
Active Surveillance of Antimicrobial Resistance and Carbapenemase-Encoding Genes According to Sites of Care and Age Groups in Mexico: Results from the INVIFAR Network
 ,
,  ,
,  , , , , , , , , , , , , , ,
, , , , , , , , , , , , , ,  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Participating Centers and Data Collection
2.2. Site of Care, Age, and Clinical Specimens
2.3. Carbapenemase-Encoding Genes
3. Results
3.1. Participating Centers and Study Population
3.2. Percentages of Resistance Detected in Critical- and High-Priority Pathogens/Phenotypes
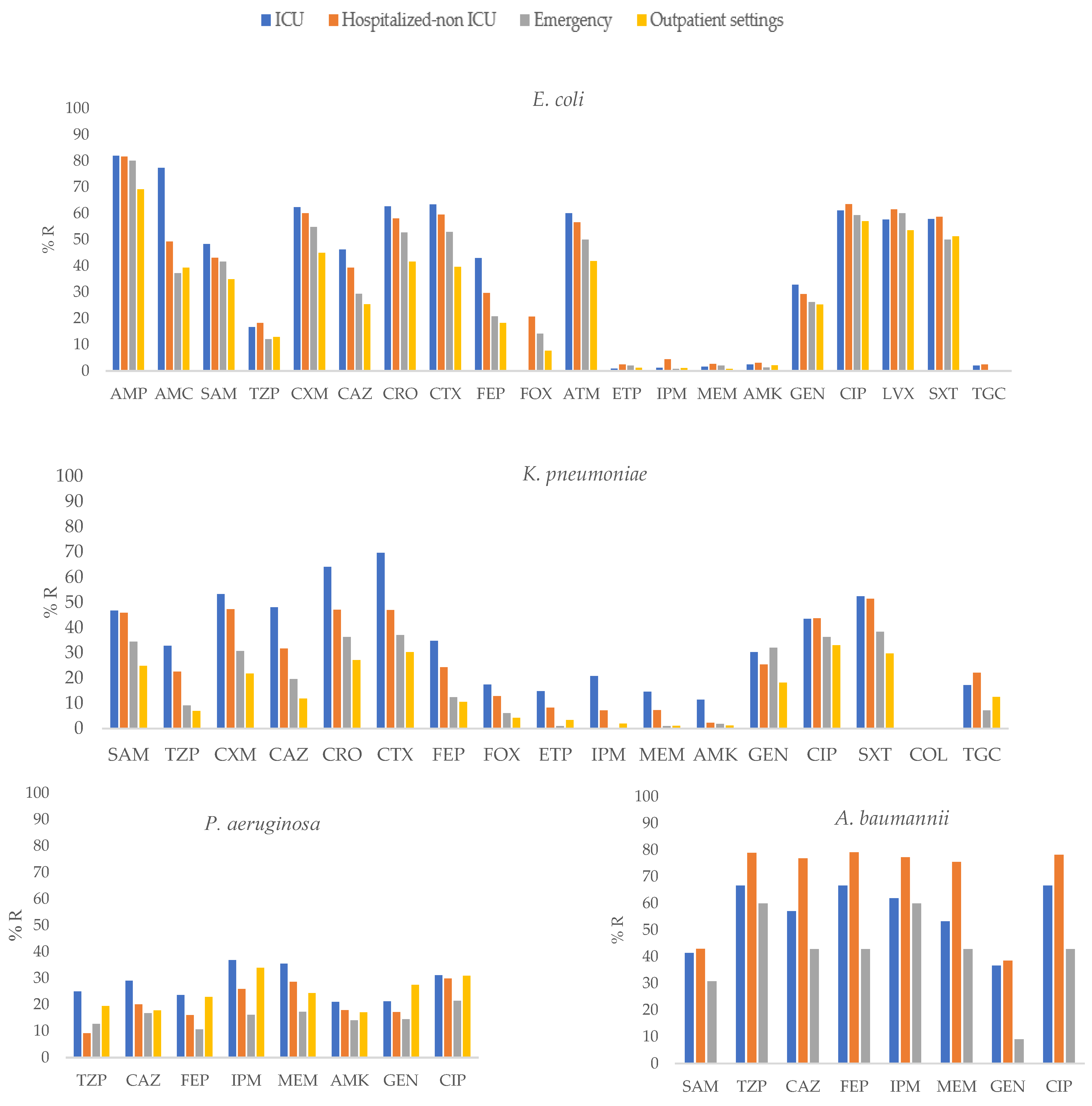
3.3. Antimicrobial Resistance of Selected Pathogens According to Site of Care
3.4. Antimicrobial Resistance of Selected Pathogens According to Patient Age Group
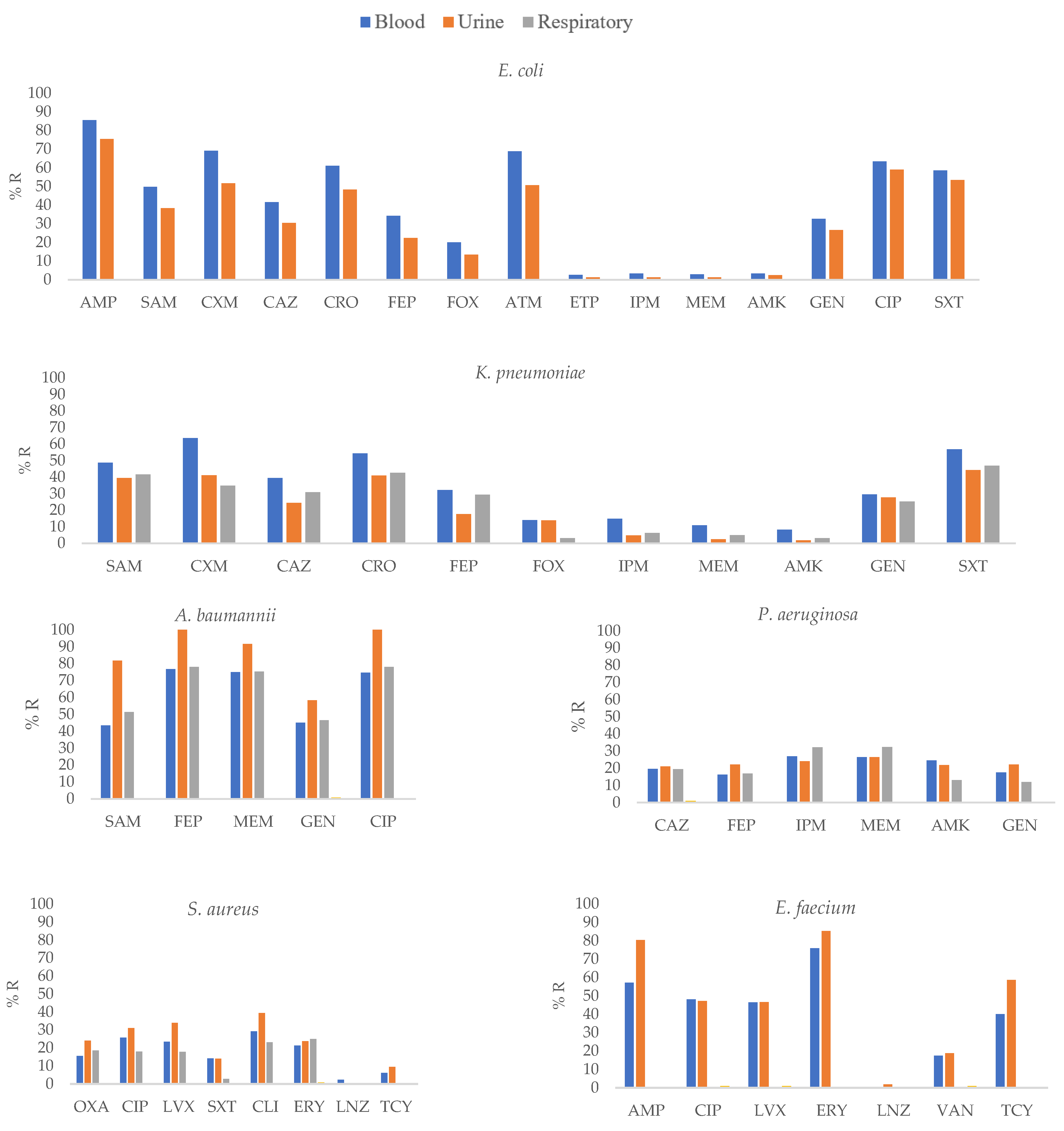
3.5. Antimicrobial Resistance of Selected Pathogens According to Clinical Specimen Type
3.6. MDR, XDR, and PDR Isolates
3.7. Carbapenemase-Encoding Genes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Gould, I. The epidemiology of antibiotic resistance. Int. J. Antimicrob. Agents 2008, 32 (Suppl. 1), S2–S9. [Google Scholar] [CrossRef]
- Arslan, H.; Azap, K.; Ergönül, O.; Timurkaynak, F.; Group UTIS. Risk factors for ciprofloxacin resistance among Escherichia coli strains isolated from community-acquired urinary tract infections in Turkey. J. Antimicrob. Chemother. 2005, 56, 914–918. [Google Scholar] [CrossRef] [PubMed]
- Colgan, R.; Johnson, J.R.; Kuskowski, M.; Gupta, K. Risk factors for trimethoprim-sulfamethoxazole resistance in patients with acute uncomplicated cystitis. Antimicrob. Agents Chemother. 2008, 52, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Barrios, H.; Garza-Ramos, U.; Reyna-Flores, F.; Sanchez-Perez, A.; Rojas-Moreno, T.; Garza-Gonzalez, E.; Llaca-Diaz, J.M.; Camacho-Ortiz, A.; Guzmán-López, S.; Silva-Sanchez, J. Isolation of carbapenem-resistant NDM-1-positive Providencia rettgeri in Mexico. J. Antimicrob. Chemother. 2013, 68, 1934–1936. [Google Scholar] [CrossRef]
- Barrios, H.; Silva-Sanchez, J.; Reyna-Flores, F.B.; Sanchez-Perez, A.Q.; Sanchez-Francia, D.Q.; Aguirre-Torres, J.A.T.; Sánchez-Rogel, J.T.; Garza-Ramos, U. Detection of a NDM-1-producing Klebsiella pneumoniae (ST22) clinical isolate at a pediatric hospital in Mexico. Pediatr. Infect. Dis. J. 2014, 33, 335. [Google Scholar] [CrossRef]
- Aquino-Andrade, A.; Merida-Vieyra, J.; de la Garza, E.A.; Arzate-Barbosa, P.; Ranero, A.D.C. Carbapenemase-producing Enterobacteriaceae in Mexico: Report of seven non-clonal cases in a pediatric hospital. BMC Microbiol. 2018, 18, 38. [Google Scholar] [CrossRef]
- Garza-Ramos, U.; Morfin-Otero, R.; Sader, H.S.; Jones, R.N.; Hernandez, E.; Rodriguez-Noriega, E.; Sanchez, A.; Carrillo, B.; Esparza-Ahumada, S.; Silva-Sanchez, J. Metallo-beta-lactamase gene bla(IMP-15) in a class 1 integron, In95, from Pseudomonas aeruginosa clinical isolates from a hospital in Mexico. Antimicrob. Agents Chemother. 2008, 52, 2943–2946. [Google Scholar] [CrossRef]
- Bocanegra-Ibarias, P.; Pena-López, C.; Camacho-Ortiz, A.; Llaca-Díaz, J.; Silva-Sánchez, J.; Barrios, H.; Garza-Ramos, U.; Rodríguez-Flores, A.M.; Garza-González, E. Genetic characterisation of drug resistance and clonal dynamics of Acinetobacter baumannii in a hospital setting in Mexico. Int. J. Antimicrob. Agents 2015, 45, 309–313. [Google Scholar] [CrossRef]
- Garza-González, E.; Bocanegra-Ibarias, P.; Bobadilla-del-Valle, M.; Ponce-de-León-Garduño, L.A.; Esteban-Kenel, V.; Silva-Sánchez, J.; Garza-Ramos, U.; Barrios-Camacho, H.; López-Jácome, L.E.; Colin-Castro, C.A.; et al. Drug resistance phenotypes and genotypes in Mexico in representative Gram-negative species: Results from the infivar network. PLoS ONE 2021, 16, e0248614. [Google Scholar] [CrossRef]
- Garza-González, E.; Morfín-Otero, R.; Mendoza-Olazarán, S.; Bocanegra-Ibarias, P.; Flores-Treviño, S.; Rodríguez-Noriega, E.; Ponce-De-León, A.; Sanchez-Francia, D.; Franco-Cendejas, R.; Arroyo-Escalante, S.; et al. A snapshot of antimicrobial resistance in Mexico. Results from 47 centers from 20 states during a six-month period. PLoS ONE 2019, 14, e0209865. [Google Scholar] [CrossRef] [PubMed]
- López-Jácome, L.E.; Fernández-Rodríguez, D.; Franco-Cendejas, R.; Camacho-Ortiz, A.; Morfin-Otero, M.D.R.; Rodríguez-Noriega, E.; Ponce-De-León, A.; Ortiz-Brizuela, E.; Rojas-Larios, F.; Velázquez-Acosta, M.D.C.; et al. Increment Antimicrobial Resistance During the COVID-19 Pandemic: Results from the Invifar Network. Microb. Drug Resist. 2021, 28, 338–345. [Google Scholar] [PubMed]
- CLSI. M100-S33; Performance Standards for Antimicrobial Susceptibility Testing. Twenty-Second Informational Supplement; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2022.
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Garza-Ramos, U.; Silva-Sánchez, J.; López-Jácome, L.E.; Hernández-Durán, M.; Colín-Castro, C.A.; Sánchez-Pérez, A.; Rodríguez-Santiago, J.; Morfín-Otero, R.; Rodriguez-Noriega, E.; Velázquez-Acosta, M.D.; et al. Carbapenemase-Encoding Genes and Colistin Resistance in Gram-Negative Bacteria During the COVID-19 Pandemic in Mexico: Results from the Invifar Network. Microb. Drug Resist. 2023, 29, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Bogaerts, P.; Rezende de Castro, R.; de Mendonça, R.; Huang, T.D.; Denis, O.; Glupczynski, Y. Validation of carbapenemase and extended-spectrum β-lactamase multiplex endpoint PCR assays according to ISO 15189. J. Antimicrob. Chemother. 2013, 68, 1576–1582. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.S.; Kim, K.; Huh, J.Y.; Jung, B.; Kang, M.S.; Hong, S.G. Multiplex PCR for rapid detection of genes encoding class A carbapenemases. Ann. Lab. Med. 2012, 32, 359–361. [Google Scholar] [CrossRef]
- Perez, F.; Hujer, A.M.; Hujer, K.M.; Decker, B.K.; Rather, P.N.; Bonomo, R.A. Global challenge of multidrug-resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2007, 51, 3471–3484. [Google Scholar] [CrossRef]
- Mulvey, M.R.; Grant, J.M.; Plewes, K.; Roscoe, D.; Boyd, D.A. New Delhi metallo-β-lactamase in Klebsiella pneumoniae and Escherichia coli, Canada. Emerg. Infect. Dis. 2011, 17, 103–106. [Google Scholar] [CrossRef]
- Spellberg, B.; Blaser, M.; Guidos, R.J.; Boucher, H.W.; Bradley, J.S.; Eisenstein, B.I.; Gerding, D.; Lynfield, R.; Reller, L.B.; Rex, J.; et al. Combating antimicrobial resistance: Policy recommendations to save lives. Clin. Infect. Dis. 2011, 52 (Suppl. 5), S397–S428. [Google Scholar]
- Dortet, L.; Poirel, L.; Nordmann, P. Worldwide dissemination of the NDM-type carbapenemases in gram-negative bacteria. BioMed Res. Int. 2014, 2014, 249856. [Google Scholar] [CrossRef]
- Patel, G.; Huprikar, S.; Factor, S.H.; Jenkins, S.G.; Calfee, D.P. Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect. Control. Hosp. Epidemiol. 2008, 29, 1099–1106. [Google Scholar] [CrossRef] [PubMed]
- De Waele, J.J.; Akova, M.; Antonelli, M.; Canton, R.; Carlet, J.; De Backer, D.; Dimopoulos, G.; Garnacho-Montero, J.; Kesecioglu, J.; Lipman, J.; et al. Antimicrobial resistance and antibiotic stewardship programs in the ICU: Insistence and persistence in the fight against resistance. A position statement from ESICM/ESCMID/WAAAR round table on multi-drug resistance. Intensive Care Med. 2018, 44, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Sommerstein, R.; Damonti, L.; Marschall, J.; Harbarth, S.; Gasser, M.; Kronenberg, A.; Buetti, N. Distribution of pathogens and antimicrobial resistance in ICU-bloodstream infections during hospitalization: A nationwide surveillance study. Sci. Rep. 2021, 11, 16876. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.F.; Lan, C.Y. Antimicrobial resistance in Acinetobacter baumannii: From bench to bedside. World J. Clin. Cases 2014, 2, 787–814. [Google Scholar] [CrossRef] [PubMed]
- Patwardhan, R.B.; Dhakephalkar, P.K.; Niphadkar, K.B.; Chopade, B.A. A study on nosocomial pathogens in ICU with special reference to multiresistant Acinetobacter baumannii harbouring multiple plasmids. Indian J. Med. Res. 2008, 128, 178–187. [Google Scholar]
- Uwingabiye, J.; Frikh, M.; Lemnouer, A.; Bssaibis, F.; Belefquih, B.; Maleb, A.; Dahraoui, S.; Belyamani, L.; Bait, A.; Haimeur, C.; et al. Acinetobacter infections prevalence and frequency of the antibiotics resistance: Comparative study of intensive care units versus other hospital units. Pan Afr. Med. J. 2016, 23, 191. [Google Scholar] [CrossRef]
- Kalanuria, A.; Zai, W.; Mirski, M. Ventilator-associated pneumonia in the ICU. Crit. Care 2014, 18, 208. [Google Scholar] [CrossRef]
- Timsit, J.-F.; Soubirou, J.-F.; Voiriot, G.; Chemam, S.; Neuville, M.; Mourvillier, B.; Sonneville, R.; Mariotte, E.; Bouadma, L.; Wolff, M. Treatment of bloodstream infections in ICUs. BMC Infect. Dis. 2014, 14, 489. [Google Scholar] [CrossRef]
- Liu, C.; Chang, Y.; Xu, Y.; Luo, Y.; Wu, L.; Mei, Z.; Li, S.; Wang, R.; Jia, X. Distribution of virulence-associated genes and antimicrobial susceptibility in clinical. Oncotarget 2018, 9, 21663–21673. [Google Scholar] [CrossRef]
- Morfin-Otero, R.; Tinoco-Favila, J.C.; Sader, H.S.; Salcido-Gutierrez, L.; Perez-Gomez, H.R.; Gonzalez-Diaz, E.; Petersen, L.; Rodriguez-Noriega, E. Resistance trends in gram-negative bacteria: Surveillance results from two Mexican hospitals, 2005–2010. BMC Res. Notes 2012, 5, 277. [Google Scholar] [CrossRef]
- Morfín-Otero, R.; Curiel, A.; Rocha, M.; Alpuche-Aranda, C.; Santos-Preciado, J.; Gayosso-Vázquez, C.; Araiza-Navarro, J.; Flores-Vaca, M.; Esparza-Ahumada, S.; González-Díaz, E.; et al. Acinetobacter baumannii infections in a tertiary care hospital in Mexico over the past 13 years. Chemotherapy 2013, 59, 57–65. [Google Scholar] [CrossRef]
- Alcántar-Curiel, M.D.; García-Torres, L.F.; González-Chávez, M.I.; Morfín-Otero, R.; Gayosso-Vázquez, C.; Jarillo-Quijada, M.D.; Fernández-Vázquez, J.L.; Giono-Cerezo, S.; Rodríguez-Noriega, E.; Santos-Preciado, J.I. Molecular mechanisms associated with nosocomial carbapenem-resistant Acinetobacter baumannii in Mexico. Arch. Med. Res. 2014, 45, 553–560. [Google Scholar] [CrossRef]
- Ponce-de-Leon, A.; Rodríguez-Noriega, E.; Morfín-Otero, R.; Cornejo-Juárez, D.P.; Tinoco, J.C.; Martínez-Gamboa, A.; Gaona-Tapia, C.J.; Guerrero-Almeida, M.L.; Martin-Onraët, A.; Vallejo Cervantes, J.L.; et al. Antimicrobial susceptibility of Gram-negative bacilli isolated from intra-abdominal and urinary-tract infections in Mexico from 2009 to 2015: Results from the Study for Monitoring Antimicrobial Resistance Trends (SMART). PLoS ONE 2018, 13, e0198621. [Google Scholar] [CrossRef] [PubMed]
- Diekema, D.; Pfaller, M.; Jones, R.; Doern, G.; Kugler, K.; Beach, M.; Sader, H. Trends in antimicrobial susceptibility of bacterial pathogens isolated from patients with bloodstream infections in the USA, Canada and Latin America. SENTRY Participants Group. Int. J. Antimicrob. Agents 2000, 13, 257–271. [Google Scholar] [CrossRef]
- Reinert, R.R.; Low, D.E.; Rossi, F.; Zhang, X.; Wattal, C.; Dowzicky, M.J. Antimicrobial susceptibility among organisms from the Asia/Pacific Rim, Europe and Latin and North America collected as part of TEST and the in vitro activity of tigecycline. J. Antimicrob. Chemother. 2007, 60, 1018–1029. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nelson, R.E.; Slayton, R.B.; Stevens, V.W.; Jones, M.M.; Khader, K.; Rubin, M.A.; Jernigan, J.A.; Samore, M.H. Attributable Mortality of Healthcare-Associated Infections Due to Multidrug-Resistant Gram-Negative Bacteria and Methicillin-Resistant Staphylococcus aureus. Infect. Control. Hosp. Epidemiol. 2017, 38, 848–856. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Ye, W.; Qi, Y.; Ying, Y.; Xia, Z. Overcoming Multidrug Resistance in Bacteria through Antibiotics Delivery in Surface-Engineered Nano-Cargos: Recent Developments for Future Nano-Antibiotics. Front. Bioeng. Biotechnol. 2021, 9, 696514. [Google Scholar] [CrossRef] [PubMed]
- Bocanegra-Ibarias, P.; Garza-González, E.; Morfín-Otero, R.; Barrios, H.; Villarreal-Treviño, L.; Rodríguez-Noriega, E.; Garza-Ramos, U.; Petersen-Morfin, S.; Silva-Sanchez, J. Molecular and microbiological report of a hospital outbreak of NDM-1-carrying Enterobacteriaceae in Mexico. PLoS ONE 2017, 12, e0179651. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Daikos, G.L.; Tiseo, G.; Bassoulis, D.; Giordano, C.; Galfo, V.; Leonildi, A.; Tagliaferri, E.; Barnini, S.; Sani, S.; et al. Efficacy of Ceftazidime-avibactam Plus Aztreonam in Patients With Bloodstream Infections Caused by Metallo-β-lactamase–Producing Enterobacterales. Clin. Infect. Dis. 2021, 72, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Kazmierczak, K.M.; Karlowsky, J.A.; de Jonge, B.L.M.; Stone, G.G.; Sahm, D.F. Epidemiology of Carbapenem Resistance Deter-minants Identified in Meropenem-Nonsusceptible. Antimicrob. Agents Chemother. 2021, 65, e0200020. [Google Scholar] [CrossRef] [PubMed]
- Mirzaei, B.; Bazgir, Z.N.; Goli, H.R.; Iranpour, F.; Mohammadi, F.; Babaei, R. Prevalence of multi-drug resistant (MDR) and extensively drug-resistant (XDR) phenotypes of Pseudomonas aeruginosa and Acinetobacter baumannii isolated in clinical samples from Northeast of Iran. BMC Res. Notes 2020, 13, 380. [Google Scholar] [CrossRef] [PubMed]
- Aliyu, S.; Smaldone, A.; Larson, E. Prevalence of multidrug-resistant gram-negative bacteria among nursing home residents: A systematic review and meta-analysis. Am. J. Infect. Control 2017, 45, 512–518. [Google Scholar] [CrossRef]
- Rodríguez-Villodres, Á.; Martín-Gandul, C.; Peñalva, G.; Guisado-Gil, A.B.; Crespo-Rivas, J.C.; Pachón-Ibáñez, M.E.; Lepe, J.A.; Cisneros, J.M. Prevalence and Risk Factors for Multidrug-Resistant Organisms Colonization in Long-Term Care Facilities around the World: A Review. Antibiotics 2021, 10, 680. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; McNeil, E.B.; Huang, Z.; Chen, L.; Lu, X.; Wang, C.; Chen, H.; Chongsuvivatwong, V. Household financial burden among multidrug-resistant tuberculosis patients in Guizhou province, China: A cross-sectional study. Medicine 2020, 99, e21023. [Google Scholar] [CrossRef] [PubMed]
- Punpanich, W.; Nithitamsakun, N.; Treeratweeraphong, V.; Suntarattiwong, P. Risk factors for carbapenem non-susceptibility and mortality in Acinetobacter baumannii bacteremia in children. Int. J. Infect. Dis. 2012, 16, e811–e815. [Google Scholar] [CrossRef] [PubMed]
- Özgür, E.S.; Horasan, E.S.; Karaca, K.; Ersöz, G.; Atış, S.N.; Kaya, A. Ventilator-associated pneumonia due to extensive drug-resistant Acinetobacter baumannii: Risk factors, clinical features, and outcomes. Am. J. Infect. Control. 2014, 42, 206–208. [Google Scholar] [CrossRef]
- Townsend, J.; Na Park, A.; Gander, R.; Orr, K.; Arocha, D.; Zhang, S.; Greenberg, D.E. Acinetobacter infections and outcomes at an academic medical center: A disease of long-term care. Open Forum Infect. Dis. 2015, 2, ofv023. [Google Scholar] [CrossRef]
- Liu, Q.; Li, W.; Du, X.; Li, W.; Zhong, T.; Tang, Y.; Feng, Y.; Tao, C.; Xie, Y. Risk and Prognostic Factors for Multidrug-Resistant Acinetobacter baumannii Complex Bacteremia: A Retrospective Study in a Tertiary Hospital of West China. PLoS ONE 2015, 10, e0130701. [Google Scholar] [CrossRef]
- Rice, L.B. Progress and challenges in implementing the research on ESKAPE pathogens. Infect. Control Hosp. Epidemiol. 2010, 31 (Suppl. 1), S7–S10. [Google Scholar] [CrossRef]
- O’Brien, T.F.; Clark, A.; Peters, R.; Stelling, J. Why surveillance of antimicrobial resistance needs to be automated and comprehensive. J. Glob. Antimicrob. Resist. 2019, 17, 8–15. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | State | Type | Level | Center Type | Total Beds | ICU Beds |
|---|---|---|---|---|---|---|
| 1 | Jalisco | Pu | Ter | Spe | 760 | 45 |
| 2 | Mexico City | Pu | Ter | Spe | 245 | 15 |
| 3 | Mexico State | Pu | Ter | Spe | 238 | 28 |
| 4 | Mexico City | Pu | Ter | Spe | 234 | 22 |
| 5 | Aguascalientes | Pu | Ter | Spe | 218 | 23 |
| 6 | Mexico State | Pu | Ter | Spe | 210 | 8 |
| 7 | Mexico City | Pu | Ter | Spe | 193 | 15 |
| 8 | Mexico City | Pu | Ter | Spe | 146 | 8 |
| 9 | Chiapas | Pu | Ter | Spe | 90 | 15 |
| 10 | Nuevo León | Pr | Ter | Spe | 83 | 8 |
| 11 | Sonora | Pu | Ter | Spe | 60 | 6 |
| 12 | Michoacán | Pr | Ter | Spe | 55 | 11 |
| 13 | Quintana Roo | Pr | Ter | Spe | 54 | 4 |
| 14 | Mexico State | Pu | Ter | Ped | 180 | 8 |
| 15 | Puebla | Pu | Ter | Ped | 130 | 10 |
| 16 | Coahuila | Pu | Sec | Ped | 74 | 5 |
| 17 | Sonora | Pu | Sec | Gen | 290 | 12 |
| 18 | Michoacán | Pu | Sec | Gen | 250 | 24 |
| 19 | Guanajuato | Pu | Sec | Gen | 221 | 20 |
| 20 | Sonora | Pu | Sec | Gen | 171 | 4 |
| 21 | Oaxaca | Pu | Sec | Gen | 162 | 12 |
| 22 | Mexico City | Pu | Sec | Gen | 145 | 10 |
| 23 | Chiapas | Pu | Sec | Gen | 140 | 18 |
| 24 | Sonora | Pu | Sec | Gen | 122 | 4 |
| 25 | Chiapas | Pu | Sec | Gen | 120 | 25 |
| 26 | Baja California Sur | Pu | Sec | Gen | 120 | 17 |
| 27 | Colima | Pu | Sec | Gen | 105 | 4 |
| 28 | Michoacán | Pu | Sec | Ped | 100 | 7 |
| 29 | Chihuahua | Pu | Sec | Gen | 100 | 6 |
| 30 | Jalisco | Pu | Sec | Gen | 87 | 5 |
| 31 | Sonora | Pu | Sec | Spe | 35 | 4 |
| 32 | Michoacán | Pr | Pri | Gen | 32 | 3 |
| 33 | Guerrero | Pu | Sec | Moth and Child | 27 | 12 |
| 34 | Quintana Roo | Pu | Sec | Moth and Child | 20 | 20 |
| 35 | Mexico State | Pr | Pri | ACL | 0 | 0 |
| 36 | Michoacán | Pr | Pri | ACL | 0 | 0 |
| 37 | Guerrero | Pr | Pri | ACL | 0 | 0 |
| 38 | Michoacán | Pr | Pri | ACL | 0 | 0 |
| 39 | Michoacán | Pr | Pri | ACL | 0 | 0 |
| 40 | Oaxaca | Pr | Pri | ACL | 0 | 0 |
| 41 | Nuevo León | Pu | Pri | ACL | 0 | 0 |
| 42 | Michoacán | Pr | Sec | ACL | 0 | 0 |
| 43 | Sonora | Pu | Pri | ACL | 0 | 0 |
| ICU | MDR n (%) | Possible XDR n (%) | True XDR n (%) | Possible PDR n (%) | Total |
|---|---|---|---|---|---|
| E. coli | 83 (62.9) | 14 (10.6) | 0 (0) | 0 (0.0) | 132 |
| K. pneumoniae | 47 (50.5) | 35 (37.6) | 0 (0) | 2 (2.2) | 93 |
| A. baumannii | 20 (66.7) | 18 (60.0) | 0 (0) | 6 (20.0) | 30 |
| P. aeruginosa | 35 (29.7) | 32 (27.1) | 2 (1.7) | 15 (12.7) | 118 |
| Hospitalized non-ICU | |||||
| E. coli | 775 (53.4) | 199 (13.7) | 0 (0) | 0 (0.0) | 1450 |
| K. pneumoniae | 152 (44.6) | 106 (31.1) | 0 (0) | 2 (0.6) | 341 |
| A. baumannii | 87 (79.1) | 86 (78.2) | 0 (0) | 41 (37.3) | 110 |
| P. aeruginosa | 87 (21.5) | 79 (19.5) | 5 (1.2) | 46 (11.4) | 405 |
| Emergency | |||||
| E. coli | 280 (48.6) | 72 (12.5) | 0 (0) | 1 (0.2) | 576 |
| K. pneumoniae | 40 (34.5) | 25 (21.6) | 0 (0) | 0 (0.0) | 116 |
| A. baumannii | 6 (42.9) | 6 (42.9) | 0 (0) | 2 (14.3) | 14 |
| P. aeruginosa | 19 (17.4) | 14 (12.8) | 1 (0.9) | 4 (3.7) | 109 |
| Outpatients | |||||
| E. coli | 744 (45.8) | 228 (14.0 | 0 (0) | 0 (0.0) | 1625 |
| K. pneumoniae | 55 (28.1) | 36 (18.4) | 0 (0) | 0 (0.0) | 196 |
| P. aeruginosa | 30 (25.4) | 2 (22.9) | 1 (0.8) | 7 (5.9) | 118 |
| N | Species | blaNDM | blaKPC | blaVIM | blaIMP | blaOXA48 | blaGES | blaOXA23 | blaOXA24 |
|---|---|---|---|---|---|---|---|---|---|
| 22 | K. pneumoniae | + | − | − | − | − | ND | ND | ND |
| 12 | K. pneumoniae | − | + | − | − | − | ND | ND | ND |
| 2 | K. pneumoniae | − | − | − | − | + | ND | ND | ND |
| 8 | K. pneumoniae | − | − | − | − | − | ND | ND | ND |
| 57 | E. coli | + | − | − | − | − | ND | ND | ND |
| 6 | E. coli | − | − | − | − | + | ND | ND | ND |
| 3 | E. coli | + | − | + | − | − | ND | ND | ND |
| 3 | E. coli | + | − | − | − | + | ND | ND | ND |
| 1 | E. coli | − | + | − | − | − | ND | ND | ND |
| 1 | E. coli | − | − | + | − | − | ND | ND | ND |
| 4 | E. coli | − | − | − | − | − | ND | ND | ND |
| 47 | P. aeruginosa | ND | ND | − | − | ND | + | ND | ND |
| 32 | P. aeruginosa | ND | ND | − | + | ND | − | ND | ND |
| 11 | P. aeruginosa | ND | ND | − | + | ND | + | ND | ND |
| 11 | P. aeruginosa | ND | ND | + | − | ND | − | ND | ND |
| 1 | P. aeruginosa | ND | ND | + | − | ND | + | ND | ND |
| 1 | P. aeruginosa | ND | ND | + | + | ND | − | ND | ND |
| 100 | P. aeruginosa | ND | ND | − | − | ND | − | ND | ND |
| 47 | A. baumannii | − | ND | ND | ND | ND | ND | − | + |
| 32 | A. baumannii | − | ND | ND | ND | ND | ND | + | − |
| 5 | A. baumannii | − | ND | ND | ND | ND | ND | + | + |
| 1 | A. baumannii | + | ND | ND | ND | ND | ND | + | − |
| 10 | A. baumannii | − | ND | ND | ND | ND | ND | − | − |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojas-Larios, F.; Martínez-Guerra, B.A.; López-Jácome, L.E.; Bolado-Martínez, E.; Vázquez-Larios, M.d.R.; Velázquez-Acosta, M.d.C.; Romero-Romero, D.; Mireles-Dávalos, C.D.; Quintana-Ponce, S.; Feliciano-Guzmán, J.M.; et al. Active Surveillance of Antimicrobial Resistance and Carbapenemase-Encoding Genes According to Sites of Care and Age Groups in Mexico: Results from the INVIFAR Network. Pathogens 2023, 12, 1144. https://doi.org/10.3390/pathogens12091144
Rojas-Larios F, Martínez-Guerra BA, López-Jácome LE, Bolado-Martínez E, Vázquez-Larios MdR, Velázquez-Acosta MdC, Romero-Romero D, Mireles-Dávalos CD, Quintana-Ponce S, Feliciano-Guzmán JM, et al. Active Surveillance of Antimicrobial Resistance and Carbapenemase-Encoding Genes According to Sites of Care and Age Groups in Mexico: Results from the INVIFAR Network. Pathogens. 2023; 12(9):1144. https://doi.org/10.3390/pathogens12091144
Chicago/Turabian StyleRojas-Larios, Fabian, Bernardo Alfonso Martínez-Guerra, Luis Esaú López-Jácome, Enrique Bolado-Martínez, María del Rosario Vázquez-Larios, María del Consuelo Velázquez-Acosta, Daniel Romero-Romero, Christian Daniel Mireles-Dávalos, Sandra Quintana-Ponce, José Manuel Feliciano-Guzmán, and et al. 2023. "Active Surveillance of Antimicrobial Resistance and Carbapenemase-Encoding Genes According to Sites of Care and Age Groups in Mexico: Results from the INVIFAR Network" Pathogens 12, no. 9: 1144. https://doi.org/10.3390/pathogens12091144
APA StyleRojas-Larios, F., Martínez-Guerra, B. A., López-Jácome, L. E., Bolado-Martínez, E., Vázquez-Larios, M. d. R., Velázquez-Acosta, M. d. C., Romero-Romero, D., Mireles-Dávalos, C. D., Quintana-Ponce, S., Feliciano-Guzmán, J. M., Pérez-Hernandez, J. M., Correa-León, Y. P., López-Gutiérrez, E., Rodriguez-Noriega, E., González-Díaz, E., Choy-Chang, E. V., Mena-Ramírez, J. P., Monroy-Colín, V. A., Ponce-de-León-Garduño, A., ... Garza-González, E. (2023). Active Surveillance of Antimicrobial Resistance and Carbapenemase-Encoding Genes According to Sites of Care and Age Groups in Mexico: Results from the INVIFAR Network. Pathogens, 12(9), 1144. https://doi.org/10.3390/pathogens12091144