
Risk Factors for Hospital Readmission for Clostridioides difficile Infection: A Statewide Retrospective Cohort Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
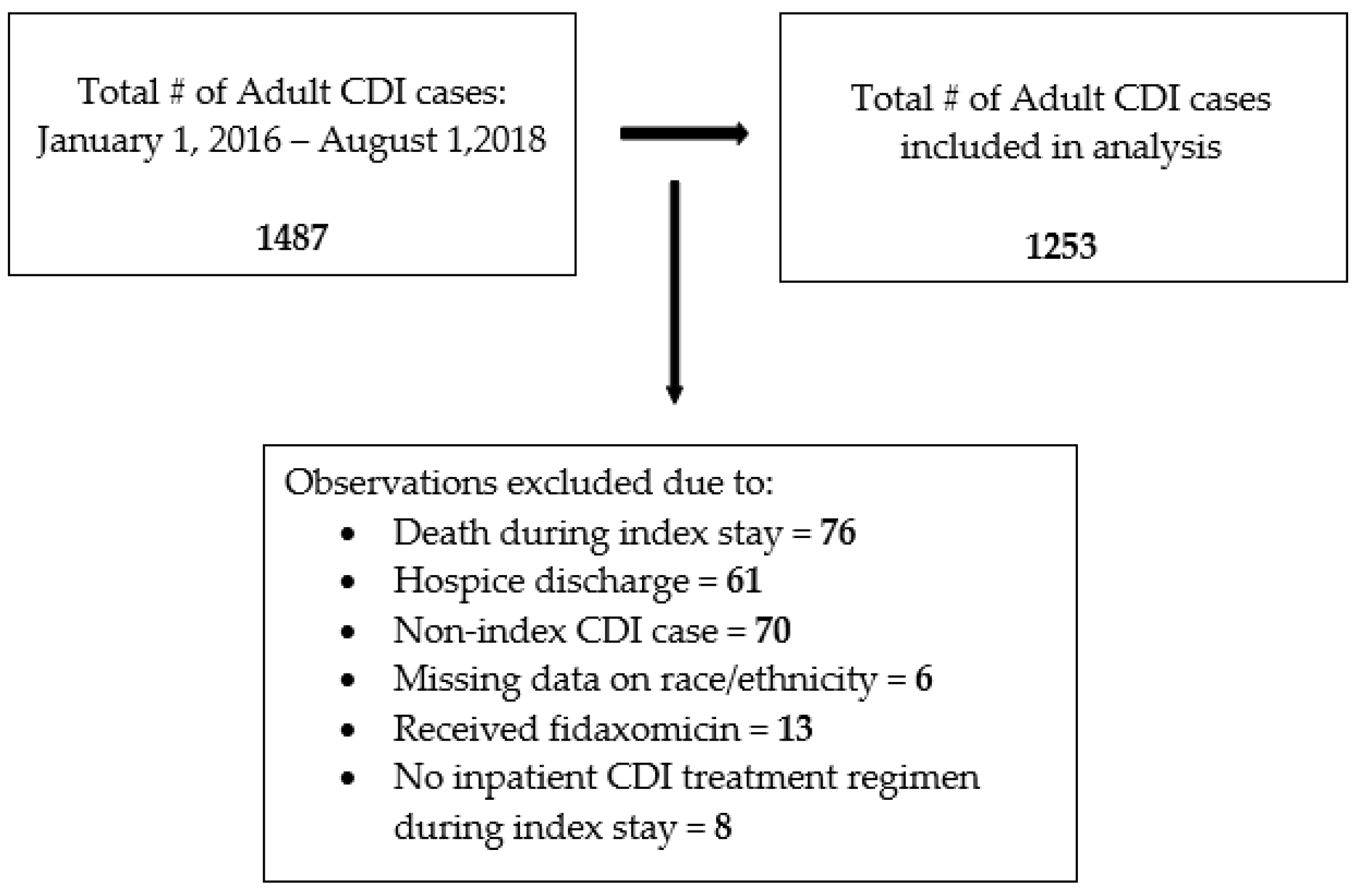
2.1. Patient Selection
2.2. CDI Index Case Definition
2.3. Study Variables
2.4. Study Outcome
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Community Associated | Specimen collected on Day 1, 2, or 3 of inpatient admission and patients were not previously discharged from an inpatient setting within 28 days of collection date |
| Community-Onset Healthcare Facility Associated | Specimen collected on Day 1, 2, or 3 of inpatient admission and patients were previously discharged from an inpatient setting within 28 days of collection date |
| Hospital-Onset | Specimen collected > 3 days after inpatient admission date |
References
- Mullish, B.H.; Williams, H.R. Clostridium difficile Infection and Antibiotic-Associated Diarrhoea. Clin. Med. 2018, 18, 237–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loo, V.G.; Bourgault, A.-M.; Poirier, L.; Lamothe, F.; Michaud, S.; Turgeon, N.; Toye, B.; Beaudoin, A.; Frost, E.H.; Gilca, R.; et al. Host and Pathogen Factors for Clostridium difficile Infection and Colonization. N. Engl. J. Med. 2011, 365, 1693–1703. [Google Scholar] [CrossRef] [Green Version]
- Henrich, T.J.; Krakower, D.; Bitton, A.; Yokoe, D.S. Clinical Risk Factors for Severe Clostridium difficile–Associated Disease. Emerg. Infect. Dis. 2009, 15, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Ofori, E.; Ramai, D.; Dhawan, M.; Mustafa, F.; Gasperino, J.; Reddy, M. Community-Acquired Clostridium difficile: Epidemiology, Ribotype, Risk Factors, Hospital and Intensive Care Unit Outcomes, and Current and Emerging Therapies. J. Hosp. Infect. 2018, 99, 436–442. [Google Scholar] [CrossRef]
- Guh, A.Y.; Mu, Y.; Winston, L.G.; Johnston, H.; Olson, D.; Farley, M.M.; Wilson, L.E.; Holzbauer, S.M.; Phipps, E.C.; Dumyati, G.K.; et al. Trends in U.S. Burden of Clostridioides Difficile Infection and Outcomes. N. Engl. J. Med. 2020, 382, 1320–1330. [Google Scholar] [CrossRef] [PubMed]
- Debast, S.B.; Bauer, M.P.; Kuijper, E.J. European Society of Clinical Microbiology and Infectious Diseases: Update of the Treatment Guidance Document for Clostridium difficile Infection. Clin. Microbiol. Infect. 2014, 20, 1–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 66, e1–e48. [Google Scholar] [CrossRef]
- Kelly, C.P. Can We Identify Patients at High Risk of Recurrent Clostridium difficile Infection? Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2012, 18 (Suppl. S6), 21–27. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.P.; LaMont, J.T. Clostridium difficile--More Difficult than Ever. N. Engl. J. Med. 2008, 359, 1932–1940. [Google Scholar] [CrossRef]
- Deshpande, A.; Pant, C.; Olyaee, M.; Donskey, C.J. Hospital Readmissions Related to Clostridium difficile Infection in the United States. Am. J. Infect. Control 2018, 46, 346–347. [Google Scholar] [CrossRef]
- Chopra, T.; Neelakanta, A.; Dombecki, C.; Awali, R.A.; Sharma, S.; Kaye, K.S.; Patel, P. Burden of Clostridium difficile Infection on Hospital Readmissions and Its Potential Impact under the Hospital Readmission Reduction Program. Am. J. Infect. Control 2015, 43, 314–317. [Google Scholar] [CrossRef] [PubMed]
- Olsen, M.A.; Yan, Y.; Reske, K.A.; Zilberberg, M.; Dubberke, E.R. Impact of Clostridium difficile Recurrence on Hospital Readmissions. Am. J. Infect. Control 2015, 43, 318–322. [Google Scholar] [CrossRef] [PubMed]
- van Walraven, C.; Austin, P.C.; Jennings, A.; Quan, H.; Forster, A.J. A Modification of the Elixhauser Comorbidity Measures into a Point System for Hospital Death Using Administrative Data. Med. Care 2009, 47, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.-C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding Algorithms for Defining Comorbidities in ICD-9-CM and ICD-10 Administrative Data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef]
- Brown, K.A.; Khanafer, N.; Daneman, N.; Fisman, D.N. Meta-Analysis of Antibiotics and the Risk of Community-Associated Clostridium difficile Infection. Antimicrob. Agents Chemother. 2013, 57, 2326–2332. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, A.; Pasupuleti, V.; Thota, P.; Pant, C.; Rolston, D.D.K.; Sferra, T.J.; Hernandez, A.V.; Donskey, C.J. Community-Associated Clostridium difficile Infection and Antibiotics: A Meta-Analysis. J. Antimicrob. Chemother. 2013, 68, 1951–1961. [Google Scholar] [CrossRef] [Green Version]
- Multidrug-Resistant Organism & Clostridioides Difficile Infection (MDRO/CDI) Module. Available online: https://www.cdc.gov/nhsn/psc/cdiff/index.html (accessed on 27 April 2022).
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile Infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef] [Green Version]
- Kulesa, A.; Krzywinski, M.; Blainey, P.; Altman, N. Sampling Distributions and the Bootstrap. Nat. Methods 2015, 12, 477–478. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. The Odds Ratio. BMJ 2000, 320, 1468. [Google Scholar] [CrossRef] [Green Version]
- DiCiccio, T.J.; Efron, B. Bootstrap Confidence Intervals. Stat. Sci. 1996, 11, 189–228. [Google Scholar] [CrossRef]
- Carpenter, J.; Bithell, J. Bootstrap Confidence Intervals: When, Which, What? A Practical Guide for Medical Statisticians. Stat. Med. 2000, 19, 1141–1164. [Google Scholar] [CrossRef]
- Psoinos, C.M.; Collins, C.E.; Ayturk, M.D.; Anderson, F.A.; Santry, H.P. Post-Hospitalization Treatment Regimen and Readmission for C. Difficile Colitis in Medicare Beneficiaries. World J. Surg. 2018, 42, 246–253. [Google Scholar] [CrossRef]
- Verheyen, E.; Dalapathi, V.; Arora, S.; Patel, K.; Mankal, P.K.; Kumar, V.; Lung, E.; Kotler, D.P.; Grinspan, A. High 30-Day Readmission Rates Associated with Clostridiumdifficile Infection. Am. J. Infect. Control 2019, 47, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Ayturk, M.D.; Anderson, F.A.; Santry, H.P. Predictors and Outcomes of Readmission for Clostridium difficile in a National Sample of Medicare Beneficiaries. J. Gastrointest. Surg. 2015, 19, 88–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, G.J.; Min, L.C.; Liu, H.; Marciniak, D.J.; Mody, L. Role of Post-Acute Care in Readmissions for Preexisting Healthcare-Associated Infections. J. Am. Geriatr. Soc. 2020, 68, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Dinh, A.; Le Monnier, A.; Emery, C.; Alami, S.; Torreton, É.; Duburcq, A.; Barbier, F. Predictors and Burden of Hospital Readmission with Recurrent Clostridioides Difficile Infection: A French Nation-Wide Inception Cohort Study. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2019, 38, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- The Core Elements of Hospital Antibiotic Stewardship Programs. Available online: https://www.cdc.gov/antibiotic-use/healthcare/pdfs/hospital-core-elements-H.pdf (accessed on 24 March 2022).
- Purba, A.K.R.; Setiawan, D.; Bathoorn, E.; Postma, M.J.; Dik, J.-W.H.; Friedrich, A.W. Prevention of Surgical Site Infections: A Systematic Review of Cost Analyses in the Use of Prophylactic Antibiotics. Front. Pharmacol. 2018, 9, 776. [Google Scholar] [CrossRef]
- Najjar, P.A.; Smink, D.S. Prophylactic Antibiotics and Prevention of Surgical Site Infections. Surg. Clin. N. Am. 2015, 95, 269–283. [Google Scholar] [CrossRef]
- Davey, P.; Marwick, C.A.; Scott, C.L.; Charani, E.; McNeil, K.; Brown, E.; Gould, I.M.; Ramsay, C.R.; Michie, S. Interventions to Improve Antibiotic Prescribing Practices for Hospital Inpatients. Cochrane Database Syst. Rev. 2017, 2, CD003543. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Xie, K.; Zhang, C.; Liang, Y.; Chen, Z.; Wang, H. C-Reactive Protein Testing to Reduce Antibiotic Prescribing for Acute Respiratory Infections in Adults: A Systematic Review and Meta-Analysis. J. Thorac. Dis. 2022, 14, 123–134. [Google Scholar] [CrossRef]
- Spigaglia, P. COVID-19 and Clostridioides Difficile Infection (CDI): Possible Implications for Elderly Patients. Anaerobe 2020, 64, 102233. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.; Gladstone, B.P.; Burkert, F.; Carrara, E.; Foschi, F.; Döbele, S.; Tacconelli, E. Effect of Antibiotic Stewardship on the Incidence of Infection and Colonisation with Antibiotic-Resistant Bacteria and Clostridium difficile Infection: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Abou Chakra, C.N.; Pepin, J.; Sirard, S.; Valiquette, L. Risk Factors for Recurrence, Complications and Mortality in Clostridium difficile Infection: A Systematic Review. PLoS ONE 2014, 9, e98400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dingle, K.E.; Didelot, X.; Quan, T.P.; Eyre, D.W.; Stoesser, N.; Golubchik, T.; Harding, R.M.; Wilson, D.J.; Griffiths, D.; Vaughan, A.; et al. Effects of Control Interventions on Clostridium difficile Infection in England: An Observational Study. Lancet Infect. Dis. 2017, 17, 411–421. [Google Scholar] [CrossRef] [Green Version]
- Wenzler, E.; Mulugeta, S.G.; Danziger, L.H. The Antimicrobial Stewardship Approach to Combating Clostridium difficile. Antibiot. Basel Switz. 2015, 4, 198–215. [Google Scholar] [CrossRef]
- Zacharioudakis, I.M.; Zervou, F.N.; Shehadeh, F.; Mylona, E.K.; Mylonakis, E. Association of Community Factors with Hospital-Onset Clostridioides (Clostridium) Difficile Infection: A Population Based U.S.-Wide Study. EClinicalMedicine 2019, 8, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.A.; Langford, B.; Schwartz, K.L.; Diong, C.; Garber, G.; Daneman, N. Antibiotic Prescribing Choices and Their Comparative C. Difficile Infection Risks: A Longitudinal Case-Cohort Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 72, 836–844. [Google Scholar] [CrossRef] [Green Version]
- Blot, S.; Ruppé, E.; Harbarth, S.; Asehnoune, K.; Poulakou, G.; Luyt, C.-E.; Rello, J.; Klompas, M.; Depuydt, P.; Eckmann, C.; et al. Healthcare-Associated Infections in Adult Intensive Care Unit Patients: Changes in Epidemiology, Diagnosis, Prevention and Contributions of New Technologies. Intensive Crit. Care Nurs. 2022, 70, 103227. [Google Scholar] [CrossRef]
- Guh, A.Y.; Adkins, S.H.; Li, Q.; Bulens, S.N.; Farley, M.M.; Smith, Z.; Holzbauer, S.M.; Whitten, T.; Phipps, E.C.; Hancock, E.B.; et al. Risk Factors for Community-Associated Clostridium difficile Infection in Adults: A Case-Control Study. Open Forum Infect. Dis. 2017, 4, ofx171. [Google Scholar] [CrossRef] [Green Version]
- Ziakas, P.D.; Zacharioudakis, I.M.; Zervou, F.N.; Grigoras, C.; Pliakos, E.E.; Mylonakis, E. Asymptomatic Carriers of Toxigenic C. Difficile in Long-Term Care Facilities: A Meta-Analysis of Prevalence and Risk Factors. PLoS ONE 2015, 10, e0117195. [Google Scholar] [CrossRef]
- Campbell, R.J.; Giljahn, L.; Machesky, K.; Cibulskas-White, K.; Lane, L.M.; Porter, K.; Paulson, J.O.; Smith, F.W.; McDonald, L.C. Clostridium difficile Infection in Ohio Hospitals and Nursing Homes during 2006. Infect. Control Hosp. Epidemiol. 2009, 30, 526–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karanika, S.; Grigoras, C.; Flokas, M.E.; Alevizakos, M.; Kinamon, T.; Kojic, E.M.; Mylonakis, E. The Attributable Burden of Clostridium difficile Infection to Long-Term Care Facilities Stay: A Clinical Study. J. Am. Geriatr. Soc. 2017, 65, 1733–1740. [Google Scholar] [CrossRef] [PubMed]
- McConeghy, K.W.; Zullo, A.R.; Lary, C.W.; Zhang, T.; Lee, Y.; Daiello, L.; Kiel, D.P.; Berry, S. Association Between Bisphosphonates and Hospitalized Clostridioides Difficile Infection Among Frail Older Adults. J. Am. Med. Dir. Assoc. 2020, 21, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Costantino, M.E.; Frey, B.; Hall, B.; Painter, P. The Influence of a Postdischarge Intervention on Reducing Hospital Readmissions in a Medicare Population. Popul. Health Manag. 2013, 16, 310–316. [Google Scholar] [CrossRef] [Green Version]
- Dubberke, E.R.; Olsen, M.A. Burden of Clostridium difficile on the Healthcare System. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 55 (Suppl. S2), S88–S892. [Google Scholar] [CrossRef]
- Zhang, S.; Palazuelos-Munoz, S.; Balsells, E.M.; Nair, H.; Chit, A.; Kyaw, M.H. Cost of Hospital Management of Clostridium difficile Infection in United States-a Meta-Analysis and Modelling Study. BMC Infect. Dis. 2016, 16, 447. [Google Scholar] [CrossRef] [Green Version]
- Tsigrelis, C. Recurrent Clostridioides Difficile Infection: Recognition, Management, Prevention. Cleve. Clin. J. Med. 2020, 87, 347–359. [Google Scholar] [CrossRef]
| Index Cases N (%) | Readmitted for CDI N (%) | Not Readmitted for CDI N (%) | p-Value | |
|---|---|---|---|---|
| Overall | 1253 | 140 | 1113 | |
| Age | 0.474 | |||
| 18–44 | 186 (15) | 24 (17) | 162 (15) | |
| 45–64 | 373 (30) | 46 (33) | 327 (29) | |
| 65–79 | 389 (31) | 36 (26) | 353 (32) | |
| Over 80 | 305 (24) | 34 (24) | 271 (24) | |
| Sex | 0.687 | |||
| Female | 718 (57) | 78 (56) | 640 (58) | |
| Male | 535 (43) | 62 (44) | 473 (42) | |
| Race/Ethnicity | 0.430 | |||
| Non-Hispanic White | 1020 (81) | 107 (76) | 913 (82) | |
| Hispanic or Latino | 117 (9) | 17 (12) | 100 (9) | |
| Non-Hispanic Black | 84 (7) | 11 (8) | 73 (6) | |
| Other | 32 (3) | 5 (4) | 27 (3) | |
| CDI Index Case Classification | 0.479 | |||
| Community Associated | 500 (40) | 52 (37) | 448 (40) | |
| Healthcare Associated | 753 (60) | 88 (63) | 665 (60) | |
| CDI Treatment Regimen | 0.479 | |||
| Vancomycin | 507 (40) | 61 (44) | 446 (40) | |
| Metronidazole | 315 (25) | 29 (21) | 286 (26) | |
| Sequential | 323 (26) | 40 (29) | 283 (25) | |
| Concurrent | 108 (9) | 10 (7) | 98 (9) | |
| Discharge Disposition | 0.019 | |||
| Healthcare Facilities | 509 (41) | 44 (31) | 465 (42) | |
| Home | 744 (59) | 96 (69) | 648 (58) | |
| High-Risk Antibiotic ° | 0.763 | |||
| No | 453 (36) | 49 (35) | 404 (36) | |
| Yes | 800 (64) | 91 (65) | 709 (64) | |
| Elixhauser Score | 0.004 | |||
| Median [IQR] | 5 [0–11] | 6 [0–13] | 5 [0–10] | |
| Length of Index Stay (days) | 0.094 | |||
| Median [IQR] | 7 [4–13] | 6 [4–10.5] | 7 [4–13] |
| Adjusted Odds Ratio | 95% CI | 95% BCa-CI | |
|---|---|---|---|
| Age | |||
| 18–44 | Reference | ||
| 45–64 | 0.91 | 0.52–1.58 | 0.52–1.58 |
| 65–79 | 0.63 | 0.35–1.15 | 0.35–1.22 |
| Over 80 | 0.84 | 0.45–1.57 | 0.43–1.65 |
| Sex | |||
| Female | Reference | ||
| Male | 1.02 | 0.71–1.47 | 0.69–1.52 |
| Race/Ethnicity | |||
| Non-Hispanic White | Reference | ||
| Hispanic or Latino | 1.17 | 0.65–2.10 | 0.62–2.04 |
| Non-Hispanic Black | 1.15 | 0.57–2.31 | 0.54–2.17 |
| Other | 1.74 | 0.64–4.76 | 0.49– 5.24 |
| CDI Index Case Classification | |||
| Community Associated | Reference | ||
| Healthcare Associated | 1.46 | 0.95–2.22 | 0.91–2.29 |
| CDI Treatment Regimen | |||
| Vancomycin | Reference | ||
| Metronidazole | 0.70 | 0.42–1.18 | 0.42–1.13 |
| Sequential | 1.13 | 0.72–1.78 | 0.76–1.83 |
| Concurrent | 0.74 | 0.35–1.56 | 0.31–1.38 |
| Discharge Disposition | |||
| Healthcare Facilities | Reference | ||
| Home | 1.64 | 1.06–2.54 | 1.03–2.71 |
| Fluoroquinolones | |||
| No | Reference | ||
| Yes | 1.58 | 1.05–2.37 | 1.01–2.31 |
| 1st/2nd Cephalosporins | |||
| No | Reference | ||
| Yes | 0.82 | 0.49–1.38 | 0.47–1.39 |
| 3rd/4th/5th Cephalosporins | |||
| No | Reference | ||
| Yes | 0.98 | 0.65–1.48 | 0.63–1.48 |
| Clindamycin | |||
| No | Reference | ||
| Yes | 0.79 | 0.32–1.95 | 0.26–1.96 |
| Penicillin | |||
| No | Reference | ||
| Yes | 0.94 | 0.46–1.89 | 0.44–1.95 |
| Penicillin with Beta Lactamase Inhibitors | |||
| No | Reference | ||
| Yes | 0.99 | 0.66–1.48 | 0.67–1.49 |
| Elixhauser Score | |||
| Unit Increase | 1.05 | 1.02–1.07 | 1.01–1.07 |
| Length of Index Stay (Day) | |||
| Unit Increase | 0.97 | 0.95–1.00 | 0.95–0.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benitez, G.; Shehadeh, F.; Kalligeros, M.; Mylona, E.K.; Tran, Q.-L.; Zacharioudakis, I.M.; Mylonakis, E. Risk Factors for Hospital Readmission for Clostridioides difficile Infection: A Statewide Retrospective Cohort Study. Pathogens 2022, 11, 555. https://doi.org/10.3390/pathogens11050555
Benitez G, Shehadeh F, Kalligeros M, Mylona EK, Tran Q-L, Zacharioudakis IM, Mylonakis E. Risk Factors for Hospital Readmission for Clostridioides difficile Infection: A Statewide Retrospective Cohort Study. Pathogens. 2022; 11(5):555. https://doi.org/10.3390/pathogens11050555
Chicago/Turabian StyleBenitez, Gregorio, Fadi Shehadeh, Markos Kalligeros, Evangelia K. Mylona, Quynh-Lam Tran, Ioannis M. Zacharioudakis, and Eleftherios Mylonakis. 2022. "Risk Factors for Hospital Readmission for Clostridioides difficile Infection: A Statewide Retrospective Cohort Study" Pathogens 11, no. 5: 555. https://doi.org/10.3390/pathogens11050555
APA StyleBenitez, G., Shehadeh, F., Kalligeros, M., Mylona, E. K., Tran, Q.-L., Zacharioudakis, I. M., & Mylonakis, E. (2022). Risk Factors for Hospital Readmission for Clostridioides difficile Infection: A Statewide Retrospective Cohort Study. Pathogens, 11(5), 555. https://doi.org/10.3390/pathogens11050555