


Acute Rickettsiosis Triggering Plasmodium vivax Relapse in a Returned Traveler: A Case Report and Clinical Review of Travel-Related Coinfections

 , and
, and {kind=link}
{kind=link}
Abstract
1. Introduction
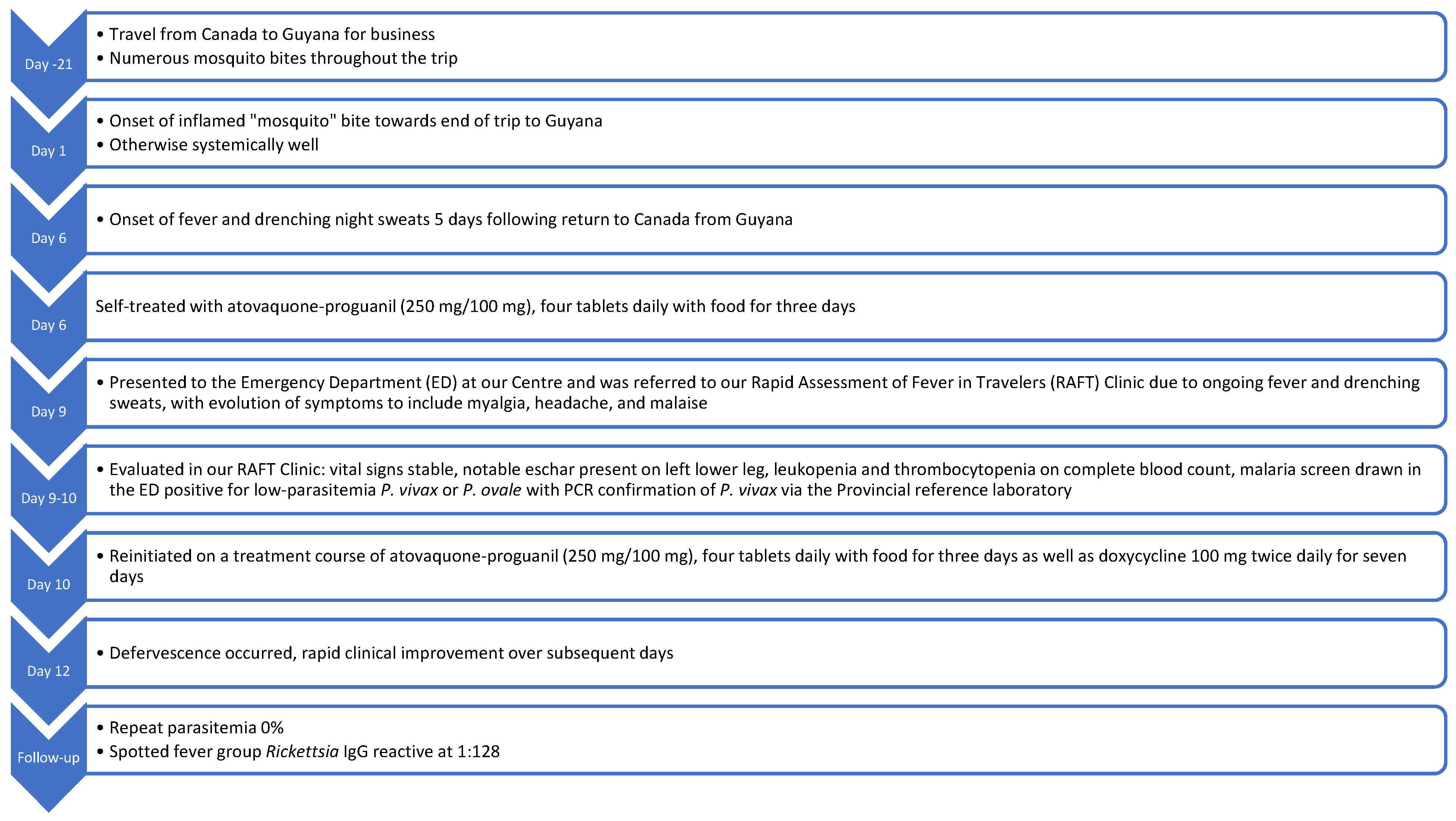
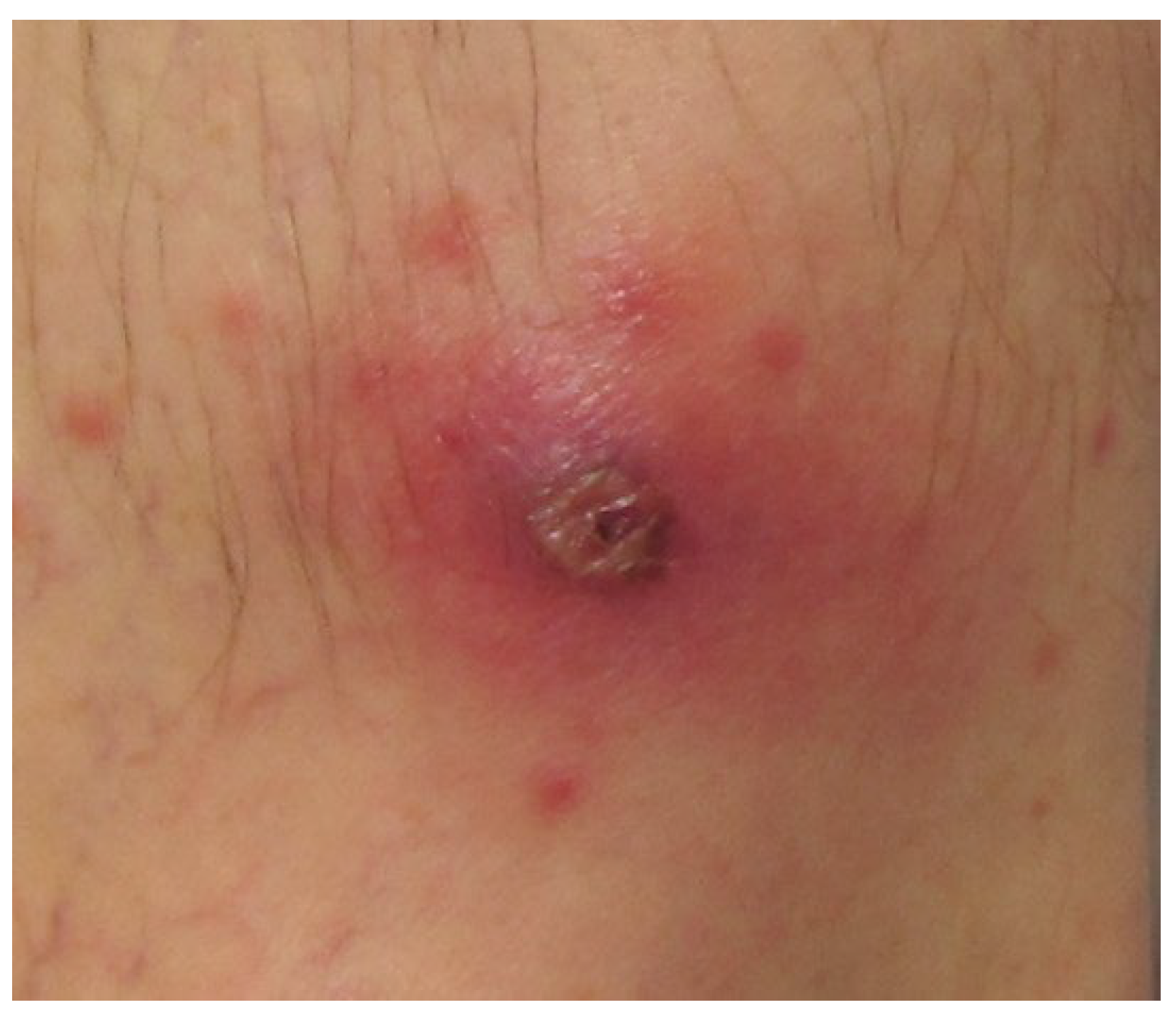
2. Clinical Case
3. Discussion
3.1. Rickettsia in South America
3.2. Rickettsia and Malaria Co-Infection
3.3. Rickettsia as a Trigger for Malaria Relapse
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, D.R. Health problems in a large cohort of Americans traveling to developing countries. J. Travel Med. 2000, 7, 259–266. [Google Scholar] [CrossRef]
- Freedman, D.O.; Weld, L.H.; Kozarsky, P.E.; Fisk, T.; Robins, R.; von Sonnenburg, F.; Keystone, J.S.; Pandey, P.; Cetron, M.S. Spectrum of disease and relation to place of exposure among ill returned tbravelers. N. Engl. J. Med. 2006, 354, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Committee to Advise on Tropical Medicine and Travel (CATMAT). Canadian Recommendations for the Prevention and Treatment of Malaria; Public Health Agency of Canada: Ottawa, ON, Canada, 2025; Available online: https://www.canada.ca/en/public-health/services/catmat/canadian-recommendations-prevention-treatment-malaria.html (accessed on 27 June 2025).
- Abdad, M.Y.; Stenos, J.; Graves, S. Rickettsia felis, an emerging flea-transmitted human pathogen. Emerg. Health Threat. J. 2011, 4, 7168. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stewart, G.; Stewart, A.G.A. An Update on the Laboratory Diagnosis of Rickettsia spp. Infection. Pathogens 2021, 10, 1319. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sirisena, P.D.N.N.; Mahilkar, S.; Sharma, C.; Jain, J.; Sunil, S. Concurrent dengue infections: Epidemiology & clinical implications. Indian J. Med. Res. 2021, 154, 669–679. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Deresinski, S. Concurrent Plasmodium vivax malaria and dengue. Emerg. Infect. Dis. 2006, 12, 1802. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lääveri, T.; Pakkanen, S.H.; Antikainen, J.; Riutta, J.; Mero, S.; Kirveskari, J.; Kantele, A. High number of diarrhoeal co-infections in travellers to Benin, West Africa. BMC Infect. Dis. 2014, 14, 81. [Google Scholar] [CrossRef]
- Lupi, O.; Ridolfi, F.; da Silva, S.; Zanini, G.M.; Lavigne, A.; Nogueira, R.M.; da Cruz Mde, F.; Daniel-Ribeiro, C.T.; Brasil, P. Dengue infection as a potential trigger of an imported Plasmodium ovale malaria relapse or a long incubation period in a non-endemic malaria region. Int. J. Infect. Dis. 2016, 44, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Kariyawasam, R.; Lecce, C.; Tan, K.; Boggild, A.K. Don’t forget co-infections! A case of intercurrent Plasmodium vivax and dengue infection in a traveler to India and the Caribbean. Travel Med. Infect. Dis. 2019, 32, 101414. [Google Scholar] [CrossRef] [PubMed]
- Phuong, M.; Lau, R.; Ralevski, F.; Boggild, A.K. Survival analysis of diagnostic assays in Plasmodium falciparum malaria. Malar. J. 2015, 14, 350. [Google Scholar] [CrossRef]
- Alvarez-Londoño, J.; Giraldo-Noreña, D.F.; Martínez-Sánchez, E.T.; Rivera-Páez, F.A.; Matta, N.E. Molecular survey of Rickettsia spp. in ticks infesting wild animals in six departments in Colombia. Ticks Tick-Borne Dis. 2024, 15, 102381. [Google Scholar] [CrossRef] [PubMed]
- Public Health Ontario. Rickettsia Testing—Test Algorithm for Rocky Mountain Spotted Fever Group and MURINE Typhus; Public Health Ontario: Toronto, ON, Canada, 2025; Available online: https://www.publichealthontario.ca/en/laboratory-services/test-information-index/rickettsia-serology (accessed on 27 June 2025).
- Parola, P.; Paddock, C.D.; Socolovschi, C.; Labruna, M.B.; Mediannikov, O.; Kernif, T.; Abdad, M.Y.; Stenos, J.; Bitam, I.; Fournier, P.E.; et al. Update on tick-borne rickettsioses around the world: A geographic approach. Clin. Microbiol. Rev. 2013, 26, 657–702, Erratum in: Clin. Microbiol. Rev. 2014, 27, 166. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lokida, D.; Hadi, U.; Lau, C.Y.; Kosasih, H.; Liang, C.J.; Rusli, M.; Sudarmono, P.; Lukman, N.; Laras, K.; Asdie, R.H.; et al. Underdiagnoses of Rickettsia in patients hospitalized with acute fever in Indonesia: Observational study results. BMC Infect. Dis. 2020, 20, 364. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, M.P.; Horta, M.C.; Melo, D.R.X.; Takeda, G.A.C.G.; Arraes-Santos, A.I.; Martins, T.F.; Pinter, A. Eco-epidemiological analysis of Rickettsia parkeri in domestic dogs and Amblyomma ovale ticks in the Atlantic rainforest of Northeast Brazil. Rev. Bras. Parasitol. Veterinária 2024, 33, e012524. [Google Scholar] [CrossRef]
- Kmetiuk, L.B.; Paula, W.V.F.; Pádua, G.T.; Delai, R.R.; Freitas, A.R.; Farinhas, J.H.; de Paula, L.G.F.; Giuffrida, R.; Pimpão, C.T.; Álvares Santarém, V.; et al. Epidemiology of Rickettsia spp. in Atlantic rainforest areas of island and seashore mainland, southern Brazil. Transbound. Emerg. Dis. 2022, 69, 3597–3605. [Google Scholar] [CrossRef]
- Parola, P.; Matsumoto, K.; Socolovschi, C.; Parzy, D.; Raoult, D. A tick-borne rickettsia of the spotted-fever group, similar to Rickettsia amblyommii, in French Guyana. Ann. Trop. Med. Parasitol. 2007, 101, 185–188. [Google Scholar] [CrossRef]
- Zhang, Y.Y.; Sun, Y.Q.; Chen, J.J.; Teng, A.Y.; Wang, T.; Li, H.; Hay, S.I.; Fang, L.Q.; Yang, Y.; Liu, W. Mapping the global distribution of spotted fever group rickettsiae: A systematic review with modelling analysis. Lancet Digit. Health 2023, 5, e5–e15. [Google Scholar] [CrossRef]
- Boggild, A.K.; Ghesquiere, W.; McCarthy, A. For the Committee to Advise on Tropical Medicine and Travel. Fever in the Returning International Traveller: Initial Assessment Guidelines. Can. Commun. Dis. Rep. 2011, 37, 1–15. Available online: https://www.canada.ca/en/public-health/services/reports-publications/canada-communicable-disease-report-ccdr/monthly-issue/2011-37/canada-communicable-disease-report-acs-3.html (accessed on 27 June 2025). [CrossRef]
- Van Eekeren, L.E.; de Vries, S.G.; Wagenaar, J.F.P.; Spijker, R.; Grobusch, M.P.; Goorhuis, A. Under-diagnosis of rickettsial disease in clinical practice: A systematic review. Travel Med. Infect. Dis. 2018, 26, 7–15. [Google Scholar] [CrossRef]
- Tay, S.T.; Kho, K.L.; Vythilingam, I.; Ooi, C.H.; Lau, Y.L. Investigation of possible rickettsial infection in patients with malaria. Trop. Biomed. 2019, 36, 257–262. [Google Scholar] [PubMed]
- Mediannikov, O.; Socolovschi, C.; Edouard, S.; Fenollar, F.; Mouffok, N.; Bassene, H.; Diatta, G.; Tall, A.; Niangaly, H.; Doumbo, O.; et al. Common epidemiology of Rickettsia felis infection and malaria, Africa. Emerg. Infect. Dis. 2013, 9, 1775–1783. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chu, C.S.; White, N.J. Management of relapsing Plasmodium vivax malaria. Expert Rev. Anti-Infect. Ther. 2016, 14, 885–900. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, C.; Zanghi, G.; Vaughan, A.M.; Kappe, S.H.I. Plasmodium vivax Latent Liver Stage Infection and Relapse: Biological Insights and New Experimental Tools. Annu. Rev. Microbiol. 2021, 75, 87–106. [Google Scholar] [CrossRef] [PubMed]
- Shanks, G.D.; White, N.J. The activation of vivax malaria hypnozoites by infectious diseases. Lancet Infect. Dis. 2013, 13, 900–906. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagga, R.; Fuller, C.; Shahzad, K.; Bado, E.; Joshi, J.; Fernando, D.; Hempel, A.; Boggild, A.K. Acute Rickettsiosis Triggering Plasmodium vivax Relapse in a Returned Traveler: A Case Report and Clinical Review of Travel-Related Coinfections. Pathogens 2025, 14, 768. https://doi.org/10.3390/pathogens14080768
Bagga R, Fuller C, Shahzad K, Bado E, Joshi J, Fernando D, Hempel A, Boggild AK. Acute Rickettsiosis Triggering Plasmodium vivax Relapse in a Returned Traveler: A Case Report and Clinical Review of Travel-Related Coinfections. Pathogens. 2025; 14(8):768. https://doi.org/10.3390/pathogens14080768
Chicago/Turabian StyleBagga, Ruchika, Charlotte Fuller, Kalsoom Shahzad, Ezra Bado, Judith Joshi, Dileesha Fernando, Amanda Hempel, and Andrea K. Boggild. 2025. "Acute Rickettsiosis Triggering Plasmodium vivax Relapse in a Returned Traveler: A Case Report and Clinical Review of Travel-Related Coinfections" Pathogens 14, no. 8: 768. https://doi.org/10.3390/pathogens14080768
APA StyleBagga, R., Fuller, C., Shahzad, K., Bado, E., Joshi, J., Fernando, D., Hempel, A., & Boggild, A. K. (2025). Acute Rickettsiosis Triggering Plasmodium vivax Relapse in a Returned Traveler: A Case Report and Clinical Review of Travel-Related Coinfections. Pathogens, 14(8), 768. https://doi.org/10.3390/pathogens14080768