Cryptococcal Endocarditis in Humans—A Narrative Review

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
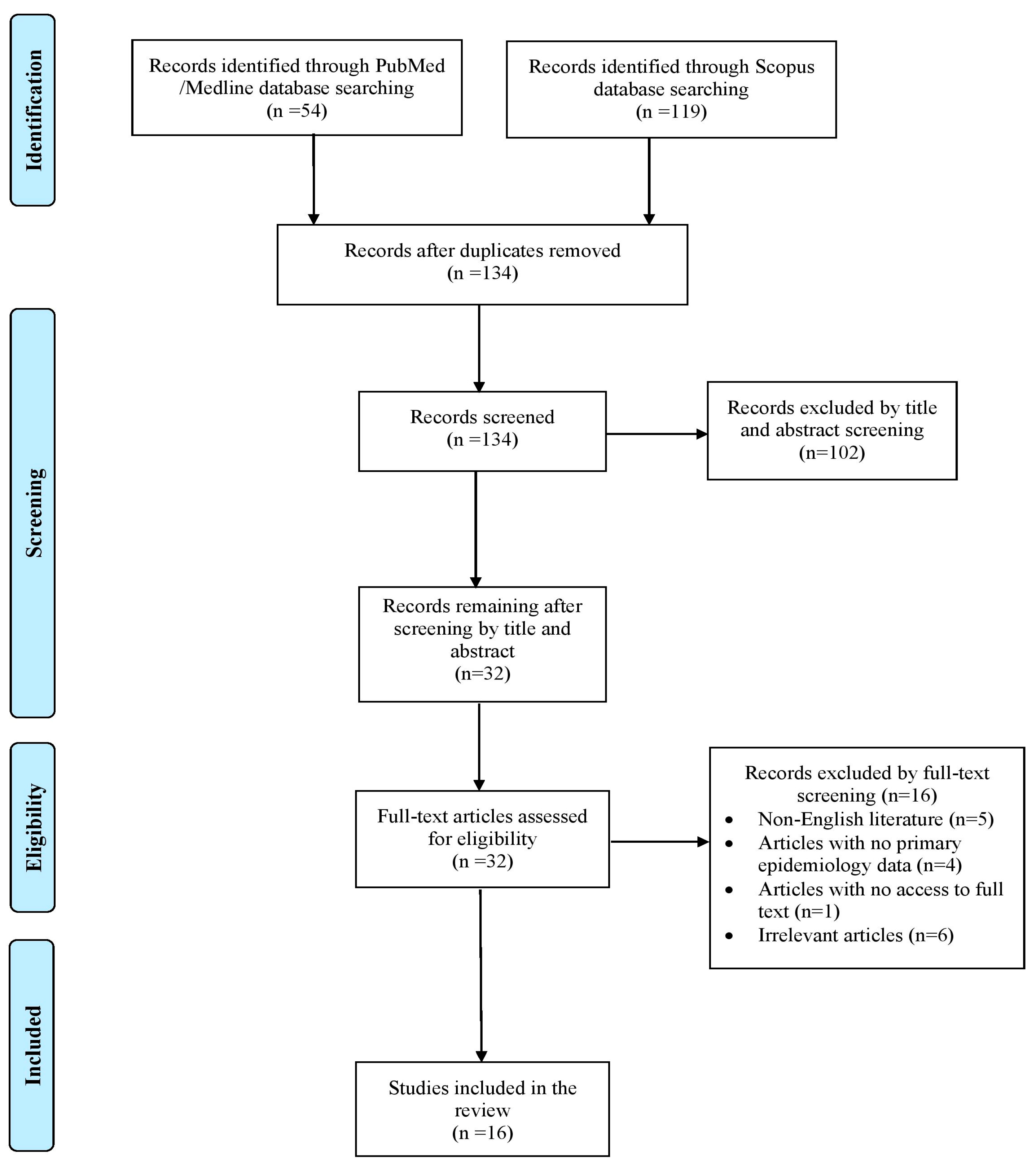
2.1. Search Strategy and Inclusion and Exclusion Criteria
2.2. Data Extraction and Definitions
3. Results
3.1. Included Studies’ Characteristics
3.2. Epidemiology of Cryptococcal Endocarditis
3.3. Microbiology and Diagnosis of Cryptococcus spp. Endocarditis
3.4. Clinical Characteristics of Cryptococcal Endocarditis
3.5. Treatment and Outcomes of Cryptococcal Endocarditis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thipmontree, W.; Lerssuttipon, U.; Chunharas, P.; Kajeekul, R.; Lewrod, A.; Yongkiettrakul, S.; Kerdsin, A. Streptococcus suis endocarditis: Prognostic factors and antimicrobial resistance. Infection 2025, 1–9. [Google Scholar] [CrossRef]
- Ioannou, P.; Ziogou, A.; Giannakodimos, I.; Giannakodimos, A.; Baliou, S.; Samonis, G. Infective Endocarditis by Lactobacillus Species-A Narrative Review. Antibiotics 2024, 13, 53. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Gaca, J.G.; Chu, V.H. Management Considerations in Infective Endocarditis: A Review. JAMA 2018, 320, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Papakonstantinou, P.E.; Samonis, G.; Andrianaki, A.M.; Christofaki, M.; Dimopoulou, D.; Papadakis, J.; Gikas, A.; Kofteridis, D.P. Epidemiology, Microbiological and Clinical Features, Treatment, and Outcomes of Infective Endocarditis in Crete, Greece. Infect. Chemother. 2018, 50, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Badiee, P.; Amirghofran, A.A.; Ghazi Nour, M.; Shafa, M.; Nemati, M.H. Incidence and outcome of documented fungal endocarditis. Int. Cardiovasc. Res. J. 2014, 8, 152–155. [Google Scholar]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miró, J.M.; Fowler, V.G.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef]
- Nakajima, T.; Oba, Y.; Takashima, J.; Ueno, K.; Kikuchi, A.; Yamada, T.; Fukunami, M. Cryptococcus endocarditis: A case report and review of the literature. J. Infect. Chemother. Off. J. Jpn. Soc. Chemother. 2019, 25, 901–905. [Google Scholar] [CrossRef]
- Zhou, H.-X.; Ning, G.-Z.; Feng, S.-Q.; Jia, H.-W.; Liu, Y.; Feng, H.-Y.; Ruan, W.-D. Cryptococcosis of lumbar vertebra in a patient with rheumatoid arthritis and scleroderma: Case report and literature review. BMC Infect. Dis. 2013, 13, 128. [Google Scholar] [CrossRef]
- Adsul, N.; Kalra, K.L.; Jain, N.; Haritwal, M.; Chahal, R.S.; Acharya, S.; Jain, S. Thoracic cryptococcal osteomyelitis mimicking tuberculosis: A case report. Surg. Neurol. Int. 2019, 10, 81. [Google Scholar] [CrossRef]
- Fountain, J.H.; Rajagopalan, K.N.; Carroll, M.; Robbins, H.; Benvenuto, L.J.; Shimbo, D.; Marboe, C.C.; Arcasoy, S.M.; Pereira, M.R. Cryptococcus neoformans infective endocarditis after lung transplantation: A case report and review of the literature. Infect. Dis. Clin. Pract. 2021, 29, e457–e461. [Google Scholar] [CrossRef]
- McGuire, C.N.; Walter, D.J. Cryptococcus neoformans endocarditis in an immunocompetentpatient a case report. BMC Cardiovasc. Disord. 2022, 22, 565. [Google Scholar] [CrossRef] [PubMed]
- Alhaji, M.; Sadikot, R.T. Cryptococcal endocarditis. South. Med. J. 2011, 104, 363–364. [Google Scholar] [CrossRef]
- Blanc, V.; Lavarde, V.; Thanh, N.T.; Tri, H.H.Q.; Guillemain, R.; Amrein, C.; Carpentier, A. Postoperative Cryptococcus neoformans endocarditis. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 1996, 2, 66–69. [Google Scholar] [CrossRef]
- Elkhatib, W.; Kwon, J.Y.; Phillips, M.B. Overwhelming cryptococcosis complicated by cryptococcal endocarditis. BMJ Case Rep. 2022, 15, e247310. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.; Ahmad, S.; Roy, A.K. Cryptococcus neoformans infective endocarditis of native valves in an immunocompetent host. IDCases 2018, 12, 66–70. [Google Scholar] [CrossRef]
- Yavari, S.K.; Lapoint, D.; Levy, A.; Pourafkari, L. Cryptococcal endocarditis of native valve in a patient with systemic lupus erythematosus. North. Clin. Istanb. 2023, 10, 277. [Google Scholar] [CrossRef]
- Kowatari, R.; Suzuki, Y.; Daitoku, K.; Fukuda, I. Cryptococcal infective endocarditis in a child with acute lymphocytic leukaemia. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 642–644. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; He, S.; Lu, Z.; Ding, C.; Wang, Q.; Li, Q.; Pan, Y.; Huang, J. Cryptococcal endocarditis of native valves without immunodeficiency or drug abuse: A case report. J. Int. Med. Res. 2020, 48, 0300060520970763. [Google Scholar] [CrossRef]
- Colmers, R.A.; Irniger, W.; Steinberg, D.H. Cryptococcus neoformans endocarditis cured by amphotericin B. JAMA 1967, 199, 762–764. [Google Scholar] [CrossRef]
- Banerjee, U.; Gupta, K.; Venugopal, P. A case of prosthetic valve endocarditis caused by Cryptococcus neoformans var. neoformans. J. Med. Vet. Mycol. Bi-Mon. Publ. Int. Soc. Hum. Anim. Mycol. 1997, 35, 139–141. [Google Scholar]
- Lombardo, T.A.; Rabson, A.S.; Dodge, H.T. Mycotic endocarditis; report of a case due to Cryptococcus neoformans. Am. J. Med. 1957, 22, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Channell, L.; Matulis, W.S.; Hernandez, J.E. Prosthetic Valve Endocarditis Due to Cryptococcus neoformans. Infect. Dis. Clin. Pract. 1996, 5, 453–455. [Google Scholar] [CrossRef]
- Child, J.S.; MacAlpin, R.N.; Moyer, G.H.; Shanley, J.D.; Layfield, L.J. Coronary ostial embolus and mitral vegetation simulating a left atrial myxoma: A case of probable cryptococcal valvulitis. Clin. Cardiol. 1979, 2, 43–48. [Google Scholar] [CrossRef]
- Harford, C.G. Postoperative Fungal Endocarditis: Fungemia, Embolism, and Therapy. Arch. Intern. Med. 1974, 134, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Subramony, H.; Raghavan, B.; Hegde, M.G.; Subbaiyan, E.; Ramanathan, K. Cryptic Presentation of Cryptococcal Osteomyelitis in an Apparently Immunocompetent Individual. Eur. J. Case Rep. Intern. Med. 2023, 10, 003737. [Google Scholar] [CrossRef] [PubMed]
- Levitz, S.M. The ecology of Cryptococcus neoformans and the epidemiology of cryptococcosis. Rev. Infect. Dis. 1991, 13, 1163–1169. [Google Scholar] [CrossRef]
- Kangogo, M.; Boga, H.; Wanyoike, W.; Bii, C. Isolation and Characterisation of Cryptococcus neoformans and Cryptococcus Gattii from Environmental Sources in Nairobi, Kenya. East Afr. Med. J. 2014, 91, 281–285. [Google Scholar]
- Chen, S.C.-A.; Meyer, W.; Sorrell, T.C. Cryptococcus gattii infections. Clin. Microbiol. Rev. 2014, 27, 980–1024. [Google Scholar] [CrossRef]
- Maziarz, E.K.; Perfect, J.R. Cryptococcosis. Infect. Dis. Clin. North Am. 2016, 30, 179–206. [Google Scholar] [CrossRef]
- Springer, D.J.; Chaturvedi, V. Projecting global occurrence of Cryptococcus gattii. Emerg. Infect. Dis. 2010, 16, 14–20. [Google Scholar] [CrossRef]
- Garcia-Hermoso, D.; Janbon, G.; Dromer, F. Epidemiological evidence for dormant Cryptococcus neoformans infection. J. Clin. Microbiol. 1999, 37, 3204–3209. [Google Scholar] [CrossRef]
- Esher, S.K.; Zaragoza, O.; Alspaugh, J.A. Cryptococcal pathogenic mechanisms: A dangerous trip from the environment to the brain. Mem. Inst. Oswaldo Cruz 2018, 113, e180057. [Google Scholar] [CrossRef] [PubMed]
- Kozubowski, L.; Lee, S.C.; Heitman, J. Signalling pathways in the pathogenesis of Cryptococcus. Cell. Microbiol. 2009, 11, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Bergman, A.; Casadevall, A. Mammalian endothermy optimally restricts fungi and metabolic costs. mBio 2010, 1, e00212-10. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, B.L.; Roberts, G.D. Rapid selective urease test for presumptive identification of Cryptococcus neoformans. J. Clin. Microbiol. 1979, 10, 380–381. [Google Scholar] [CrossRef]
- Vecchiarelli, A.; Pericolini, E.; Gabrielli, E.; Kenno, S.; Perito, S.; Cenci, E.; Monari, C. Elucidating the immunological function of the Cryptococcus neoformans capsule. Future Microbiol. 2013, 8, 1107–1116. [Google Scholar] [CrossRef]
- Kozel, T.R.; Gotschlich, E.C. The capsule of Cryptococcus neoformans passively inhibits phagocytosis of the yeast by macrophages. J. Immunol. 1982, 129, 1675–1680. [Google Scholar] [CrossRef]
- Rosas, A.L.; Casadevall, A. Melanization affects susceptibility of Cryptococcus neoformans to heat and cold. FEMS Microbiol. Lett. 1997, 153, 265–272. [Google Scholar] [CrossRef]
- Kwon-Chung, K.J.; Polacheck, I.; Popkin, T.J. Melanin-lacking mutants of Cryptococcus neoformans and their virulence for mice. J. Bacteriol. 1982, 150, 1414–1421. [Google Scholar] [CrossRef]
- Park, B.J.; Wannemuehler, K.A.; Marston, B.J.; Govender, N.; Pappas, P.G.; Chiller, T.M. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS 2009, 23, 525–530. [Google Scholar] [CrossRef]
- Duvall, C.P.; Carbone, P.P. Cryptococcus neoformans pericarditis associated with Hodgkin’s disease. Ann. Intern. Med. 1966, 64, 850–856. [Google Scholar] [CrossRef] [PubMed]
- López, J.; Revilla, A.; Vilacosta, I.; Villacorta, E.; González-Juanatey, C.; Gómez, I.; Rollán, M.J.; San Román, J.A. Definition, clinical profile, microbiological spectrum, and prognostic factors of early-onset prosthetic valve endocarditis. Eur. Heart J. 2007, 28, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.; Athan, E.; Pappas, P.A.; Fowler, V.G.; Olaison, L.; Paré, C.; Almirante, B.; Muñoz, P.; Rizzi, M.; Naber, C.; et al. Contemporary clinical profile and outcome of prosthetic valve endocarditis. JAMA 2007, 297, 1354–1361. [Google Scholar] [CrossRef]
- Challa, S.; Prayaga, A.K.; Vemu, L.; Sadasivan, J.; Jagarlapudi, M.K.M.; Digumarti, R.; Prabhala, R. Fungal endocarditis: An autopsy study. Asian Cardiovasc. Thorac. Ann. 2004, 12, 95–98. [Google Scholar] [CrossRef]
- Taramasso, L.; Tatarelli, P.; Di Biagio, A. Bloodstream infections in HIV-infected patients. Virulence 2016, 7, 320–328. [Google Scholar] [CrossRef]
- Varghese, G.M.; Sobel, J.D. Fungal endocarditis. Curr. Infect. Dis. Rep. 2008, 10, 275–279. [Google Scholar] [CrossRef]
- Qin, Y.; Zou, X.; Jin, Y.; Li, J.; Cai, Q. Cryptococcus neoformans Osteomyelitis of the Right Ankle Diagnosed by Metagenomic Next-Generation Sequencing in a HIV-Negative Patient with Tuberculous Lymphadenitis and Pulmonary Tuberculosis: A Case Report and Recent Literature Review. Infect. Drug Resist. 2024, 17, 3805–3812. [Google Scholar] [CrossRef]
- Tanner, D.C.; Weinstein, M.P.; Fedorciw, B.; Joho, K.L.; Thorpe, J.J.; Reller, L. Comparison of commercial kits for detection of cryptococcal antigen. J. Clin. Microbiol. 1994, 32, 1680–1684. [Google Scholar] [CrossRef] [PubMed]
- Pasqualotto, A.C.; Bittencourt Severo, C.; de Mattos Oliveira, F.; Severo, L.C. Cryptococcemia. An analysis of 28 cases with emphasis on the clinical outcome and its etiologic agent. Rev. Iberoam. Micol. 2004, 21, 143–146. [Google Scholar]
- Lancellotti, P.; Price, S.; Edvardsen, T.; Cosyns, B.; Neskovic, A.N.; Dulgheru, R.; Flachskampf, F.A.; Hassager, C.; Pasquet, A.; Gargani, L.; et al. The use of echocardiography in acute cardiovascular care: Recommendations of the European Association of Cardiovascular Imaging and the Acute Cardiovascular Care Association. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 119–146. [Google Scholar] [CrossRef]
- Perfect, J.R.; Dismukes, W.E.; Dromer, F.; Goldman, D.L.; Graybill, J.R.; Hamill, R.J.; Harrison, T.S.; Larsen, R.A.; Lortholary, O.; Nguyen, M.-H.; et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the infectious diseases society of america. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2010, 50, 291–322. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Harrison, T.S.; A Bicanic, T.; Chayakulkeeree, M.; Sorrell, T.C.; Warris, A.; Hagen, F.; Spec, A.; Oladele, R.; Govender, N.P.; et al. Global guideline for the diagnosis and management of cryptococcosis: An initiative of the ECMM and ISHAM in cooperation with the ASM. Lancet Infect. Dis. 2024, 24, e495–e512. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals from the American Heart Association. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef]
- Pasha, A.K.; Lee, J.Z.; Low, S.-W.; Desai, H.; Lee, K.S.; Al Mohajer, M. Fungal Endocarditis: Update on Diagnosis and Management. Am. J. Med. 2016, 129, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Legris, T.; Massad, M.; Purgus, R.; Vacher-Coponat, H.; Ranque, S.; Girard, N.; Berland, Y.; Moal, V. Immune reconstitution inflammatory syndrome mimicking relapsing cryptococcal meningitis in a renal transplant recipient. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2011, 13, 303–308. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | All Patients (n = 16) * | Survived (n = 7) * | Died (n = 9) * |
|---|---|---|---|
| Age, years, median (IQR) | 50 | 26 | 53.5 |
| Male gender, n (%) | 13 (81.25) | 7 (100) | 6 (66.67) |
| Predisposing factors | |||
| Immunosuppression, n (%) | 5 (31.25) | 2 (28.57) | 3 (33.3) |
| End-stage renal disease, n (%) | 4 (25) | 1 (14.28) | 3 (33.3) |
| Prosthetic cardiac valve, n (%) | 4 (25) | 1 (14.28) | 3 (33.3) |
| Malignancy, n (%) | 3 (18.75) | 1 (14.28) | 2 (22.2) |
| Rheumatic heart disease, n (%) | 3 (18.75) | 1 (14.28) | 2 (22.2) |
| Recent cardiac surgery, n (%) | 2 (12.5) | 1 (14.28) | 1 (11.1) |
| IVDU, n (%) | 2 (12.5) | 1 (14.28) | 1 (11.1) |
| Recent antibiotic administration, n(%) | 2 (12.5) | 2 (28.57) | 0 |
| Concomitant infection, n (%) | 7 (43.75) | 2 (28.57) | 5 (55.56) |
| Clinical characteristics | |||
| Fever, n (%) | 11/14 (78.57) | 4/5 (80) | 7 (77.78) |
| Sepsis, n (%) | 4/14 (28.57) | 0 | 4 (44.44) |
| Treatment | |||
| Amphotericin, n (%) | 14/16 (87.5) | 6 (85.71) | 8 (88.88) |
| Fluconazole, n (%) | 7/16 (43.75) | 3 (42.85) | 4 (44.44) |
| Micafungin, n (%) | 4/16 (25) | 2 (28.57) | 2 (22.2) |
| Flucytosine, n (%) | 4/16 (25) | 2 (28.57) | 2 (22.2) |
| Caspofungin, n (%) | 1/16 (6.25) | 1 (14.28) | 0 |
| Antifungal Combination | 10/16 (62.5) | 5 (71.42) | 5 (55.5) |
| Outcomes | |||
| Deaths due to infection, n (%) | 8/16 (50) | NA | NA |
| Deaths overall, n (%) | 9/16 (56.25) | NA | NA |
| Characteristic | All Patients (n = 16) * | Survived (n = 7) * | Died (n = 9) * |
|---|---|---|---|
| Fever, n (%) | 5/15 (33.3) | 4/5 (80) | 7 (77.77) |
| Embolic phenomena, n (%) | 9/15 (60) | 4 (57.14) | 5/8 (62.5) |
| Heart failure, n (%) | 7/13 (53.84) | 2 (28.57) | 5/6 (83.3) |
| Need for ICU, n (%) | 5/14 (35.71) | 1 (14.28) | 4/7 (57.14) |
| Sepsis, n (%) | 4/14 (28.57) | 0 | 4/7 (57.14) |
| Shock, n (%) | 2 (12.5) | 0 | 2 (22.2) |
| Paravalvular abscess, n (%) | 1 (6.25) | 0 | 1 (11.1) |
| Treatment | |||
| Amphotericin, n (%) | 14 (87.5) | 6 (85.71) | 8 (88.88) |
| Fluconazole, n (%) | 7 (43.75) | 3 (42.85) | 4 (44.4) |
| Flucytosine, n (%) | 4 (25) | 2 (28.57) | 2 (22.2) |
| Micafungin, n (%) | 4 (25) | 2 (28.57) | 2 (22.2) |
| Voriconazole, n (%) | 2 (12.5) | 2 (28.57) | 0 |
| Caspofungin, n (%) | 1 (6.25) | 1 (14.28) | 0 |
| Surgical Management, n (%) | 4 (25) | 3 (42.85) | 1 (11.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannou, P.; Ziogou, A.; Giannakodimos, A.; Giannakodimos, I.; Tsantes, A.G.; Samonis, G. Cryptococcal Endocarditis in Humans—A Narrative Review. Pathogens 2025, 14, 547. https://doi.org/10.3390/pathogens14060547
Ioannou P, Ziogou A, Giannakodimos A, Giannakodimos I, Tsantes AG, Samonis G. Cryptococcal Endocarditis in Humans—A Narrative Review. Pathogens. 2025; 14(6):547. https://doi.org/10.3390/pathogens14060547
Chicago/Turabian StyleIoannou, Petros, Afroditi Ziogou, Alexios Giannakodimos, Ilias Giannakodimos, Andreas G. Tsantes, and George Samonis. 2025. "Cryptococcal Endocarditis in Humans—A Narrative Review" Pathogens 14, no. 6: 547. https://doi.org/10.3390/pathogens14060547
APA StyleIoannou, P., Ziogou, A., Giannakodimos, A., Giannakodimos, I., Tsantes, A. G., & Samonis, G. (2025). Cryptococcal Endocarditis in Humans—A Narrative Review. Pathogens, 14(6), 547. https://doi.org/10.3390/pathogens14060547