
Oral Bacterial Microbiota in Digestive Cancer Patients: A Systematic Review

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Development and Literature Search
- Population: adult patients with a diagnosis of digestive cancer (all types of cancers located in the digestive apparatus).
- Intervention: analysis of oral microbiota composition and/or oral microbiome with or without a concomitant oral/periodontal examination. No restriction was applied for the type of microbiological technique used to sample and analyze the oral microbiota/microbiome, which include culture-dependent and genome sequencing methods.
- Comparison(s): adult patients without cancer.
- Outcome(s): oral microbiota composition (quality and quantity of bacterial species and pathogens related to oral diseases, particularly periodontitis).
- Study designs: All types of descriptive (case series, cross-sectional) and analytic studies (cohort, case-control, clinical trial) estimating the magnitude of the association between oral microbiota dysbiosis and digestive cancers.
2.2. Data Extraction
2.3. Study Quality Assessment and Risk of Bias
3. Results
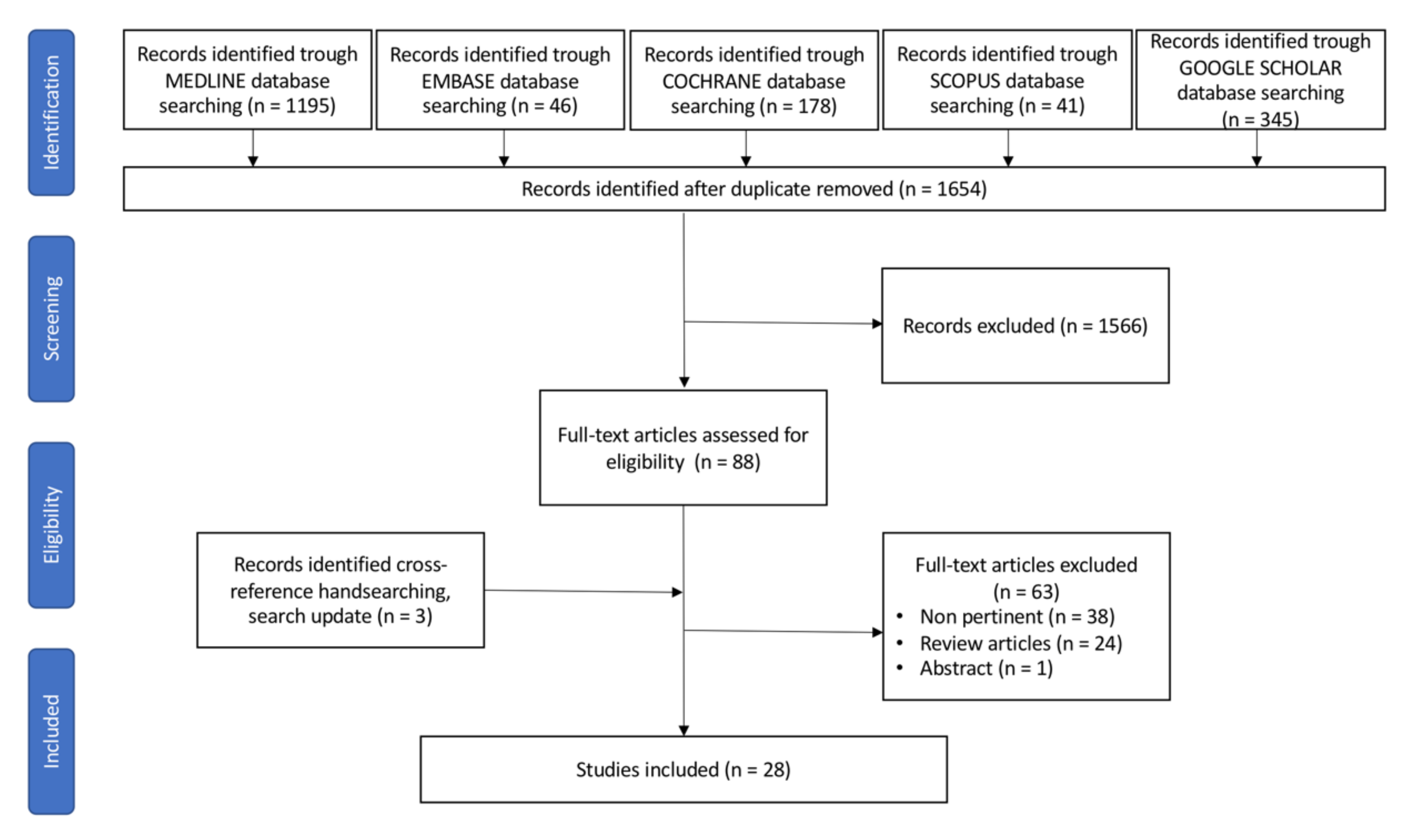
3.1. Literature Search and Selection
3.2. Studies Characteristics
3.3. Oral Microbiota and Esophageal Cancer (EC)
3.4. Oral Microbiota and Liver Cancer (LC)
3.5. Oral Microbiota and Pancreatic Cancer (PC)
3.6. Oral Microbiota and Gastric Cancer (GC)
3.7. Oral Microbiota and Colorectal Cancer (CRC)
3.8. Study Quality Assessment
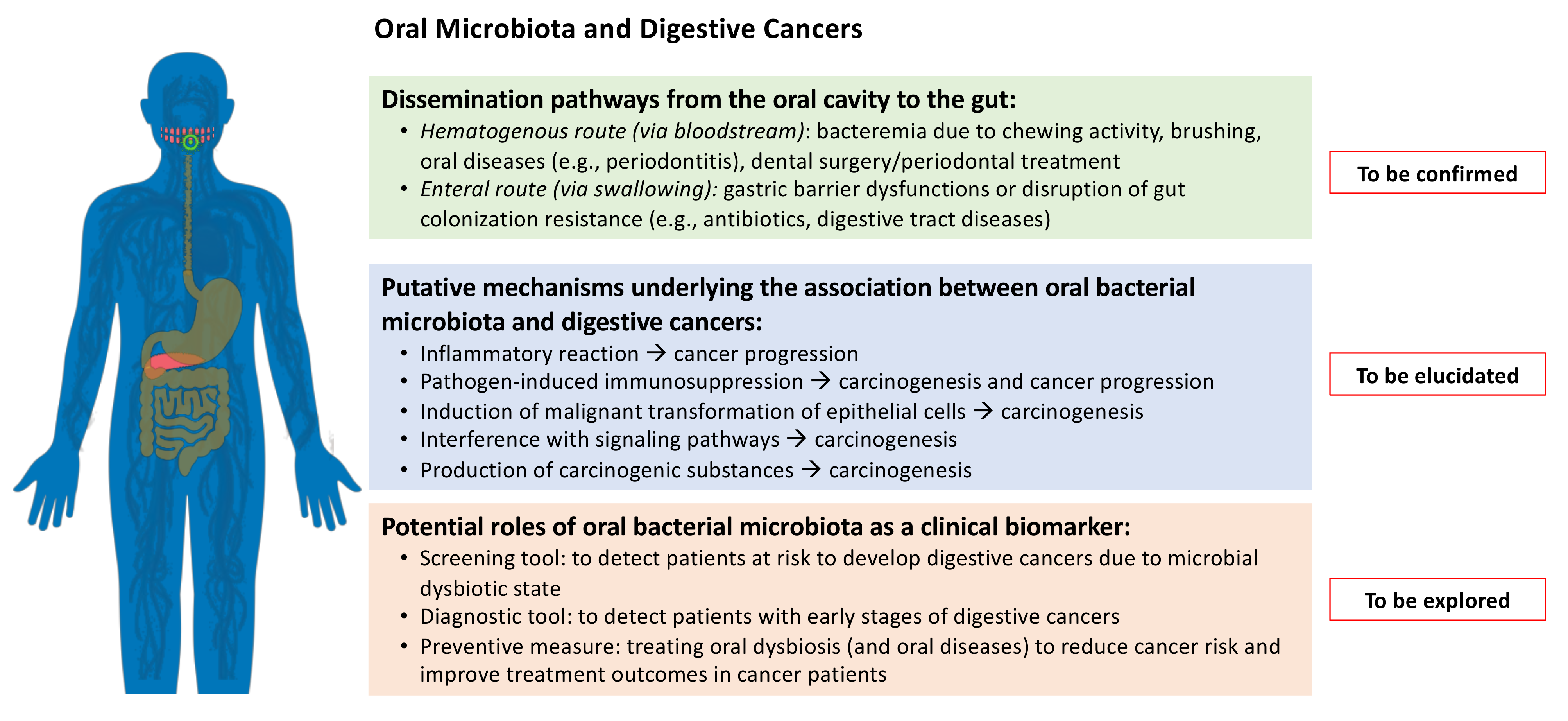
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nagai, H.; Kim, Y.H. Cancer prevention from the perspective of global cancer burden patterns. J. Thorac. Dis. 2017, 9, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Abnet, C.C.; Neale, R.E.; Vignat, J.; Giovannucci, E.L.; McGlynn, K.A.; Bray, F. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gastroenterology 2020, 159, 335–349. [Google Scholar] [CrossRef]
- Flemer, B.; Warren, R.D.; Barrett, M.P.; Cisek, K.; Das, A.; Jeffery, I.B.; Hurley, E.; O‘Riordain, M.; Shanahan, F.; O’Toole, P.W. The oral microbiota in colorectal cancer is distinctive and predictive. Gut 2017, 67, 1454–1463. [Google Scholar] [CrossRef] [Green Version]
- Cani, P.D. Human gut microbiome: Hopes, threats and promises. Gut 2018, 67, 1716–1725. [Google Scholar] [CrossRef] [PubMed]
- Huttenhower, C.; Gevers, D.; Knight, R.; Abubucker, S.; Badger, J.H.; Chinwalla, A.T.; Creasy, H.H.; Earl, A.M.; Fitzgerald, M.G.; Fulton, R.S.; et al. Structure, function and diversity of the healthy human microbiome. Nature 2012, 486, 207–214. [Google Scholar]
- Peters, B.; Wu, J.; Pei, Z.; Yang, L.; Purdue, M.P.; Freedman, N.D.; Jacobs, E.J.; Gapstur, S.M.; Hayes, R.; Ahn, J. Oral Microbiome Composition Reflects Prospective Risk for Esophageal Cancers. Cancer Res. 2017, 77, 6777–6787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauka, L.; Reitano, E.; Carra, M.C.; Gaiani, F.; Gavriilidis, P.; Brunetti, F.; de’Angelis, G.L.; Sobhani, I.; de’Angelis, N. Role of the intestinal microbiome in colorectal cancer surgery outcomes. World J. Surg. Oncol. 2019, 17, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, C.; Round, J.L. Defining dysbiosis and its influence on host immunity and disease. Cell. Microbiol. 2014, 16, 1024–1033. [Google Scholar] [CrossRef]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the Normal Bacterial Flora of the Oral Cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef] [Green Version]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef] [Green Version]
- Helmink, B.A.; Khan, M.A.W.; Hermann, A.; Gopalakrishnan, V.; Wargo, J.A. The microbiome, cancer, and cancer therapy. Nat. Med. 2019, 25, 377–388. [Google Scholar] [CrossRef]
- Lamont, R.J.; Hajishengallis, G. Polymicrobial synergy and dysbiosis in inflammatory disease. Trends Mol. Med. 2015, 21, 172–183. [Google Scholar] [CrossRef] [Green Version]
- Jangi, S.; Gandhi, R.; Cox, L.; Li, N.; Von Glehn, F.; Yan, R.; Patel, B.; Mazzola, M.A.; Liu, S.; Glanz, B.L.; et al. Alterations of the human gut microbiome in multiple sclerosis. Nat. Commun. 2016, 7, 12015. [Google Scholar] [CrossRef]
- Novakovic, M.; Rout, A.; Kingsley, T.; Kirchoff, R.; Singh, A.; Verma, V.; Kant, R.; Chaudhary, R. Role of gut microbiota in cardiovascular diseases. World J. Cardiol. 2020, 12, 110–122. [Google Scholar] [CrossRef] [PubMed]
- Duranti, S.; Gaiani, F.; Mancabelli, L.; Milani, C.; Grandi, A.; Bolchi, A.; Santoni, A.; Lugli, G.A.; Ferrario, C.; Mangifesta, M.; et al. Elucidating the gut microbiome of ulcerative colitis: Bifidobacteria as novel microbial biomarkers. FEMS Microbiol. Ecol. 2016, 92, fiw191. [Google Scholar] [CrossRef] [Green Version]
- Kato, I.; Vasquez, A.A.; Moyerbrailean, G.; Land, S.; Sun, J.; Lin, H.-S.; Ram, J.L. Oral microbiome and history of smoking and colorectal cancer. J. Epidemiol. Res. 2015, 2, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Luo, G.-H. Porphyromonas gingivalisand digestive system cancers. World J. Clin. Cases 2019, 7, 819–829. [Google Scholar] [CrossRef]
- Lee, S.A.; Liu, F.; Riordan, S.M.; Lee, C.S.; Zhang, L. Global Investigations of Fusobacterium nucleatum in Human Colorectal Cancer. Front. Oncol. 2019, 9, 566. [Google Scholar] [CrossRef] [Green Version]
- Koliarakis, I.; Messaritakis, I.; Nikolouzakis, T.K.; Hamilos, G.; Souglakos, J.; Tsiaoussis, J. Oral Bacteria and Intestinal Dysbiosis in Colorectal Cancer. Int. J. Mol. Sci. 2019, 20, 4146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.; Li, Q.; Fu, X. Fusobacterium nucleatum Contributes to the Carcinogenesis of Colorectal Cancer by Inducing Inflammation and Suppressing Host Immunity. Transl. Oncol. 2019, 12, 846–851. [Google Scholar] [CrossRef]
- McCoy, A.N.; Araújo-Pérez, F.; Azcarate-Peril, M.A.; Yeh, J.J.; Sandler, R.S.; Keku, T.O. Fusobacterium Is Associated with Colorectal Adenomas. PLoS ONE 2013, 8, e53653. [Google Scholar] [CrossRef]
- Rubinstein, M.R.; Wang, X.; Liu, W.; Hao, Y.; Cai, G.; Han, Y.W. Fusobacterium nucleatum Promotes Colorectal Carcinogenesis by Modulating E-Cadherin/β-Catenin Signaling via its FadA Adhesin. Cell Host Microbe 2013, 14, 195–206. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Niu, Q.; Fan, W.; Huang, F.; He, H. Oral microbiota and gastrointestinal cancer. OncoTargets Ther. 2019, 12, 4721–4728. [Google Scholar] [CrossRef] [Green Version]
- Kostic, A.D.; Chun, E.; Robertson, L.; Glickman, J.N.; Gallini, C.A.; Michaud, M.; Clancy, T.E.; Chung, D.C.; Lochhead, P.; Hold, G.L.; et al. Fusobacterium nucleatum Potentiates Intestinal Tumorigenesis and Modulates the Tumor-Immune Microenvironment. Cell Host Microbe 2013, 14, 207–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Weng, W.; Peng, J.; Hong, L.; Yang, L.; Toiyama, Y.; Gao, R.; Liu, M.; Yin, M.; Pan, C.; et al. Fusobacterium nucleatum Increases Proliferation of Colorectal Cancer Cells and Tumor Development in Mice by Activating Toll-Like Receptor 4 Signaling to Nuclear Factor−κB, and Up-regulating Expression of MicroRNA-21. Gastroenterology 2017, 152, 851–866.e24. [Google Scholar] [CrossRef] [Green Version]
- Flynn, K.J.; Baxter, N.T.; Schloss, P.D. Metabolic and Community Synergy of Oral Bacteria in Colorectal Cancer. mSphere 2016, 1, e00102-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, L.; Schmid, J.; Ebert, M.; Soucek, P.; Kunicka, T.; Liška, V.; Bruha, J.; Neary, P.; DeZeeuw, N.; Tommasino, M.; et al. Fusobacterium nucleatum associates with stages of colorectal neoplasia development, colorectal cancer and disease outcome. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1381–1390. [Google Scholar] [CrossRef]
- Pascual, L.M.; Cabrera-Rubio, R.; Ocon, S.; Costales, P.; Parra, A.; Suarez, A.; Moris, F.; Rodrigo, L.; Mira, A.; Collado, M.C. Microbial mucosal colonic shifts associated with the development of colorectal cancer reveal the presence of different bacterial and archaeal biomarkers. J. Gastroenterol. 2015, 50, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Tahara, T.; Yamamoto, E.; Suzuki, H.; Maruyama, R.; Chung, W.; Garriga, J.; Jelinek, J.; Yamano, H.-O.; Sugai, T.; An, B.; et al. Fusobacterium in Colonic Flora and Molecular Features of Colorectal Carcinoma. Cancer Res. 2014, 74, 1311–1318. [Google Scholar] [CrossRef] [Green Version]
- Farrell, J.J.; Zhang, L.; Zhou, H.; Chia, D.; Elashoff, D.; Akin, D.; Paster, B.J.; Joshipura, K.; Wong, D.T.W. Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer. Gut 2018, 61, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Chen, X.; Yu, H.; Zhou, H.; Xu, S. Oral Microbiota as Promising Diagnostic Biomarkers for Gastrointestinal Cancer: A Systematic Review. OncoTargets Ther. 2019, 12, 11131–11144. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0; John Wiley & Sons: New Jersey, NJ, USA, 2019. [Google Scholar]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F. Preferred Reporting Items for a Systematic Review and Meta-analysis of Individual Participant Data: The PRISMA-IPD statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiology 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mai, X.; Genco, R.J.; LaMonte, M.J.; Hovey, K.M.; Freudenheim, J.L.; Andrews, C.; Wactawski-Wende, J. Periodontal Pathogens and Risk of Incident Cancer in Postmenopausal Females: The Buffalo OsteoPerio Study. J. Periodontol. 2016, 87, 257–267. [Google Scholar] [CrossRef] [Green Version]
- Russo, E.; Bacci, G.; Chiellini, C.; Fagorzi, C.; Niccolai, E.; Taddei, A.; Ricci, F.; Ringressi, M.N.; Borrelli, R.; Melli, F.; et al. Preliminary Comparison of Oral and Intestinal Human Microbiota in Patients with Colorectal Cancer: A Pilot Study. Front. Microbiol. 2018, 8, 2699. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Cai, Q.; Shu, X.; Steinwandel, M.D.; Blot, W.J.; Zheng, W.; Long, J. Prospective study of oral microbiome and colorectal cancer risk in low-income and African American populations. Int. J. Cancer 2019, 144, 2381–2389. [Google Scholar] [CrossRef]
- Schmidt, T.S.; Hayward, M.R.; Coelho, L.P.; Li, S.S.; Costea, P.I.; Voigt, A.Y.; Wirbel, J.; Maistrenko, O.M.; Alves, R.J.; Bergsten, E.; et al. Extensive transmission of microbes along the gastrointestinal tract. eLife 2019, 8, e42693. [Google Scholar] [CrossRef]
- Han, S.; Yang, X.; Qi, Q.; Pan, Y.; Chen, Y.; Shen, J.; Liao, H.; Ji, Z. Potential screening and early diagnosis method for cancer: Tongue diagnosis. Int. J. Oncol. 2016, 48, 2257–2264. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Kong, C.; Yang, Y.; Cai, S.; Li, X.; Cai, G.; Ma, Y. Human oral microbiome dysbiosis as a novel non-invasive biomarker in detection of colorectal cancer. Theranostics 2020, 10, 11595–11606. [Google Scholar] [CrossRef] [PubMed]
- Guven, D.C.; Dizdar, O.; Alp, A.; Kittana, F.N.A.; Karakoc, D.; Hamaloglu, E.; Lacin, S.; Karakas, Y.; Kilickap, S.; Hayran, M.; et al. Analysis of Fusobacterium nucleatum and Streptococcus gallolyticus in saliva of colorectal cancer patients. Biomark. Med. 2019, 13, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Vogtmann, E.; Han, Y.; Caporaso, J.G.; Bokulich, N.; Mohamadkhani, A.; MoayyedKazemi, A.; Hua, X.; Kamangar, F.; Wan, Y.; Suman, S.; et al. Oral microbial community composition is associated with pancreatic cancer: A case-control study in Iran. Cancer Med. 2019, 9, 797–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, P.J.; Fletcher, E.M.; Gibbons, S.; Bouvet, M.; Doran, K.S.; Kelley, S.T. Characterization of the salivary microbiome in patients with pancreatic cancer. PeerJ 2015, 3, e1373. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.H.; Satagopan, J.; Xu, Y.; Ling, L.; Leong, S.; Orlow, I.; Saldia, A.; Lilan, L.; Nunes, P.; Madonia, V.; et al. The oral microbiota in patients with pancreatic cancer, patients with IPMNs, and controls: A pilot study. Cancer Causes Control. 2017, 28, 959–969. [Google Scholar] [CrossRef]
- Fan, X.; Alekseyenko, A.V.; Wu, J.; Peters, B.A.; Jacobs, E.J.; Gapstur, S.M.; Purdue, M.P.; Abnet, C.C.; Stolzenberg-Solomon, R.; Miller, G.; et al. Human oral microbiome and prospective risk for pancreatic cancer: A population-based nested case-control study. Gut 2018, 67, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Ren, Z.; Li, A.; Li, J.; Xu, S.; Zhang, H.; Jiang, J.; Yang, J.; Luo, Q.; Zhou, K.; et al. Tongue coating microbiome data distinguish patients with pancreatic head cancer from healthy controls. J. Oral Microbiol. 2019, 11, 1563409. [Google Scholar] [CrossRef]
- Wei, A.-L.; Li, M.; Li, G.-Q.; Wang, X.; Hu, W.-M.; Li, Z.-L.; Yuan, J.; Liu, H.-Y.; Zhou, L.-L.; Li, K.; et al. Oral microbiome and pancreatic cancer. World J. Gastroenterol. 2020, 26, 7679–7692. [Google Scholar] [CrossRef]
- Hu, J.; Han, S.; Chen, Y.; Ji, Z. Variations of Tongue Coating Microbiota in Patients with Gastric Cancer. BioMed Res. Int. 2015, 2015, 173729. [Google Scholar] [CrossRef] [Green Version]
- Huang, K.; Gao, X.; Wu, L.; Yan, B.; Wang, Z.; Zhang, X.; Peng, L.; Yu, J.; Sun, G.; Yang, Y. Salivary Microbiota for Gastric Cancer Prediction: An Exploratory Study. Front. Cell. Infect. Microbiol. 2021, 11, 640309. [Google Scholar] [CrossRef]
- Sun, J.; Li, X.; Yin, J.; Li, Y.; Hou, B.; Zhang, Z. A screening method for gastric cancer by oral microbiome detection. Oncol. Rep. 2018, 39, 2217–2224. [Google Scholar] [CrossRef]
- Wu, J.; Xu, S.; Xiang, C.; Cao, Q.; Li, Q.; Huang, J.; Shi, L.; Zhang, J.; Zhan, Z. Tongue Coating Microbiota Community and Risk Effect on Gastric Cancer. J. Cancer 2018, 9, 4039–4048. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Xiang, C.; Zhang, C.; Xu, B.; Wu, J.; Wang, R.; Yang, Y.; Shi, L.; Zhang, J.; Zhan, Z. Microbial biomarkers of common tongue coatings in patients with gastric cancer. Microb. Pathog. 2019, 127, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Winckler, B.; Lu, M.; Cheng, H.; Yuan, Z.; Yang, Y.; Jin, L.; Ye, W. Oral Microbiota and Risk for Esophageal Squamous Cell Carcinoma in a High-Risk Area of China. PLoS ONE 2015, 10, e0143603. [Google Scholar] [CrossRef]
- Wang, Q.; Rao, Y.; Guo, X.; Liu, N.; Liu, S.; Wen, P.; Li, S.; Li, Y. Oral Microbiome in Patients with Oesophageal Squamous Cell Carcinoma. Sci. Rep. 2019, 9, 19055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Q.; Yang, T.; Yan, Y.; Zhang, Y.; Li, Z.; Wang, Y.; Yang, J.; Xia, Y.; Xiao, H.; Han, H.; et al. Alterations of Oral Microbiota in Chinese Patients with Esophageal Cancer. Front. Cell. Infect. Microbiol. 2020, 10, 541144. [Google Scholar] [CrossRef] [PubMed]
- Kawasaki, M.; Ikeda, Y.; Ikeda, E.; Takahashi, M.; Tanaka, D.; Nakajima, Y.; Arakawa, S.; Izumi, Y.; Miyake, S. Oral infectious bacteria in dental plaque and saliva as risk factors in patients with esophageal cancer. Cancer 2021, 127, 512–519. [Google Scholar] [CrossRef]
- Lu, H.; Ren, Z.; Li, A.; Zhang, H.; Jiang, J.; Xu, S.; Luo, Q.; Zhou, K.; Sun, X.; Zheng, S.; et al. Deep sequencing reveals microbiota dysbiosis of tongue coat in patients with liver carcinoma. Sci. Rep. 2016, 6, 33142. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Xi, W.; Zhang, Z.; Ren, L.; Deng, C.; Chen, J.; Sun, C.; Zhang, N.; Xu, J. Oral microbial community analysis of the patients in the progression of liver cancer. Microb. Pathog. 2020, 149, 104479. [Google Scholar] [CrossRef]
- Sun, J.; Tang, Q.; Yu, S.; Xie, M.; Xie, Y.; Chen, G.; Chen, L. Role of the oral microbiota in cancer evolution and progression. Cancer Med. 2020, 9, 6306–6321. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, R.F.; Jobin, C. The microbiome and cancer. Nat. Rev. Cancer 2013, 13, 800–812. [Google Scholar] [CrossRef] [Green Version]
- Atarashi, K.; Suda, W.; Luo, C.; Kawaguchi, T.; Motoo, I.; Narushima, S.; Kiguchi, Y.; Yasuma, K.; Watanabe, E.; Tanoue, T.; et al. Ectopic colonization of oral bacteria in the intestine drives T H 1 cell induction and inflammation. Science 2017, 358, 359–365. [Google Scholar] [CrossRef]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef]
- Berg, R.D. Bacterial translocation from the gastrointestinal tract. Adv. Exp. Med. Biol. 1999, 473, 11–30. [Google Scholar] [PubMed]
- Ito, M.; Kanno, S.; Nosho, K.; Sukawa, Y.; Mitsuhashi, K.; Kurihara, H.; Igarashi, H.; Takahashi, T.; Tachibana, M.; Takahashi, H.; et al. Association of Fusobacterium nucleatum with clinical and molecular features in colorectal serrated pathway. Int. J. Cancer 2015, 137, 1258–1268. [Google Scholar] [CrossRef] [PubMed]
- Park, C.H.; Han, D.S.; Oh, Y.-H.; Lee, A.-R.; Lee, Y.-R.; Eun, C.S. Role of Fusobacteria in the serrated pathway of colorectal carcinogenesis. Sci. Rep. 2016, 6, 25271. [Google Scholar] [CrossRef] [PubMed]
- Yamamura, K.; Baba, Y.; Nakagawa, S.; Mima, K.; Miyake, K.; Nakamura, K.; Sawayama, H.; Kinoshita, K.; Ishimoto, T.; Iwatsuki, M.; et al. Human Microbiome Fusobacterium Nucleatum in Esophageal Cancer Tissue Is Associated with Prognosis. Clin. Cancer Res. 2016, 22, 5574–5581. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Guo, F.; Yu, Y.; Sun, T.; Ma, D.; Han, J.; Qian, Y.; Kryczek, I.; Sun, D.; Nagarsheth, N.; et al. Fusobacterium nucleatum Promotes Chemoresistance to Colorectal Cancer by Modulating Autophagy. Cell 2017, 170, 548–563.e16. [Google Scholar] [CrossRef] [Green Version]
- Serna, G.; Ruiz-Pace, F.; Hernando, J.; Alonso, L.; Fasani, R.; Landolfi, S.; Comas, R.; Jimenez, J.; Elez, E.; Bullman, S.; et al. Fusobacterium nucleatum persistence and risk of recurrence after preoperative treatment in locally advanced rectal cancer. Ann. Oncol. 2020, 31, 1366–1375. [Google Scholar] [CrossRef]
- Ojima, M.; Hanioka, T.; Shimada, K.; Haresaku, S.; Yamamoto, M.; Tanaka, K. The role of tobacco use on dental care and oral disease severity within community dental clinics in Japan. Tob. Induc. Dis. 2013, 11, 13. [Google Scholar] [CrossRef] [Green Version]
- Fan, X.; Peters, B.A.; Jacobs, E.J.; Gapstur, S.M.; Purdue, M.P.; Freedman, N.D.; Alekseyenko, A.V.; Wu, J.; Yang, L.; Pei, Z.; et al. Drinking alcohol is associated with variation in the human oral microbiome in a large study of American adults. Microbiome 2018, 6, 59. [Google Scholar] [CrossRef] [Green Version]
- Matsui, M.; Chosa, N.; Shimoyama, Y.; Minami, K.; Kimura, S.; Kishi, M. Effects of tongue cleaning on bacterial flora in tongue coating and dental plaque: A crossover study. BMC Oral Health 2014, 14, 4. [Google Scholar] [CrossRef] [Green Version]
- Lassalle, F.; Spagnoletti, M.; Fumagalli, M.; Shaw, L.; Dyble, M.; Walker, C.; Thomas, M.G.; Migliano, A.B.; Balloux, F. Oral microbiomes from hunter-gatherers and traditional farmers reveal shifts in commensal balance and pathogen load linked to diet. Mol. Ecol. 2018, 27, 182–195. [Google Scholar] [CrossRef] [Green Version]
- Ndegwa, N.; Ploner, A.; Liu, Z.; Roosaar, A.; Axéll, T.; Ye, W. Association between poor oral health and gastric cancer: A prospective cohort study. Int. J. Cancer 2018, 143, 2281–2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.; Jung, K.U.; Kim, H.O.; Kim, H.; Chun, H.-K. Association between oral health and colorectal adenoma in a screening population. Medicine 2018, 97, e12244. [Google Scholar] [CrossRef] [PubMed]
- Momen-Heravi, F.; Babic, A.; Tworoger, S.S.; Zhang, L.; Wu, K.; Smith-Warner, S.A.; Ogino, S.; Chan, A.T.; Meyerhardt, J.; Giovannucci, E.; et al. Periodontal disease, tooth loss and colorectal cancer risk: Results from the Nurses’ Health Study. Int. J. Cancer 2017, 140, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.W.; Singh, N.; Ng, K.F.; Lam, D.K.; Goldberg, M.B.; Tenenbaum, H.C.; Neufeld, J.D.; Beiko, R.G.; Senadheera, D.B. Inter-personal diversity and temporal dynamics of dental, tongue, and salivary microbiota in the healthy oral cavity. NPJ Biofilms Microbiomes 2017, 3, 2. [Google Scholar] [CrossRef]
- Slots, J.; Slots, H. Bacterial and viral pathogens in saliva: Disease relationship and infectious risk. Periodontol. 2000 2010, 55, 48–69. [Google Scholar] [CrossRef]
- Jo, R.; Nishimoto, Y.; Umezawa, K.; Yama, K.; Aita, Y.; Ichiba, Y.; Murakami, S.; Kakizawa, Y.; Kumagai, T.; Yamada, T.; et al. Comparison of oral microbiome profiles in stimulated and unstimulated saliva, tongue, and mouth-rinsed water. Sci. Rep. 2019, 9, 16124. [Google Scholar] [CrossRef] [Green Version]
- Gomar-Vercher, S.; Simon-Soro, A.; Montiel-Company, J.M.; Almerich-Silla, J.M.; Mira, A. Stimulated and unstimulated saliva samples have significantly different bacterial profiles. PLoS ONE 2018, 13, e0198021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, W.; Li, X.; Li, Y.; Li, C.; Gao, B.; Gan, H.; Li, S.; Shen, J.; Kang, J.; Ding, S.; et al. Tongue coating microbiome regulates the changes in tongue texture and coating in patients with post-menopausal osteoporosis of Gan-shen deficiency syndrome type. Int. J. Mol. Med. 2013, 32, 1069–1076. [Google Scholar] [CrossRef] [Green Version]
- Haririan, H.; Andrukhov, O.; Bertl, K.; Lettner, S.; Kierstein, S.; Moritz, A.; Rausch-Fan, X. Microbial Analysis of Subgingival Plaque Samples Compared to that of Whole Saliva in Patients with Periodontitis. J. Periodontol. 2014, 85, 819–828. [Google Scholar] [CrossRef]
- Haffajee, A.D.; Bogren, A.; Hasturk, H.; Feres, M.; Lopez, N.J.; Socransky, S.S. Subgingival microbiota of chronic periodontitis subjects from different geographic locations. J. Clin. Periodontol. 2004, 31, 996–1002. [Google Scholar] [CrossRef] [PubMed]
- Bergsten, E.; Mestivier, D.; Sobhani, I. The Limits and Avoidance of Biases in Metagenomic Analyses of Human Fecal Microbiota. Microorganisms 2020, 8, 1954. [Google Scholar] [CrossRef]
- Gupta, V.; Paul, S.; Dutta, C. Geography, Ethnicity or Subsistence-Specific Variations in Human Microbiome Composition and Diversity. Front. Microbiol. 2017, 8, 1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, S.A. Genetic predisposition to cancer—Insights from population genetics. Nat. Rev. Genet. 2004, 5, 764–772. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Reference | Country | Study Design | Study Sample Size (n) | Digestive Cancer Type | Oral Examination/Diagnosis |
|---|---|---|---|---|---|
| Farrell, J. et al. Gut 2012 [30] | USA | Matched case-control | 103 | PC | Not reported |
| Chen, X. et al. PloS ONE 2015 [53] | China | Case-control | 235 | ESCC | Number of teeth; Missing and filled teeth (MFT score), oral hygiene habits |
| Hu, J. et al. Biomed. Res. Int. 2015 [48] | China | Case-control | 146 | GC | No oral disease |
| May, X. et al. J. Periodontol. 2015 [35] | USA | Prospective cohort | 1252 | CRC | Periodontal examination, oral hygiene habits |
| Torres, P. et al. Peer J. 2015 [43] | USA | Case-control | 108 | PC | Not reported |
| Han, S. et al. Int. J. Oncol. 2016 [39] | China | Case-control | 290 | CRC and GC | Tongue examination; No oral disease |
| Kato, I. et al. J. Epidemiol. Res. 2016 [16] | USA | Population-based case-control | 190 | CRC | Not reported |
| Lu, H. et al. Sci. Rep. 2016 [57] | China | Matched case-control | 60 | LC | Full oral examination; No oral disease |
| Peters, B.A. et al. Cancer Res. 2017 [6] | USA | Case control | 316 | ESCC and EAC | Not reported |
| Olson, S. et al. Cancer Causes Control. 2017 [44] | USA | Case-control | 137 | PC, PDAC and IPMN | Number of missing teeth missing; periodontal diseases; number of dental visits in the past 10 years for checkup or cleaning; use of mouthwash at least once a week in the past 5 years |
| Fan, X. et al. Gut 2018 [45] | USA | Population-based nested matched case-control study | 732 | PC | Not reported |
| Flemer, B. et al. Gut 2018 [3] | Ireland | Case-control | 234 | CRC | Not reported |
| Russo, E. et al. Front. Microbiol. 2018 [36] | Italy | Case-control | 20 | CRC | Not reported |
| Sun, J. et al. Oncol. Rep. 2018 [50] | China | Case-control | 50 | GC | Not reported |
| Wu, J. et al. J. Cancer 2018 [51] | China | Case-control | 137 | GC | Not reported |
| Xu, J. et al. Microb. Pathog. 2019 [52] | China | Case-control | 150 | GC | Not reported |
| Lu, H. et al. J. Oral Microbiol. 2019 [46] | China | Case-control | 55 | PC | No oral disease |
| Schmidt, T. et al. eLife 2019 [38] | Europe | Case-control (Multicentric study) | 520 | CRC | Not reported |
| Yang, Y. et al. Int. J. Cancer 2019 [37] | USA | Nested matched case-control study | 693 | CRC | Oral health history |
| Wang, Q. et al. Sci. Rep. 2019 [54] | China | Case-control | 41 | ESCC | Oral health history |
| Guven, D.C. et al. Biomark. Med. 2019 [41] | Turkey | Case-control | 148 | CRC | Oral health history |
| Vogtmann, E. et al. Cancer Med. 2020 [42] | Iran | Case-control | 558 | PC | Not reported |
| Zhao, Q. et al. Front. Cell. Infect. Microbiol. 2020 [55] | China | Case-control | 90 | ESCC | Not reported |
| Zhang, S. et al. Theranostics 2020 [40] | China | Case-control | 253 | CRC | Not reported |
| Kawasaky, M. et al. Cancer 2020 [56] | Japan | Case-control | 122 | ESCC | Not reported |
| Li, D. et al. Microb. Phatog. 2020 [58] | China | Case-control | 24 | LC | Not reported |
| Wei, A.L. et al. World J. Gastroenterol. 2020 [47] | China | Case-control | 114 | PC | Not reported |
| Huang, K. et al. Front. Cell. Infect. Microbiol. 2021 [49] | China | Prospective cohort | 293 | GC | Not reported |
| Reference | Study Population Characteristics (n) | Sampling Method and Type(s) of Microbiological Analysis | Microbiota Associated with Cancer | Bacterial Quantification | Main Finding(s) |
|---|---|---|---|---|---|
| Farrell, J. et al. Gut 2012 [30] | Discovery cohort:
| Saliva
|
| Absolute amount | 31 bacterial species/clusters were increased in the saliva of PC patients, and 25 bacterial species/clusters were decreased in comparison with healthy controls. Salivary microbiota may be a non-invasive biomarker. |
| Chen, X. et al. PloS ONE 2015 [53] |
| Saliva
|
| Relative abundance | ESCC patients had a decreased microbial diversity compared with healthy controls and patients with dysplasia. |
| Hu, J. et al. Biomed. Res. Int. 2015 [48] |
| Tongue coating
|
| Relative abundance | Thick tongue coatings observed in GC patients presented lower microbial community diversity than thin tongue coatings of healthy controls. |
| May, X. et al. J. Periodontol. 2015 [35] | Buffalo Osteoporosis and Periodontal Disease Study cohort of postmenopausal females
| Subgingival plaque
|
| Relative abundance | No associations were found between the presence of individual subgingival periodontal pathogens and the incident risk of cancer. |
| Torres, P. et al. Peer J. 2015 [43] |
| Saliva
|
| Relative abundance | Several bacterial genera differed in abundance between PC patients and controls. Bacteria abundance profiles in saliva may be useful biomarkers. |
| Han, S. et al. Int. J. Oncol. 2016 [39] |
| Tongue coating
|
| Relative abundance | Tongue coating is thicker in cancer patients than in healthy controls. Six microorganisms at the species level were significantly different. |
| Kato, I. et al. J. Epidemiol. Res. 2016 [16] |
| Oral rinse
|
| Relative abundance | No association between Fusobacterium abundance or presence and CRC. |
| Lu, H. et al. Sci. Rep. 2016 [57] |
| Tongue coating
|
| Absolute amount | Significant microbial dysbiosis of tongue coats in LC patients. |
| Peters, B.A. et al. Cancer Res. 2017 [6] |
| Oral rinse
|
| Relative abundance | Differences in oral microbiota composition between cases and controls. Possible application for screening purpose. |
| Olson, S. et al. Cancer Causes Control. 2017 [44] |
| Saliva
|
| Relative abundance | PDAC cases did not differ in microbiota diversity from controls or IPMN patients. |
| Fan, X. et al. Gut 2018 [45] | From the CPS II and PLCO cohorts
| Oral rinse
|
| Relative abundance | Carriage of the periodontal pathogens and decreased relative abundance of Fusobacteria and its genus Leptotrichia are associated with subsequent risk of PC. |
| Flemer, B. et al. Gut 2018 [3] |
| Oral swabs
|
| Absolute amount | A classification model of oral swab microbiota distinguishes individuals with CRC or polyps from controls. |
| Russo, E. et al. Front. Microbiol. 2018 [36] |
| Saliva
|
| Relative abundance | Bacterial community composition differed significantly between CRC patients and healthy controls. |
| Sun, J. et al. Oncol. Rep. 2018 [50] |
| Dental plaque and saliva
|
| Absolute amount | There are differences in the biomass, species richness, and species diversity between GC patients and controls. A microbiome scoring system was designed to be a potential screening method for GC. |
| Wu, J. et al. J. Cancer 2018 [51] |
| Tongue coating
|
| Relative abundance | Microbiome in tongue coating may have potential guiding value for early detection and prevention of GC. |
| Xu, J. et al. Microb. Pathog. 2019 [52] |
| Tongue coating
|
| Relative abundance | Richness and diversity of microbiome are not related to the variation of the four common types of tongue coating in GC patients. |
| Lu, H. et al. J. Oral. Microbiol. 2019 [46] |
| Tongue coating
|
| Absolute amount | PC patients are colonized by remarkably different tongue coating microbiota than healthy controls. |
| Schmidt, T. et al. eLife 2019 [38] |
| Saliva
|
| Relative abundance | The oral cavity is an endogenous reservoir for gut microbial strains, with increased levels of transmission in CRC patients. |
| Yang, Y. et al. Int. J. Cancer 2019 [37] |
| Oral rinse
|
| Relative abundance | Multiple oral bacterial taxa are associated with CRC risk. |
| Wang, Q. et al. Sci. Rep. 2019 [54] |
| Saliva
|
| Relative abundance | Association between oral dysbiosis and risk of ESCC. |
| Guven, D.C. et al. Biomark. Med. 2019 [41] |
| Saliva
|
| Absolute amount | Higher amounts of Fusobacterium nucleatum and Streptococcus gallolyticus in CRC patients. |
| Vogtmann, E. et al. Cancer. Med. 2020 [42] |
| Saliva
|
| Relative abundance | Increased levels of some oral bacteria and PC, with the overall microbial community different between PC patients and controls. |
| Zhao, Q. et al. Front. Cell. Infect. Microbiol.. 2020 [55] |
| Saliva
|
| Relative abundance | Differences in oral microbiota composition between cases and controls. |
| Zhang, S. et al. Theranostics 2020 [40] |
| Oral swabs
|
| Relative abundance. | Oral microbial composition and diversity were significantly different among the three groups, and the CRA group had the highest diversity. |
| Kawasaky, M. et al. Cancer 2020 [56] |
| Dental plaque and saliva
|
| Relative abundance | Differences in oral microbiota composition between cases and controls. Stronger microbiota association with dental plaque sample. Possible application for screening purpose. |
| Li, D. et al. Microb. Phatog. 2020 [58] |
| Saliva
|
| Relative abundance | Difference in oral microbiota composition according to the different grade of disease. |
| Wei, A.L. et al. World J. Gastroenterol. 2020 [47] |
| Saliva
|
| Relative abundances | Differences in microbiota composition between cases and controls. |
| Huang, K. et al. Front. Cell. Infect. Microbiol. 2021 [49] |
| Saliva
|
| Relative abundance | A distinct salivary microbiota was observed in patients with GC when comparing with SG and AG. Salivary microbiota could be used to predict GC as well as its non-malignant stages. |
| Selection | Comparability | Outcome | Total Score | |
|---|---|---|---|---|
| Farrell, J. et al. Gut 2012 [30] | *** | * | ** | 6 |
| Chen, X. et al. PloS ONE 2015 [53] | ** | ** | ** | 6 |
| Hu, J. et al. Biomed. Res. Int. 2015 [48] | ** | ** | ** | 6 |
| May, X. et al. J. Periodontol. 2015 [35] | ** | ** | *** | 7 |
| Torres, P. et al. Peer J. 2015 [43] | **** | * | ** | 7 |
| Han, S. et al. Int. J. Oncol. 2016 [39] | **** | * | ** | 7 |
| Kato, I. et al. J. Epidemiol. Res. 2016 [16] | ** | * | ** | 5 |
| Lu, H. et al. Sci. Rep. 2016 [57] | ** | ** | ** | 6 |
| Peters, B.A. et al. Cancer Res. 2017 [6] | ** | ** | ** | 6 |
| Olson, S. et al. Cancer Causes Control. 2017 [44] | **** | * | ** | 7 |
| Fan, X. et al. Gut 2018 [45] | *** | ** | ** | 7 |
| Flemer, B. et al. Gut 2018 [3] | ** | * | *** | 6 |
| Russo, E. et al. Front. Microbiol. 2018 [36] | ** | * | *** | 6 |
| Sun, J. et al. Oncol. Rep. 2018 [50] | **** | * | ** | 7 |
| Wu, J. et al. J. Cancer 2018 [51] | *** | * | ** | 6 |
| Xu, J. et al. Microb. Pathog. 2019 [52] | ** | ** | ** | 6 |
| Lu, H. et al. J. Oral Microbiol. 2019 [46] | *** | * | ** | 6 |
| Schmidt, T. et al. eLife 2019 [38] | ** | * | ** | 5 |
| Yang, Y. et al. Int. J. Cancer 2019 [37] | ** | ** | ** | 6 |
| Wang, Q. et al. Sci. Rep. 2019 [54] | ** | * | ** | 5 |
| Guven, D.C. et al. Biomark. Med. 2019 [41] | ** | ** | ** | 6 |
| Vogtmann, E. et al. Cancer Med. 2020 [42] | ** | ** | ** | 6 |
| Zhao, Q. et al. Front. Cell. Infect. Microbiol. 2020 [55] | ** | ** | ** | 6 |
| Zhang, S. et al. Theranostics 2020 [40] | *** | ** | ** | 7 |
| Kawasaky, M. et al. Cancer 2020 [56] | *** | ** | ** | 7 |
| Li, D. et al. Microb. Phatog. 2020 [58] | ** | ** | ** | 6 |
| Wei, A.L. et al. World J. Gastroenterol. 2020 [47] | ** | * | ** | 5 |
| Huang, K. et al. Front. Cell. Infect. Microbiol. 2021 [49] | ** | ** | ** | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reitano, E.; de’Angelis, N.; Gavriilidis, P.; Gaiani, F.; Memeo, R.; Inchingolo, R.; Bianchi, G.; de’Angelis, G.L.; Carra, M.C. Oral Bacterial Microbiota in Digestive Cancer Patients: A Systematic Review. Microorganisms 2021, 9, 2585. https://doi.org/10.3390/microorganisms9122585
Reitano E, de’Angelis N, Gavriilidis P, Gaiani F, Memeo R, Inchingolo R, Bianchi G, de’Angelis GL, Carra MC. Oral Bacterial Microbiota in Digestive Cancer Patients: A Systematic Review. Microorganisms. 2021; 9(12):2585. https://doi.org/10.3390/microorganisms9122585
Chicago/Turabian StyleReitano, Elisa, Nicola de’Angelis, Paschalis Gavriilidis, Federica Gaiani, Riccardo Memeo, Riccardo Inchingolo, Giorgio Bianchi, Gian Luigi de’Angelis, and Maria Clotilde Carra. 2021. "Oral Bacterial Microbiota in Digestive Cancer Patients: A Systematic Review" Microorganisms 9, no. 12: 2585. https://doi.org/10.3390/microorganisms9122585
APA StyleReitano, E., de’Angelis, N., Gavriilidis, P., Gaiani, F., Memeo, R., Inchingolo, R., Bianchi, G., de’Angelis, G. L., & Carra, M. C. (2021). Oral Bacterial Microbiota in Digestive Cancer Patients: A Systematic Review. Microorganisms, 9(12), 2585. https://doi.org/10.3390/microorganisms9122585