
Advancing Extrapulmonary Tuberculosis Diagnosis: Potential of MPT64 Immunochemistry-Based Antigen Detection Test in a High-TB, Low-HIV Endemic Setting



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Population
2.2. Study Questionnaire and Data Collection
2.3. Biological Sample Collection, Processing, and Transportation
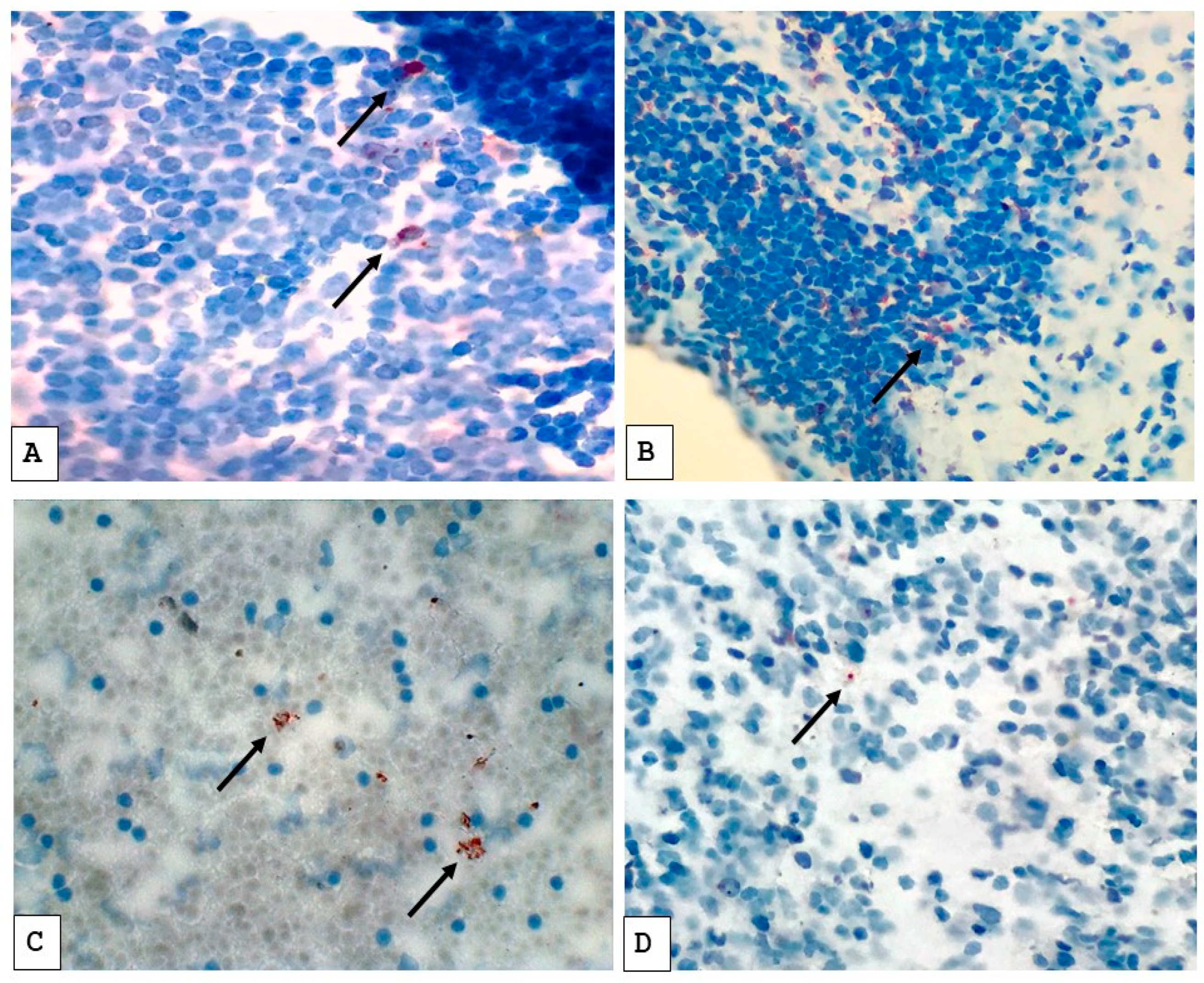
2.4. Assessment of Immunostainings with MPT64
2.5. Patient Categorization and Disease Severity Criteria
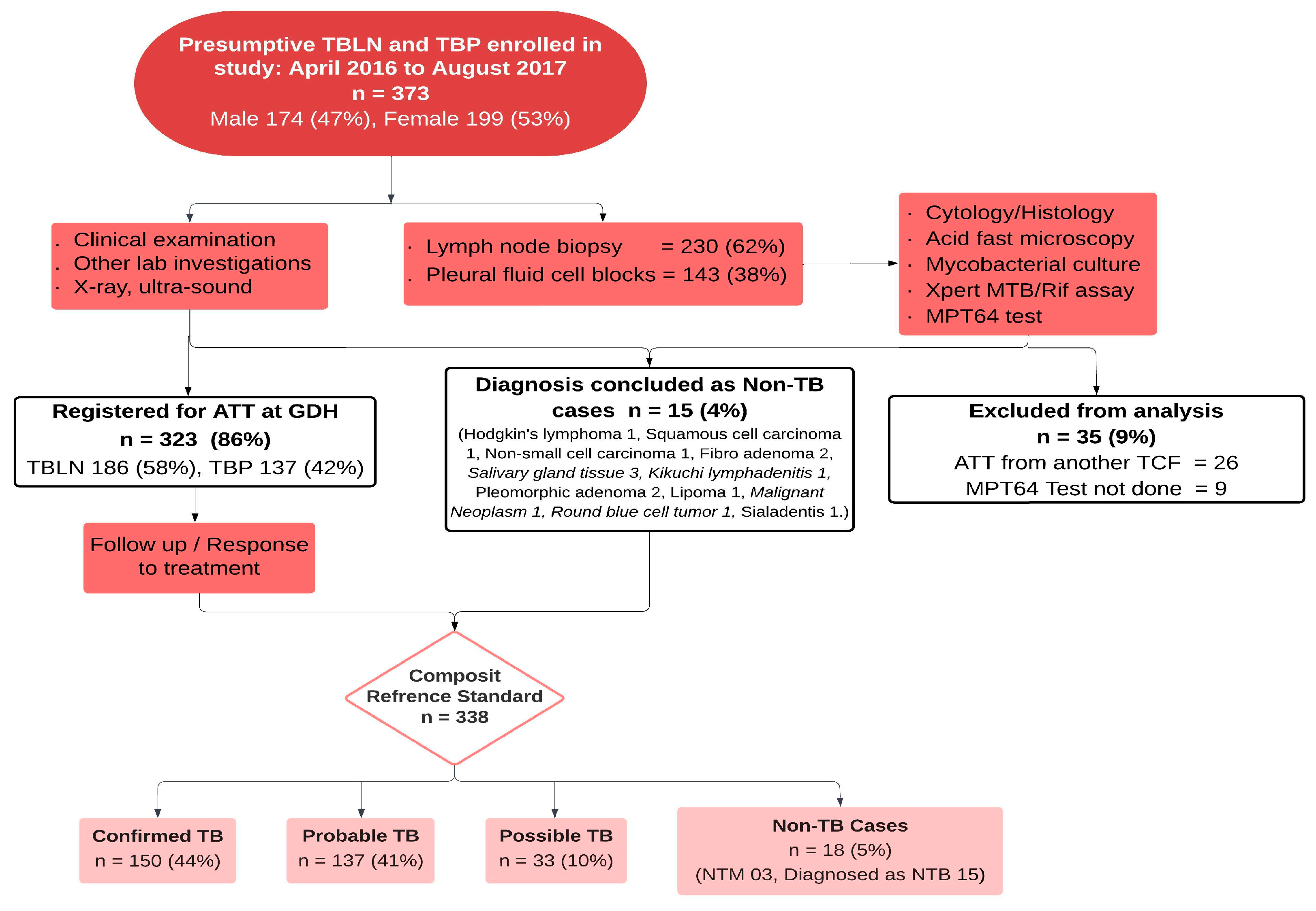
2.6. Study Flow
2.7. Statistical Analysis
2.8. Ethics Approval and Consent to Participate
3. Results
3.1. Patient Diagnostics and Clinical Characteristics
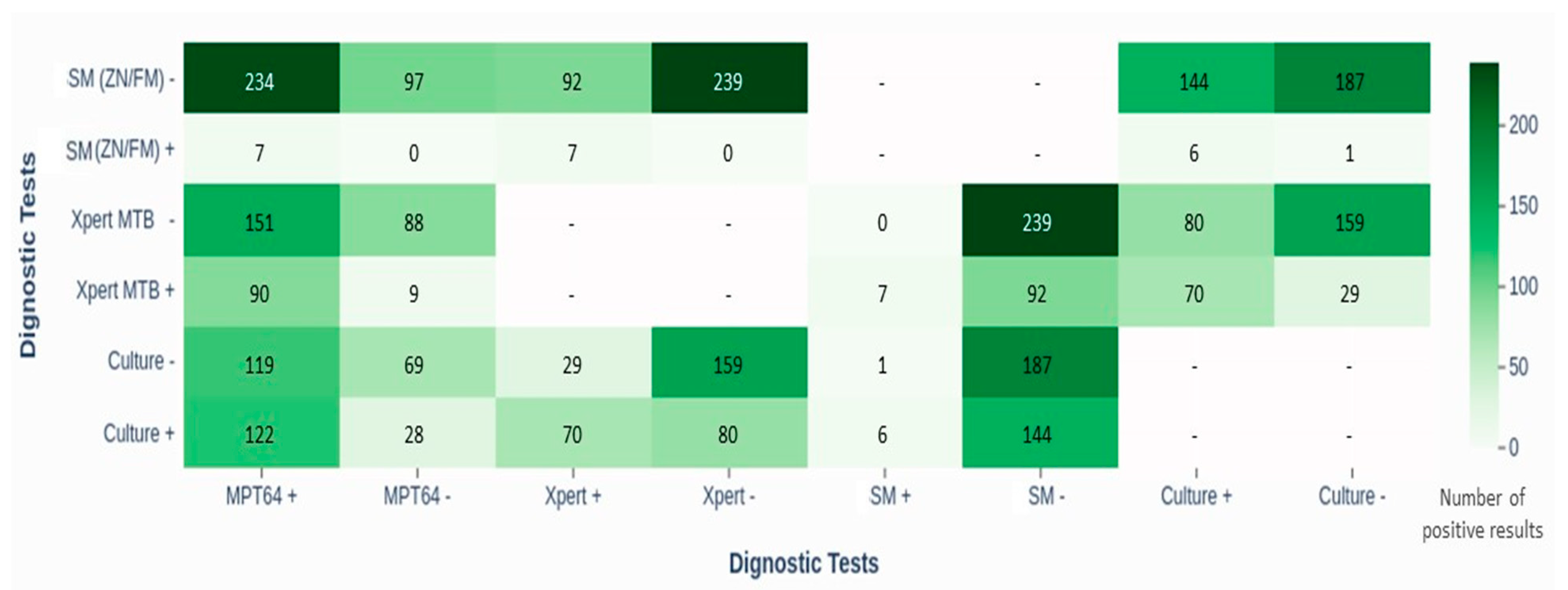
3.2. Validity and Comparative Performance of Diagnostic Tests
3.3. Impact of Diagnostic Delays and Disease Severity on Test Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ATT | Anti-tuberculosis treatment |
| CRS | Composite reference standard |
| EPTB | Extrapulmonary tuberculosis |
| GDH | Gulab Devi Hospital |
| HIV | Human immunodeficiency virus |
| HPGs | Histopathological groups |
| ICC | Immunocytochemistry |
| IHC | Immunohistochemistry |
| MOTT | Mycobacterium other than tuberculosis |
| MTB | Mycobacterium tuberculosis |
| NPV | Negative predictive value |
| NTM | Non-tuberculosis mycobacterium |
| PPV | Positive predictive value |
| SKMH | Shaukat Khanum Memorial Hospital |
| STB | Suggestive of TB |
| TB | Tuberculosis |
| TBLN | Tuberculous lymphadenitis |
| TBP | Tuberculous pleuritis |
| WHO | World Health Organization |
References
- Purohit, M.; Mustafa, T. Laboratory Diagnosis of Extrapulmonary Tuberculosis (EPTB) in Resource- constrained Setting: State of the Art, Challenges and the Need. J. Clin. Diagn. Res. 2015, 9, 1–6. [Google Scholar] [CrossRef]
- Tahseen, S.; Khanzada, F.M.; Baloch, A.Q.; Abbas, Q.; Bhutto, M.M.; Alizai, A.W.; Zaman, S.; Qasim, Z.; Durrani, M.N.; Farough, M.K.; et al. Extrapulmonary tuberculosis in Pakistan- A nation-wide multicenter retrospective study. PLoS ONE 2020, 15, 1–16. [Google Scholar] [CrossRef]
- Gopalaswamy, R.; Dusthackeer, V.N.A.; Kannayan, S.; Subbian, S. Extrapulmonary Tuberculosis—An Update on the Diagnosis, Treatment and Drug Resistance. J. Respir. 2021, 1, 141–164. [Google Scholar] [CrossRef]
- Golden, M.P.; Vikram, H.R. Extrapulmonary Tuberculosis: An Overview. Am. Fam. Physician 2005, 72, 1761–1768. [Google Scholar] [PubMed]
- Lee, J.Y. Diagnosis and treatment of extrapulmonary tuberculosis. Tuberc. Respir. Dis. 2015, 78, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Tadele, A.; Beyene, D.; Hussein, J.; Gemechu, T.; Birhanu, A.; Mustafa, T.; Tsegaye, A.; Aseffa, A.; Sviland, L. Immunocytochemical detection of Mycobacterium Tuberculosis complex specific antigen, MPT64, improves diagnosis of tuberculous lymphadenitis and tuberculous pleuritis. BMC Infect. Dis. 2014, 14, 585. [Google Scholar] [CrossRef]
- Zhai, K.; Lu, Y.; Shi, H.Z. Tuberculous pleural effusion. J. Thorac. Dis. 2016, 8, E486–E494. [Google Scholar] [CrossRef]
- WHO. Global Tuberculosis Report 2023. Geneva. 2023. Available online: https://iris.who.int/handle/10665/373828 (accessed on 11 December 2024).
- WHO. Global Tuberculosis Report 2024. Geneva. 2024. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2024 (accessed on 11 December 2024).
- Sharma, K.; Appannanavar, S.B.; Goyal, K.; Sharma, A. Recent Advances in the Diagnosis of Tuberculosis. J. Postgrad. Med. Educ. Res. 2013, 47, 181–187. [Google Scholar] [CrossRef]
- Maclean, E.; Kohli, M.; Weber, S.F.; Suresh, A. Advances in Molecular Diagnosis of Tuberculosis. J. Clin. Microbiol. 2020, 58, 1–13. [Google Scholar] [CrossRef]
- Mustafa, T.; Wiker, H.G.; Mfinanga, S.G.M.; Mørkve, O. Immunohistochemistry using a Mycobacterium tuberculosis complex specific antibody for improved diagnosis of tuberculous lymphadenitis. Mod. Pathol. 2006, 19, 1606–1614. [Google Scholar] [CrossRef]
- Lawn, S.D.; Zumla, A.I. Diagnosis of extrapulmonary tuberculosis using the Xpert® MTB/RIF assay. Eur. Respir. J. 2013, 10, 631–635. [Google Scholar] [CrossRef]
- Lawn, S.D.; Mwaba, P.; Bates, M.; Piatek, A.; Alexander, H.; Marais, B.J.; Cuevas, L.E.; McHugh, T.D.; Zijenah, L.; Kapata, N.; et al. Advances in tuberculosis diagnostics: The Xpert MTB/RIF assay and future prospects for a point-of-care test. Lancet Infect. Dis. 2016, 13, 349–361. [Google Scholar] [CrossRef] [PubMed]
- Jørstad, M.D.; Marijani, M.; Dyrhol-Riise, A.M.; Sviland, L.; Mustafa, T. MPT64 antigen detection test improves routine diagnosis of extrapulmonary tuberculosis in a low-resource setting: A study from the tertiary care hospital in Zanzibar. PLoS ONE 2018, 13, e0196723. [Google Scholar] [CrossRef]
- Arora, J.; Kumar, G.; Verma, A.K.; Bhalla, M.; Sarin, R.; Myneedu, V.P. Utility of MPT64 Antigen Detection for Rapid Confirmation of Mycobacterium Tuberculosis Complex. J. Glob. Infect. Dis. 2015, 7, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.G.; Urs, T.A.; Ranganath, R.R. MPT 64 Antigen detection for rapid confirmation of M. tuberculosis isolates. BMC Res. Notes 2011, 4, 79. [Google Scholar] [CrossRef] [PubMed]
- Hoel, I.M.; Sviland, L.; Syre, H.; Dyrhol-Riise, A.M.; Skarstein, I.; Jebsen, P.; Jørstad, M.D.; Wiker, H.; Mustafa, T. Diagnosis of extrapulmonary tuberculosis using the MPT64 antigen detection test in a high-income low tuberculosis prevalence setting. BMC Infect. Dis. 2020, 20, 1–12. [Google Scholar] [CrossRef]
- Mustafa, T.; Leversen, N.A.; Sviland, L.; Wiker, H.G. Differential in vivo expression of mycobacterial antigens in Mycobacterium tuberculosis infected lungs and lymph node tissues. BMC Infect. Dis. 2014, 14, 535. [Google Scholar] [CrossRef]
- Purohit, M.R.; Sviland, L.; Wiker, H.; Mustafa, T. Rapid and Specific Diagnosis of Extrapulmonary Tuberculosis by Immunostaining of Tissues and Aspirates with Anti-MPT64. Appl. Immunohistochem. Mol. Morphol. 2017, 25, 282–288. [Google Scholar] [CrossRef]
- Tahseen, S.; Ambreen, A.; Masood, F.; Qadir, M.; Hussain, A.; Jamil, M.; Safdar, N.; Sviland, L.; Mustafa, T. Primary drug resistance in extra-pulmonary tuberculosis: A hospital-based prospective study from Pakistan. Int. J. Tuberc. Lung Dis. 2019, 23, 900–906. [Google Scholar] [CrossRef]
- Said, K.; Hella, J.; Mhalu, G.; Chiryankubi, M.; Masika, E.; Maroa, T.; Mhimbira, F.; Kapalata, N.; Fenner, L. Diagnostic delay and associated factors among patients with pulmonary tuberculosis in Dar es Salaam, Tanzania. Infect. Dis. Poverty 2017, 6, 64. [Google Scholar] [CrossRef]
- Nagai, S.; Wiker, H.G.; Harboe, M.; Kinomoto, M. Isolation and partial characterization of major protein antigens in the culture fluid of Mycobacterium tuberculosis. Infect. Immun. 1991, 59, 372–382. [Google Scholar] [CrossRef]
- Pal, R.; Bisht, M.K.; Mukhopadhyay, S. Secretory proteins of Mycobacterium tuberculosis and their roles in modulation of host immune responses: Focus on therapeutic targets. FEBS J. 2022, 289, 4146–4171. [Google Scholar] [CrossRef]
- WHO. Module 3: Diagnosis Rapid Diagnostics for Tuberculosis Detection. Consolidated Guidelines on Tuberculosis; World Health Organization: Geneva, Switzerland, 2021; p. 164. Available online: https://www.who.int/publications/i/item/9789240030589 (accessed on 11 December 2024).
- WHO. Module 4: Treatment Drug-susceptible Tuberculosis Treatment. Module 5: Management of Tuberculosis in Children and Adolescents. Operational Handbook on Tuberculosis; World Health Organization: Geneva, Switzerland, 2022; p. 264. Available online: https://apps.who.int/iris/bitstream/handle/10665/340256/9789240022614-eng.pdf (accessed on 11 December 2024).
- Khan, S.; Omar, T.; Michelow, P. Effectiveness of the cell block technique in diagnostic cytopathology. J. Cytol. 2012, 29, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Grønningen, E.; Nanyaro, M.; Sviland, L.; Ngadaya, E.; Muller, W.; Torres, L.; Mfinanga, S.; Mustafa, T. Improved diagnosis of extrapulmonary tuberculosis in adults with and without HIV in Mbeya, Tanzania using the MPT64 antigen detection test. PLoS Glob. Public Health 2022, 2, 29. [Google Scholar] [CrossRef] [PubMed]
- Roy, B.; Shak, H.J.; Lee, Y.C.G. Pleural fluid investigations for pleural infections. J. Lab. Precis. Med. 2021, 6, 1–13. [Google Scholar] [CrossRef]
- Shaozae, C.K.; Das, D.; Kumar, M. Diagnosis of Tuberculosis in Low-Resource Settings: Overcoming Challenges Within Laboratory Practice. Eur. Med. J. 2023, 8, 82–91. [Google Scholar] [CrossRef]
- Purohit, M.R.; Mustafa, T.; Wiker, H.G.; Mørkve, O.; Sviland, L. Immunohistochemical diagnosis of abdominal and lymph node tuberculosis by detecting Mycobacterium tuberculosis complex specific antigen MPT64. Diagn. Pathol. 2007, 2, 36. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Confirmed TB Case | Positive Mycobacterial Culture |
|---|---|
| Probable TB case | Clinically presumptive extrapulmonary tuberculosis AND
|
| Possible TB case | Clinically presumptive extrapulmonary tuberculosis AND one of the following:
|
| Non-TB case (control subject) | Negative Mycobacterium tuberculosis complex and/or detected NTM on culture AND cytology/histology examination concluded specific diagnosis other than TB. |
| TB, tuberculosis; NTM, non-tuberculous mycobacteria; ATT, anti-tuberculosis treatment. Definitions:
| |
| Characteristics | N = 338 | EPTB Cases | Non-EPTB Cases |
|---|---|---|---|
| n = 320 (95%) | n = 18 (5%) | ||
| Gender | |||
| Male | 160 (47) | 155 (48) | 5 (28) |
| Female | 178 (53) | 165 (52) | 13 (72) |
| Age (years) | |||
| 0–14 | 54 (16) | 53 (17) | 1 (6) |
| 15–44 | 245 (72) | 231 (72) | 14 (78) |
| ≥45 | 39 (12) | 36 (11) | 3 (17) |
| Presumptive EPTB site | |||
| Lymphadenitis | 201 (59) | 186 (58) | 15 (83) |
| Pleuritis | 137 (41) | 134 (42) | 3 (17) |
| HIV status | |||
| Positive | 0 (0) | 0 (0) | 0 (0) |
| Non-reactive | 80 (24) | 80 (25) | 0 (0) |
| Not done | 258 (76) | 240 (75) | 18 (100) |
| Characteristics | N | Positive Test Results/Total Tests (%) | |||
|---|---|---|---|---|---|
| EPTB Cases | Non-EPTB Cases | ||||
| TBP | TBLN | TBP | TBLN | ||
| TB diagnostic tests | |||||
| Microscopy (ZN/FM) | 338 | 0/134 (0) | 7/186 (4) | 0/3 (0) | 0/15 (0) |
| Xpert MTB/Rif assay | 338 | 9/134 (7) | 89/186 (48) | 0/3 (0) | 1/15 (7) |
| Culture | 338 | 42/134 (31) | 108/186 (58) | 0/3 (0) | 0/15 (0) |
| MPT64 | 338 | 69/134 (51) | 157/186 (84) | 3/3 (100) | 12/15 (80) |
| Histopathology reports | |||||
| Consistent with TB | 168 | 0/134 (0) | 168/186 (90) | 0/3 (0) | 0/15 (0) |
| Concluded as non-TB | 15 | 0/134 (0) | 0/186 (0) | 0/3 (0) | 15/15 (100) |
| Others | 17 | 0/134 (0) | 17/186 (9) | 0/3 (0) | 0/15 (0) |
| Not done | 138 | 134/134 (100) | 1/186 (1) | 3/3 (0) | 0/15 (0) |
| Characteristics | Sensitivity | Specificity | PPV | NPV | Accuracy |
|---|---|---|---|---|---|
| % (95% CI) | % (95% CI) | % | % | % | |
| Culture as reference | |||||
| All cases | |||||
| MPT64 test | 81 (74.1–87.2) | 37 (29.8–44.0) | 51 | 71 | 56 |
| Xpert assay | 47 (38.5–55.0) | 85 (78.6–89.4) | 78 | 66 | 68 |
| SM (ZN/FM) | 4 (1.5–8.5) | 99 (97.1–99.9) | 86 | 56 | 57 |
| TB lymphadenitis | |||||
| MPT64 test | 91 (83.6–95.5) | 24 (15.5–33.6) | 58 | 69 | 60 |
| Xpert assay | 61 (51.2–70.3) | 74 (64.1–82.1) | 73 | 62 | 67 |
| SSM (ZN/FM) | 6 (2.1–11.7) | 99 (94.2–99.9) | 86 | 47 | 49 |
| TB pleuritis | |||||
| MPT64 test | 57 (41.0–72.3) | 49 (39.1–59.9) | 33 | 72 | 52 |
| Xpert assay | 10 (2.7–22.6) | 95 (88.1–98.3) | 44 | 70 | 69 |
| SM (ZN/FM) | 0 (0.0–8.4) | 100 (96.1–100) | - | 69 | 69 |
| CRS as reference | |||||
| All cases | |||||
| MPT64 test | 70 (65.0–75.4) | 15 (3.2–37.9) | 93 | 3 | 67 |
| Culture | 47 (41.2–52.8) | 100 (83.1–52.8) | 100 | 11 | 50 |
| Xpert assay | 31 (25.5–35.9) | 90 (68.3–98.8) | 98 | 8 | 34 |
| SM (ZN/FM) | 2 (0.8–4.5) | 100 (83.1–100) | 100 | 6 | 8 |
| TB lymphadenitis | |||||
| MPT64 test | 84 (78.2–89.2) | 18 (3.8–43.4) | 92 | 9 | 79 |
| Culture | 59 (51.2–65.9) | 100 (80.5–100) | 100 | 18 | 62 |
| Xpert assay | 48 (40.4–55.3) | 88 (63.6–98.5) | 98 | 13 | 51 |
| SM (ZN/FM) | 4 (1.5–7.7) | 100 (80.5–100) | 100 | 9 | 12 |
| TB pleuritis | |||||
| MPT64 test | 51 (42.7–60.2) | 0 (0.0–70.8) | 96 | 0 | 50 |
| Culture | 31 (23.6–39.9) | 100 (29.2–100) | 100 | 3 | 33 |
| Xpert assay | 7 (3.1–12.4) | 100 (29.2–100) | 100 | 2 | 9 |
| SM (ZN/FM) | 0 (0.0–2.7) | 100 (29.2–100) | - | 2 | 2 |
| n | MPT64 | Culture | Xpert | SM (ZN/FM) | |||||
|---|---|---|---|---|---|---|---|---|---|
| + | − | + | − | + | − | + | − | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Morphology STB | 168 | ||||||||
| HPG-1 | 3 | 3 (100) | 0 (0) | 2 (67) | 1 (33) | 1 (33) | 2 (67) | 0 (0) | 3 (100) |
| HPG-2 | 90 | 73 (81) | 17 (19) | 58 (64) | 32 (36) *1 | 39 (43) | 51 (57) ^3 | 2 (2) | 88 (98) |
| HPG-3 | 65 | 57 (88) | 8 (12) | 35 (54) | 30 (46) *1 | 34 (52) | 31 (48) | 3 (5) | 62 (95) |
| HPG-4 | 10 | 10 (100) | 0 (0) | 7 (70) | 3 (30) | 7 (70) | 3 (30) | 1 (10) | 9 (90) |
| Morphology NSTB | 32 | ||||||||
| HPG-0 | 17 | 13 (76) | 4 (24) | 6 (35) | 11 (65) | 7 (41) | 10 (59) ^1 | 1 (6) | 16 (94) |
| HPG-5 | 15 | 12 (80) | 3 (20) | 0 (0) | 15 (10) *1 | 1 (7) | 14 (93) ^1 | 0 (0) | 15 (100) |
| Diagnostic delay TBLN | 186 | ||||||||
| Delayed | 110 | 94 (85) | 16 (15) | 63 (57) | 47 (43) *1 | 49 (45) | 61 (55) ^3 | 5 (5) | 105 (98) |
| Not-delayed | 76 | 63 (83) | 13 (17) | 45 (59) | 31 (41) *1 | 40 (53) | 36 (43) ^1 | 2 (3) | 74 (97) |
| Diagnostic delay TBP | 134 | ||||||||
| Delayed | 51 | 27 (53) | 24 (47) | 17 (33) | 34 (67) | 4 (8) | 47 (92) ^2 | 0 (0) | 83 (100) |
| Not-delayed | 83 | 42 (51) | 41 (49) | 25 (30) | 58 (70) | 5 (6) | 78 (94) ^4 | 0 (0) | 51 (100) |
| Disease severity TBLN | 201 | ||||||||
| Severe | 57 | 47 (82) | 10 (18) | 38 (67) | 19 (33) | 23 (40) | 34 (60) ^3 | 5 (9) | 52 (91) |
| Less severe | 144 | 122 (85) | 22 (15) | 70 (49) | 74 (51) *3 | 67 (47) | 77 (53) ^2 | 2 (1) | 142 (99) |
| Disease severity TBP | 137 | ||||||||
| Severe | 58 | 22 (38) | 36 (62) | 19 (33) | 39 (67) | 5 (6) | 74 (94) ^1 | 0 (0) | 58 (100) |
| Less severe | 79 | 50 (63) | 29 (37) | 23 (29) | 56 (71) *3 | 4 (7) | 54 (93) ^5 | 0 (0) | 79 (100) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wali, A.; Safdar, N.; Ambreen, A.; Loya, A.; Mustafa, T. Advancing Extrapulmonary Tuberculosis Diagnosis: Potential of MPT64 Immunochemistry-Based Antigen Detection Test in a High-TB, Low-HIV Endemic Setting. Pathogens 2025, 14, 741. https://doi.org/10.3390/pathogens14080741
Wali A, Safdar N, Ambreen A, Loya A, Mustafa T. Advancing Extrapulmonary Tuberculosis Diagnosis: Potential of MPT64 Immunochemistry-Based Antigen Detection Test in a High-TB, Low-HIV Endemic Setting. Pathogens. 2025; 14(8):741. https://doi.org/10.3390/pathogens14080741
Chicago/Turabian StyleWali, Ahmad, Nauman Safdar, Atiqa Ambreen, Asif Loya, and Tehmina Mustafa. 2025. "Advancing Extrapulmonary Tuberculosis Diagnosis: Potential of MPT64 Immunochemistry-Based Antigen Detection Test in a High-TB, Low-HIV Endemic Setting" Pathogens 14, no. 8: 741. https://doi.org/10.3390/pathogens14080741
APA StyleWali, A., Safdar, N., Ambreen, A., Loya, A., & Mustafa, T. (2025). Advancing Extrapulmonary Tuberculosis Diagnosis: Potential of MPT64 Immunochemistry-Based Antigen Detection Test in a High-TB, Low-HIV Endemic Setting. Pathogens, 14(8), 741. https://doi.org/10.3390/pathogens14080741