–602. [Google Scholar] [CrossRef]
- Mosepele, M.; Mazo, D.; Cohn, J. Bartonella Infection in Immunocompromised Hosts: Immunology of Vascular Infection and Vasoproliferation. Clin. Dev. Immunol. 2012, 2012, 612809. [Google Scholar] [CrossRef]
- Parker, A.R.; Skold, M.; Ramsden, D.B.; Ocejo-Vinyals, J.G.; López-Hoyos, M.; Harding, S. The Clinical Utility of Measuring IgG Subclass Immunoglobulins during Immunological Investigation for Suspected Primary Antibody Deficiencies. Lab. Med. 2017, 48, 314–325. [Google Scholar] [CrossRef] [PubMed]
- Woldehiwet, Z. Immune Evasion and Immunosuppression by Anaplasma Phagocytophilum, the Causative Agent of Tick-Borne Fever of Ruminants and Human Granulocytic Anaplasmosis. Vet. J. 2008, 175, 37–44. [Google Scholar] [CrossRef]
- Homer, M.J.; Aguilar-Delfin, I.; Telford, S.R.; Krause, P.J.; Persing, D.H. Babesiosis. Clin. Microbiol. Rev. 2000, 13, 451–469. [Google Scholar] [CrossRef]
- Schlam, D.; Canton, J.; Carreño, M.; Kopinski, H.; Freeman, S.A.; Grinstein, S.; Fairn, G.D. Gliotoxin Suppresses Macrophage Immune Function by Subverting Phosphatidylinositol 3,4,5-Trisphosphate Homeostasis. mBio 2016, 7, e02242. [Google Scholar] [CrossRef]
- Hansmann, Y.; DeMartino, S.; Piémont, Y.; Meyer, N.; Mariet, P.; Heller, R.; Christmann, D.; Jaulhac, B. Diagnosis of Cat Scratch Disease with Detection of Bartonella henselae by PCR: A Study of Patients with Lymph Node Enlargement. J. Clin. Microbiol. 2005, 43, 3800–3806. [Google Scholar] [CrossRef] [PubMed]
- Vesty, A.; Henderson, G.; Blakiston, M.; Chhibber, A.V.; Fox-Lewis, A.; Roberts, S.; Basu, I. Evaluation of SsrA-Targeted Real Time PCR for the Detection of Bartonella Species in Human Clinical Samples and Reflex Sequencing for Species-Level Identification. Pathology 2022, 54, 449–452. [Google Scholar] [CrossRef]
- Shapira, L.; Rasis, M.; Binsky Ehrenreich, I.; Maor, Y.; Katchman, E.A.; Treves, A.; Velan, A.; Halutz, O.; Graidy-Varon, M.; Leibovitch, C.; et al. Laboratory Diagnosis of 37 Cases of Bartonella Endocarditis Based on Enzyme Immunoassay and Real-Time PCR. J. Clin. Microbiol. 2021, 59, e02217-20. [Google Scholar] [CrossRef]
- Maggi, R.G.; Richardson, T.; Breitschwerdt, E.B.; Miller, J.C. Development and Validation of a Droplet Digital PCR Assay for the Detection and Quantification of Bartonella Species within Human Clinical Samples. J. Microbiol. Methods 2020, 176, 106022. [Google Scholar] [CrossRef]
- Mallqui, V.; Speelmon, E.C.; Verástegui, M.; Maguiña-Vargas, C.; Pinell-Salles, P.; Lavarello, R.; Delgado, J.; Kosek, M.; Romero, S.; Arana, Y.; et al. Sonicated Diagnostic Immunoblot for Bartonellosis. Clin. Diagn. Lab. Immunol. 2000, 7, 1–5. [Google Scholar] [CrossRef]
- Middelveen, M.J.; Cruz, I.D.; Fesler, M.C.; Stricker, R.B.; Shah, J.S. Detection of Tick-Borne Infection in Morgellons Disease Patients by Serological and Molecular Techniques. Clin. Cosmet. Investig. Derm. 2018, 11, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Kempf, V.A.; Volkmann, B.; Schaller, M.; Sander, C.A.; Alitalo, K.; Riess, T.; Autenrieth, I.B. Evidence of a Leading Role for VEGF in Bartonella henselae-Induced Endothelial Cell Proliferations. Cell Microbiol. 2001, 3, 623–632. [Google Scholar] [CrossRef]
- Breitschwerdt, E.B. Bartonellosis: One Health Perspectives for an Emerging Infectious Disease. ILAR J. 2014, 55, 46–58. [Google Scholar] [CrossRef]
- Reis, C.; Cote, M.; Le Rhun, D.; Lecuelle, B.; Levin, M.L.; Vayssier-Taussat, M.; Bonnet, S.I. Vector Competence of the Tick Ixodes ricinus for Transmission of Bartonella birtlesii. PLoS Negl. Trop. Dis. 2011, 5, e1186. [Google Scholar] [CrossRef] [PubMed]
- Müller, A.; Reiter, M.; Schötta, A.M.; Stockinger, H.; Stanek, G. Detection of Bartonella spp. in Ixodes ricinus Ticks and Bartonella seroprevalence in Human Populations. Ticks Tick Borne Dis. 2016, 7, 763–767. [Google Scholar] [CrossRef]
- Król, N.; Militzer, N.; Stöbe, E.; Nijhof, A.M.; Pfeffer, M.M.; Kempf, V.A.J.; Obiegala, A. Evaluating Transmission Paths for Three Different Bartonella spp. in Ixodes ricinus Ticks Using Artificial Feeding. Microorganisms 2021, 9, 901. [Google Scholar] [CrossRef]
- Chang, C.C.; Chomel, B.B.; Kasten, R.W.; Romano, V.; Tietze, N. Molecular Evidence of Bartonella spp. in Questing Adult Ixodes pacificus Ticks in California. J. Clin. Microbiol. 2001, 39, 1221–1226. [Google Scholar] [CrossRef]
- Maggi, R.G.; Toliver, M.; Richardson, T.; Mather, T.; Breitschwerdt, E.B. Regional Prevalences of Borrelia burgdorferi, Borrelia bissettiae, and Bartonella henselae in Ixodes affinis, Ixodes pacificus and Ixodes scapularis in the USA. Ticks Tick Borne Dis. 2019, 10, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L.; Shapiro, M.; Mankoff, J. Removing the Mask of Average Treatment Effects in Chronic Lyme Disease Research Using Big Data and Subgroup Analysis. Healthcare 2018, 6, 124. [Google Scholar] [CrossRef] [PubMed]
- Onyiche, T.E.; Răileanu, C.; Fischer, S.; Silaghi, C. Global Distribution of Babesia Species in Questing Ticks: A Systematic Review and Meta-Analysis Based on Published Literature. Pathogens 2021, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Bloch, E.M.; Krause, P.J.; Tonnetti, L. Preventing Transfusion-Transmitted Babesiosis. Pathogens 2021, 10, 1176. [Google Scholar] [CrossRef]
- Saetre, K.; Godhwani, N.; Maria, M.; Patel, D.; Wang, G.; Li, K.I.; Wormser, G.P.; Nolan, S.M. Congenital Babesiosis after Maternal Infection with Borrelia burgdorferi and Babesia microti. J. Pediatr. Infect. Dis. Soc. 2018, 7, e1–e5. [Google Scholar] [CrossRef]
- Horowitz, R.; Freeman, P.R. Healthy Fetal Outcomes Using a Novel Treatment for Maternal Lyme Disease and Babesiosis during Consecutive Pregnancies: A Case Study and Literature Review. Arch. Med. Case Rep. 2020, 2, 1–19. [Google Scholar] [CrossRef]
- Brennan, M.B.; Herwaldt, B.L.; Kazmierczak, J.J.; Weiss, J.W.; Klein, C.L.; Leith, C.P.; He, R.; Oberley, M.J.; Tonnetti, L.; Wilkins, P.P.; et al. Transmission of Babesia microti Parasites by Solid Organ Transplantation. Emerg. Infect. Dis. 2016, 22, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Goethert, H.K.; Molloy, P.; Berardi, V.; Weeks, K.; Telford, S.R. Zoonotic Babesia microti in the Northeastern U.S.: Evidence for the Expansion of a Specific Parasite Lineage. PLoS ONE 2018, 13, e0193837. [Google Scholar] [CrossRef] [PubMed]
- Eskow, E.S.; Krause, P.J.; Spielman, A.; Freeman, K.; Aslanzadeh, J. Southern Extension of the Range of Human Babesiosis in the Eastern United States. J. Clin. Microbiol. 1999, 37, 2051–2052. [Google Scholar] [CrossRef]
- Hildebrandt, A.; Zintl, A.; Montero, E.; Hunfeld, K.-P.; Gray, J. Human Babesiosis in Europe. Pathogens 2021, 10, 1165. [Google Scholar] [CrossRef]
- Prince, H.E.; Lapé-Nixon, M.; Patel, H.; Yeh, C. Comparison of the Babesia duncani (WA1) IgG Detection Rates among Clinical Sera Submitted to a Reference Laboratory for WA1 IgG Testing and Blood Donor Specimens from Diverse Geographic Areas of the United States. Clin. Vaccine Immunol. 2010, 17, 1729–1733. [Google Scholar] [CrossRef]
- Scott, J.D.; Scott, C.M. Human Babesiosis Caused by Babesia duncani Has Widespread Distribution across Canada. Healthcare 2018, 6, 49. [Google Scholar] [CrossRef]
- Milnes, E.L.; Thornton, G.; Léveillé, A.N.; Delnatte, P.; Barta, J.R.; Smith, D.A.; Nemeth, N. Babesia odocoilei and Zoonotic Pathogens Identified from Ixodes scapularis Ticks in Southern Ontario, Canada. Ticks Tick Borne Dis. 2019, 10, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Burgess, H.J.; Pattullo, K.M.; Rainbow, C.A.; Zimmer, M.; Lockerbie, B.P.; Bollinger, T.K. Surveillance of Babesia odocoilei in Wild and Farmed Cervid Populations of Saskatchewan, Canada. Can. Vet. J. 2022, 63, 735–739. [Google Scholar] [PubMed]
- Scott, J.D.; Pascoe, E.L.; Sajid, M.S.; Foley, J.E. Detection of Babesia odocoilei in Ixodes scapularis Ticks Collected in Southern Ontario, Canada. Pathogens 2021, 10, 327. [Google Scholar] [CrossRef] [PubMed]
- Waldrup, K.A.; Kocan, A.A.; Qureshi, T.; Davis, D.S.; Baggett, D.; Wagner, G.G. Serological Prevalence and Isolation of Babesia odocoilei among White-Tailed Deer (Odocoileus virginianus) in Texas And Oklahoma. J. Wildl. Dis. 1989, 25, 194–201. [Google Scholar] [CrossRef]
- Scott, J.D.; Sajid, M.S.; Pascoe, E.L.; Foley, J.E. Detection of Babesia odocoilei in Humans with Babesiosis Symptoms. Diagnostics 2021, 11, 947. [Google Scholar] [CrossRef]
- Karshima, S.N.; Karshima, M.N.; Ahmed, M.I. Global Meta-Analysis on Babesia Infections in Human Population: Prevalence, Distribution and Species Diversity. Pathog. Glob. Health 2022, 116, 220–235. [Google Scholar] [CrossRef]
- Dorman, S.E.; Cannon, M.E.; Telford, S.R.; Frank, K.M.; Churchill, W.H. Fulminant Babesiosis Treated with Clindamycin, Quinine, and Whole-Blood Exchange Transfusion. Transfusion 2000, 40, 375–380. [Google Scholar] [CrossRef]
- Mordue, D.G.; Wormser, G.P. Could the Drug Tafenoquine Revolutionize Treatment of Babesia microti Infection? J. Infect. Dis. 2019, 220, 442–447. [Google Scholar] [CrossRef]
- Tuvshintulga, B.; Vannier, E.; Tayebwa, D.S.; Gantuya, S.; Sivakumar, T.; Guswanto, A.; Krause, P.J.; Yokoyama, N.; Igarashi, I. Clofazimine, a Promising Drug for the Treatment of Babesia microti Infection in Severely Immunocompromised Hosts. J. Infect. Dis. 2020, 222, 1027–1036. [Google Scholar] [CrossRef]
- Tuvshintulga, B.; Sivakumar, T.; Nugraha, A.B.; Ahedor, B.; Batmagnai, E.; Otgonsuren, D.; Liu, M.; Xuan, X.; Igarashi, I.; Yokoyama, N. Combination of Clofazimine and Atovaquone as a Potent Therapeutic Regimen for the Radical Cure of Babesia microti Infection in Immunocompromised Hosts. J. Infect. Dis. 2022, 225, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Vannier, E.; Gelfand, J.A. Clofazimine for Babesiosis: Preclinical Data Support a Clinical Trial. J. Infect. Dis. 2022, 225, 187–189. [Google Scholar] [CrossRef] [PubMed]
- McGuffin, S.A.; Pottinger, P.S.; Harnisch, J.P. Clofazimine in Nontuberculous Mycobacterial Infections: A Growing Niche. Open Forum Infect. Dis. 2017, 4, ofx147. [Google Scholar] [CrossRef]
- Moniuszko-Malinowska, A.; Swiecicka, I.; Dunaj, J.; Zajkowska, J.; Czupryna, P.; Zambrowski, G.; Chmielewska-Badora, J.; Żukiewicz-Sobczak, W.; Swierzbinska, R.; Rutkowski, K.; et al. Infection with Babesia microti in Humans with Non-Specific Symptoms in North East Poland. Infect. Dis. 2016, 48, 537–543. [Google Scholar] [CrossRef]
- Arsuaga, M.; Gonzalez, L.M.; Lobo, C.A.; de la Calle, F.; Bautista, J.M.; Azcárate, I.G.; Puente, S.; Montero, E. First Report of Babesia microti-Caused Babesiosis in Spain. Vector Borne Zoonotic Dis. 2016, 16, 677–679. [Google Scholar] [CrossRef]
- Krause, P.J.; Gewurz, B.E.; Hill, D.; Marty, F.M.; Vannier, E.; Foppa, I.M.; Furman, R.R.; Neuhaus, E.; Skowron, G.; Gupta, S.; et al. Persistent and Relapsing Babesiosis in Immunocompromised Patients. Clin. Infect. Dis. 2008, 46, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Wormser, G.P.; Prasad, A.; Neuhaus, E.; Joshi, S.; Nowakowski, J.; Nelson, J.; Mittleman, A.; Aguero-Rosenfeld, M.; Topal, J.; Krause, P.J. Emergence of Resistance to Azithromycin-Atovaquone in Immunocompromised Patients with Babesia microti Infection. Clin. Infect. Dis. 2010, 50, 381–386. [Google Scholar] [CrossRef]
- Simon, M.S.; Westblade, L.F.; Dziedziech, A.; Visone, J.E.; Furman, R.R.; Jenkins, S.G.; Schuetz, A.N.; Kirkman, L.A. Clinical and Molecular Evidence of Atovaquone and Azithromycin Resistance in Relapsed Babesia microti Infection Associated with Rituximab and Chronic Lymphocytic Leukemia. Clin. Infect. Dis. 2017, 65, 1222–1225. [Google Scholar] [CrossRef]
- Lemieux, J.E.; Tran, A.D.; Freimark, L.; Schaffner, S.F.; Goethert, H.; Andersen, K.G.; Bazner, S.; Li, A.; McGrath, G.; Sloan, L.; et al. A Global Map of Genetic Diversity in Babesia microti Reveals Strong Population Structure and Identifies Variants Associated with Clinical Relapse. Nat. Microbiol. 2016, 1, 16079. [Google Scholar] [CrossRef] [PubMed]
- Content created by Office of HIV/AIDS; Infectious Disease Policy. Report of the Other Tick-Borne Diseases and Co-Infections Subcommittee to the Tick-Borne Disease Working Group. Available online: https://www.hhs.gov/ash/advisory-committees/tickbornedisease/reports/other-tbds-2018-5-9/index.html (accessed on 25 June 2023).
- Rajapakse, P.; Bakirhan, K. Autoimmune Hemolytic Anemia Associated with Human Babesiosis. J. Hematol. 2021, 10, 41–45. [Google Scholar] [CrossRef]
- Narurkar, R.; Mamorska-Dyga, A.; Nelson, J.C.; Liu, D. Autoimmune Hemolytic Anemia Associated with Babesiosis. Biomark. Res. 2017, 5, 14. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. Tafenoquine. In Assessment of Long-Term Health Effects of Antimalarial Drugs When Used for Prophylaxis; National Academies Press (US): Cambridge, MA, USA, 2020. [Google Scholar]
- McDonagh, E.M.; Bautista, J.M.; Youngster, I.; Altman, R.B.; Klein, T.E. PharmGKB Summary: Methylene Blue Pathway. Pharm. Genom. 2013, 23, 498–508. [Google Scholar] [CrossRef] [PubMed]
- Dapsone—An Overview|ScienceDirect Topics. Available online: https://www.sciencedirect.com/topics/neuroscience/dapsone (accessed on 25 June 2023).
- Hemolytic Anemia from Combined Use of Dapsone and Hydrochlorothiazide. Available online: https://www.emra.org/emresident/article/hemolytic-anemia (accessed on 25 June 2023).
- Baldwin, C.; Pandey, J.; Olarewaju, O. Hemolytic Anemia; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Golusin, Z.; Poljacki, M.; Preveden, R.; Stojanović, S.; Rajić, N. What do we know today about diaminodiphenylsulfone? Med. Pregl. 2000, 53, 369–372. [Google Scholar]
- Zuidema, J.; Hilbers-Modderman, E.S.; Merkus, F.W. Clinical Pharmacokinetics of Dapsone. Clin. Pharm. 1986, 11, 299–315. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.N.; Kim, S.-J. Dermatitis Herpetiformis: An Update on Diagnosis, Disease Monitoring, and Management. Medicina 2021, 57, 843. [Google Scholar] [CrossRef]
- Sorkin, E.M.; Darvey, D.L. Review of Cimetidine Drug Interactions. Drug Intell. Clin. Pharm. 1983, 17, 110–120. [Google Scholar] [CrossRef]
- Chen, J.; Raymond, K. Roles of Rifampicin in Drug-Drug Interactions: Underlying Molecular Mechanisms Involving the Nuclear Pregnane X Receptor. Ann. Clin. Microbiol. Antimicrob. 2006, 5, 3. [Google Scholar] [CrossRef]
- National Institute of Diabetes and Digestive and Kidney Diseases. Rifampin. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. [Google Scholar]
- National Institute of Diabetes and Digestive and Kidney Diseases. Pyrazinamide. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. [Google Scholar]
- Riphagen, I.J.; Minović, I.; Groothof, D.; Post, A.; Eggersdorfer, M.L.; Kootstra-Ros, J.E.; de Borst, M.H.; Navis, G.; Muskiet, F.A.J.; Kema, I.P.; et al. Methylmalonic Acid, Vitamin B12, Renal Function, and Risk of All-Cause Mortality in the General Population: Results from the Prospective Lifelines-MINUTHE Study. BMC Med. 2020, 18, 380. [Google Scholar] [CrossRef]
- Whyte, M.P. Hypophosphatasia: An Overview for 2017. Bone 2017, 102, 15–25. [Google Scholar] [CrossRef]
- Kikuchi, M.; Ushida, Y.; Shiozawa, H.; Umeda, R.; Tsuruya, K.; Aoki, Y.; Suganuma, H.; Nishizaki, Y. Sulforaphane-Rich Broccoli Sprout Extract Improves Hepatic Abnormalities in Male Subjects. World J. Gastroenterol. 2015, 21, 12457–12467. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Diabetes and Digestive and Kidney Diseases. Milk Thistle. In LiverTox: Clinical and Research Information on Drug-Induced Liver Injury; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. [Google Scholar]
- Bayard, M.; Holt, J.; Boroughs, E. Nonalcoholic Fatty Liver Disease. AFP 2006, 73, 1961–1968. [Google Scholar]
- Sinha, S.; Du, Q.; Jovanović, S.; Sukhodub, A.; Jovanović, A. Pyrazinamide May Possess Cardioprotective Properties. J. Antibiot. 2019, 72, 714–717. [Google Scholar] [CrossRef]
- Stehr, M.; Elamin, A.A.; Singh, M. Pyrazinamide: The Importance of Uncovering the Mechanisms of Action in Mycobacteria. Expert Rev. Anti-Infect. Ther. 2015, 13, 593–603. [Google Scholar] [CrossRef]
- Paz, S. Effects of Climate Change on Vector-Borne Diseases: An Updated Focus on West Nile Virus in Humans. Emerg. Top. Life Sci. 2019, 3, 143–152. [Google Scholar] [CrossRef]
- Caminade, C.; McIntyre, K.M.; Jones, A.E. Impact of Recent and Future Climate Change on Vector-borne Diseases. Ann. N. Y. Acad. Sci. 2019, 1436, 157–173. [Google Scholar] [CrossRef] [PubMed]
- Dumic, I.; Severnini, E. “Ticking Bomb”: The Impact of Climate Change on the Incidence of Lyme Disease. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 5719081. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, E.A.; Coyle, P.K.; Krupp, L.B. Post-Lyme Syndrome and Chronic Fatigue Syndrome. Neuropsychiatric Similarities and Differences. Arch. Neurol. 1997, 54, 1372–1376. [Google Scholar] [CrossRef]
- Goldenberg, D.L. Fibromyalgia, Chronic Fatigue Syndrome, and Myofascial Pain Syndrome. Curr. Opin. Rheumatol. 1995, 7, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Cameron, D. Severity of Lyme Disease with Persistent Symptoms. Insights from a Double-Blind Placebo-Controlled Clinical Trial. Minerva Med. 2008, 99, 489–496. [Google Scholar]
- Mareedu, N.; Schotthoefer, A.M.; Tompkins, J.; Hall, M.C.; Fritsche, T.R.; Frost, H.M. Risk Factors for Severe Infection, Hospitalization, and Prolonged Antimicrobial Therapy in Patients with Babesiosis. Am. J. Trop. Med. Hyg. 2017, 97, 1218–1225. [Google Scholar] [CrossRef]
- Eisen, R.J.; Paddock, C.D. Tick and Tickborne Pathogen Surveillance as a Public Health Tool in the United States. J. Med. Entomol. 2021, 58, 1490–1502. [Google Scholar] [CrossRef]
- Adkison, H.; Embers, M.E. Lyme Disease and the Pursuit of a Clinical Cure. Front. Med. 2023, 10, 1183344. [Google Scholar] [CrossRef]
- Sapi, E.; Kaur, N.; Anyanwu, S.; Luecke, D.F.; Datar, A.; Patel, S.; Rossi, M.; Stricker, R.B. Evaluation of In-Vitro Antibiotic Susceptibility of Different Morphological Forms of Borrelia burgdorferi. Infect. Drug Resist. 2011, 4, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Potula, H.-H.S.K.; Shahryari, J.; Inayathullah, M.; Malkovskiy, A.V.; Kim, K.-M.; Rajadas, J. Repurposing Disulfiram (Tetraethylthiuram Disulfide) as a Potential Drug Candidate against Borrelia burgdorferi In Vitro and In Vivo. Antibiotics 2020, 9, 633. [Google Scholar] [CrossRef] [PubMed]
- Klempner, M.S.; Hu, L.T.; Evans, J.; Schmid, C.H.; Johnson, G.M.; Trevino, R.P.; Norton, D.; Levy, L.; Wall, D.; McCall, J.; et al. Two Controlled Trials of Antibiotic Treatment in Patients with Persistent Symptoms and a History of Lyme Disease. N. Engl. J. Med. 2001, 345, 85–92. [Google Scholar] [CrossRef]
- Klempner, M.S. Controlled Trials of Antibiotic Treatment in Patients with Post-Treatment Chronic Lyme Disease. Vector Borne Zoonotic Dis. 2002, 2, 255–263. [Google Scholar] [CrossRef]
- Krupp, L.B.; Hyman, L.G.; Grimson, R.; Coyle, P.K.; Melville, P.; Ahnn, S.; Dattwyler, R.; Chandler, B. Study and Treatment of Post Lyme Disease (STOP-LD): A Randomized Double Masked Clinical Trial. Neurology 2003, 60, 1923–1930. [Google Scholar] [CrossRef]
- Fallon, B.A.; Keilp, J.G.; Corbera, K.M.; Petkova, E.; Britton, C.B.; Dwyer, E.; Slavov, I.; Cheng, J.; Dobkin, J.; Nelson, D.R.; et al. A Randomized, Placebo-Controlled Trial of Repeated IV Antibiotic Therapy for Lyme Encephalopathy. Neurology 2008, 70, 992–1003. [Google Scholar] [CrossRef]
- Berende, A.; ter Hofstede, H.J.M.; Donders, A.R.T.; van Middendorp, H.; Kessels, R.P.C.; Adang, E.M.M.; Vos, F.J.; Evers, A.W.M.; Kullberg, B.J. Persistent Lyme Empiric Antibiotic Study Europe (PLEASE)—Design of a Randomized Controlled Trial of Prolonged Antibiotic Treatment in Patients with Persistent Symptoms Attributed to Lyme Borreliosis. BMC Infect. Dis. 2014, 14, 543. [Google Scholar] [CrossRef] [PubMed]
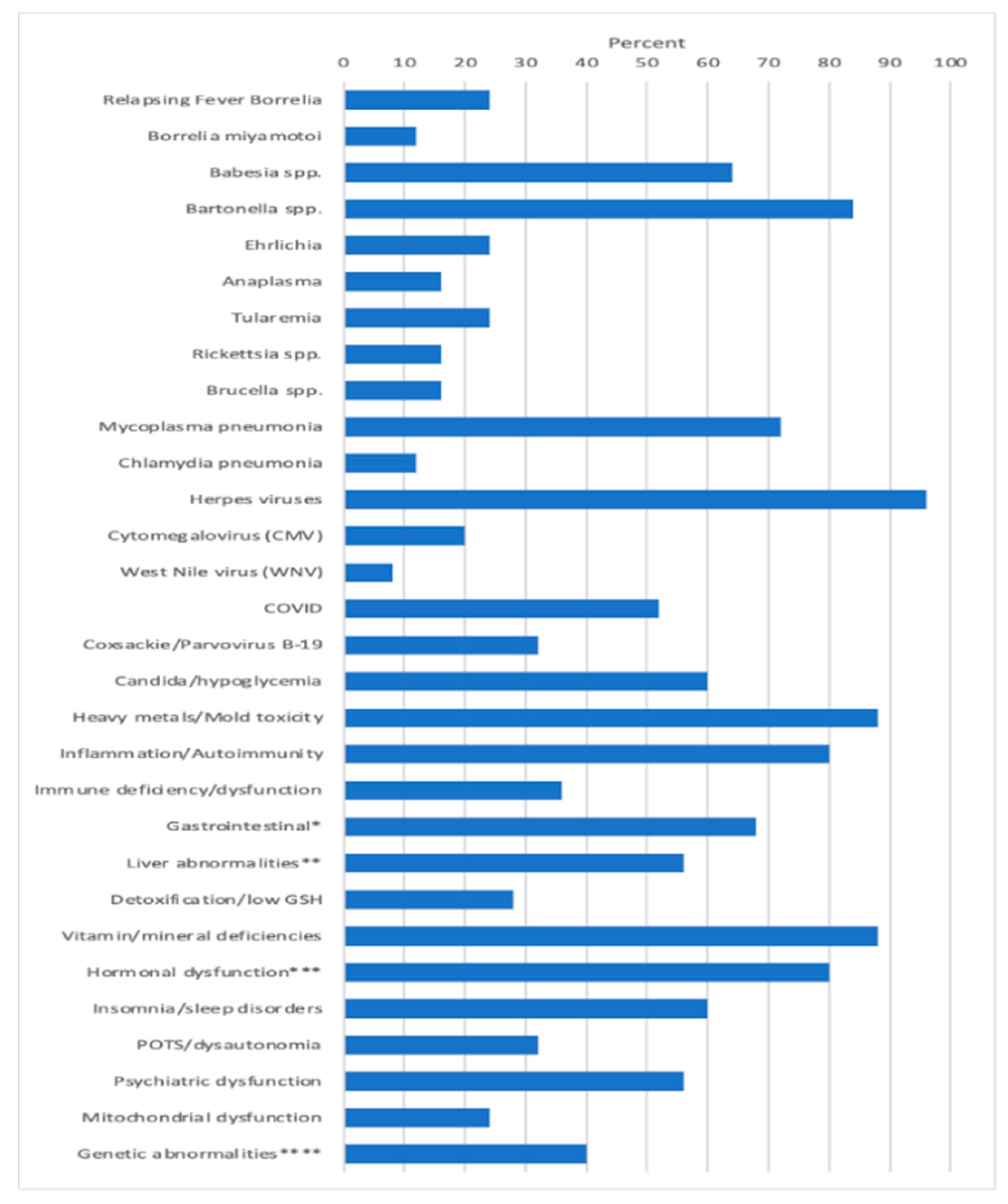


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horowitz, R.I.; Fallon, J.; Freeman, P.R. Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections. Microorganisms 2023, 11, 2301. https://doi.org/10.3390/microorganisms11092301
Horowitz RI, Fallon J, Freeman PR. Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections. Microorganisms. 2023; 11(9):2301. https://doi.org/10.3390/microorganisms11092301
Chicago/Turabian StyleHorowitz, Richard I., John Fallon, and Phyllis R. Freeman. 2023. "Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections" Microorganisms 11, no. 9: 2301. https://doi.org/10.3390/microorganisms11092301
APA StyleHorowitz, R. I., Fallon, J., & Freeman, P. R. (2023). Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections. Microorganisms, 11(9), 2301. https://doi.org/10.3390/microorganisms11092301