
Healthcare-Associated Bloodstream Infections Due to Multidrug-Resistant Acinetobacter baumannii in COVID-19 Intensive Care Unit: A Single-Center Retrospective Study


 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Definitions and Data Collection
2.3. Laboratory Procedures and Statistical Analysis
2.4. Molecular Analysis of Carbapenem Resistance Determinants
2.5. Molecular Epidemiology
2.6. Statistical Analysis
3. Results
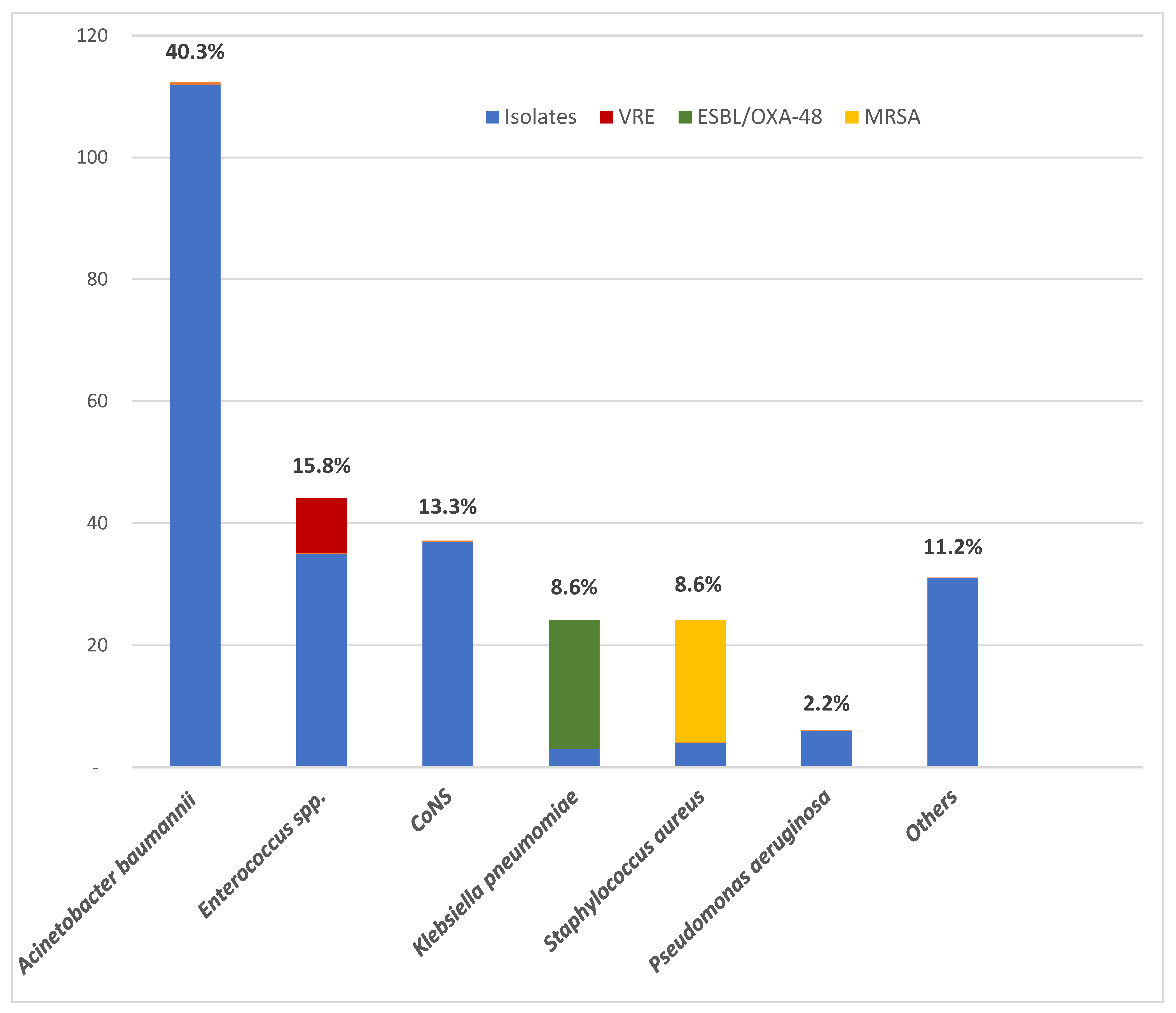
3.1. Bacterial Isolates and Resistance
3.2. Patients with BSI Caused by MDR A. baumannii
3.2.1. Characteristics of Patients
3.2.2. Antimicrobial Resistance Pattern
3.2.3. Carbapenem Resistance Determinants
3.2.4. Molecular Epidemiology Results
3.3. Hospital Environment and Infection Control
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 14 February 2023).
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Grasselli, G.; Pesenti, A.; Cecconi, M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: Early experience and forecast during an emergency response. JAMA 2020, 323, 1545. [Google Scholar] [CrossRef]
- Timsit, J.-F.; Ruppé, E.; Barbier, F.; Tabah, A.; Bassetti, M. Bloodstream infections in critically ill patients: An expert statement. Intensiv. Care Med. 2020, 46, 266–284. [Google Scholar] [CrossRef]
- Buetti, N.; Ruckly, S.; de Montmollin, E.; Reignier, J.; Terzi, N.; Cohen, Y.; Siami, S.; Dupuis, C.; Timsit, J.-F. COVID-19 increased the risk of ICU-acquired bloodstream infections: A case–cohort study from the multicentric OUTCOMEREA network. Intensiv. Care Med. 2021, 47, 180–187. [Google Scholar] [CrossRef]
- Russo, A.; Bassetti, M.; Ceccarelli, G.; Carannante, N.; Losito, A.R.; Bartoletti, M.; Corcione, S.; Granata, G.; Santoro, A.; Giacobbe, D.R.; et al. Bloodstream infections caused by carbapenem-resistant Acinetobacter baumannii: Clinical features, therapy and outcome from a multicenter study. J. Infect. 2019, 79, 130–138. [Google Scholar] [CrossRef]
- Kim, U.J.; Kim, H.K.; An, J.H.; Cho, S.K.; Park, K.-H.; Jang, H.-C. Update on the epidemiology, treatment, and outcomes of carbapenem-resistant Acinetobacter infections. Chonnam Med. J. 2014, 50, 37–44. [Google Scholar] [CrossRef][Green Version]
- Bergogne-Bérézin, E.; Towner, K.J. Acinetobacter spp. as nosocomial pathogens: Microbiological, clinical, and epidemiological features. Clin. Microbiol. Rev. 1996, 9, 148–165. [Google Scholar] [CrossRef]
- Maragakis, L.L.; Perl, T.M. Acinetobacter baumannii: Epidemiology, antimicrobial resistance, and treatment options. Clin. Infect. Dis. 2008, 46, 1254–1263. [Google Scholar] [CrossRef]
- Croatian Academy of Medical Sciences. Antibiotic Resistance in Croatia. 2021. Available online: https://iskra.bfm.hr/wp-content/uploads/2022/11/Knjiga-2021-za-web-final.pdf (accessed on 1 December 2022).
- Poirel, L.; Nordmann, P. Carbapenem resistance in Acinetobacter baumannii: Mechanisms and epidemiology. Clin. Microbiol. Infect. 2006, 12, 826–836. [Google Scholar] [CrossRef]
- Bonnin, R.; Poirel, L.; Naas, T.; Pirs, M.; Seme, K.; Schrenzel, J.; Nordmann, P. Dissemination of New Delhi metallo-β-lactamase-1-producing Acinetobacter baumannii in Europe. Clin. Microbiol. Infect. 2012, 18, E362–E365. [Google Scholar] [CrossRef]
- Turton, J.F.; Ward, M.E.; Woodford, N.; Kaufmann, M.E.; Pike, R.; Livermore, D.M.; Pitt, T.L. The role of ISAba1 in expression of OXA carbapenemase genes in Acinetobacter baumannii. FEMS Microbiol. Lett. 2006, 258, 72–77. [Google Scholar] [CrossRef]
- Mugnier, P.D.; Poirel, L.; Naas, T.; Nordmann, P. Worldwide dissemination of the blaOXA-23 carbapenemase gene of Acinetobacter baumannii. Emerg. Infect. Dis. 2010, 16, 35–40. [Google Scholar] [CrossRef]
- Lukovic, B.; Gajic, I.; Dimkić, I.; Kekic, D.; Zornic, S.; Pozder, T.; Radisavljevic, S.; Opavski, N.; Kojic, M.; Ranin, L. The first nationwide multicenter study of Acinetobacter baumannii recovered in Serbia: Emergence of OXA-72, OXA-23 and NDM-1-producing isolates. Antimicrob. Resist. Infect. Control 2020, 9, 101. [Google Scholar] [CrossRef]
- Franolić-Kukina, I.; Bedenić, B.; Budimir, A.; Herljević, Z.; Vraneš, J.; Higgins, P.G. Clonal spread of carbapenem-resistant OXA-72-positive Acinetobacter baumannii in a Croatian university hospital. Int. J. Infect. Dis. 2011, 15, e706–e709. [Google Scholar] [CrossRef][Green Version]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef]
- Elzi, L.; Babouee, B.; Vögeli, N.; Laffer, R.; Dangel, M.; Frei, R.; Battegay, M.; Widmer, A. How to discriminate contamination from bloodstream infection due to coagulase-negative staphylococci: A prospective study with 654 patients. Clin. Microbiol. Infect. 2012, 18, E355–E361. [Google Scholar] [CrossRef]
- Downes, K.J.; Metlay, J.P.; Bell, L.M.; McGowan, K.L.; Elliott, M.R.; Shah, S.S. Polymicrobial Bloodstream Infections among Children and Adolescents with Central Venous Catheters Evaluated in Ambulatory Care. Clin. Infect. Dis. 2008, 46, 387–394. [Google Scholar] [CrossRef]
- Bonazzetti, C.; Morena, V.; Giacomelli, A.; Oreni, L.; Casalini, G.; Galimberti, L.R.; Bolis, M.; Rimoldi, M.; Ballone, E.; Colombo, R.; et al. Unexpectedly High Frequency of Enterococcal Bloodstream Infections in Coronavirus Disease 2019 Patients Admitted to an Italian ICU: An Observational Study. Crit. Care Med. 2021, 49, e31–e40. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing (EUCAST): Clinical Breakpoints-Breakpoints and Guidance. Available online: http://www.eucast.org/clinical_breakpoints/ (accessed on 15 October 2020).
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 30th ed. CLSI Supplement M100. Clinical and Laboratory Standards Institute, 2020. Available online: https://clsi.org/media/3481/m100ed30_sample.pdf (accessed on 15 October 2020).
- Woodford, N.; Ellington, M.J.; Coelho, J.M.; Turton, J.F.; Ward, M.E.; Brown, S.; Amyes, S.G.; Livermore, D.M. Multiplex PCR for genes encoding prevalent OXA carbapenemases in Acinetobacter spp. Int. J. Antimicrob. Agents 2006, 27, 351–353. [Google Scholar] [CrossRef]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef]
- Nguyen, A.T.; Pham, S.C.; Ly, A.K.; Nguyen, C.V.V.; Vu, T.T.; Ha, T.M. Overexpression of blaOXA-58 Gene Driven by ISAba3 Is Associated with Imipenem Resistance in a Clinical Acinetobacter baumannii Isolate from Vietnam. BioMed Res. Int. 2020, 2020, 7213429. [Google Scholar] [CrossRef] [PubMed]
- Seifert, H.; Dolzani, L.; Bressan, R.; van der Reijden, T.; van Strijen, B.; Stefanik, D.; Heersma, H.; Dijkshoorn, L. Standardization and interlaboratory reproducibility assessment of pulsed-field gel electrophoresis-generated fingerprints of Acinetobacter baumannii. J. Clin. Microbiol. 2005, 43, 4328–4335. [Google Scholar] [CrossRef]
- Diancourt, L.; Passet, V.; Nemec, A.; Dijkshoorn, L.; Brisse, S. The population structure of Acinetobacter baumannii: Expanding multiresistant clones from an ancestral susceptible genetic pool. PLoS ONE 2010, 7, e10034. [Google Scholar] [CrossRef] [PubMed]
- Pournaras, S.; Gogou, V.; Giannouli, M.; Dimitroulia, E.; Dafopoulou, K.; Tsakris, A.; Zarrilli, R. Single-Locus-sequence-based typing of bla OXA-51-like genes for rapid assignment of Acinetobacter baumannii clinical isolates to international clonal lineages. J. Clin. Microbiol. 2014, 52, 1653–1657. [Google Scholar] [CrossRef] [PubMed]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Vijay, S.; Bansal, N.; Rao, B.K.; Veeraraghavan, B.; Rodrigues, C.; Wattal, C.; Goyal, J.P.; Tadepalli, K.; Mathur, P.; Venkateswaran, R.; et al. Secondary infections in hospitalized COVID-19 patients: Indian experience. Infect. Drug Resist. 2021, 14, 1893–1903. [Google Scholar] [CrossRef]
- Palanisamy, N.; Vihari, N.; Meena, D.S.; Kumar, D.; Midha, N.; Tak, V.; Sharma, A.; Bohra, G.K.; Kothari, N.; Dutt, N.; et al. Clinical profile of bloodstream infections in COVID-19 patients: A retrospective cohort study. BMC Infect. Dis. 2021, 21, 933. [Google Scholar] [CrossRef]
- Kokkoris, S.; Papachatzakis, I.; Gavrielatou, E.; Ntaidou, T.; Ischaki, E.; Malachias, S.; Vrettou, C.; Nichlos, C.; Kanavou, A.; Zervakis, D.; et al. ICU-acquired bloodstream infections in critically ill patients with COVID-19. J. Hosp. Infect. 2021, 107, 95–97. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Battaglini, D.; Ball, L.; Brunetti, I.; Bruzzone, B.; Codda, G.; Crea, F.; De Maria, A.; Dentone, C.; Di Biagio, A.; et al. Bloodstream infections in critically ill patients with COVID-19. Eur. J. Clin. Investig. 2020, 50, e13319. [Google Scholar] [CrossRef]
- Elabbadi, A.; Turpin, M.; Gerotziafas, G.T.; Teulier, M.; Voiriot, G.; Fartoukh, M. Bacterial coinfection in critically ill COVID-19 patients with severe pneumonia. Infection 2021, 43, 559–562. [Google Scholar] [CrossRef]
- Chedid, M.; Waked, R.; Haddad, E.; Chetata, N.; Saliba, G.; Choucair, J. Antibiotics in treatment of COVID-19 complications: A review of frequency, indications, and efficacy. J. Infect. Public Health 2021, 14, 570–576. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, W.; Wang, Z.; Chen, H.; Tian, L.; Liu, D. Nosocomial infection among patients with COVID-19: A retrospective data analysis of 918 cases from a single center in Wuhan, China. Infect. Control Hosp. Epidemiol. 2020, 41, 982–983. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef]
- Wang, D.; Yin, Y.; Hu, C.; Liu, X.; Zhang, X.; Zhou, S.; Jian, M.; Xu, H.; Prowle, J.; Hu, B.; et al. Clinical course and outcome of 107 patients infected with the novel coronavirus, SARS-CoV-2, discharged from two hospitals in Wuhan, China. Crit. Care 2020, 24, 188. [Google Scholar] [CrossRef]
- Muntean, D.; Licker, M.; Horhat, F.; Dumitrașcu, V.; Săndesc, D.; Bedreag, O.; Dugăeșescu, D.; Coșniță, D.A.; Krasta, A.; Bădițoiu, L. Extensively drug-resistant Acinetobacter baumannii and Proteeae association in a Romanian intensive care unit: Risk factors for acquisition. Infect. Drug Resist. 2018, 11, 2187–2197. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2022–2020 Data. Available online: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-surveillance-europe-2022-2020-data (accessed on 10 March 2023).
- Paul, M.; Carrara, E.; Retamar, P.; Tängdén, T.; Bitterman, R.; Bonomo, R.A.; de Waele, J.; Daikos, G.L.; Akova, M.; Harbarth, S.; et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin. Microbiol. Infect. 2022, 28, 521–547. [Google Scholar] [CrossRef]
- Montero, A.; Ariza, J.; Corbella, X.; Doménech, A.; Cabellos, C.; Ayats, J.; Tubau, F.; Borraz, C.; Gudiol, F. Antibiotic combinations for serious infections caused by carbapenem-resistant Acinetobacter baumannii in a mouse pneumonia model. J. Antimicrob. Chemother. 2004, 54, 1085–1091. [Google Scholar] [CrossRef]
- Levin, A. Multiresistant Acinetobacter infections: A role for sulbactam combinations in overcoming an emerging worldwide problem. Clin. Microbiol. Infect. 2002, 8, 144–153. [Google Scholar] [CrossRef]
- Petrosillo, N.; Giannella, M.; Antonelli, M.; Antonini, M.; Barsic, B.; Belancic, L.; Inkaya, A.C.; De Pascale, G.; Grilli, E.; Tumbarello, M.; et al. Clinical experience of colistin-glycopeptide combination in critically ill patients infected with gram-negative bacteria. Antimicrob. Agents Chemother. 2014, 58, 851–858. [Google Scholar] [CrossRef]
- Yu, K.; Zeng, W.; Xu, Y.; Liao, W.; Xu, W.; Zhou, T.; Cao, J.; Chen, L. Bloodstream infections caused by ST2 Acinetobacter baumannii: Risk factors, antibiotic regimens, and virulence over 6 years period in China. Antimicrob. Resist. Infect. Control 2021, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Bliziotis, I.A.; Siempos, I.I. Attributable mortality of Acinetobacter baumannii infections in critically ill patients: A systematic review of matched cohort and case-control studies. Crit. Care 2006, 10, R48. [Google Scholar] [CrossRef]
- Goic-Barisic, I.; Bedenic, B.; Tonkic, M.; Katic, S.; Kalenic, S.; Punda-Polic, V. First report of molecular characterization of carbapenem-resistant Acinetobacter baumannii in different intensive care units in University Hospital Split, Croatia. J. Chemother. 2007, 19, 462–464. [Google Scholar] [CrossRef]
- Zarrilli, R.; Pournaras, S.; Giannouli, M.; Tsakris, A. Global evolution of multidrugresistant Acinetobacter baumannii clonal lineages. Int. J. Antimicrob. Agents 2013, 41, 11–19. [Google Scholar] [CrossRef]
- Karah, N.; Sundsfjord, A.; Towner, K.; Samuelsen, Ø. Insights into the global molecular epidemiology of carbapenem non-susceptible clones of Acinetobacter baumannii. Drug Resist. Update 2012, 15, 237–247. [Google Scholar] [CrossRef]
- Goić Barišić, I. Epidemiologija i rezistencija kliničkih izolata Acinetobacter baumannii u Hrvatskoj tijekom desetogodišnjeg razdoblja—Što se promijenilo? Med. Flum. 2018, 54, 268–273. [Google Scholar] [CrossRef][Green Version]
- Goic-Barisic, I.; Towner, K.; Kovacic, A.; Sisko-Kraljevic, K.; Tonkic, M.; Novak, A.; Punda-Polic, V. Outbreak in Croatia caused by a new carbapenem-resistant clone of Acinetobacter baumannii producing OXA-72 carbapenemase. J. Hosp. Infect. 2011, 77, 368–369. [Google Scholar] [CrossRef]
- Vranić-Ladavac, M.; Bedenić, B.; Minandri, F.; Ištok, M.; Bošnjak, Z.; Frančula-Zaninović, S.; Ladavac, R.; Visca, P. Carbapenem resistance and acquired class D beta-lactamases in Acinetobacter baumannii from Croatia 2009–2010. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 471–478. [Google Scholar] [CrossRef] [PubMed]
- D’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; Tarsitani, L. Post-traumatic stress symptoms in healthcare workers dealing with the COVID-19 pandemic: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 601. [Google Scholar] [CrossRef]
- Sturdy, A.; Basarab, M.; Cotter, M.; Hager, K.; Shakespeare, D.; Shah, N.; Randall, P.; Spray, D.; Arnold, A. Severe COVID-19 and healthcare-associated infections on the ICU: Time to remember the basics? J. Hosp. Infect. 2020, 105, 593–595. [Google Scholar] [CrossRef] [PubMed]
- Yap, F.H.Y.; Gomersall, C.; Fung, K.S.C.; Ho, P.L.; Ho, O.-M.; Lam, P.K.N.; Lam, D.T.C.; Lyon, D.J.; Joynt, G. Increase in methicillin-resistant staphylococcus aureus acquisition rate and change in pathogen pattern associated with an outbreak of severe acute respiratory syndrome. Clin. Infect. Dis. 2004, 39, 511–516. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | N (%) |
|---|---|
| Age, median (range), in years | 72 (89–48) |
| Male (%) | 83 (78.3) |
| Comorbidity * | |
| Without comorbidity | 28 (26.4) |
| With comorbidity | 78 (73.6) |
| Diabetes mellitus | 40 (37.7) |
| Peripheral artery disease | 22 (20.7) |
| Coronary artery disease | 19 (17.9) |
| Cardiomyopathy | 12 (11.3) |
| Neurologic disease | 11 (10.4) |
| Chronic renal insufficiency | 9 (8.5) |
| COPD | 6 (5.7) |
| Characteristics at ICU admission | |
| Duration of disease prior to admission, mean (range), in days | 10 (1–36) |
| Bilateral pneumonia | 99 (93.4) |
| PaO2/FiO2 (median) | 67.9 |
| SOFA score (median) | 4 |
| APACHE II score (median) | 13 |
| SAPS II score (median) | 30.5 |
| Treatment and outcome | |
| Antiviral therapy | 21 (19.8) |
| Immunomodulatory therapy | 65 (61.3) |
| ATB treatment prior to BSI: | 99 (93.4) |
| Ceftriaxone | 57 (53.8) |
| Meropenem | 24 (22.6) |
| Piperacillin/tazobactam | 18 (16.9) |
| Amoxicillin/clavulanic acid | 12 (11.3) |
| Duration of ATB treatment for BSI (median days, mean) | 6 (8.3) |
| ATB treatment of BSI | |
| Colistin monotherapy | 47 (44.3) |
| Colistin in combination with other antibiotics | 29 (27.3) |
| ATB therapy not including colistin | 6 (5.7) |
| Outcome | |
| Discharged from hospital | 15 (14.2) |
| Fatal outcome in ICU | 91 (85.8) |
| Antibiotic | Proportion of Resistant Isolates N (%) |
|---|---|
| Imipenem | 112 (100.0) |
| Meropenem | 112 (100.0) |
| Ciprofloxacin | 112 (100.0) |
| Gentamicin | 111 (99.1) |
| Amikacin | 100 (89.3) |
| Trimethoprim/sulfamethoxazole | 43 (38.4) |
| Ampicillin/sulbactam | 11 (9.8) |
| Colistin * | 4 (3.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrović, K.; Škrobo, T.; Selec, K.; Jelić, M.; Čivljak, R.; Peršec, J.; Sakan, S.; Bušić, N.; Mihelčić, A.; Hleb, S.; et al. Healthcare-Associated Bloodstream Infections Due to Multidrug-Resistant Acinetobacter baumannii in COVID-19 Intensive Care Unit: A Single-Center Retrospective Study. Microorganisms 2023, 11, 774. https://doi.org/10.3390/microorganisms11030774
Dobrović K, Škrobo T, Selec K, Jelić M, Čivljak R, Peršec J, Sakan S, Bušić N, Mihelčić A, Hleb S, et al. Healthcare-Associated Bloodstream Infections Due to Multidrug-Resistant Acinetobacter baumannii in COVID-19 Intensive Care Unit: A Single-Center Retrospective Study. Microorganisms. 2023; 11(3):774. https://doi.org/10.3390/microorganisms11030774
Chicago/Turabian StyleDobrović, Karolina, Tea Škrobo, Katarina Selec, Marko Jelić, Rok Čivljak, Jasminka Peršec, Sanja Sakan, Nikolina Bušić, Antonija Mihelčić, Sonja Hleb, and et al. 2023. "Healthcare-Associated Bloodstream Infections Due to Multidrug-Resistant Acinetobacter baumannii in COVID-19 Intensive Care Unit: A Single-Center Retrospective Study" Microorganisms 11, no. 3: 774. https://doi.org/10.3390/microorganisms11030774
APA StyleDobrović, K., Škrobo, T., Selec, K., Jelić, M., Čivljak, R., Peršec, J., Sakan, S., Bušić, N., Mihelčić, A., Hleb, S., & Andrašević, A. T. (2023). Healthcare-Associated Bloodstream Infections Due to Multidrug-Resistant Acinetobacter baumannii in COVID-19 Intensive Care Unit: A Single-Center Retrospective Study. Microorganisms, 11(3), 774. https://doi.org/10.3390/microorganisms11030774