
Human Colonic Microbiota and Short-Term Postoperative Outcomes in Colorectal Cancer Patients: A Pilot Study


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Samples Collection
2.3. DNA Extraction
2.4. DNA Sequencing and Data Analysis
2.5. Statistical Analysis
3. Results
3.1. Prokaryote DNA Characteristics
3.2. Metagenomic Analysis
3.2.1. General Analysis
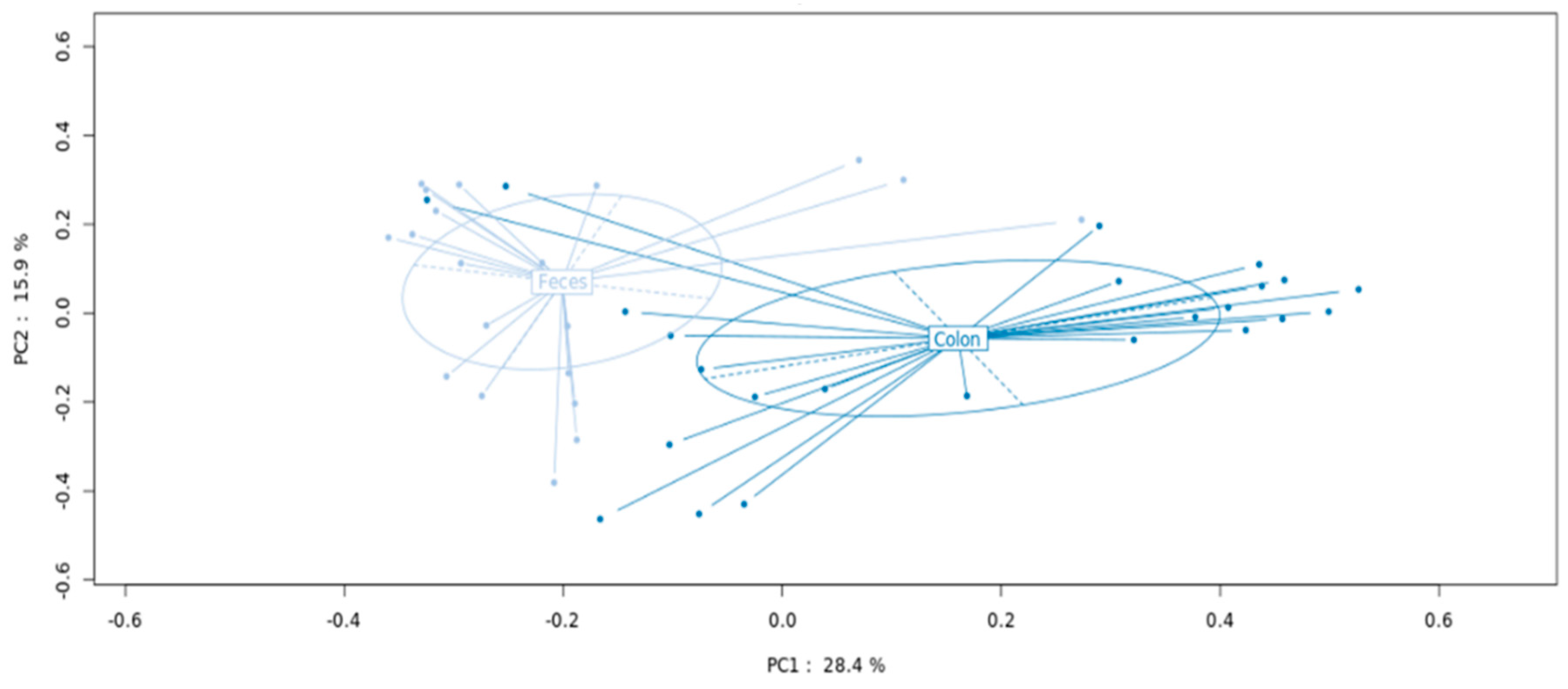
3.2.2. MAM versus LM Signatures
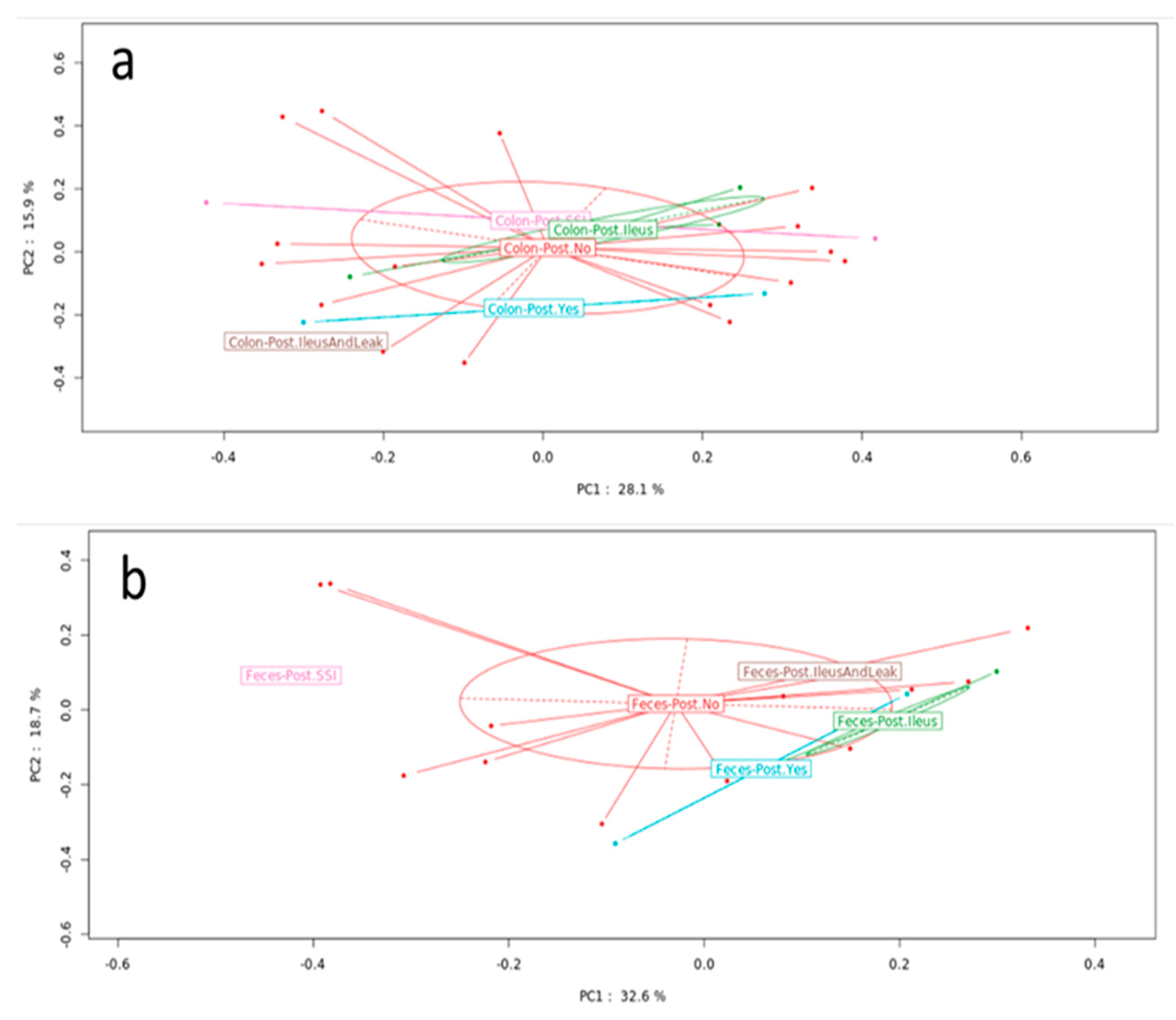
3.2.3. Microbiota Analyses According to the Presence of Postoperative Complications
3.2.4. Effect of Neoadjuvant Therapy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kulu, Y.; Tarantio, I.; Warschkow, R.; Kny, S.; Schneider, M.; Schmied, B.M.; Büchler, M.W.; Ulrich, A. Anastomotic leakage is associated with impaired overall and disease-free survival after curative rectal cancer resection: A propensity score analysis. Ann. Surg. Oncol. 2015, 22, 2059–2067. [Google Scholar] [CrossRef]
- Alverdy, J.C. Microbiome medicine: This changes everything. J. Am. Coll. Surg. 2018, 226, 719–729. [Google Scholar] [CrossRef] [Green Version]
- Meyer, J.; Naiken, S.; Christou, N.; Liot, E.; Toso, C.; Buchs, N.C.; Ris, F. Reducing anastomotic leak in colorectal surgery: The old dogmas and the new challenges. World J. Gastroenterol. 2019, 25, 5017–5025. [Google Scholar] [CrossRef] [PubMed]
- Sciuto, A.; Merola, G.; De Palma, G.D.; Sodo, M.; Pirozzi, F.; Bracale, U.M.; Bracale, U. Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J. Gastroenterol. 2018, 24, 2247–2260. [Google Scholar] [CrossRef] [PubMed]
- Krezalek, M.A.; Hyoju, S.; Zaborin, A.; Okafor, E.; Chandrasekar, L.; Bindokas, V.; Guyton, K.; Montgomery, C.P.; Daum, R.S.; Zaborina, O.; et al. Can methicillin-resistant staphylococcus aureus silently travel from the gut to the wound and cause postoperative infection? Modeling the “trojan horse hypothesis”. Ann. Surg. 2018, 267, 749–758. [Google Scholar] [CrossRef]
- Pohl, J.M.; Gutweiler, S.; Thiebes, S.; Volke, J.K.; Klein-Hitpass, L.; Zwanziger, D.; Gunzer, M.; Jung, S.; Agace, W.W.; Kurts, C.; et al. Irf4-dependent cd103(+)cd11b(+) dendritic cells and the intestinal microbiome regulate monocyte and macrophage activation and intestinal peristalsis in postoperative ileus. Gut 2017, 66, 2110–2120. [Google Scholar] [CrossRef] [Green Version]
- Bachmann, R.; Leonard, D.; Delzenne, N.; Kartheuser, A.; Cani, P.D. Novel insight into the role of microbiota in colorectal surgery. Gut 2017, 66, 738–749. [Google Scholar] [CrossRef]
- van Praagh, J.B.; de Goffau, M.C.; Bakker, I.S.; van Goor, H.; Harmsen, H.J.M.; Olinga, P.; Havenga, K. Mucus microbiome of anastomotic tissue during surgery has predictive value for colorectal anastomotic leakage. Ann. Surg. 2019, 269, 911–916. [Google Scholar] [CrossRef]
- Palmisano, S.; Campisciano, G.; Iacuzzo, C.; Bonadio, L.; Zucca, A.; Cosola, D.; Comar, M.; de Manzini, N. Role of preoperative gut microbiota on colorectal anastomotic leakage: Preliminary results. Updates Surg. 2020, 72, 1013–1022. [Google Scholar] [CrossRef]
- Jin, Y.; Geng, R.; Liu, Y.; Liu, L.; Jin, X.; Zhao, F.; Feng, J.; Wei, Y. Prediction of postoperative ileus in patients with colorectal cancer by preoperative gut microbiota. Front. Oncol. 2020, 10, 526009. [Google Scholar] [CrossRef] [PubMed]
- Lauka, L.; Reitano, E.; Carra, M.C.; Gaiani, F.; Gavriilidis, P.; Brunetti, F.; de’Angelis, G.L.; Sobhani, I.; de’Angelis, N. Role of the intestinal microbiome in colorectal cancer surgery outcomes. World J. Surg. Oncol. 2019, 17, 204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ringel, Y.; Maharshak, N.; Ringel-Kulka, T.; Wolber, E.A.; Sartor, R.B.; Carroll, I.M. High throughput sequencing reveals distinct microbial populations within the mucosal and luminal niches in healthy individuals. Gut Microbes 2015, 6, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Krarup, P.M.; Nordholm-Carstensen, A.; Jorgensen, L.N.; Harling, H. Anastomotic leak increases distant recurrence and long-term mortality after curative resection for colonic cancer: A nationwide cohort study. Ann. Surg. 2014, 259, 930–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Guidelines for the Prevention of Surgical Site Infection, 2nd ed.; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Rahbari, N.N.; Weitz, J.; Hohenberger, W.; Heald, R.J.; Moran, B.; Ulrich, A.; Holm, T.; Wong, W.D.; Tiret, E.; Moriya, Y.; et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the international study group of rectal cancer. Surgery 2010, 147, 339–351. [Google Scholar] [CrossRef] [PubMed]
- Bergsten, E.; Mestivier, D.; Sobhani, I. The limits and avoidance of biases in metagenomic analyses of human fecal microbiota. Microorganisms 2020, 8, 1954. [Google Scholar] [CrossRef] [PubMed]
- Magoč, T.; Salzberg, S.L. Flash: Fast length adjustment of short reads to improve genome assemblies. Bioinformatics 2011, 27, 2957–2963. [Google Scholar] [CrossRef]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef] [Green Version]
- Callahan, B.J.; McMurdie, P.J.; Rosen, M.J.; Han, A.W.; Johnson, A.J.; Holmes, S.P. Dada2: High-resolution sample inference from illumina amplicon data. Nat. Methods 2016, 13, 581–583. [Google Scholar] [CrossRef] [Green Version]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The silva ribosomal rna gene database project: Improved data processing and web-based tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef] [PubMed]
- Volant, S.; Lechat, P.; Woringer, P.; Motreff, L.; Campagne, P.; Malabat, C.; Kennedy, S.; Ghozlane, A. Shaman: A user-friendly website for metataxonomic analysis from raw reads to statistical analysis. BMC Bioinform. 2020, 21, 345. [Google Scholar] [CrossRef]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for rna-seq data with deseq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakkis, Z.; Manceau, G.; Bridoux, V.; Brouquet, A.; Kirzin, S.; Maggiori, L.; de Chaisemartin, C.; Lefevre, J.H.; Panis, Y. Management of rectal cancer: The 2016 french guidelines. Colorectal Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2017, 19, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Phelip, J.M.; Tougeron, D.; Léonard, D.; Benhaim, L.; Desolneux, G.; Dupré, A.; Michel, P.; Penna, C.; Tournigand, C.; Louvet, C.; et al. Metastatic colorectal cancer (mcrc): French intergroup clinical practice guidelines for diagnosis, treatments and follow-up (snfge, ffcd, gercor, unicancer, sfcd, sfed, sfro, sfr). Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2019, 51, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Goel, N.; Nadler, A.; Reddy, S.; Hoffman, J.P.; Pitt, H.A. Biliary microbiome in pancreatic cancer: Alterations with neoadjuvant therapy. HPB Off. J. Int. Hepato. Pancreato. Biliary Assoc. 2019, 21, 1753–1760. [Google Scholar] [CrossRef]
- Montassier, E.; Gastinne, T.; Vangay, P.; Al-Ghalith, G.A.; Bruley des Varannes, S.; Massart, S.; Moreau, P.; Potel, G.; de La Cochetière, M.F.; Batard, E.; et al. Chemotherapy-driven dysbiosis in the intestinal microbiome. Aliment. Pharmacol. Ther. 2015, 42, 515–528. [Google Scholar] [CrossRef] [PubMed]
- Scarborough, J.E.; Mantyh, C.R.; Sun, Z.; Migaly, J. Combined mechanical and oral antibiotic bowel preparation reduces incisional surgical site infection and anastomotic leak rates after elective colorectal resection: An analysis of colectomy-targeted acs nsqip. Ann. Surg 2015, 262, 331–337. [Google Scholar] [CrossRef]
- Mima, K.; Sakamoto, Y.; Kosumi, K.; Ogata, Y.; Miyake, K.; Hiyoshi, Y.; Ishimoto, T.; Iwatsuki, M.; Baba, Y.; Iwagami, S.; et al. Mucosal cancer-associated microbes and anastomotic leakage after resection of colorectal carcinoma. Surg. Oncol. 2020, 32, 63–68. [Google Scholar] [CrossRef]
- Nagata, N.; Tohya, M.; Fukuda, S.; Suda, W.; Nishijima, S.; Takeuchi, F.; Ohsugi, M.; Tsujimoto, T.; Nakamura, T.; Shimomura, A.; et al. Effects of bowel preparation on the human gut microbiome and metabolome. Sci. Rep. 2019, 9, 4042. [Google Scholar] [CrossRef]
- Toh, J.W.T.; Phan, K.; Hitos, K.; Pathma-Nathan, N.; El-Khoury, T.; Richardson, A.J.; Morgan, G.; Engel, A.; Ctercteko, G. Association of mechanical bowel preparation and oral antibiotics before elective colorectal surgery with surgical site infection: A network meta-analysis. JAMA Netw. Open 2018, 1, e183226. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 25) | Complications (n = 8) | No Complications (n = 17) | p Value | |
|---|---|---|---|---|
| Demographic and clinical variables | ||||
| Gender (male/female, n (%)) | 14 (56)/11 (44) | 7/1 | 7/10 | 0.042 |
| Age (years, mean (SD)) | 68.64 (±11.64) | 69.63 (±8.31) | 68.18 (±12.89) | 0.977 |
| BMI ≥ 30 (kg/m2, n (%)) | 6 (24) | 2 | 4 | 0.370 |
| Weight loss $ (n (%)) | 3 (12) | 1 | 2 | 1 |
| ASA score (n (%)) | ||||
| 16 (64) | 2 | 14 | 0.01 |
| 9 (36) | 6 | 3 | |
| CCI scores (n(%)) | ||||
| 3 (12) 5 (20) 4 (16) 13 (52) | 0 1 3 4 | 3 4 1 9 | 0.374 |
| Previous abdominal operations (n (%)) | 11 (44) | 2 | 9 | 0.234 |
| Drug use with potential impact on microbiota * (n (%)) | 6 (24) | 4 | 2 | 0.059 |
| Cancer location (n (%)) | 0.941 | |||
| 3 (12) | 1 | 2 | |
| 4 (16) | 1 | 3 | |
| 2 (8) | 1 | 1 | |
| 16 (64) | 5 | 11 | |
| Synchronous metastases (n (%)) | 3 (12) | 1 | 2 | 1 |
Neoadjuvant therapy (n (%))
| 14 (56) 11 (44) 1 (4) | 4 3 0 | 10 8 1 | 1 |
| 2 (8) | 1 | 1 | |
| 11 (44) | 4 | 7 | |
| Prealbumin levels (ng/L, mean (SD)) | 278 (±68.87) | 277.75 (±41.61) | 277.6 (±79.68) | 0.975 |
| Operative variables | ||||
| Type of anastomosis (n (%)) | 0.948 | |||
| 15 (60) | 5 | 10 | |
| 6 (24) | 2 | 4 | |
| 4 (16) | 1 | 3 | |
| Ileostomy (n (%)) | 11 (44) | 4 | 7 | 1 |
| Surgical approach (n (%)) | 0.637 | |||
| 17 (68) | 5 | 12 | |
| 7 (28) | 3 | 4 | |
| 1 (2) | 0 | 1 | |
| Conversion to open (n (%)) | 0 | 0 | 0 | NA |
| Operative time (min, mean (SD)) | 357.4 (±91.44) | 383.75 (±96.23) | 345 (±86.36) | 0.344 |
| Transfusions (n (%)) | 0 | 0 | 0 | NA |
| All Patients (n = 25) | Complications (n = 8) | No Complications (n = 17) | p Value | |
|---|---|---|---|---|
| Postoperative variables | ||||
| Overall complications (patients, n (%)) | 8 (32) | 8 | 0 | NA |
| 4 | |||
| 2 | |||
| 1 | |||
| 1 | |||
| 2 | |||
| 2 | |||
| 1 | ||||
| Clavien–Dindo ≥3 | 2 | 2 | 0 | NA |
| Mortality | 0 | 0 | 0 | NA |
| Hospital stay (days, mean (SD)) | 11.36 (±4.75) | 15.75 (±4.15) | 9.29 (±3.46) | 0.01 |
| Reoperation | 0 | 0 | 0 | NA |
| Readmission (n (%)) | 2 (8) | 2 | 0 | 0.547 |
| Genus | Base Mean | log2 Fold Change | Adjusted p Value |
|---|---|---|---|
| Significantly more abundant in MAM | |||
| Escherichia/Shigella | 42,410.3 | 2.534 | 0.005 |
| Streptococcus | 13,446.3 | 2.522 | 0.001 |
| Enterococcus | 11,135.19 | 4.805 | 0.000003 |
| Granulicatella | 783.79 | 4.59 | 8.567−7 |
| Actinomyces | 111.03 | 2.071 | 0.04989 |
| Significantly more abundant in LM | |||
| Bacteroides | 25,946.21 | −1.26 | 0.008 |
| Alistipes | 2395.64 | −3.415 | 5.466−14 |
| Barnesiella | 959.38 | −2.766 | 0.00069 |
| Odoribacter | 587.57 | −1.611 | 0.041 |
| Phascolarctobacterium | 499.36 | −2.987 | 0.001 |
| Bilophila | 344.62 | −2.577 | 0.0008 |
| Butyricimonas | 341.26 | −2.666 | 0.003 |
| Acidaminococcus | 277.84 | −3.423 | 0.024 |
| Desulfovibrio | 272.76 | −3.694 | 0.000013 |
| Paraprevotella | 241.54 | −3.499 | 0.023 |
| Succiniclasticum | 166.3 | −4.527 | 0.041 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauka, L.; Sobhani, I.; Brunetti, F.; Mestivier, D.; de’Angelis, N. Human Colonic Microbiota and Short-Term Postoperative Outcomes in Colorectal Cancer Patients: A Pilot Study. Microorganisms 2022, 10, 41. https://doi.org/10.3390/microorganisms10010041
Lauka L, Sobhani I, Brunetti F, Mestivier D, de’Angelis N. Human Colonic Microbiota and Short-Term Postoperative Outcomes in Colorectal Cancer Patients: A Pilot Study. Microorganisms. 2022; 10(1):41. https://doi.org/10.3390/microorganisms10010041
Chicago/Turabian StyleLauka, Lelde, Iradj Sobhani, Francesco Brunetti, Denis Mestivier, and Nicola de’Angelis. 2022. "Human Colonic Microbiota and Short-Term Postoperative Outcomes in Colorectal Cancer Patients: A Pilot Study" Microorganisms 10, no. 1: 41. https://doi.org/10.3390/microorganisms10010041
APA StyleLauka, L., Sobhani, I., Brunetti, F., Mestivier, D., & de’Angelis, N. (2022). Human Colonic Microbiota and Short-Term Postoperative Outcomes in Colorectal Cancer Patients: A Pilot Study. Microorganisms, 10(1), 41. https://doi.org/10.3390/microorganisms10010041