
Impact of COVID-19 Countermeasures on Pediatric Infections

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
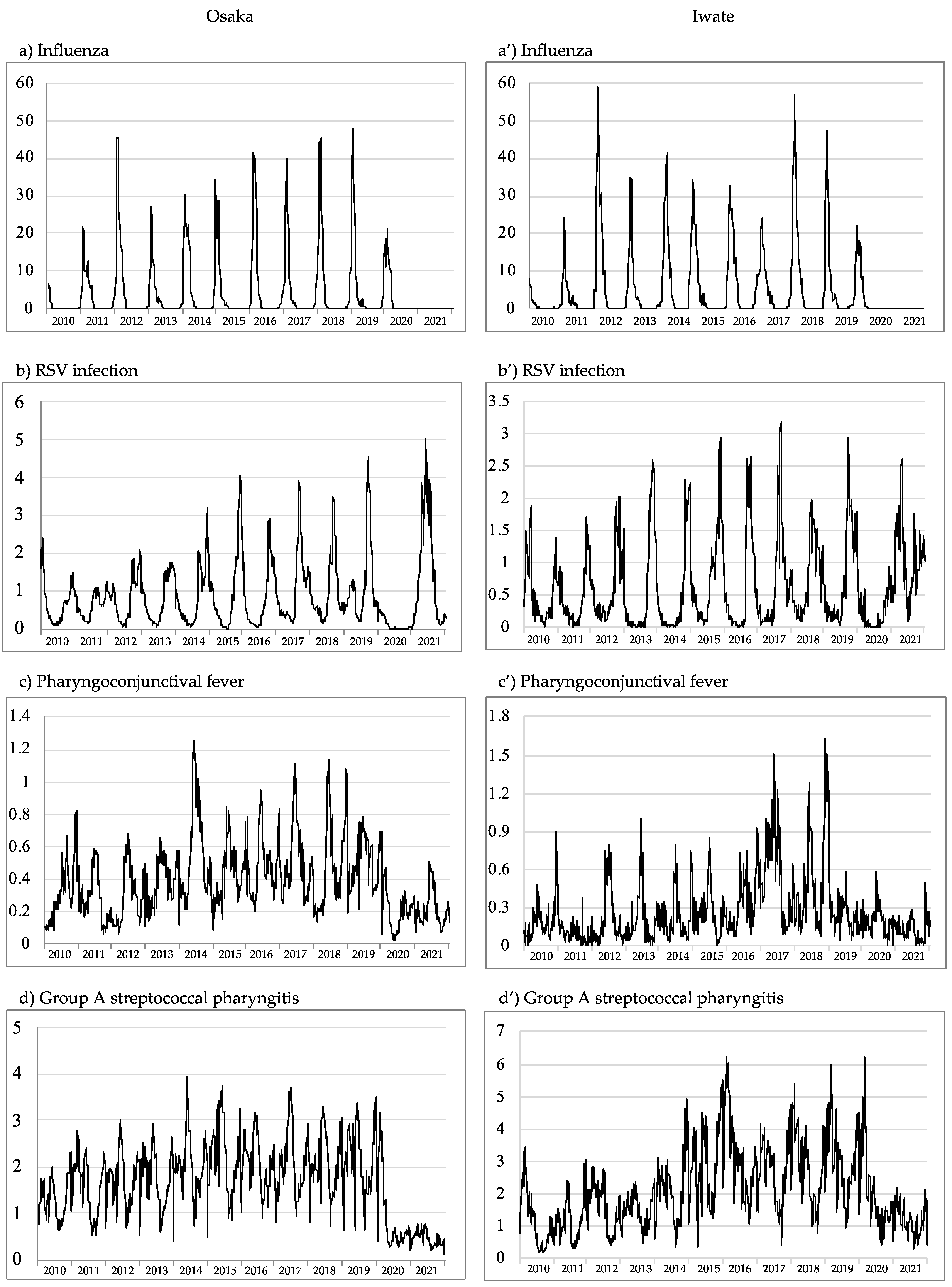
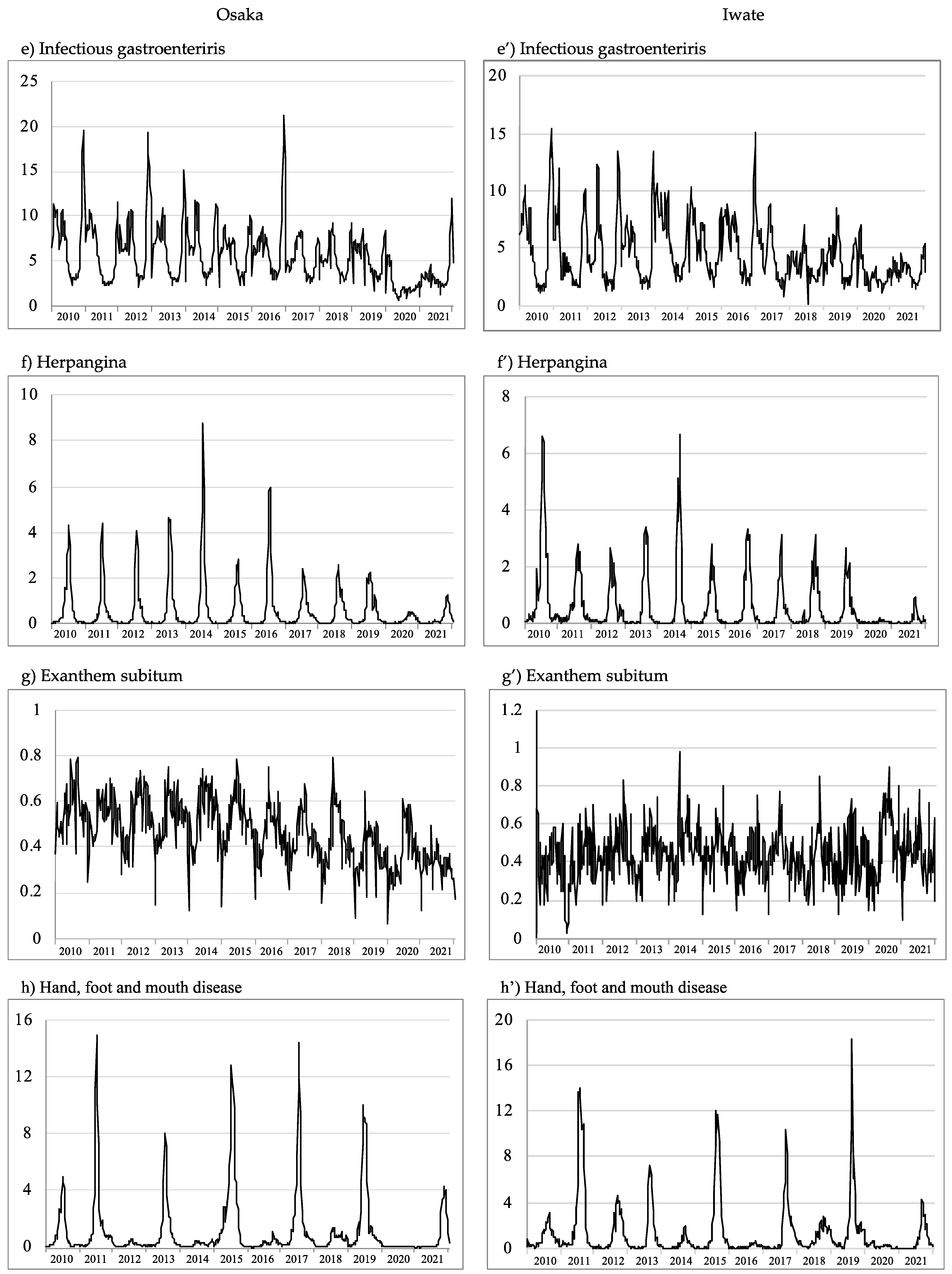
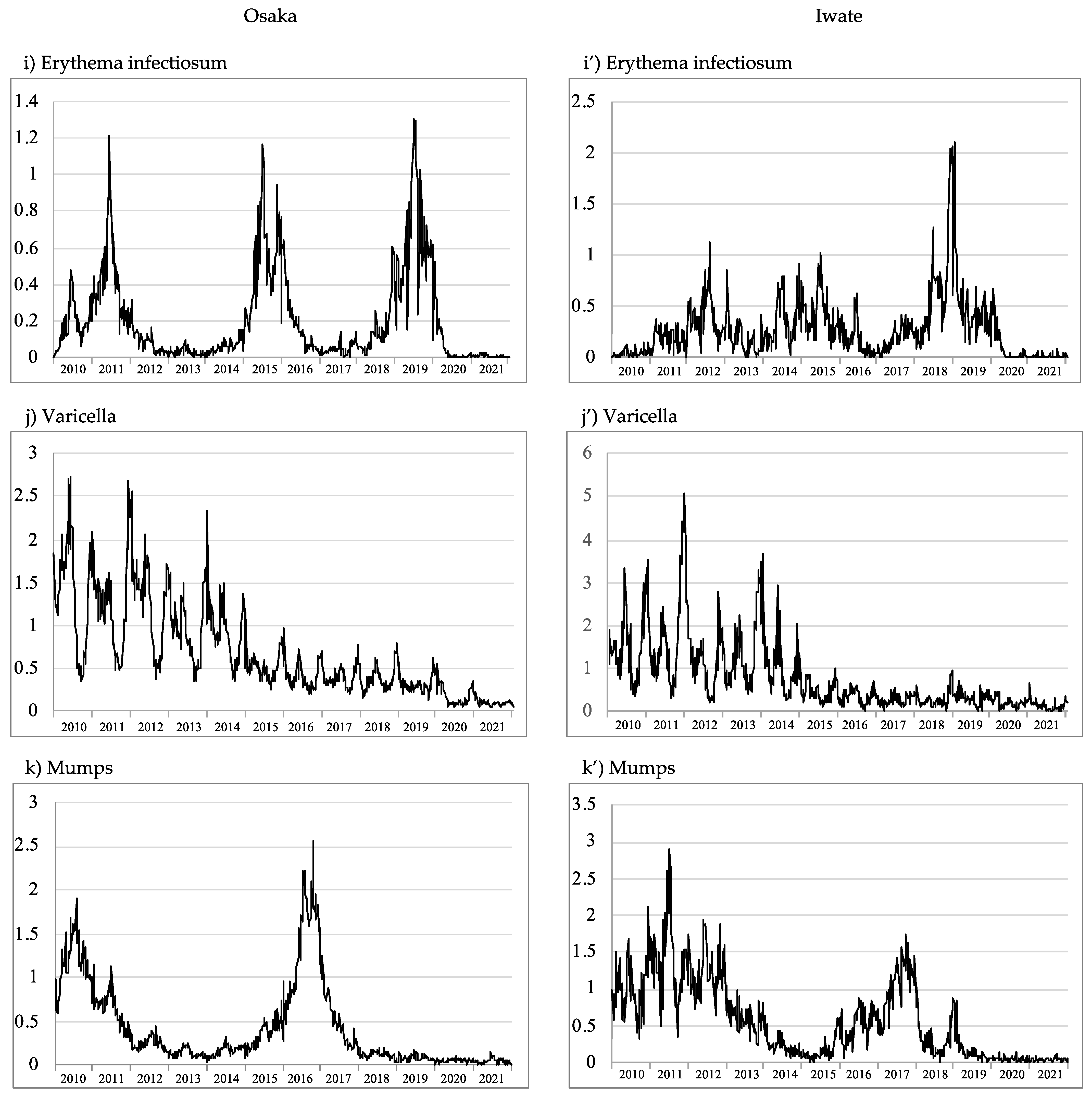
3.1. General Trends of Pediatric Infections in Osaka and Iwate before the COVID-19 Pandemic
3.2. Pediatric Infections during the COVID-19 Pandemic in Osaka and Iwate
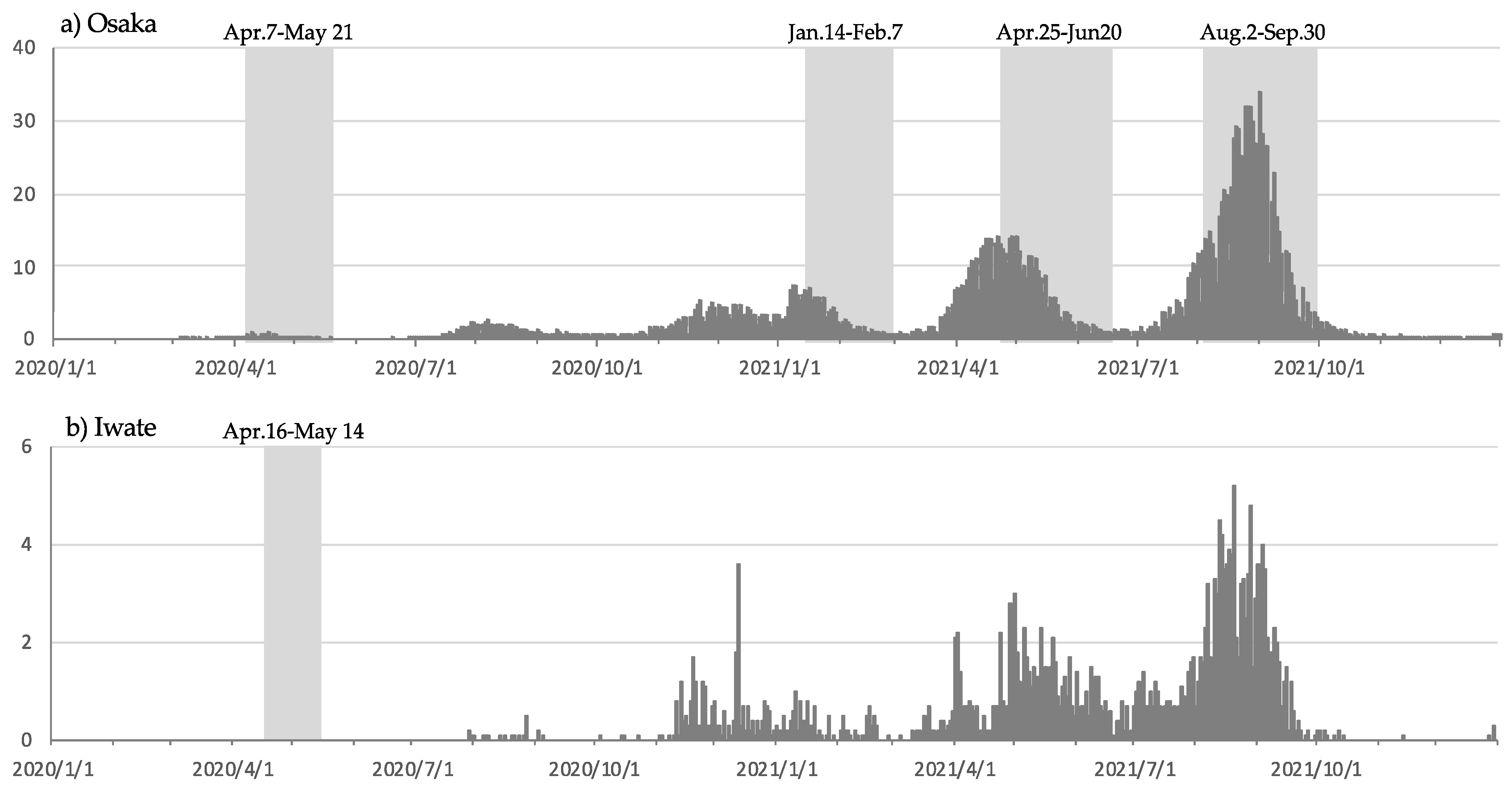
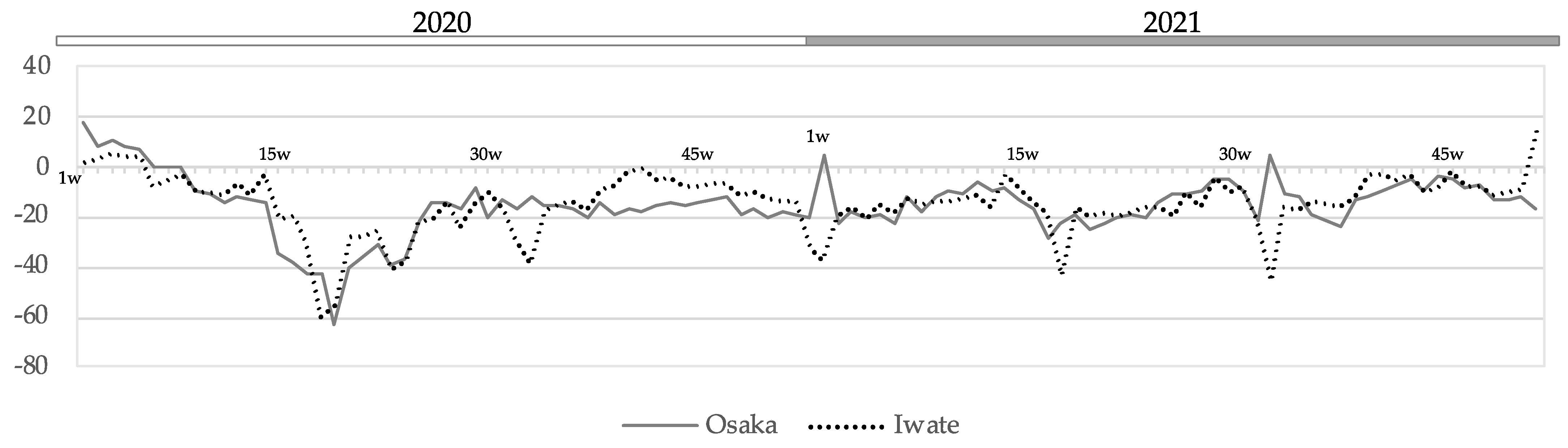
3.2.1. Human Mobility Flow and Infectious Diseases during the Mild Lockdown
3.2.2. Pediatric Infections during the COVID-19 Pandemic and Their Comparison with the 5-Week Moving Average over the Past 5 Years
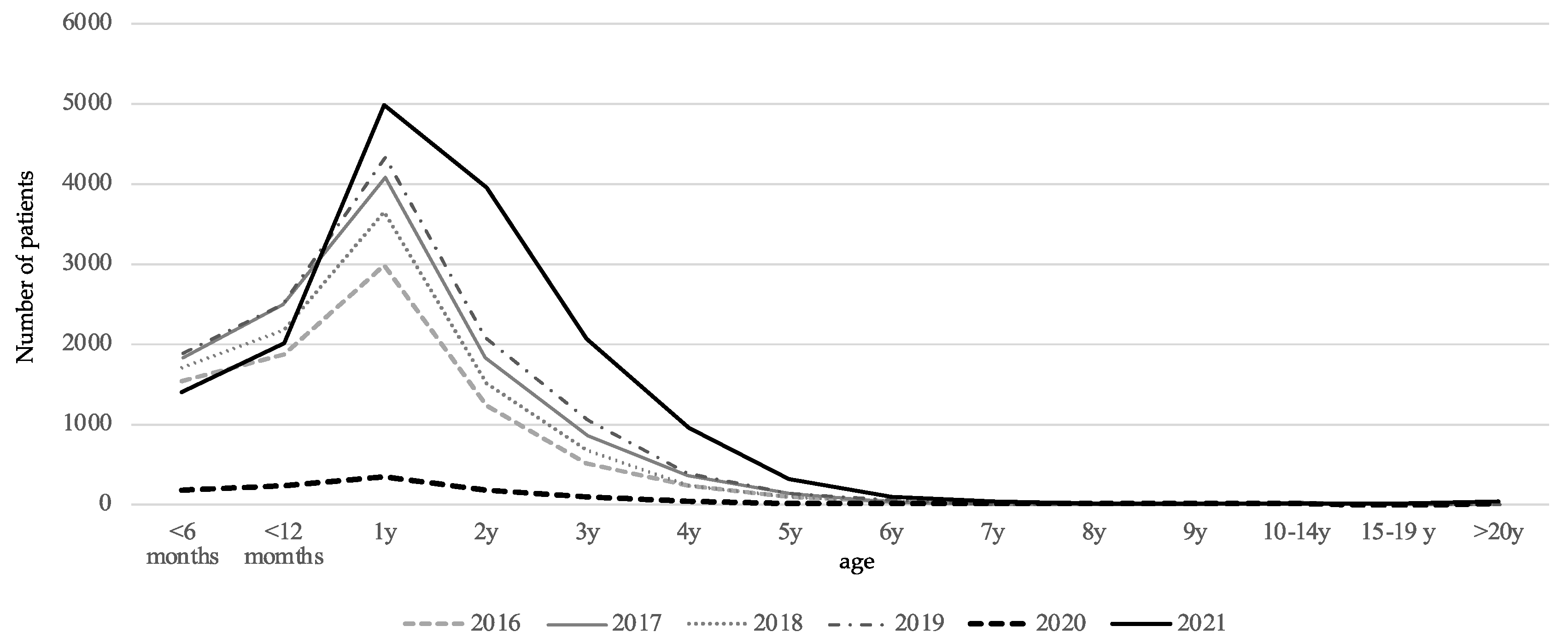
3.3. Analysis of RSV Infections by Age Group
4. Discussion
5. Conclusions
References
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| January | February | March | April | May | June | July | August | September | October | November | December | Total Number of Patients in Norovirus FB | Total Number of FB Patients | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2010 | 14 | 32 | 146 | 0 | 34 | 0 | 0 | 0 | 0 | 0 | 4 | 164 | 394 | 1158 |
| 2011 | 81 | 20 | 0 | 14 | 0 | 30 | 3 | 0 | 118 | 0 | 54 | 12 | 332 | 1951 |
| 2012 | 52 | 38 | 101 | 15 | 0 | 0 | 7 | 0 | 0 | 0 | 187 | 167 | 567 | 877 |
| 2013 | 61 | 10 | 120 | 162 | 80 | 0 | 0 | 0 | 0 | 0 | 0 | 164 | 597 | 953 |
| 2014 | 84 | 60 | 19 | 0 | 0 | 0 | 4 | 0 | 0 | 0 | 3 | 40 | 210 | 742 |
| 2015 | 382 | 81 | 58 | 35 | 0 | 27 | 32 | 0 | 0 | 0 | 17 | 9 | 641 | 1191 |
| 2016 | 37 | 13 | 20 | 31 | 0 | 10 | 0 | 0 | 19 | 0 | 76 | 88 | 294 | 1179 |
| 2017 | 60 | 103 | 77 | 0 | 0 | 59 | 0 | 0 | 0 | 0 | 0 | 32 | 331 | 821 |
| 2018 | 31 | 23 | 31 | 27 | 19 | 0 | 0 | 0 | 0 | 0 | 43 | 0 | 174 | 500 |
| 2019 | 5 | 50 | 229 | 154 | 12 | 0 | 0 | 0 | 0 | 0 | 11 | 0 | 461 | 897 |
| 2020 | 0 | 0 | 14 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 14 | 587 |
| 2021 | 0 | 30 | 0 | 7 | 0 | 26 | 0 | 0 | 0 | 0 | 24 | 21 | 108 | 322 |
References
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef]
- Hui, D.S.; Azhar, E.I.; Madani, T.A.; Ntoumi, F.; Kock, R.; Dar, O.; Ippolito, G.; McHugh, T.D.; Memish, Z.A.; Drosten, C.; et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int. J. Infect. Dis. 2020, 91, 264–266. [Google Scholar] [CrossRef] [PubMed]
- Olsen, S.J.; Azziz-Baumgartner, E.; Budd, A.P.; Brammer, L.; Sullivan, S.; Pineda, R.F.; Cohen, C.; Fry, A.M. Decreased Influenza activity during the COVID-19 pandemic—United States, Australia, Chile, and South Africa, 2020. Am. J. Transplamt. 2020, 20, 3681–3685. [Google Scholar] [CrossRef] [PubMed]
- Stefanoff, P.; Løvlie, A.L.; Elstrøm, P.; Macdonald, E.A. Reporting of notifiable infectious diseases during the COVID-19 response. Tidsskr. Nor. Laegeforen. 2020, 140. [Google Scholar] [CrossRef]
- Lennon, R.P.; Griffin, C.; Miller, E.L.; Dong, H.; Rabago, D.; Zgierska, A.E. Norovirus infections drop 49% in the United States with strict COVID-19 public health Interventions. Acta Med. Acad. 2020, 49, 278–280. [Google Scholar] [CrossRef] [PubMed]
- Hotham, M. Potential future implications of the COVID-19 pandemic on Norovirus infections in England. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Zhan, C.; Yuan, T.; Sun, Y.; Wang, W.; Chen, L. Impact of the COVID-19 pandemic on infectious disease hospitalizations of neonates at a tertiary academic hospital: A cross-sectional study. BMC Infect. Dis. 2022, 22, 206. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, H.; Smith, C.M.; Lee Ddo, H.; Hirst, R.A.; Easton, A.J.; O’Callaghan, C. Evidence of respiratory syncytial virus spread by aerosol. Time to revisit infection control strategies? Am. J. Respir. Crit. Care Med. 2016, 194, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Otomaru, H.; Kamigaki, T.; Tamaki, R.; Okamoto, M.; Alday, P.P.; Tan, A.G.; Manalo, J.I.; Segubre-Mercado, E.; Inobaya, M.T.; Tallo, V.; et al. Transmission of Respiratory Syncytial Virus Among Children Under 5 Years in Households of Rural Communities, the Philippines. Open Forum Infect. Dis. 2019, 6, ofz045. [Google Scholar] [CrossRef] [PubMed]
- Reis, J.; Shaman, J. Retrospective Parameter estimation and forecast of respiratory syncytial virus in the United States. PLoS Comput. Biol. 2016, 12, e105133. [Google Scholar] [CrossRef] [PubMed]
- Biggerstaff, M.; Cauchemez, S.; Reed, C.; Gambhir, M.; Finelli, L. Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: A systematic review of the literature. BMC Infect. Dis. 2014, 14, 480. [Google Scholar] [CrossRef]
- Chowell, G.; Miller, M.A.; Viboud, C. Seasonal influenza in the United States, France, and Australia: Transmission and prospects for control. Epidemiol. Infect. 2008, 136, 852–864. [Google Scholar] [CrossRef] [PubMed]





| Influenza | RSV Infection (RSV) | Pharyngoconjunc-Tival Fever (PCF) | Group A Streptococcal Pharyngitis (GASP) | Infectious Gastroenteritis (GE) | Herpangina | Exanthem Subitem (ES) | Hand, Foot and Mouth Disease (HFMD) | Erythema Infectiosum (EI) | Varicella | Mumps | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| pathogen | influenza virus | Respiratory syncytial virus | Adenovirus | Streptococcus pyogenes | Rotavirus A, Norovirus etc. | Coxsackie-virus A | Human herpes virus 6, | Enterovirus A (mainly CA16, EV71) | Human parvovirus B19 | varicella zoster virus | Mumps virus |
| (mainly 3,4,7) | Human herpes virus 7 | ||||||||||
| transmission | droplet or contact infection | droplet or contact infection | droplet or contact infection | droplet or contact infection | fecol-oral, contact infection, foodborn | fecol-oral, respiratory route | droplet or contact infection | fecol-oral, respiratory route | droplet or contact infection | droplet or contact infection, airborn | via respiratory droplets and saliva |
| target population of the surveillance | All populations | <15 years old | <15 years old | <15 years old | <15 years old (mainly) | <15 years old | <15 years old | <15 years old | <15 years old | <15 years old | <15 years old |
| predominant age | <10 | <1 years old | <5 years old (60%) | 5 to 9 years old | Not particular | <5 years old (90%) | 5 to 9 yars old | <5 years old (90%) | <1 years old | <9 years old | 5 to 9 yars old |
| seasonality in Japan | January–Februart | November-January | July–August | April-July & October–December | November–January (Norovirus), | July–August | June–July | July | none | December–July | none |
| April (Rotavirus) | |||||||||||
| periodicity | every year | every year | every year | every year | every year | every year | every 3–4 years | every other year | none | every year | every 5–6 years |
| vaccination | routine: elderly | routine: Rotavirus A vaccine from October 2020 | routine: to 1 years old from October 2014 | voluntary |
| 2020 (15–52 w) | 2021 | |||
| Osaka | Iwate | Osaka | Iwate | |
| Influenza | 0.0053 | p< 0.001 | p < 0.001 | p < 0.001 |
| RSV infection | p < 0.001 | p < 0.001 | 0.02061 | 0.01278 |
| Pharyngoconjunctival fever | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Group A streptococcal pharyngitis | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Infectious gastroenteriris | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| Herpangina | p < 0.001 | p < 0.001 | 0.0052 | p < 0.001 |
| Exanthem subitum | 0.002433 | p < 0.001 * | p < 0.001 | 0.19267 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakon, N.; Takahashi, T.; Yoshida, T.; Shirai, T.; Komano, J. Impact of COVID-19 Countermeasures on Pediatric Infections. Microorganisms 2022, 10, 1947. https://doi.org/10.3390/microorganisms10101947
Sakon N, Takahashi T, Yoshida T, Shirai T, Komano J. Impact of COVID-19 Countermeasures on Pediatric Infections. Microorganisms. 2022; 10(10):1947. https://doi.org/10.3390/microorganisms10101947
Chicago/Turabian StyleSakon, Naomi, Tomoko Takahashi, Toshiaki Yoshida, Tatsuya Shirai, and Jun Komano. 2022. "Impact of COVID-19 Countermeasures on Pediatric Infections" Microorganisms 10, no. 10: 1947. https://doi.org/10.3390/microorganisms10101947
APA StyleSakon, N., Takahashi, T., Yoshida, T., Shirai, T., & Komano, J. (2022). Impact of COVID-19 Countermeasures on Pediatric Infections. Microorganisms, 10(10), 1947. https://doi.org/10.3390/microorganisms10101947