


Mpox Patient Journey in Israel

Abstract
:1. Introduction
2. Materials and Methods
3. Results
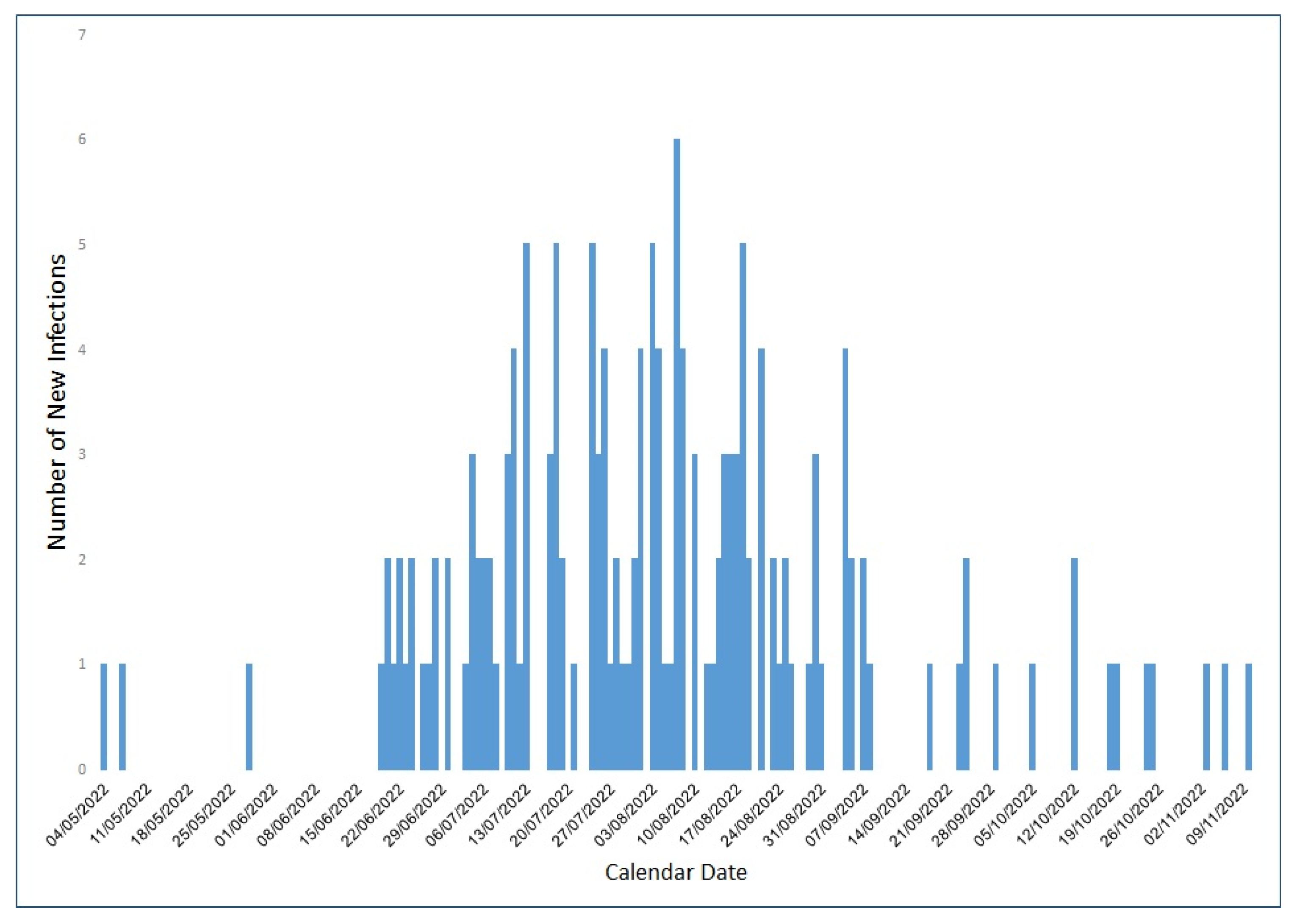
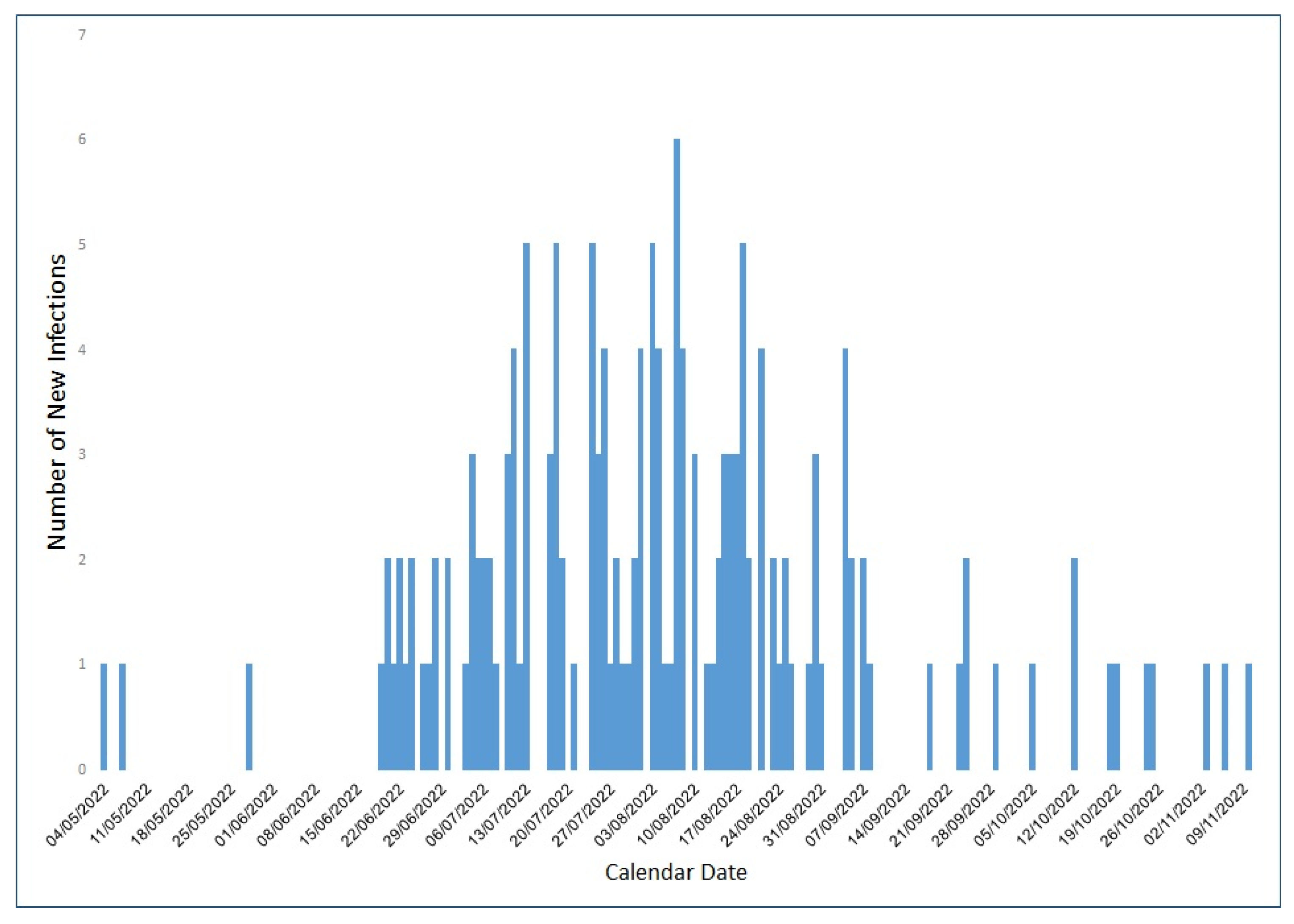
3.1. Characteristics of All Mpox Patients in MHS
3.2. Detailed Patient Journey of 18 Individuals
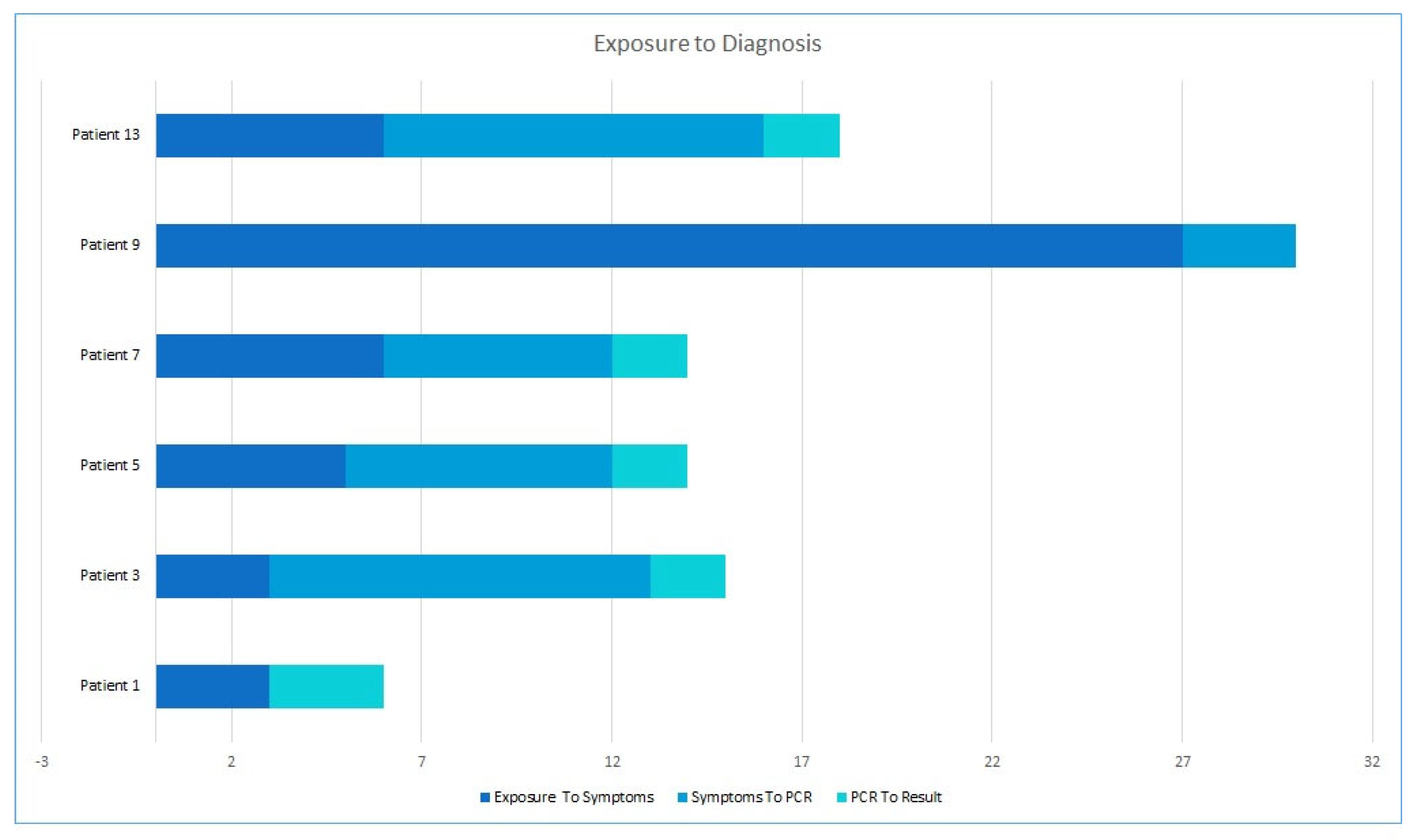
3.2.1. Exposure and Journey to Diagnosis
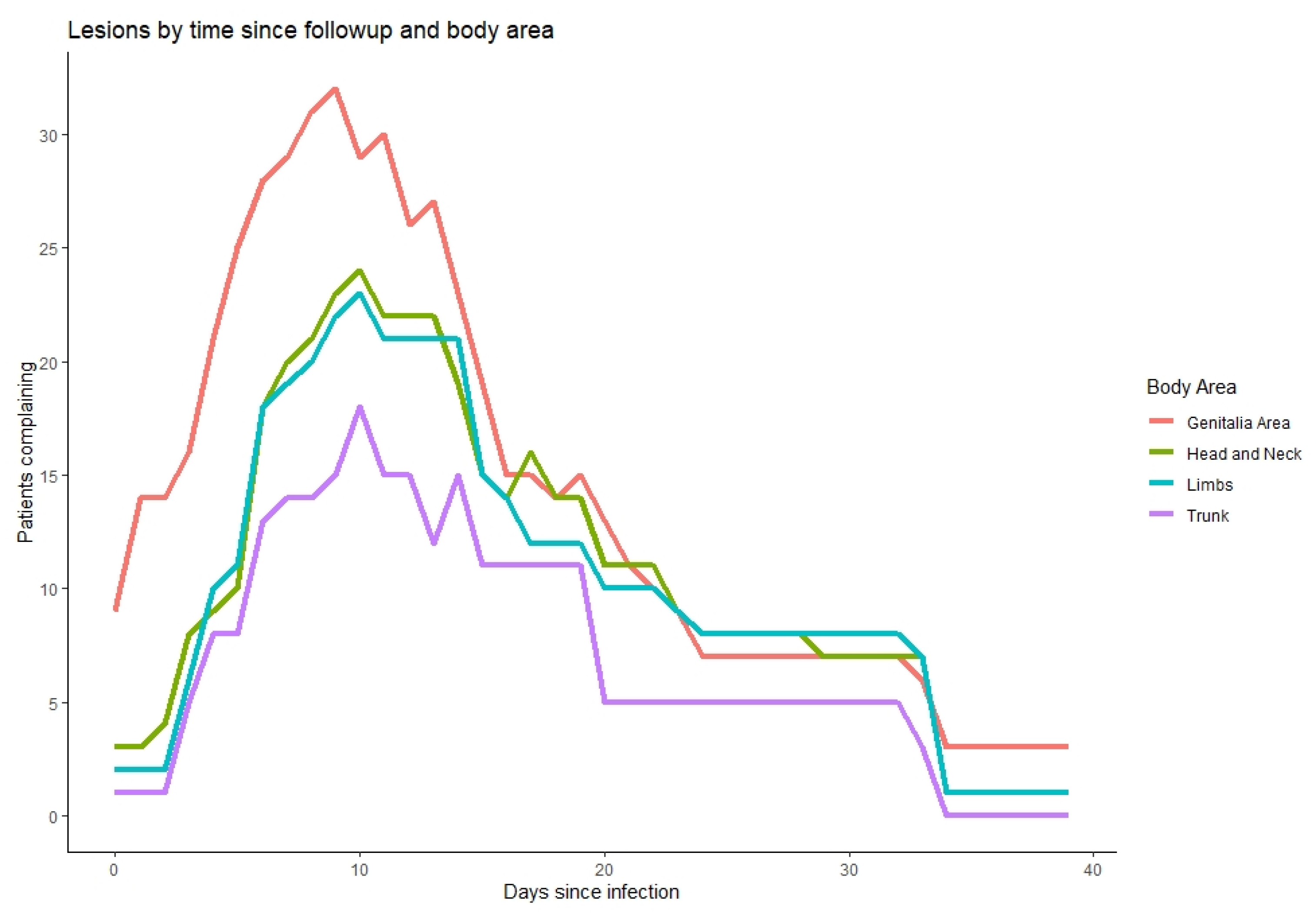
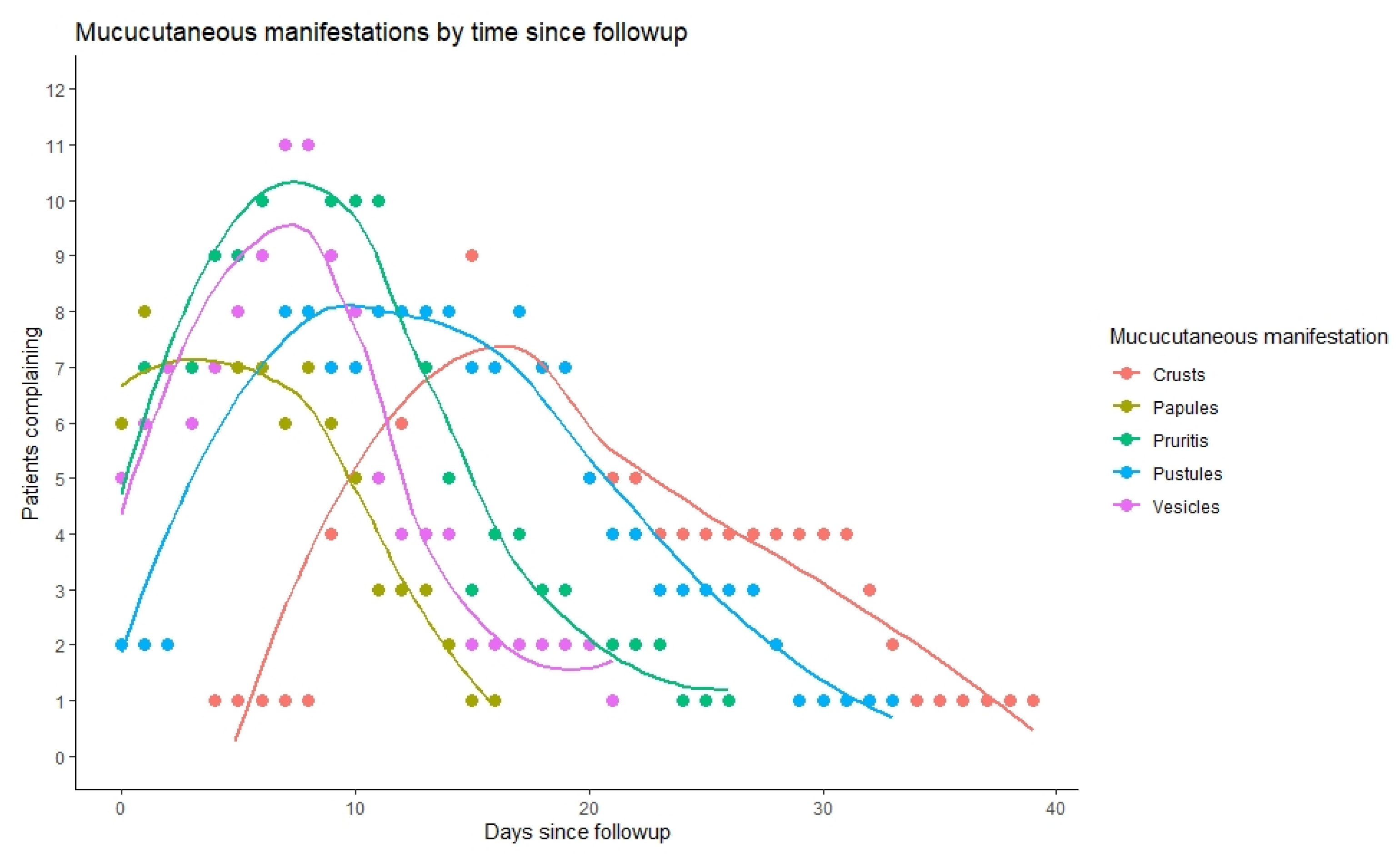
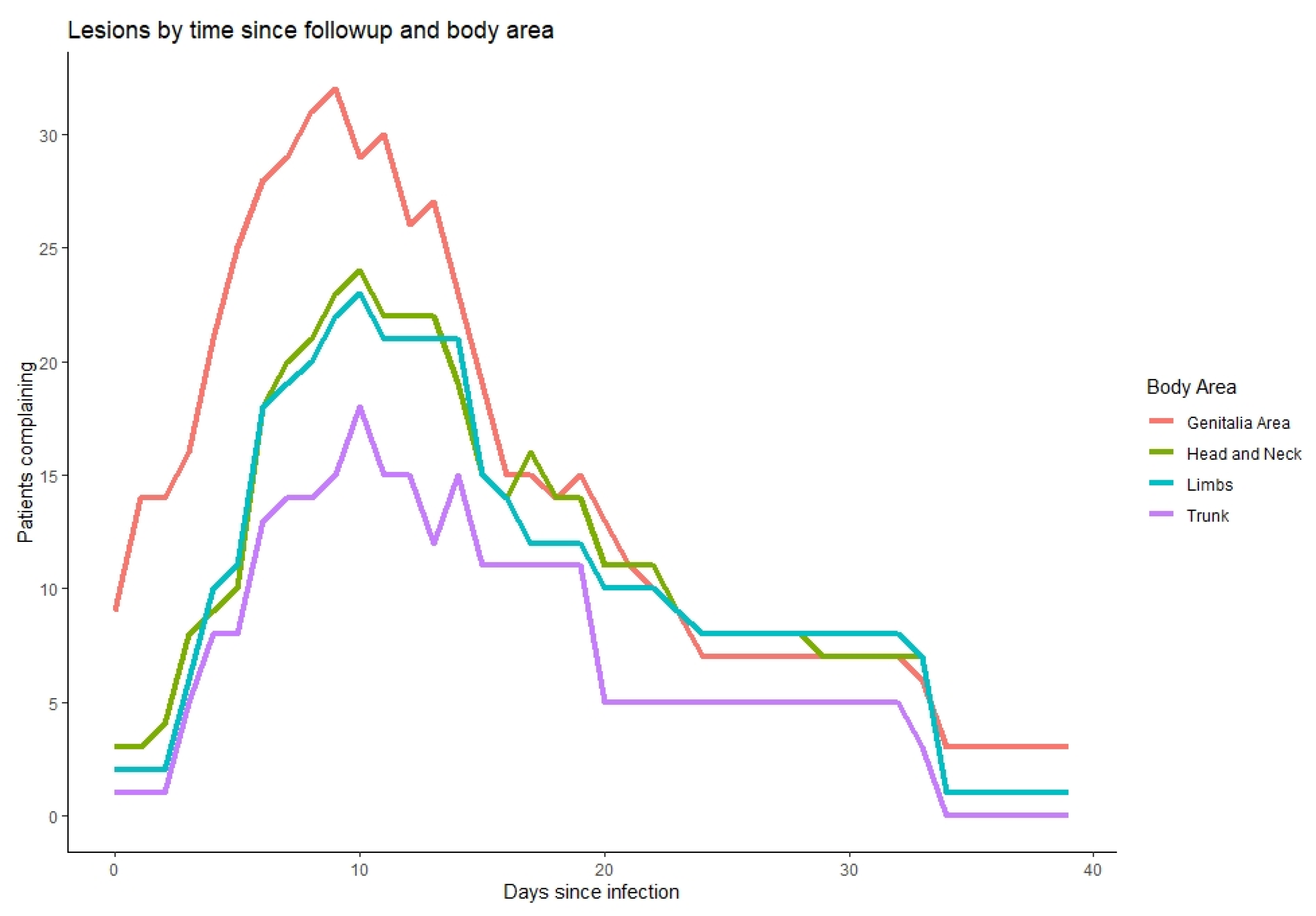
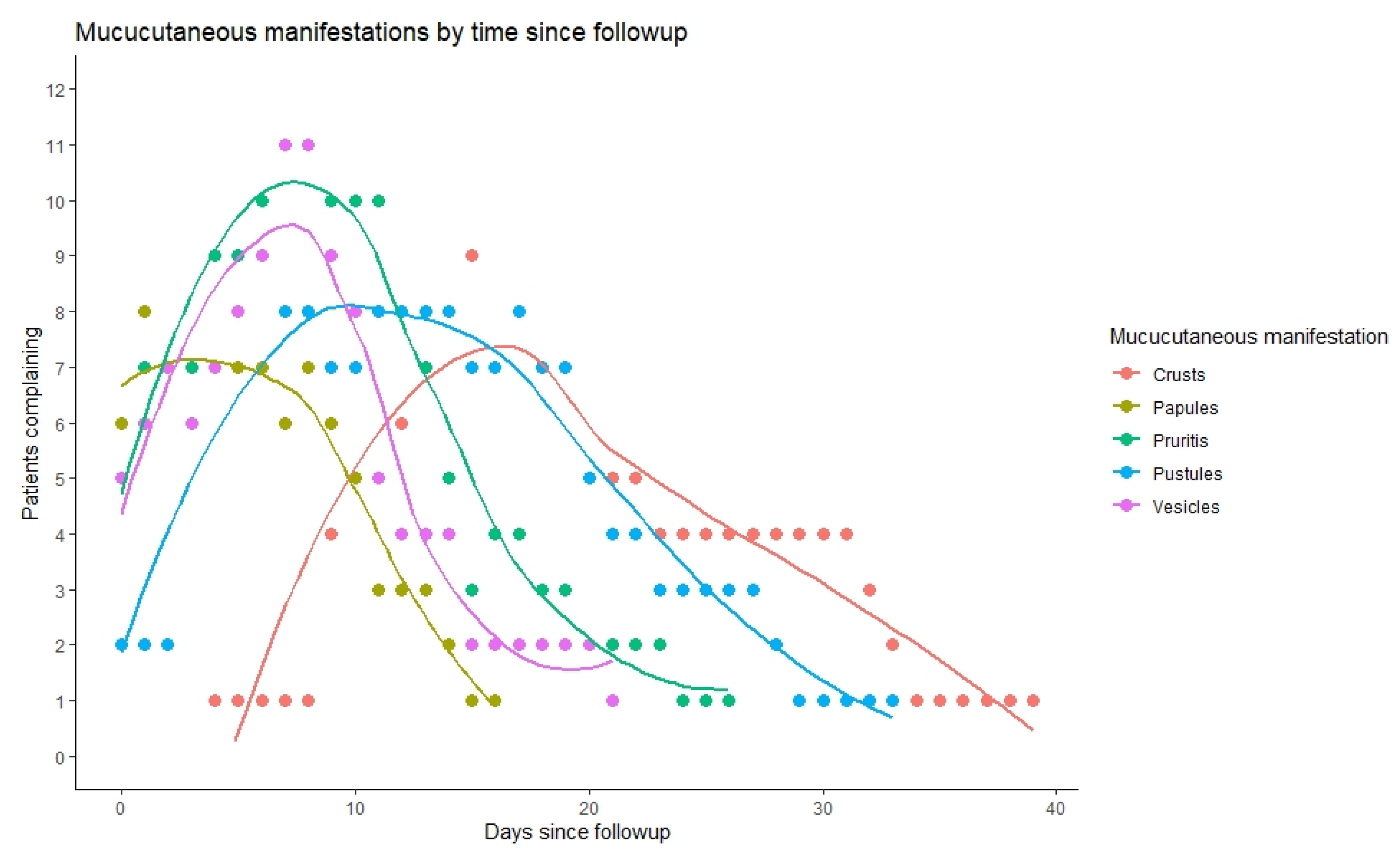
3.2.2. Mucocutaneal Manifestations
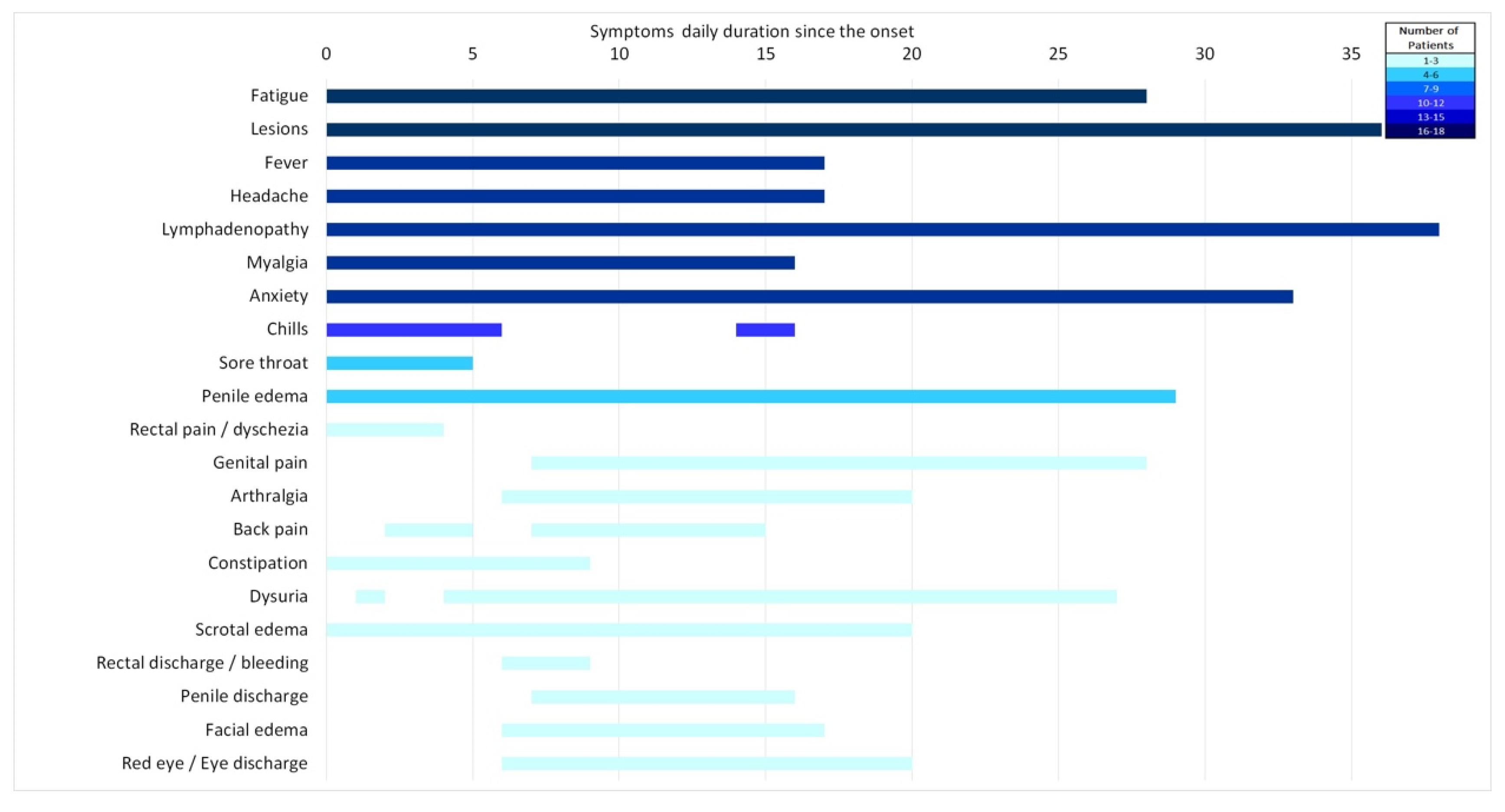
3.2.3. Other Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bunge, E.M.; Hoet, B.; Chen, L.; Lienert, F.; Weidenthaler, H.; Baer, L.R.; Steffen, R. The Changing Epidemiology of Human Monkeypox—A Potential Threat? A Systematic Review. PLoS Negl. Trop. Dis. 2022, 16, e0010141. [Google Scholar] [CrossRef] [PubMed]
- 2022 Mpox Outbreak Global Map. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 18 February 2023).
- Monkeypox|Ministry of Health. Available online: https://www.gov.il/en/Departments/Guides/disease-monkeypox (accessed on 7 March 2023).
- Multi-Country Monkeypox Outbreak: Situation Update. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON396 (accessed on 3 July 2022).
- Mpox (Monkeypox)—Symptoms, Diagnosis and Treatment|BMJ Best Practice US. Available online: https://bestpractice.bmj.com/topics/en-us/1611 (accessed on 7 March 2023).
- Israel Central Bureau of Statistics. Characterization and Classification of Geographical Units by the Socio-Economic Level of the Population 2015; Israel Central Bureau of Statistics: Jerusalem, Israel, 2019. [Google Scholar]
- Shalev, V.; Chodick, G.; Goren, I.; Silber, H.; Kokia, E.; Heymann, A.D. The Use of an Automated Patient Registry to Manage and Monitor Cardiovascular Conditions and Related Outcomes in a Large Health Organization. Int. J. Cardiol. 2011, 152, 345–349. [Google Scholar] [CrossRef]
- Chodick, G.; Heymann, A.D.; Shalev, V.; Kookia, E. The Epidemiology of Diabetes in a Large Israeli HMO. Eur. J. Epidemiol. 2003, 18, 1143–1146. [Google Scholar] [CrossRef] [PubMed]
- Israel National Cancer Registry. Available online: https://www.health.gov.il/English/MinistryUnits/HealthDivision/Icdc/Icr/Pages/default.aspx (accessed on 28 December 2021).
- Patel, A.; Bilinska, J.; Tam, J.C.H.; da Silva Fontoura, D.; Mason, C.Y.; Daunt, A.; Snell, L.B.; Murphy, J.; Potter, J.; Tuudah, C.; et al. Clinical Features and Novel Presentations of Human Monkeypox in a Central London Centre during the 2022 Outbreak: Descriptive Case Series. BMJ 2022, 378, e072410. [Google Scholar] [CrossRef]
- Tarín-Vicente, E.J.; Alemany, A.; Agud-Dios, M.; Ubals, M.; Suñer, C.; Antón, A.; Arando, M.; Arroyo-Andrés, J.; Calderón-Lozano, L.; Casañ, C.; et al. Clinical Presentation and Virological Assessment of Confirmed Human Monkeypox Virus Cases in Spain: A Prospective Observational Cohort Study. Lancet 2022, 400, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Thornhill, J.P.; Barkati, S.; Walmsley, S.; Rockstroh, J.; Antinori, A.; Harrison, L.B.; Palich, R.; Nori, A.; Reeves, I.; Habibi, M.S.; et al. Monkeypox Virus Infection in Humans across 16 Countries—April–June 2022. N. Engl. J. Med. 2022, 387, 679–691. [Google Scholar] [CrossRef]
- Girometti, N.; Byrne, R.; Bracchi, M.; Heskin, J.; McOwan, A.; Tittle, V.; Gedela, K.; Scott, C.; Patel, S.; Gohil, J.; et al. Demographic and Clinical Characteristics of Confirmed Human Monkeypox Virus Cases in Individuals Attending a Sexual Health Centre in London, UK: An Observational Analysis. Lancet Infect. Dis. 2022, 22, 1321–1328. [Google Scholar] [CrossRef]
- Gomez-Garberi, M.; Sarrio-Sanz, P.; Martinez-Cayuelas, L.; Delgado-Sanchez, E.; Bernabeu-Cabezas, S.; Peris-Garcia, J.; Sanchez-Caballero, L.; Nakdali-Kassab, B.; Egea-Sancho, C.; Olarte-Barragan, E.H.; et al. Genitourinary Lesions Due to Monkeypox. Eur. Urol. 2022, 82, 625–630. [Google Scholar] [CrossRef]
- Betancort-Plata, C.; Lopez-Delgado, L.; Jaén-Sanchez, N.; Tosco-Nuñez, T.; Suarez-Hormiga, L.; Lavilla-Salgado, C.; Pisos-Álamo, E.; Hernández-Betancor, A.; Hernández-Cabrera, M.; Carranza-Rodríguez, C.; et al. Monkeypox and HIV in the Canary Islands: A Different Pattern in a Mobile Population. Trop. Med. Infect. Dis. 2022, 7, 318. [Google Scholar] [CrossRef]
- Accordini, S.; Cordioli, M.; Pomari, E.; Tacconelli, E.; Castilletti, C. People with Asymptomatic or Unrecognised Infection Potentially Contribute to Monkeypox Virus Transmission. Lancet Microbe 2022, 4, e209. [Google Scholar] [CrossRef]
- van Dijck, C.; de Baetselier, I.; Kenyon, C.; Liesenborghs, L.; Vercauteren, K.; van Esbroeck, M.; van Dijck, C.; de Baetselier, I.; Kenyon, C.; Brosius, I.; et al. Mpox Screening in High-Risk Populations Finds No Asymptomatic Cases. Lancet Microbe 2022, 4, e132–e133. [Google Scholar] [CrossRef]
- Chemtob, D.; Mor, Z.; Harel, N.; Averick, N. HIV Infection among Men Who Have Sex with Men in Israel: A 35-Year Epidemiological and Clinical Overview, 1981–2015. BMC Public Health 2019, 19, 747. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. HIV/AIDS Surveillance in Europe 2022: 2021 Data; European Centre for Disease Prevention and Control: Stockholm City, Sweden, 2022. [Google Scholar]
- Allan-Blitz, L.-T.; Gandhi, M.; Adamson, P.; Park, I.; Bolan, G.; Klausner, J.D. A Position Statement on Mpox as a Sexually Transmitted Disease. Clin. Infect. Dis. 2022. [Google Scholar] [CrossRef] [PubMed]
- Golden, M.R.; Wasserheit, J.N. Monkeypox—A Sobering Sentinel for Pandemic Preparedness and Sexual Health System Capacity. N. Engl. J. Med. 2022, 387, 1826–1829. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; d’Abreu de Paulo, K.J.I.; Gültzow, T.; Zimmermann, H.M.L.; Jonas, K.J. Monkeypox Self-Diagnosis Abilities, Determinants of Vaccination and Self-Isolation Intention after Diagnosis among MSM, the Netherlands, July 2022. Eurosurveillance 2022, 27, 2200603. [Google Scholar] [CrossRef]
- Antinori, A.; Mazzotta, V.; Vita, S.; Carletti, F.; Tacconi, D.; Lapini, L.E.; D’Abramo, A.; Cicalini, S.; Lapa, D.; Pittalis, S.; et al. Epidemiological, Clinical and Virological Characteristics of Four Cases of Monkeypox Support Transmission through Sexual Contact, Italy, May 2022. Eurosurveillance 2022, 27, 2200421. [Google Scholar] [CrossRef]
- Hammerschlag, Y.; MacLeod, G.; Papadakis, G.; Sanchez, A.A.; Druce, J.; Taiaroa, G.; Savic, I.; Mumford, J.; Roberts, J.; Caly, L.; et al. Monkeypox Infection Presenting as Genital Rash, Australia, May 2022. Eurosurveillance 2022, 27, 2200411. [Google Scholar] [CrossRef]
- Martins-Filho, P.R.; Tanajura, D.M.; Alves dos Santos, C. Polymerase Chain Reaction Positivity and Cycle Threshold Values in Biological Samples from Patients with Monkeypox: A Meta-Analysis. Travel. Med. Infect. Dis. 2022, 50, 102448. [Google Scholar] [CrossRef]
- Ahmed, S.K.; Saied, A.R.A.; Ravi, R.K.; Mohammed, M.G.; Hussein, S.H.; Essa, R.A.; Abdulqadir, S.O.; Abdulla, A.Q. The 2022 Monkeypox Outbreak and Associated Psychiatric Morbidities. Int. J. Surg. 2022, 106, 106913. [Google Scholar] [CrossRef]
- Ahmed, S.K.; Abdulqadir, S.O.; Hussein, S.H.; Omar, R.M.; Ahmed, N.A.; Essa, R.A.; Dhama, K.; Lorenzo, J.M.; Abdulla, A.Q. The Impact of Monkeypox Outbreak on Mental Health and Counteracting Strategies: A Call to Action. Int. J. Surg. 2022, 106, 106943. [Google Scholar] [CrossRef]
- Dsouza, V.S.; Rajkhowa, P.; Mallya, B.R.; Raksha, D.S.; Mrinalini, V.; Cauvery, K.; Raj, R.; Toby, I.; Pattanshetty, S.; Brand, H. A Sentiment and Content Analysis of Tweets on Monkeypox Stigma among the LGBTQ+ Community: A Cue to Risk Communication Plan. Dialogues Health 2022, 2, 100095. [Google Scholar] [CrossRef] [PubMed]
- Stumbar, S.E.; Nusynowitz, J.; Jamneshan, L.; Samuels, M.; Nana, |; Garba, A. The Need for Emerging Diseases Curricula: A Case Study of Mpox. PRiMER 2022, 6, 46. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Trial Participants | All MHS Mpox Patients | |
|---|---|---|
| (N = 18) | (N = 159) | |
| Demographics | ||
| Sex—n (%) | ||
| Female | 0 (0%) | 15 (9.4%) |
| Male | 18 (100%) | 144 (90.6%) |
| Age at Mpox diagnosis | ||
| Mean (SD) | 37.6 (6.27) | 36.3 (12.5) |
| Median [Min, Max] | 36.6 [27.3, 58.2] | 35.0 [0.970, 84.7] |
| Socioeconomic status—n (%) | ||
| High (7–10) | 13 (72.2%) | 92 (57.9%) |
| Middle (4–6) | 5 (27.8%) | 63 (39.6%) |
| Low (1–3) | 0 (0%) | 4 (2.5%) |
| Periphery indicator—n (%) | ||
| No | 18 (100%) | 154 (96.9%) |
| Yes | 0 (0%) | 5 (3.1%) |
| Comorbidities—n (%) | ||
| Diabetes Mellitus (Yes) | 0 (0%) | 1 (0.6%) |
| Hypertension (Yes) | 1 (5.6%) | 8 (5.0%) |
| Cardiovascular diseases (Yes) | 0 (0%) | 5 (3.1%) |
| Obesity (BMI ≥30) (Yes) | 0 (0%) | 10 (6.3%) |
| Concomitant Sexually Transmitted Infection (STI)—n (%) | ||
| Any concomitant STI (Yes) | 4 (22.2%) | 22 (13.8%) |
| Chlamydia (Yes) | 0 (0%) | 2 (1.3%) |
| Condyloma Acuminatum (Yes) | 1 (5.6%) | 3 (1.9%) |
| Gonorrhea (Yes) | 2 (11.1%) | 7 (4.4%) |
| Mycoplasma genitalium (Yes) | 0 (0%) | 1 (0.6%) |
| Syphilis (Yes) | 1 (5.6%) | 8 (5.0%) |
| Herpes Genitalis (Yes) | 0 (0%) | 1 (0.6%) |
| HIV status and antiretroviral treatment | ||
| HIV positive (Yes) | 4 (22.2%) | 16 (10.1%) |
| Antiretroviral treatment among HIV (Yes) | 4 (100%) | 16 (100%) |
| Use of preexposure prophylaxis (PrEP) against HIV in HIV negative (Yes) | 12 (66.7%) | 70 (44.0%) |
| Prior Sexually Transmitted Infection—n (%) | ||
| Any prior STI (Yes) | 14 (77.8%) | 99 (62.3%) |
| Chlamydia (Yes) | 5 (27.8%) | 35 (22.0%) |
| Condyloma acuminatum (Yes) | 7 (38.9%) | 41 (25.8%) |
| Gonorrhea (Yes) | 8 (44.4%) | 35 (22.0%) |
| Mycoplasma genitalium (Yes) | 2 (11.1%) | 15 (9.4%) |
| Syphilis (Yes) | 4 (22.2%) | 28 (17.6%) |
| Herpes genitalis (Yes) | 2 (11.1%) | 6 (3.8%) |
| Phthirus pubis (Yes) | 5 (27.8%) | 15 (9.4%) |
| Clinical Trial Participants | All MHS Mpox Patients | |
|---|---|---|
| (N = 18) | (N = 159) | |
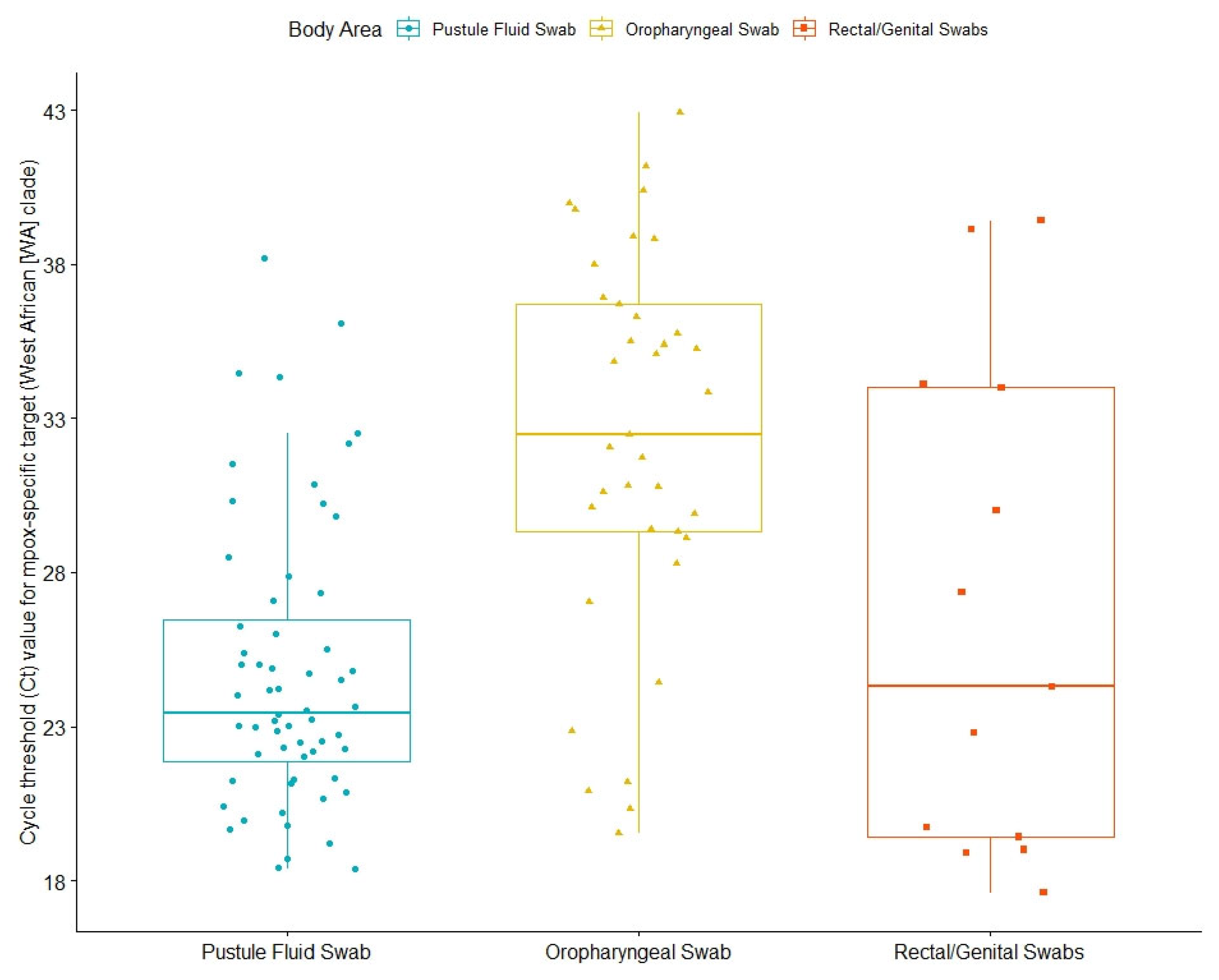
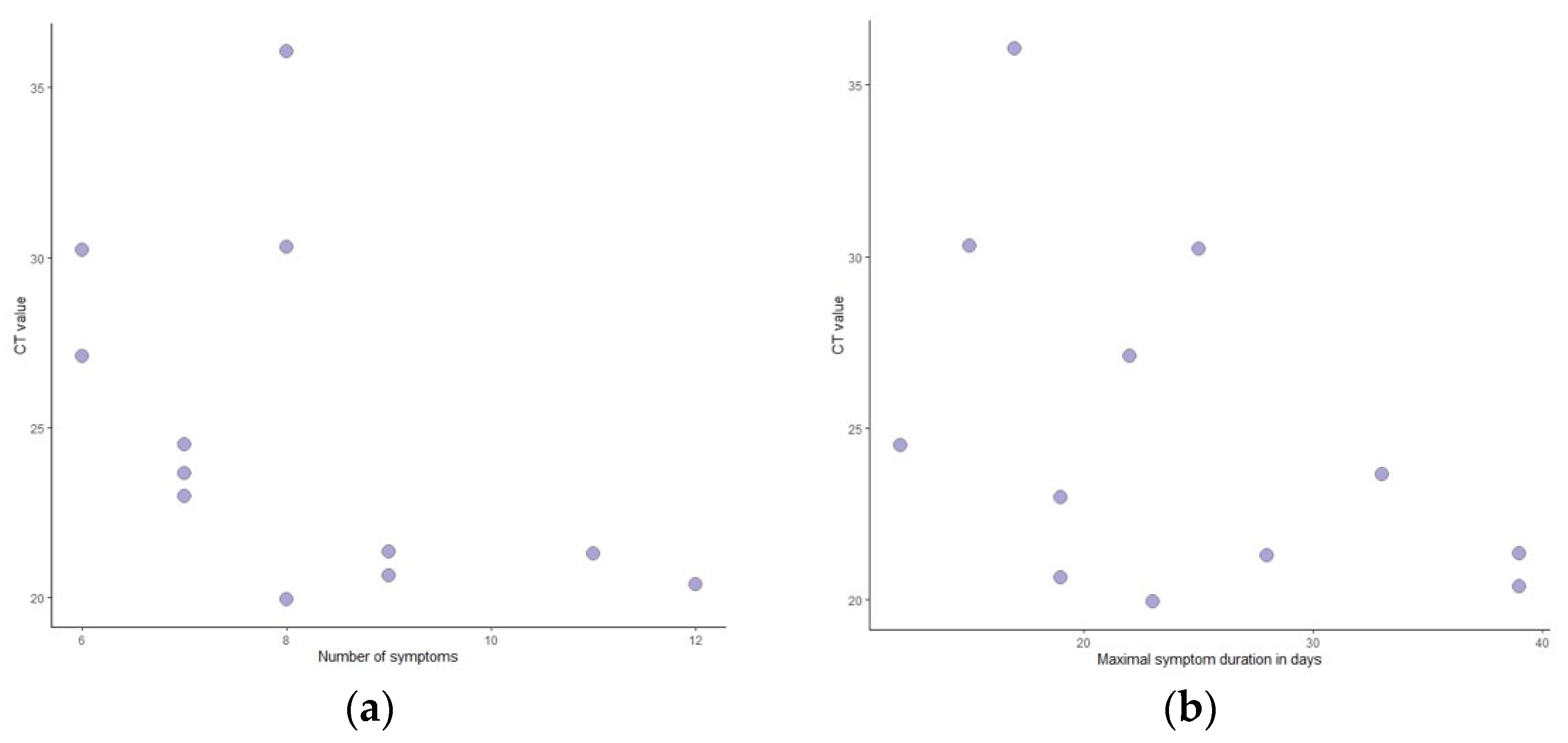
| Ct Values | ||
| Overall mean Ct | ||
| Mean (SD) | 28.0 (4.56) | 27.5 (4.74) |
| Median [Min, Max] | 27.4 [21.1, 36.1] | 27.3 [18.4, 38.8] |
| Missing | 6 (33.3%) | 96 (60.4%) |
| Oropharyngeal swab | ||
| Mean (SD) | 31.6 (7.90) | 32.2 (6.31) |
| Median [Min, Max] | 33.6 [19.6, 40.4] | 32.3 [19.6, 42.9] |
| Missing | 10 (55.6%) | 123 (77.4%) |
| Skin lesion swab | ||
| Mean (SD) | 24.9 (5.05) | 24.9 (4.69) |
| Median [Min, Max] | 23.3 [19.9, 36.1] | 23.5 [18.4, 38.2] |
| Missing | 6 (33.3%) | 108 (67.9%) |
| Rectal swabs | ||
| Mean (SD) | 34.1 (NA) | 26.6 (7.96) |
| Median [Min, Max] | 34.1 [34.1, 34.1] | 24.3 [17.6, 39.4] |
| Missing | 17 (94.4%) | 146 (91.8%) |
| Females | Males | All | |
|---|---|---|---|
| (N = 15) | (N = 144) | (N = 159) | |
| Demographics | |||
| Age at Mpox diagnosis | |||
| Mean (SD) | 46.0 (23.1) | 35.3 (10.5) | 36.3 (12.5) |
| Median [Min, Max] | 48.3 [0.970, 84.7] | 34.3 [2.84, 72.8] | 35.0 [0.970, 84.7] |
| Socioeconomic status—n (%) | |||
| High (7–10) | 7 (46.7%) | 85 (59.0%) | 92 (57.9%) |
| Middle (4–6) | 8 (53.3%) | 55 (38.2%) | 63 (39.6%) |
| Low (1–3) | 0 (0%) | 4 (2.8%) | 4 (2.5%) |
| Periphery indicator—n (%) | |||
| No | 15 (100%) | 139 (96.5%) | 154 (96.9%) |
| Yes | 0 (0%) | 5 (3.5%) | 5 (3.1%) |
| Comorbidities—n (%) | |||
| Diabetes Mellitus (Yes) | 1 (6.7%) | 0 (0%) | 1 (0.6%) |
| Hypertension (Yes) | 2 (13.3%) | 6 (4.2%) | 8 (5.0%) |
| Cardiovascular diseases (Yes) | 2 (13.3%) | 3 (2.1%) | 5 (3.1%) |
| Obesity (BMI ≥30) (Yes) | 1 (6.7%) | 9 (6.2%) | 10 (6.3%) |
| Concomitant Sexually Transmitted Infection—n (%) | |||
| Chlamydia (Yes) | 0 (0%) | 2 (1.4%) | 2 (1.3%) |
| Condyloma Acuminatum (Yes) | 0 (0%) | 3 (2.1%) | 3 (1.9%) |
| Gonorrhea (Yes) | 0 (0%) | 7 (4.9%) | 7 (4.4%) |
| Mycoplasma genitalium (Yes) | 0 (0%) | 1 (0.7%) | 1 (0.6%) |
| Syphilis (Yes) | 0 (0%) | 8 (5.6%) | 8 (5.0%) |
| Herpes Genitalis (Yes) | 0 (0%) | 1 (0.7%) | 1 (0.6%) |
| HIV status and antiretroviral treatment | |||
| HIV positive (Yes) | 0 (0%) | 16 (11.1%) | 16 (10.1%) |
| Antiretroviral treatment among HIV (Yes) | 0 (100%) | 16 (100%) | 16 (100%) |
| Use of preexposure prophylaxis (PrEP) against HIV in HIV negative (Yes) | 0 (0%) | 70 (48.6%) | 70 (44.0%) |
| Prior Sexually Transmitted Infection—n (%) | |||
| Any prior infection (Yes) | 4 (26.7%) | 95 (66.0%) | 99 (62.3%) |
| Chlamydia (Yes) | 0 (0%) | 35 (24.3%) | 35 (22.0%) |
| Condyloma acuminatum (Yes) | 2 (13.3%) | 39 (27.1%) | 41 (25.8%) |
| Gonorrhea (Yes) | 0 (0%) | 35 (24.3%) | 35 (22.0%) |
| Mycoplasma genitalium (Yes) | 0 (0%) | 15 (10.4%) | 15 (9.4%) |
| Syphilis (Yes) | 0 (0%) | 28 (19.4%) | 28 (17.6%) |
| Herpes genitalis (Yes) | 1 (6.7%) | 5 (3.5%) | 6 (3.8%) |
| Phthirus pubis (Yes) | 0 (0%) | 15 (10.4%) | 15 (9.4%) |
| N | % | |
|---|---|---|
| Exposure | ||
| Traveling abroad within a month prior to Mpox diagnosis | ||
| No | 6 | 33% |
| Yes | 6 | 33% |
| Known exposure to Mpox | 10 | 56% |
| Sexual history | ||
| Sexual intercourse within two months prior to the disease | 18 | 100% |
| Sexual history in the month prior to diagnosis | ||
| Unprotected Sexual intercourse | 16 | 89% |
| Unprotected sexual intercourse with men | 14 | 78% |
| Unprotected sexual intercourse with women | 1 | 6% |
| Unprotected oral sexual intercourse | 11 | 61% |
| Unprotected anal sexual intercourse | 11 | 61% |
| First suspicion raised by | ||
| The patient | 13 | 72% |
| A close contact (friend or family) | 1 | 6% |
| The primary care physician | 1 | 6% |
| An emergency department physician | 2 | 11% |
| Time from symptom to first suspicion (days) median [min, max] | 3.5 | [0, 10] |
| Symptoms | ||
| Mucocutaneal lesions | ||
| Number of regions | ||
| 1 region | 3 | 17% |
| 2–5 regions | 8 | 44% |
| ≥5 regions | 6 | 33% |
| Lesion location | ||
| Face | 8 | 44% |
| Neck | 4 | 22% |
| Shoulders | 1 | 6% |
| Chest | 2 | 11% |
| Abdomen | 4 | 22% |
| Back | 3 | 17% |
| Buttocks | 0 | 0% |
| Arms/legs | 12 | 67% |
| Hands/Feet | 2 | 11% |
| Groin | 7 | 39% |
| Penis | 9 | 50% |
| Scrotum | 0 | 0% |
| Anal/perianal | 6 | 33% |
| Oropharynx | 1 | 6% |
| Pain of lesions | 1 | 6% |
| Constitutional symptoms (-any) | 18 | 100% |
| Fever | 15 | 83% |
| Chills | 11 | 61% |
| Fatigue | 18 | 100% |
| Headache | 14 | 78% |
| Myalgia | 13 | 72% |
| Back pain | 2 | 11% |
| Arthralgia | 2 | 11% |
| Lymphadenopathy (-any) | 14 | 78% |
| Submandibular | 2 | 11% |
| Cervical | 4 | 22% |
| Axillary | 0 | 0% |
| Inguinal | 14 | 78% |
| Sore throat | 4 | 22% |
| Eye pain, red eye or discharge | 1 | 6% |
| Facial edema | 1 | 6% |
| Fear of the disease [0, 1–5] (median) (min., max.) | 4 | [2, 5] |
| Rectal pain/dyschezia | 5 | 28% |
| Rectal discharge or bleeding | 1 | 6% |
| Constipation | 2 | 11% |
| Dysuria | 2 | 11% |
| Pain in genitals | 1 | 6% |
| Penile edema | 5 | 28% |
| Penile pruritis | 4 | 22% |
| Penile discharge | 1 | 6% |
| Edema of scrotum | 2 | 11% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patalon, T.; Perez, G.; Saciuk, Y.; Refaeli, Z.; Gazit, S. Mpox Patient Journey in Israel. Microorganisms 2023, 11, 1042. https://doi.org/10.3390/microorganisms11041042
Patalon T, Perez G, Saciuk Y, Refaeli Z, Gazit S. Mpox Patient Journey in Israel. Microorganisms. 2023; 11(4):1042. https://doi.org/10.3390/microorganisms11041042
Chicago/Turabian StylePatalon, Tal, Galit Perez, Yaki Saciuk, Ziva Refaeli, and Sivan Gazit. 2023. "Mpox Patient Journey in Israel" Microorganisms 11, no. 4: 1042. https://doi.org/10.3390/microorganisms11041042
APA StylePatalon, T., Perez, G., Saciuk, Y., Refaeli, Z., & Gazit, S. (2023). Mpox Patient Journey in Israel. Microorganisms, 11(4), 1042. https://doi.org/10.3390/microorganisms11041042