
Clinical Outcomes of Third-Generation Cephalosporin Definitive Therapy for Bloodstream Infections Due to Enterobacterales with Potential AmpC Induction: A Single-Center Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Population
2.2. Definitions
2.3. Outcomes
2.4. Data Management
2.5. Statistical Analysis
3. Results
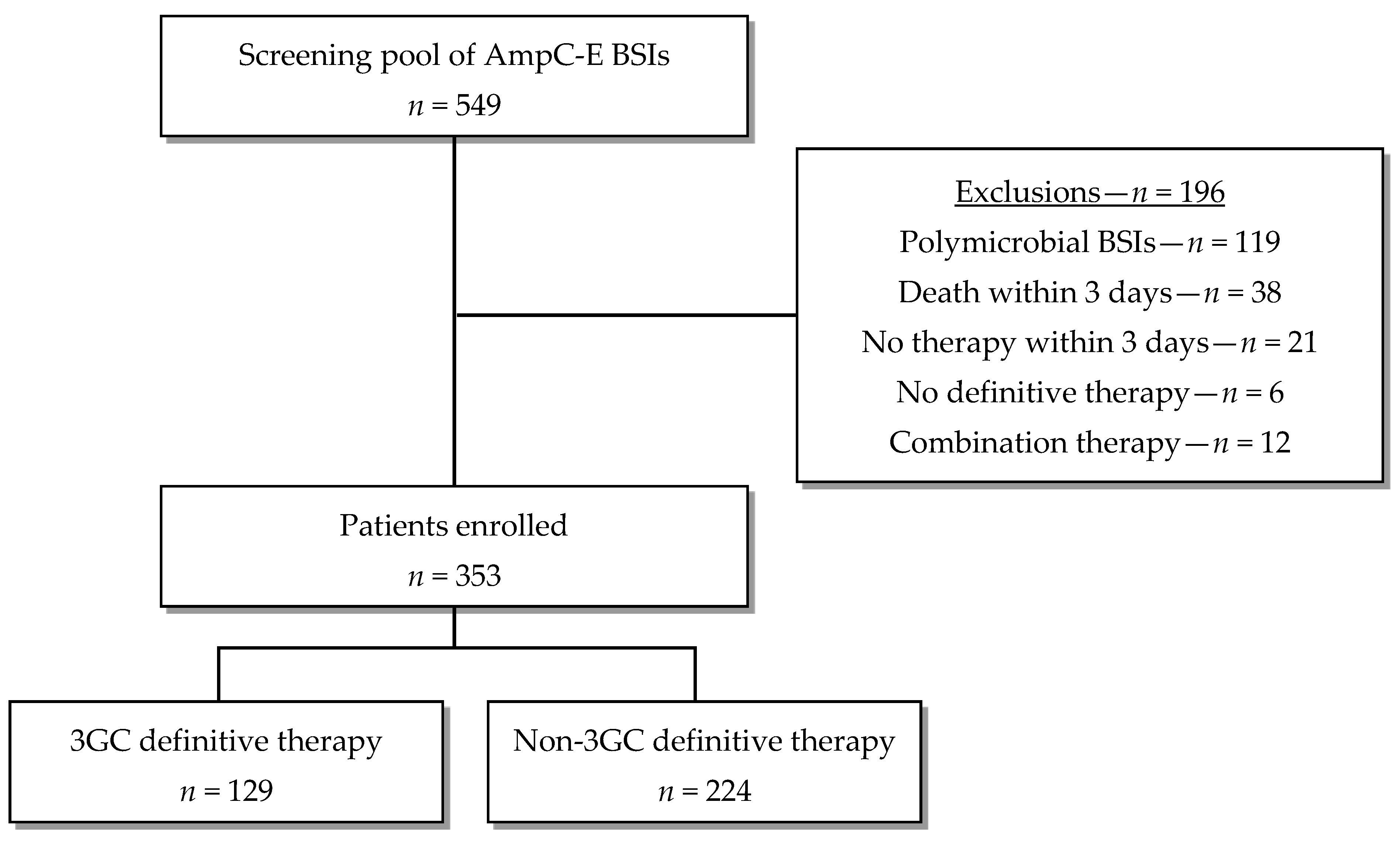
3.1. Participants
3.2. Antibiotic Therapy
3.3. Outcomes for Principal Analysis—3GCs vs. Non-3GCs for All Amp-C E
3.4. Outcomes for First Subgroup Analysis—3GCs vs. Cefepime/Carbapenems for All AmpC-E
3.5. Outcomes for Second Subgroup Analysis—3GCs vs. Non-3GCs for High-Risk AmpC-E
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morris, S.; Cerceo, E. Trends, Epidemiology, and Management of Multi-Drug Resistant Gram-Negative Bacterial Infections in the Hospitalized Setting. Antibiotics 2020, 9, 196. [Google Scholar] [CrossRef]
- Bush, K. Past and Present Perspectives on β-Lactamases. Antimicrob. Agents Chemother. 2018, 62, e01076-18. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for Drug-Resistant Bacterial Infections, Including Tuberculosis; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Center for Disease Control and Prevention. Antibiotic Resistance Threats in the United States; CDC: Atlanta, GA, USA, 2019. [Google Scholar]
- Jacoby, G.A. AmpC β-Lactamases. Clin. Microbiol. Rev. 2009, 22, 161–182. [Google Scholar] [CrossRef]
- Kohlmann, R.; Bähr, T.; Gatermann, S.G. Species-specific mutation rates for ampC derepression in Enterobacterales with chromosomally encoded inducible AmpC β-lactamase. J. Antimicrob. Chemother. 2018, 73, 1530–1536. [Google Scholar] [CrossRef] [PubMed]
- Sageerabanoo, S.; Malini, A.; Mangaiyarkarasi, T.; Hemalatha, G. Phenotypic detection of extended spectrum β-lactamase and Amp-C β-lactamase producing clinical isolates in a Tertiary Care Hospital: A preliminary study. J. Nat. Sci. Biol. Med. 2015, 6, 383–387. [Google Scholar] [CrossRef]
- Polsfuss, S.; Bloemberg, G.V.; Giger, J.; Meyer, V.; Böttger, E.C.; Hombach, M. Practical Approach for Reliable Detection of AmpC Beta-Lactamase-Producing Enterobacteriaceae▿. J. Clin. Microbiol. 2011, 49, 2798–2803. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America 2023 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2023, ciad428. [Google Scholar] [CrossRef]
- Kaye, K.S.; Cosgrove, S.; Harris, A.; Eliopoulos, G.M.; Carmeli, Y. Risk factors for emergence of resistance to broad-spectrum cephalosporins among Enterobacter spp. Antimicrob. Agents Chemother. 2001, 45, 2628–2630. [Google Scholar] [CrossRef]
- Chow, J.W.; Fine, M.J.; Shlaes, D.M.; Quinn, J.P.; Hooper, D.C.; Johnson, M.P.; Ramphal, R.; Wagener, M.M.; Miyashiro, D.K.; Yu, V.L. Enterobacter bacteremia: Clinical features and emergence of antibiotic resistance during therapy. Ann. Intern. Med. 1991, 115, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Schwaber, M.J.; Graham, C.S.; Sands, B.E.; Gold, H.S.; Carmeli, Y. Treatment with a broad-spectrum cephalosporin versus piperacillin-tazobactam and the risk for isolation of broad-spectrum cephalosporin-resistant Enterobacter species. Antimicrob. Agents Chemother. 2003, 47, 1882–1886. [Google Scholar] [CrossRef]
- Kang, C.-I.; Kim, S.-H.; Park, W.B.; Lee, K.-D.; Kim, H.-B.; Oh, M.; Kim, E.-C.; Choe, K.-W. Bloodstream infections caused by Enterobacter species: Predictors of 30-day mortality rate and impact of broad-spectrum cephalosporin resistance on outcome. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2004, 39, 812–818. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.-H.; Lee, J.E.; Park, S.J.; Choi, S.-H.; Lee, S.-O.; Jeong, J.-Y.; Kim, M.-N.; Woo, J.H.; Kim, Y.S. Emergence of antibiotic resistance during therapy for infections caused by Enterobacteriaceae producing AmpC beta-lactamase: Implications for antibiotic use. Antimicrob. Agents Chemother. 2008, 52, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.N.A.; Peri, A.M.; Pelecanos, A.M.; Hughes, C.M.; Paterson, D.L.; Ferguson, J.K. Risk factors for relapse or persistence of bacteraemia caused by Enterobacter spp.: A case–control study. Antimicrob. Resist. Infect. Control 2017, 6, 14. [Google Scholar] [CrossRef] [PubMed]
- Derrick, C.; Bookstaver, P.B.; Lu, Z.K.; Bland, C.M.; King, S.T.; Stover, K.R.; Rumley, K.; MacVane, S.H.; Swindler, J.; Kincaid, S.; et al. Multicenter, Observational Cohort Study Evaluating Third-Generation Cephalosporin Therapy for Bloodstream Infections Secondary to Enterobacter, Serratia, and Citrobacter Species. Antibiot. Basel 2020, 9, 254. [Google Scholar] [CrossRef]
- Drozdinsky, G.; Neuberger, A.; Rakedzon, S.; Nelgas, O.; Cohen, Y.; Rudich, N.; Mushinsky, L.; Ben-Zvi, H.; Paul, M.; Yahav, D. Treatment of Bacteremia Caused by Enterobacter spp.: Should the Potential for AmpC Induction Dictate Therapy? A Retrospective Study. Microb. Drug Resist. 2021, 27, 410–414. [Google Scholar] [CrossRef]
- Mounier, R.; Le Guen, R.; Woerther, P.-L.; Nacher, M.; Bonnefon, C.; Mongardon, N.; Langeron, O.; Levesque, E.; Couffin, S.; Houcke, S.; et al. Clinical outcome of wild-type AmpC-producing Enterobacterales infection in critically ill patients treated with β-lactams: A prospective multicenter study. Ann. Intensive Care 2022, 12, 107. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Jacobson, K.L.; Cohen, S.H.; Inciardi, J.F.; King, J.H.; Lippert, W.E.; Iglesias, T.; VanCouwenberghe, C.J. The relationship between antecedent antibiotic use and resistance to extended-spectrum cephalosporins in group I beta-lactamase-producing organisms. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1995, 21, 1107–1113. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 30th ed.; CLSI document M100; Clinical and Laboratory Standards Institute, 2020; Available online: https://teams.microsoft.com/l/message/19:485487f0-48a5-4c0d-903e-a677d3a230af_7e058200-ea59-495e-9074-e4de8ecc2872@unq.gbl.spaces/1694401183146?context=%7B%22contextType%22%3A%22chat%22%7D (accessed on 7 September 2023).
- The European Committee on Antimicrobial Susceptibility Testing. Expert Rules on Enterobacterales, v 3.2. 2023. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Expert_Rules/2023/ExpertRules_V3.2_20230123_Enterobacterales.pdf (accessed on 7 September 2023).
- Bush, K.; Bradford, P.A. Interplay between β-lactamases and new β-lactamase inhibitors. Nat. Rev. Microbiol. 2019, 17, 295–306. [Google Scholar] [CrossRef]
- Cheng, M.P.; Lee, R.S.; Cheng, A.P.; De L’étoile-Morel, S.; Demir, K.; Yansouni, C.P.; Harris, P.; Mcdonald, E.G.; Lee, T.C. Beta-Lactam/Beta-Lactamase Inhibitor Therapy for Potential AmpC-Producing Organisms: A Systematic Review and Meta-Analysis. Open Forum Infect. Dis. 2019, 6, ofz248. [Google Scholar] [CrossRef]
- Stewart, A.G.; Paterson, D.L.; Young, B.; Lye, D.C.; Davis, J.S.; Schneider, K.; Yilmaz, M.; Dinleyici, R.; Runnegar, N.; Henderson, A.; et al. Meropenem Versus Piperacillin-Tazobactam for Definitive Treatment of Bloodstream Infections Caused by AmpC β-Lactamase-Producing Enterobacter spp, Citrobacter freundii, Morganella morganii, Providencia spp, or Serratia marcescens: A Pilot Multicenter Randomized Controlled Trial (MERINO-2). Open Forum Infect. Dis. 2021, 8, ofab387. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.; Zahar, J.-R.; Lesprit, P.; Ruppe, E.; Leone, M.; Chastre, J.; Lucet, J.-C.; Paugam-Burtz, C.; Brun-Buisson, C.; Timsit, J.-F.; et al. Elaboration of a consensual definition of de-escalation allowing a ranking of β-lactams. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2015, 21, 649.e1–649.e10. [Google Scholar] [CrossRef] [PubMed]
- Payne, L.E.; Gagnon, D.J.; Riker, R.R.; Seder, D.B.; Glisic, E.K.; Morris, J.G.; Fraser, G.L. Cefepime-induced neurotoxicity: A systematic review. Crit. Care Lond. Engl. 2017, 21, 276. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.P.R. Sparing carbapenem usage. J. Antimicrob. Chemother. 2017, 72, 2410–2417. [Google Scholar] [CrossRef] [PubMed]
- Management Sciences for Health (MSH). International Medical Products Price Guide; MSH: Medford, MA, USA, 2015. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | 3GC Definitive Therapy n = 129 | Non-3GC Definitive Therapy n = 224 | p-Value |
|---|---|---|---|
| General characteristics | |||
| Sex, male 1 | 86 (66.7) | 164 (73.2) | 0.19 |
| Age (years) 2 | 66.2 ± 14.4 | 64.3 ± 14.6 | 0.23 |
| Weight (kg) 2 | 78.6 ± 18.4 | 76.8 ± 18.7 | 0.42 |
| Height (m) 2 | 169.6 ± 10.0 | 171.1 ± 8.7 | 0.23 |
| BMI (kg/m2) 2 | 27.0 ± 6.7 | 26.0 ± 6.0 | 0.24 |
| Renal function (mL/min) 3 | 65.1 (34.9;113.0) | 74.6 (50.9;106.6) | 0.14 |
| Penicillin allergy 1 | 12 (9.3) | 20 (8.9) | 0.91 |
| Charlson comorbidity index 2 | 4.2 ± 2.9 | 4.1 ± 3.0 | 0.70 |
| Antimicrobial therapy 1 | |||
| Adequate empiric therapy | 120 (93.0) | 209 (93.3) | 0.92 |
| Adequate definitive therapy | 128 (99.2) | 222 (99.1) | 1.00 4 |
| Aminoglycoside use | 25 (19.4) | 29 (12.9) | 0.11 |
| Severity of illness | |||
| ICU admission 1 | 54 (41.9) | 57 (25.4) | 0.0014 |
| qPitt score 3 | 1.50 (1.00;2.00) | 1.00 (0.00;2.00) | 0.0017 |
| qSOFA score 3 | 1.00 (0.00;2.00) | 1.00 (0.00;2.00) | 0.0017 |
| Sedated and intubated 1 | 19 (14.7) | 22 (9.8) | 0.17 |
| Source 1 | 0.014 | ||
| Respiratory | 36 (27.9) | 46 (20.5) | |
| Urinary tract | 17 (13.2) | 51 (22.8) | |
| Catheter-related | 28 (21.7) | 38 (17.0) | |
| Intra-abdominal | 15 (11.6) | 42 (18.8) | |
| Soft tissue | 11 (8.5) | 10 (4.5) | |
| Other | 8 (6.2) | 5 (2.2) | |
| Unknown | 14 (10.9) | 32 (14.3) | |
| Pathogen 1 | 0.21 4 | ||
| E. cloacae complex | 44 (34.1) | 103 (46.0) | |
| S. marcescens | 44 (34.1) | 55 (24.6) | |
| M. morganii | 19 (14.7) | 25 (11.2) | |
| K. aerogenes | 10 (7.7) | 23 (10.3) | |
| C. freundii | 11 (8.5) | 15 (6.7) | |
| P. stuartii | 1 (0.8) | 2 (0.9) | |
| H. alvei | 0 (0.0) | 1 (0.5) |
| Empiric Therapy | Definitive Therapy | |||
|---|---|---|---|---|
| Antibiotic | 3GC Definitive Therapy 1 n = 129 | Non-3GC Definitive Therapy 1 n = 224 | 3GC Definitive Therapy 1 n = 129 | Non-3GC Definitive Therapy 1 n = 224 |
| Penicillins | ||||
| Amoxicillin | 0 (0.0) | 1 (0.4) | / | 0 (0.0) |
| Amoxicillin + clavulanate | 4 (3.1) | 5 (2.2) | / | 1 (0.5) |
| Flucloxacillin | 1 (0.8) | 1 (0.4) | / | 0 (0.0) |
| Temocillin | 0 (0.0) | 2 (0.9) | / | 4 (1.8) |
| Piperacillin + tazobactam | 32 (24.8) | 103 (46.0) | / | 56 (25.0) |
| 2GC | / | |||
| Cefuroxime | 1 (0.8) | 4 (1.8) | / | 3 (1.3) |
| 3GC | ||||
| Cefotaxime | 33 (25.6) | 5 (2.2) | 57 (44.2) | / |
| Ceftriaxone | 22 (17.1) | 18 (8.0) | 44 (34.1) | / |
| Ceftazidime | 21 (16.3) | 6 (2.7) | 28 (21.7) | / |
| 4GC | ||||
| Cefepime | 6 (4.7) | 16 (7.1) | / | 18 (8.0) |
| Carbapenems | / | |||
| Meropenem | 7 (5.4) | 24 (10.7) | / | 19 (8.5) |
| Fluoroquinolones | ||||
| Ciprofloxacin | 0 (0.0) | 25 (11.2) | / | 84 (37.5) |
| Moxifloxacin | 0 (0.0) | 4 (1.8) | / | 3 (1.3) |
| Others | ||||
| Minocycline | 0 (0.0) | 1 (0.4) | / | 1 (0.5) |
| Tigecycline | 1 (0.8) | 1 (0.4) | / | 0 (0.0) |
| TMP-SMX | 1 (0.8) | 8 (3.6) | / | 35 (15.6) |
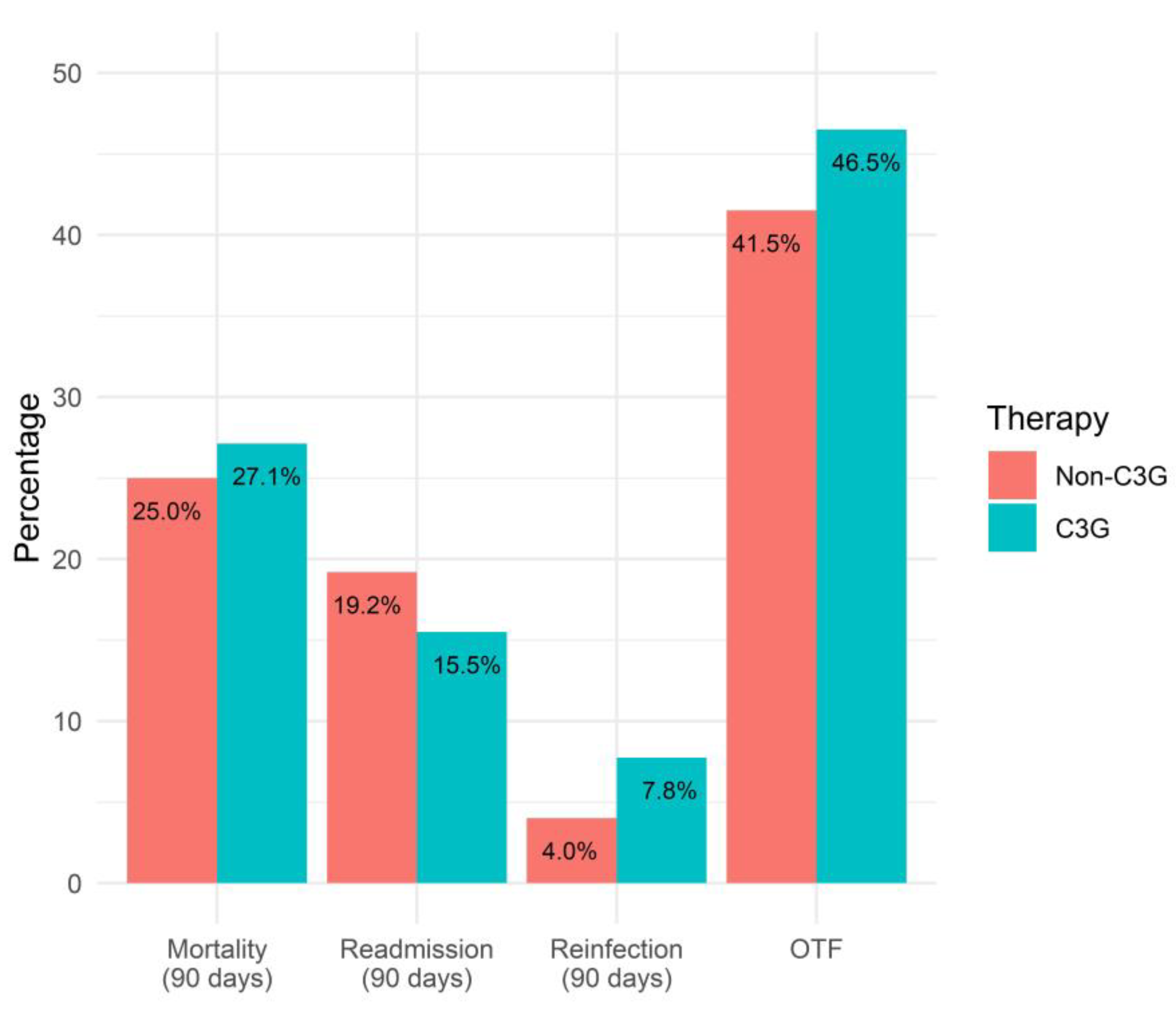
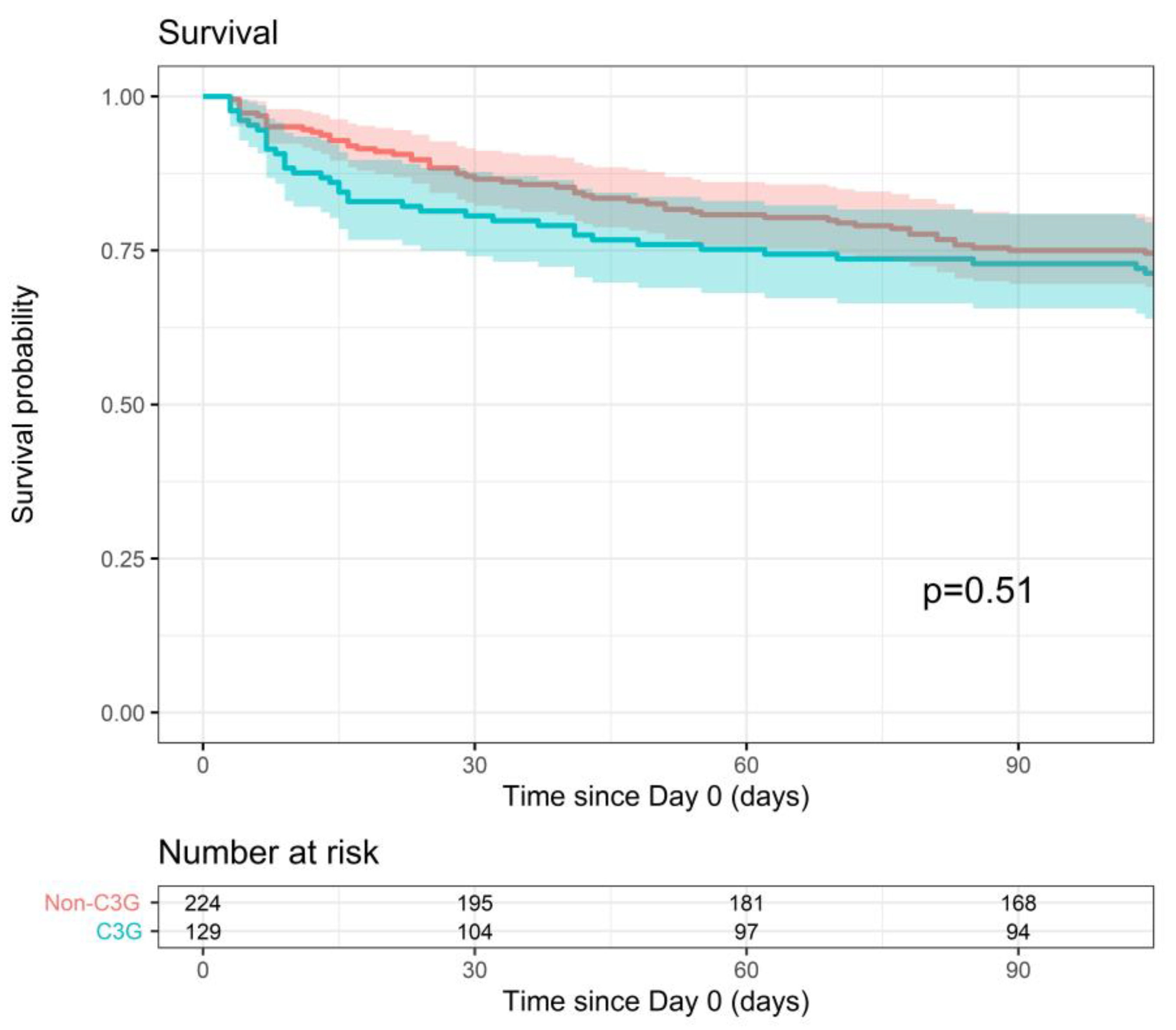
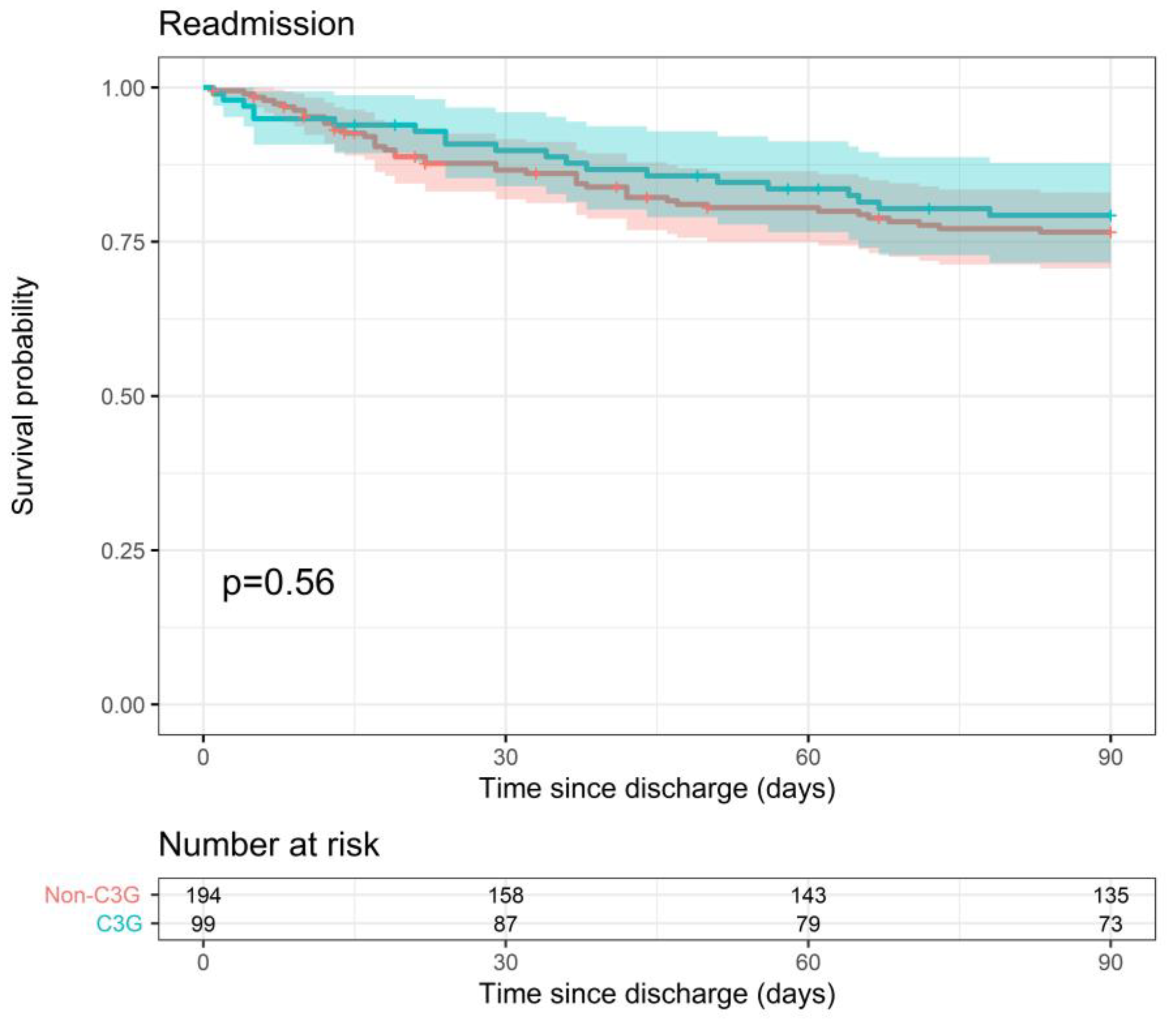
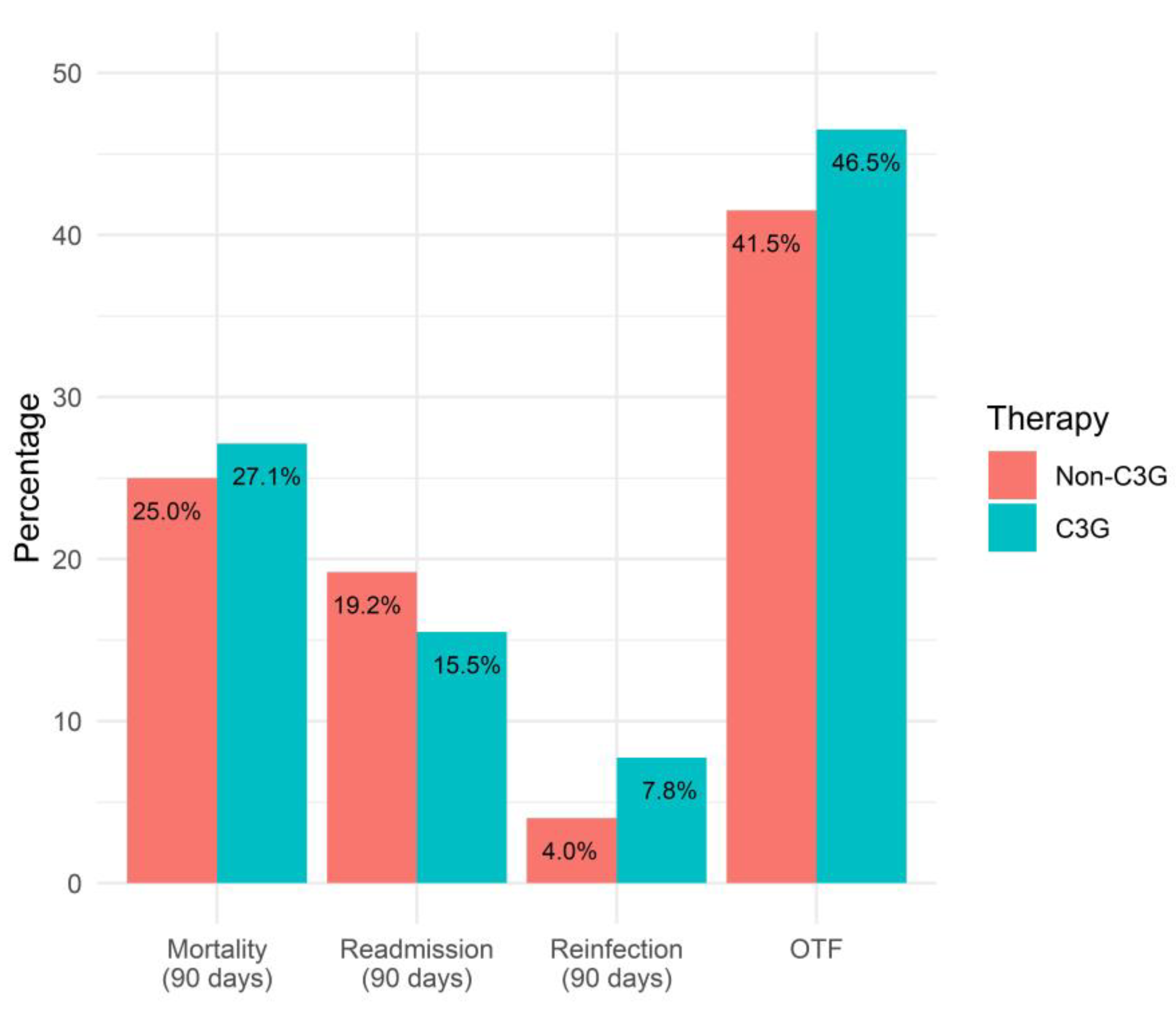
| Outcome | 3GC Definitive Therapy n = 129 | Non-3GC Definitive Therapy n = 224 | p-Value 1 |
|---|---|---|---|
| OTF 2 | 60 (46.5) | 93 (41.5) | 0.36 |
| Survival for: | |||
| Death (all-cause) within 90 days 3 | 72.9 | 75 | 0.51 a |
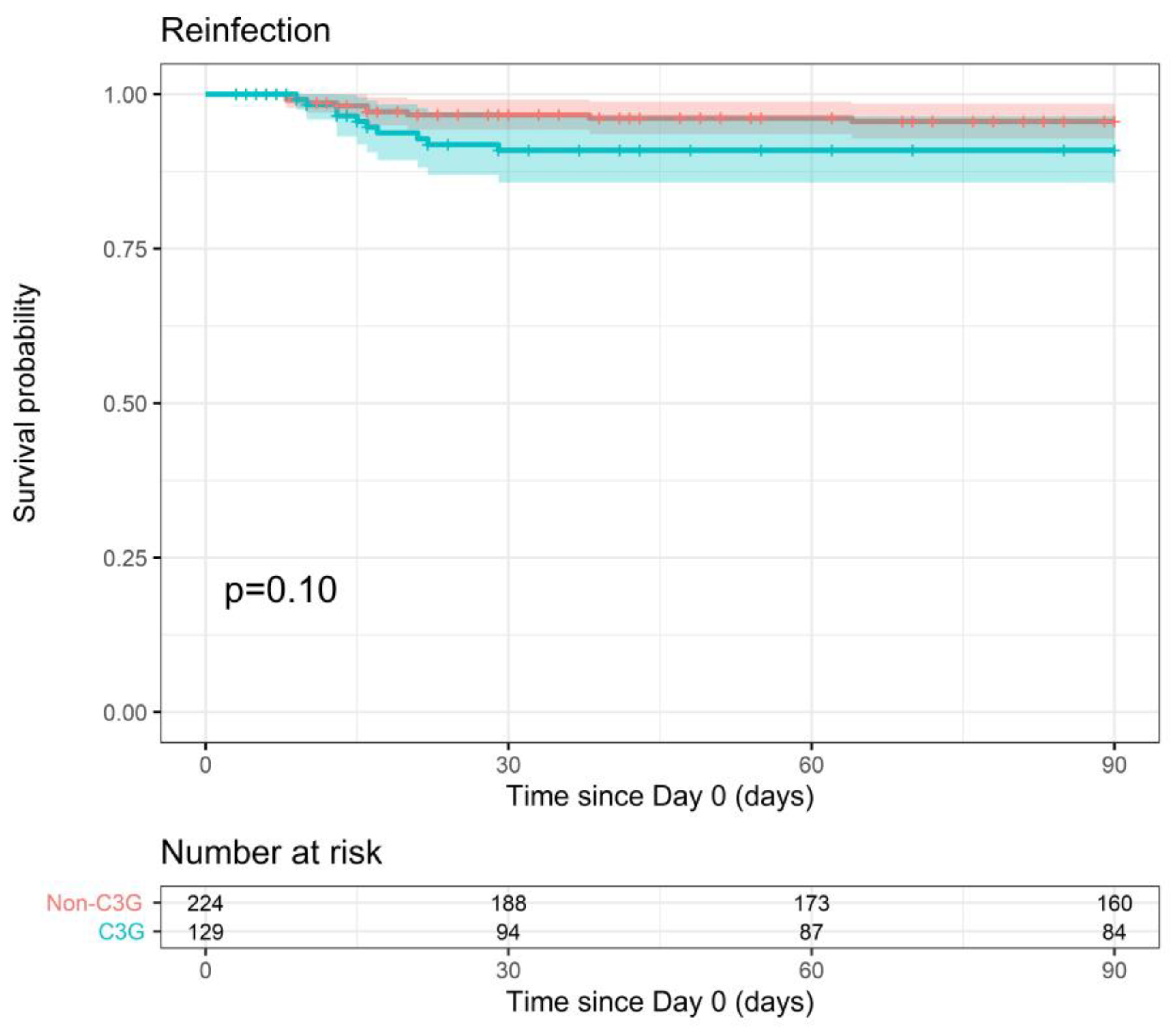
| Reinfection within 90 days 3 | 90.9 | 95.6 | 0.10 b |
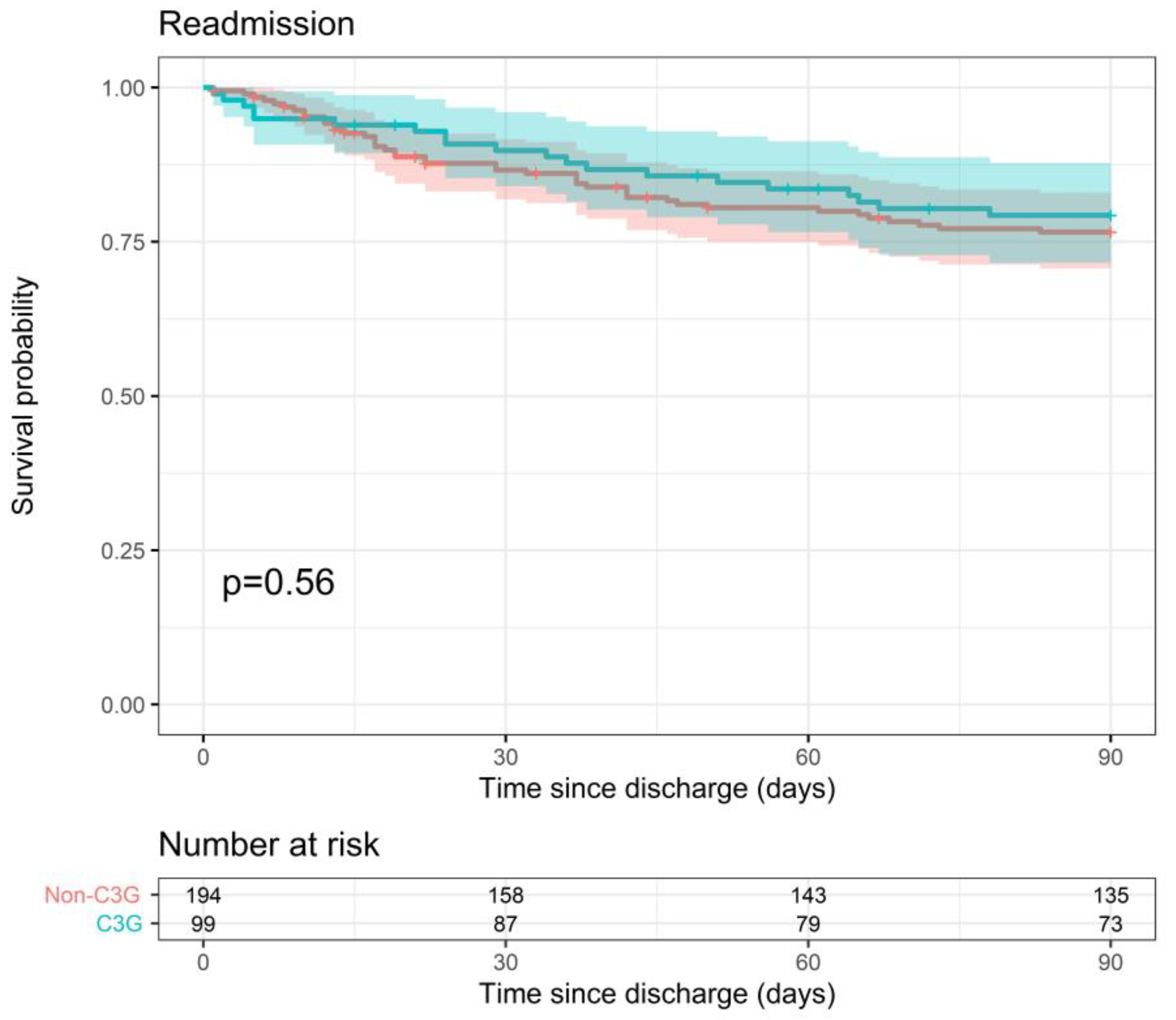
| Readmission within 90 days 3 | 79.3 | 76.6 | 0.56 c |
| Length of stay 4 (days) | 38.0 (15.0;61.0) | 21.0 (10.0;43.5) | 0.0003 |
| In-hospital all-cause mortality 2 | 30 (23.3) | 30 (13.4) | 0.019 a |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vossius, G.; Meex, C.; Moerman, F.; Thys, M.; Ernst, M.; Bourgeois, M.-E.; Wagner, L.; Delahaye, T.; Darcis, G. Clinical Outcomes of Third-Generation Cephalosporin Definitive Therapy for Bloodstream Infections Due to Enterobacterales with Potential AmpC Induction: A Single-Center Retrospective Study. Pathogens 2023, 12, 1152. https://doi.org/10.3390/pathogens12091152
Vossius G, Meex C, Moerman F, Thys M, Ernst M, Bourgeois M-E, Wagner L, Delahaye T, Darcis G. Clinical Outcomes of Third-Generation Cephalosporin Definitive Therapy for Bloodstream Infections Due to Enterobacterales with Potential AmpC Induction: A Single-Center Retrospective Study. Pathogens. 2023; 12(9):1152. https://doi.org/10.3390/pathogens12091152
Chicago/Turabian StyleVossius, Gilles, Cécile Meex, Filip Moerman, Marie Thys, Marie Ernst, Marie-Eve Bourgeois, Léa Wagner, Thibaut Delahaye, and Gilles Darcis. 2023. "Clinical Outcomes of Third-Generation Cephalosporin Definitive Therapy for Bloodstream Infections Due to Enterobacterales with Potential AmpC Induction: A Single-Center Retrospective Study" Pathogens 12, no. 9: 1152. https://doi.org/10.3390/pathogens12091152
APA StyleVossius, G., Meex, C., Moerman, F., Thys, M., Ernst, M., Bourgeois, M.-E., Wagner, L., Delahaye, T., & Darcis, G. (2023). Clinical Outcomes of Third-Generation Cephalosporin Definitive Therapy for Bloodstream Infections Due to Enterobacterales with Potential AmpC Induction: A Single-Center Retrospective Study. Pathogens, 12(9), 1152. https://doi.org/10.3390/pathogens12091152