

Postoperative Prevention of Urinary Tract Infections in Patients after Urogynecological Surgeries—Nonantibiotic Herbal (Canephron) versus Antibiotic Prophylaxis (Fosfomycin Trometamol): A Parallel-Group, Randomized, Noninferiority Experimental Trial
 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
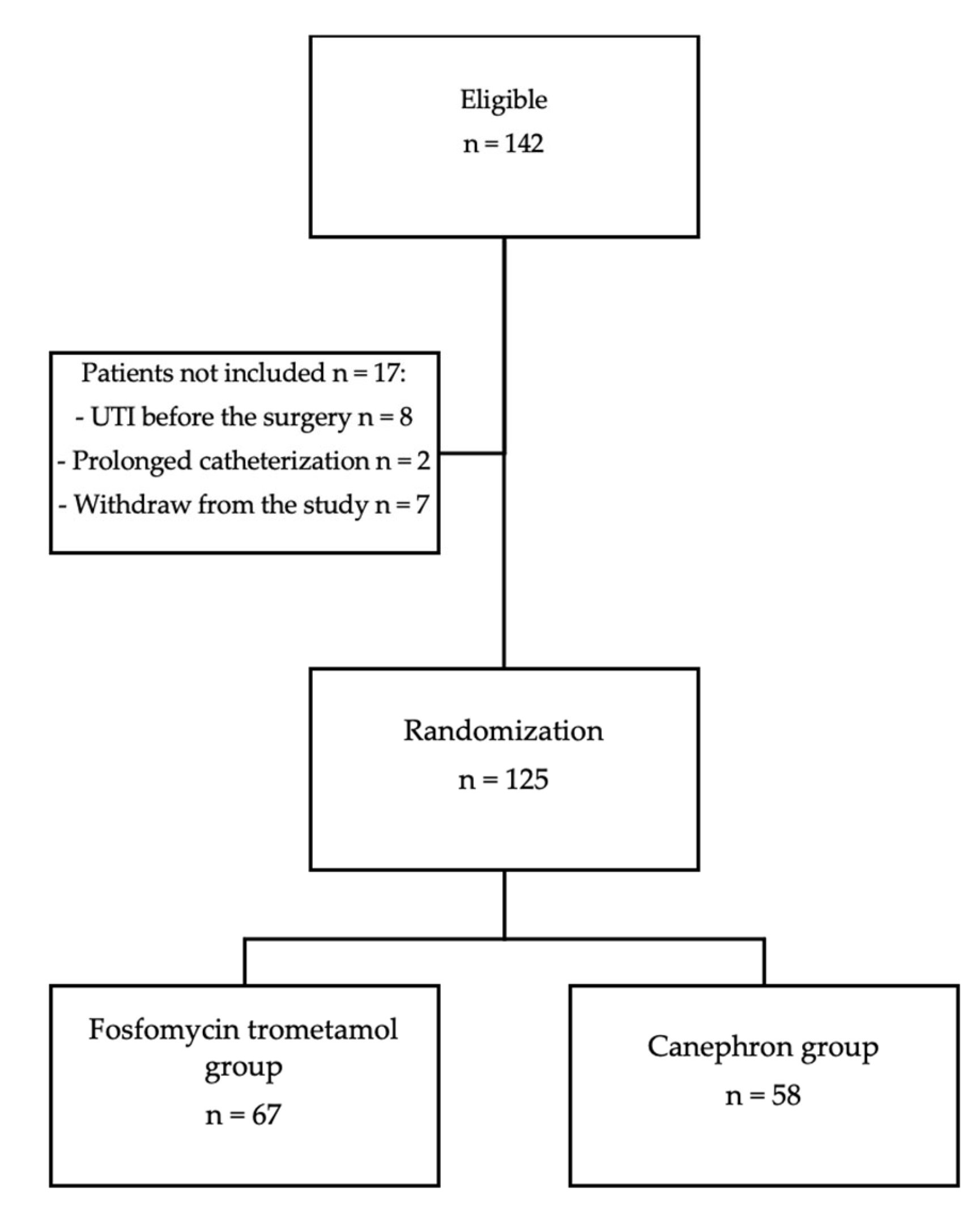
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomas-White, K.J.; Gao, X.; Lin, H.; Fok, C.S.; Ghanayem, K.; Mueller, E.R.; Dong, Q.; Brubaker, L.; Wolfe, A.J. Urinary microbes and postoperative urinary tract infection risk in urogynecologic surgical patients. Int. Urogynecol. J. 2018, 29, 1797–1805. [Google Scholar] [CrossRef] [PubMed]
- Anger, J.T.; Litwin, M.S.; Wang, Q.; Pashos, C.L.; Rodríguez, L.V. Complications of sling surgery among female Medicare beneficiaries. Obstet. Gynecol. 2007, 109, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Miotla, P.; Romanek-Piva, K.; Bogusiewicz, M.; Markut-Miotla, E.; Adamiak, A.; Wróbel, A.; Zebrowska, M.; Wawrysiuk, S.; Mendyk, K.; Rechberger, E.; et al. Antimicrobial Resistance Patterns in Women with Positive Urine Culture: Does Menopausal Status Make a Significant Difference? Biomed. Res. Int. 2017, 2017, 4192908. [Google Scholar] [CrossRef]
- Foxman, B. The epidemiology of urinary tract infection. Nat. Rev. Urol. 2010, 7, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Milan, P.B.; Ivan, I.M. Catheter-associated and nosocomial urinary tract infections: Antibiotic resistance and influence on commonly used antimicrobial therapy. Int. Urol. Nephrol. 2009, 41, 461–464. [Google Scholar] [CrossRef] [PubMed]
- Tandogdu, Z.; Cek, M.; Wagenlehner, F.; Naber, K.; Tenke, P.; van Ostrum, E.; Johansen, T.B. Resistance patterns of nosocomial urinary tract infections in urology departments: 8-year results of the global prevalence of infections in urology study. World J. Urol. 2014, 32, 791–801. [Google Scholar] [CrossRef]
- Naber, K.G. Efficacy and safety of the phytotherapeutic drug Canephron N in prevention and treatment of urogenital and gestational disease: Review of clinical experience in Eastern Europe and Central Asia. Res. Rep. Urol. 2013, 5, 39–46. [Google Scholar] [PubMed]
- Wagenlehner, F.M.; Abramov-Sommariva, D.; Holler, M.; Steindl, H.; Naber, K.G. Non-Antibiotic Herbal Therapy (BNO 1045) versus Antibiotic Therapy (Fosfomycin Trometamol) for the Treatment of Acute Lower Uncomplicated Urinary Tract Infections in Women: A Double-Blind, Parallel-Group, Randomized, Multicentre, Non-Inferiority Phase III Trial. Urol. Int. 2018, 101, 327–336. [Google Scholar]
- Höller, M.; Steindl, H.; Abramov-Sommariva, D.; Wagenlehner, F.; Naber, K.G.; Kostev, K. Treatment of Urinary Tract Infections with Canephron¬ģ in Germany: A Retrospective Database Analysis. Antibiotics 2021, 10, 685. [Google Scholar] [CrossRef]
- Naber, K.G.; Kogan, M.; Wagenlehner, F.M.E.; Siener, R.; Gessner, A. How the microbiome is in- fluenced by the therapy of urological diseases: Standard versus alternative approaches. Clin. Phytosci. 2017, 3, 8. [Google Scholar] [CrossRef]
- Alidjanov, J.F.; Naber, K.G.; Abdufattaev, U.A.; Pilatz, A.; Wagenlehner, F.M. Reevaluation of the Acute Cystitis Symptom Score, a Self-Reporting Questionnaire. Part I. Development, Diagnosis and Differential Diagnosis. Antibiotics 2018, 7, 6. [Google Scholar] [CrossRef]
- Seok, H.; Jeon, J.H.; Choi, H.K.; Choi, W.S.; Park, D.W.; Wi, Y.M.; Ko, K.S.; Peck, K.R. 611. Fosfomycin Resistance of Multidrug-Resistant Escherichia coli and Mechanisms of Fosfomycin Resistance. Open Forum Infect. Dis. 2019, 6 (Suppl. 2), S285. [Google Scholar] [CrossRef]
- Kresken, M.; Pfeifer, Y.; Hafner, D.; Wresch, R.; Korber-Irrgang, B. Occurrence of multidrug resistance to oral antibiotics among Escherichia coli urine isolates from outpatient departments in Germany: Extended-spectrum beta-lactamases and the role of fosfomycin. Int. J. Antimicrob. Agents 2014, 44, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Campbell, I. Chi‚ Äźsquared and Fisher-Irwin tests of two‚ Äźby‚ Äźtwo tables with small sample recommendations. Stat. Med. 2007, 26, 3661–3675. [Google Scholar] [CrossRef] [PubMed]
- Busing, F.M.; Weaver, B.; Dubois, S. 2 √ó 2 Tables: A note on Campbell’s recommendation. Stat. Med. 2016, 15, 1354–1358. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Berger, A.A.; Tan-Kim, J.; Menefee, S.A. The impact of midurethral sling surgery on the development of urinary tract infections. Int. Urogynecol. J. 2022, 33, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Miotla, P.; Wawrysiuk, S.; Naber, K.; Markut-Miotla, E.; Skorupski, P.; Skorupska, K.; Rechberger, T. Should We Always Use Antibiotics after Urodynamic Studies in High-Risk Patients? Biomed. Res. Int. 2018, 5, 1607425. [Google Scholar] [CrossRef]
- Xie, N.; Hu, Z.; Ye, Z.; Xu, Q.; Chen, J.; Lin, Y. A systematic review comparing early with late removal of indwelling urinary catheters after pelvic organ prolapse surgery. Int. Urogynecol. J. 2021, 32, 1361–1372. [Google Scholar] [CrossRef]
- Kranz, J.; Schmidt, S.; Wagenlehner, F.; Schneidewind, L. Catheter-Associated Urinary Tract Infections in Adult Patients. Dtsch. Arztebl. Int. 2020, 117, 83–88. [Google Scholar] [CrossRef]
- Nicolle, L.E. Catheter-related urinary tract infection. Drugs Aging 2005, 22, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Trautner, B.W.; Darouiche, R.O. Role of biofilm in catheter-associated urinary tract infection. Am. J. Infect. Control 2004, 32, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Kingdom, J.C.; Kitchener, H.C.; MacLean, A.B. Postoperative urinary tract infection in gynecology: Implications for an antibiotic prophylaxis policy. Obstet. Gynecol. 1990, 76, 636–638. [Google Scholar] [CrossRef] [PubMed]
- Rogers, R.G.; Kammerer-Doak, D.; Olsen, A.; Thompson, P.K.; Walters, M.D.; Lukacz, E.S.; Qualls, C. A randomized, double-blind, placebo-controlled comparison of the effect of nitrofurantoin monohydrate macrocrystals on the development of urinary tract infections after surgery for pelvic organ prolapse and/or stress urinary incontinence with suprapubic catheterization. Am. J. Obstet. Gynecol. 2004, 191, 182–187. [Google Scholar] [PubMed]
- van der Wall, E.; Verkooyen, R.P.; Mintjes-de Groot, J.; Oostinga, J.; van Dijk, A.; Hustinx, W.N.; Verbrugh, H.A. Prophylactic ciprofloxacin for catheter-associated urinary-tract infection. Lancet 1992, 18, 946–951. [Google Scholar]
- Jung, C.; Brubaker, L. The etiology and management of recurrent urinary tract infections in postmenopausal women. Climacteric 2019, 22, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Sanaee, M.S.; Pan, K.; Lee, T.; Koenig, N.A.; Geoffrion, R. Urinary tract infection after clean-contaminated pelvic surgery: A retrospective cohort study and prediction model. Int. Urogynecol. J. 2020, 31, 1821–1828. [Google Scholar] [CrossRef]
- Semins, M.J.; Shore, A.D.; Makary, M.A.; Weiner, J.; Matlaga, B.R. The impact of obesity on urinary tract infection risk. Urology 2012, 79, 266–269. [Google Scholar] [CrossRef]
- Weintraub, A.Y.; Reuven, Y.; Paz-Levy, D.; Yohay, Z.; Idan, I.; Elharar, D.; Glinter, H.; Tzur, T.; Yohay, D. Prevalence and risk factors for urinary tract infection up to one year following midurethral sling incontinence surgery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 222, 146–150. [Google Scholar] [CrossRef]
- Bretschneider, C.E.; Sheyn, D.; Mahajan, S.; Propst, K.; Ridgeway, B. Complications following vaginal colpopexy for the repair of pelvic organ prolapse. Int. Urogynecol. J. 2021, 32, 993–999. [Google Scholar] [CrossRef]
- Sutkin, G.; Alperin, M.; Meyn, L.; Wiesenfeld, H.C.; Ellison, R.; Zyczynski, H.M. Symptomatic urinary tract infections after surgery for prolapse and/or incontinence. Int. Urogynecol. J. 2010, 21, 955–961. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Fosfomycin Trometamol (n = 67) | Canephron (n = 58) | p |
|---|---|---|---|
| Age (years), M ± SD | 57.6 ± 12.5 | 57.7 ± 13.0 | p = 0.989 |
| BMI (kg/m2), M ± SD | 28.8 ± 5.8 | 28.4 ± 4.8 | p = 0.616 |
| Parity, M ± SD | 2.1 ± 0.8 | 2.0 ± 0.7 | p = 0.716 |
| Menopause, number (%) | 47 (70%) | 38 (66%) | p = 0.332 |
| Total Scores in ACSS Domains | Fosfomycin Trometamol | Canephron | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Day 1 | Day 14 | z Value | p Value | Day 1 | Day 14 | z Value | p Value | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||||
| “Typical” | 3.21 | 3.58 | 1.45 | 2.88 | 5.20 | <0.001 | 2.72 | 2.81 | 0.62 | 1.17 | 4.34 | <0.001 |
| “Differential” | 0.63 | 1.51 | 0.28 | 0.77 | 1.85 | 0.064 | 1.07 | 1.69 | 0.24 | 0.78 | 3.12 | 0.002 |
| “Quality of life” | 2.13 | 2.30 | 0.93 | 1.69 | 3.45 | 0.001 | 1.26 | 1.51 | 0.64 | 1.18 | 2.94 | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wawrysiuk, S.; Rechberger, T.; Kubik-Komar, A.; Kolodynska, A.; Naber, K.; Miotla, P. Postoperative Prevention of Urinary Tract Infections in Patients after Urogynecological Surgeries—Nonantibiotic Herbal (Canephron) versus Antibiotic Prophylaxis (Fosfomycin Trometamol): A Parallel-Group, Randomized, Noninferiority Experimental Trial. Pathogens 2023, 12, 27. https://doi.org/10.3390/pathogens12010027
Wawrysiuk S, Rechberger T, Kubik-Komar A, Kolodynska A, Naber K, Miotla P. Postoperative Prevention of Urinary Tract Infections in Patients after Urogynecological Surgeries—Nonantibiotic Herbal (Canephron) versus Antibiotic Prophylaxis (Fosfomycin Trometamol): A Parallel-Group, Randomized, Noninferiority Experimental Trial. Pathogens. 2023; 12(1):27. https://doi.org/10.3390/pathogens12010027
Chicago/Turabian StyleWawrysiuk, Sara, Tomasz Rechberger, Agnieszka Kubik-Komar, Aleksandra Kolodynska, Kurt Naber, and Pawel Miotla. 2023. "Postoperative Prevention of Urinary Tract Infections in Patients after Urogynecological Surgeries—Nonantibiotic Herbal (Canephron) versus Antibiotic Prophylaxis (Fosfomycin Trometamol): A Parallel-Group, Randomized, Noninferiority Experimental Trial" Pathogens 12, no. 1: 27. https://doi.org/10.3390/pathogens12010027
APA StyleWawrysiuk, S., Rechberger, T., Kubik-Komar, A., Kolodynska, A., Naber, K., & Miotla, P. (2023). Postoperative Prevention of Urinary Tract Infections in Patients after Urogynecological Surgeries—Nonantibiotic Herbal (Canephron) versus Antibiotic Prophylaxis (Fosfomycin Trometamol): A Parallel-Group, Randomized, Noninferiority Experimental Trial. Pathogens, 12(1), 27. https://doi.org/10.3390/pathogens12010027