
Phenotypic and Molecular Characterization of Nonfermenting Gram-Negative Bacilli Causing Peritonitis in Peritoneal Dialysis Patients

 ,
,  and
and
Abstract
:1. Introduction
2. Results
2.1. Sampling and Identification
2.2. In Vitro Susceptibility
2.3. Biofilm Production
2.4. Virulence Profile
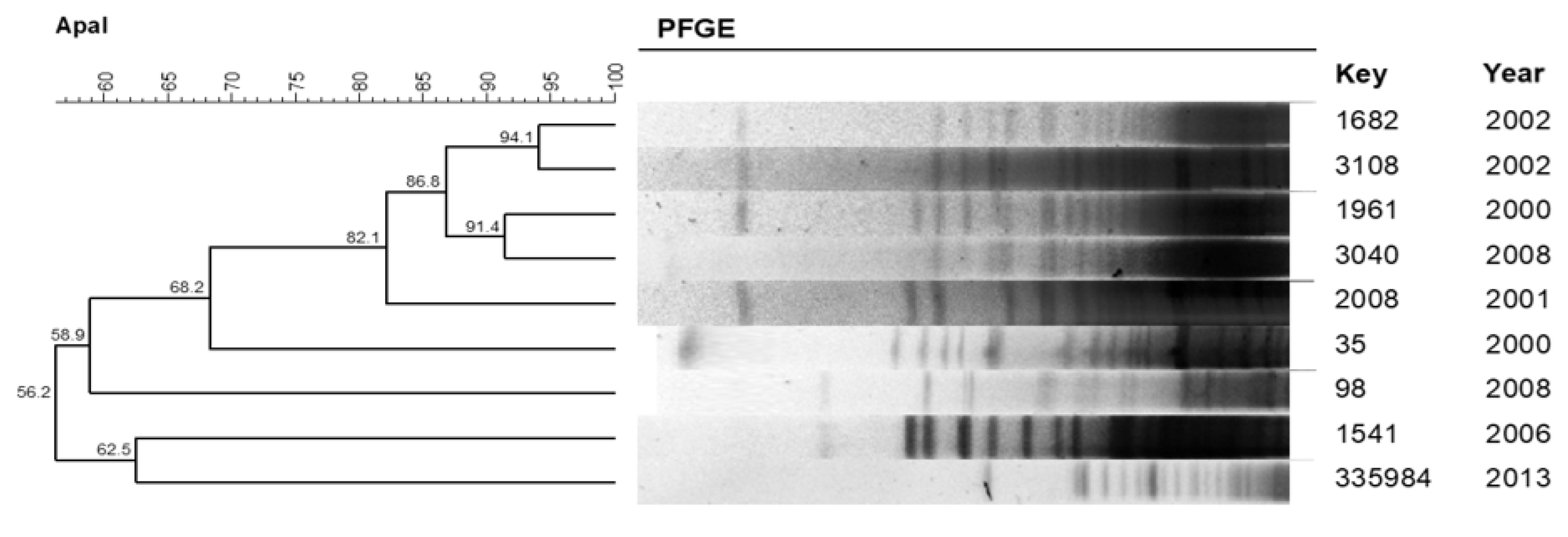
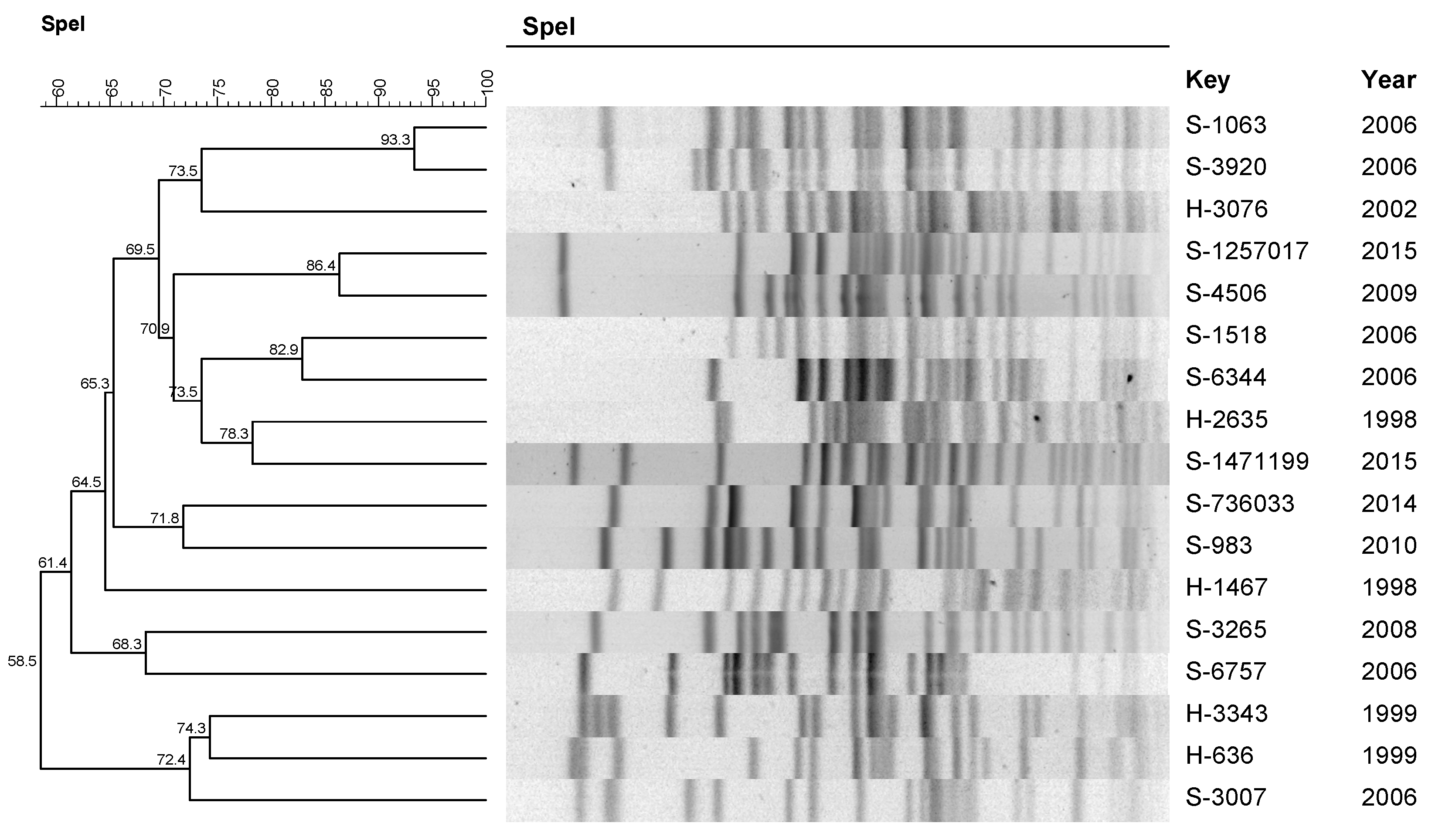
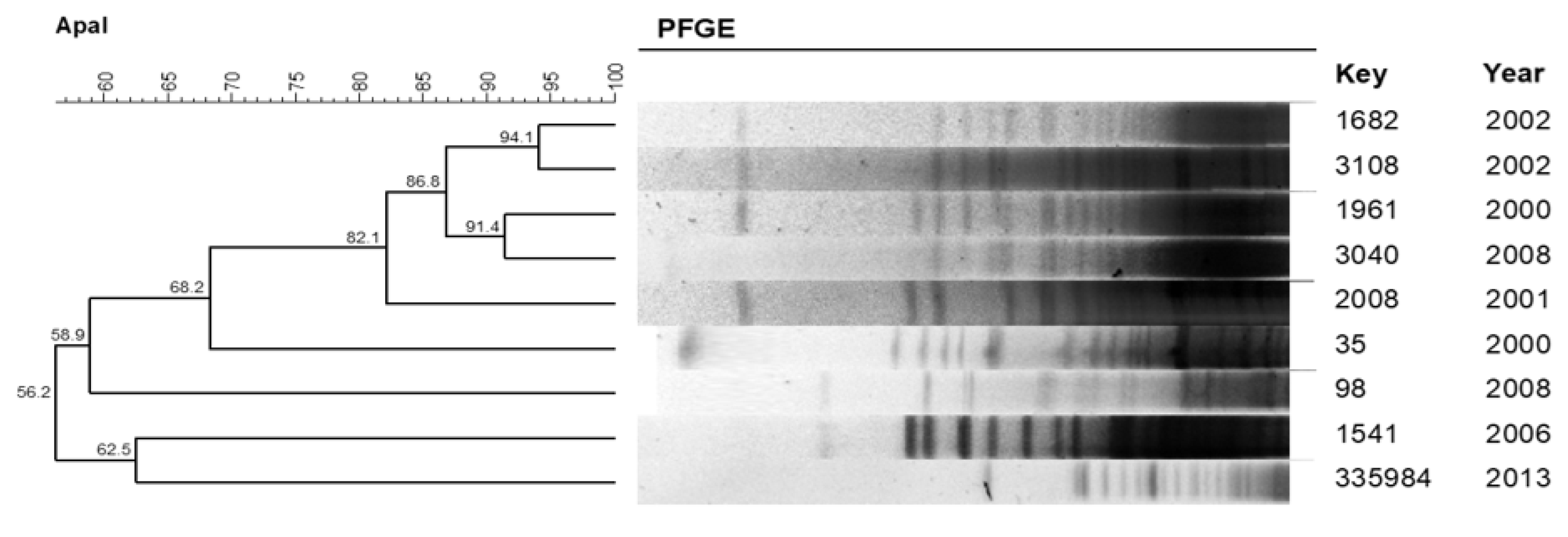
2.5. Clonal Profile
2.6. Peritonitis Outcomes
2.7. Predictors of Peritonitis Outcome—Logistic Regression Analysis
3. Discussion
4. Materials and Methods
4.1. Sampling and Identification
4.2. In Vitro Susceptibility
4.3. Biofilm Production
4.4. Virulence Profile of Pseudomonas aeruginosa
4.5. Clonal Profile
4.6. Clinical-Microbiological Associations
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Piraino, B.; Bernardini, J.; Florio, T.; Fried, L. Staphylococcus aureus prophylaxis and trends in gram-negative infections in peritoneal dialysis patients. Perit. Dial. Int. 2003, 23, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Ozisik, L.; Ozdemir, F.N.; Tanriover, M.D. The changing trends of peritoneal dialysis related peritonitis and novel risk factors. Ren. Fail. 2015, 37, 1027–1032. [Google Scholar] [CrossRef] [PubMed]
- Davenport, A. Peritonitis remains the major clinical complication of peritoneal dialysis: The London, UK, peritonitis audit 2002–2003. Perit. Dial. Int. 2009, 29, 297–302. [Google Scholar] [CrossRef]
- Barretti, P.; Bastos, K.A.; Dominguez, J.; Caramori, J.C. Peritonitis in Latin America. Perit. Dial. Int. 2007, 27, 332–339. [Google Scholar] [CrossRef]
- De Moraes, T.P.; Figueiredo, A.E.; de Campos, L.G.; Olandoski, M.; Barretti, P.; Pecoits-Filho, R. BRAZPD Investigators. Characterization of the BRAZPD II cohort and description of trends in peritoneal dialysis outcome across time periods. Perit. Dial. Int. 2014, 34, 714–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pecoits-Filho, R.; Yabumoto, F.M.; Campos, L.G.; Moraes, T.P.; Figueiredo, A.E.; Olandoski, M.; Shimakura, S.E.; Barretti, P. BRAZPD Investigators. Peritonitis as a risk factor for long-term cardiovascular mortality in peritoneal dialysis patients: The case of a friendly fire? Nephrology 2018, 23, 253–258. [Google Scholar] [CrossRef]
- Li, P.K.; Szeto, C.C.; Piraino, B.; de Arteaga, J.; Fan, S.; Figueiredo, A.E.; Fish, D.N.; Goffin, E.; Kim, Y.L.; Salzer, W.; et al. ISPD Peritonitis Recommendations: 2016 Update on Prevention and Treatment. Perit. Dial. Int. 2018, 36, 481–508, Erratum in Perit. Dial. Int. 2018, 38, 313. [Google Scholar] [CrossRef] [Green Version]
- Barretti, P.; Montelli, A.C.; Batalha, J.E.; Caramori, J.C.; Cunha, M.D.L. The role of virulence factors in the outcome of staphylococcal peritonitis in CAPD patients. BMC Infect. Dis. 2009, 9, 212. [Google Scholar] [CrossRef] [Green Version]
- Troidle, L.; Gorban-Brennan, N.; Kliger, A.; Finkelstein, F. Differing outcomes of gram-positive and gram-negative peritonitis. Am. J. Kidney Dis. 1998, 32, 623–628. [Google Scholar] [CrossRef]
- De Moraes, T.P.; Olandoski, M.; Caramori, J.C.; Martin, L.C.; Fernandes, N.; Divino-Filho, J.C.; Pecoits-Filho, R.; Barretti, P. Novel predictors of peritonitis-related outcomes in the BRAZPD cohort. Perit. Dial. Int. 2014, 34, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siva, B.; Hawley, C.M.; McDonald, S.P.; Brown, F.G.; Rosman, J.B.; Wiggins, K.J.; Bannister, K.M.; Johnson, D.W. Pseudomonas peritonitis in Australia: Predictors, treatment, and outcomes in 191 cases. Clin. J. Am. Soc. Nephrol. 2009, 4, 957–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, W.; Kwan, B.C.; Chow, K.M.; Pang, W.F.; Leung, C.B.; Li, P.K.; Szeto, C.C. Peritoneal dialysis-related peritonitis caused by Pseudomonas species: Insight from a post-millennial case series. PLoS ONE 2018, 13, e0196499. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.; Forster, T.; Mayer, O.; Curtin, J.J.; Lehman, S.M.; Donlan, R.M. Bacteriophage cocktail for the prevention of biofilm formation by Pseudomonas aeruginosa on catheters in an in vitro model system. Antimicrob. Agents Chemother. 2010, 54, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harper, D.R.; Parracho, H.M.R.T.; Walker, J.; Sharp, R.; Hughes, G.; Werthén, M.; Lehman, S.; Morales, S. Bacteriophages and Biofilms. Antibiotics 2014, 3, 270–284. [Google Scholar] [CrossRef]
- Simpson, J.A.; Smith, S.E.; Dean, R.T. Alginate inhibition of the uptake of Pseudomonas aeruginosa by macrophages. J. Gen. Microbiol. 1988, 134, 29–36. [Google Scholar] [CrossRef]
- Wei, Q.; Ma, L.Z. Biofilm matrix and its regulation in Pseudomonas aeruginosa. Int. J. Mol. Sci. 2013, 14, 20983–21005. [Google Scholar] [CrossRef]
- Jyot, J.; Balloy, V.; Jouvion, G.; Verma, A.; Touqui, L.; Huerre, M.; Chignard, M.; Ramphal, R. Type II secretion system of Pseudomonas aeruginosa: In vivo evidence of a significant role in death due to lung infection. J. Infect. Dis. 2011, 203, 1369–1377. [Google Scholar] [CrossRef] [Green Version]
- Badamchi, A.; Masoumi, H.; Javadinia, S.; Asgarian, R.; Tabatabaee, A. Molecular detection of six virulence genes in Pseudomonas aeruginosa isolates detected in children with urinary tract infection. Microb. Pathog. 2017, 107, 44–47. [Google Scholar] [CrossRef]
- Dos Santos, A.C.M.L.; Hernandes, R.T.; Montelli, A.C.; Monteiro, A.C.M.; Barbosa, T.A.; Camargo, C.H.; Ferreira, A.M.; Mondelli, A.L.; da Cunha, M.D.L.R.D.S.; Barretti, P. Clinical and microbiological factors predicting outcomes of nonfermenting gram-negative bacilli peritonitis in peritoneal dialysis. Sci. Rep. 2021, 11, 12248. [Google Scholar] [CrossRef]
- Keane, W.F.; Alexander, S.R.; Bailie, G.R.; Boeschoten, E.; Gokal, R.; Golper, T.A.; Holmes, C.J.; Huang, C.C.; Kawaguchi, Y.; Piraino, B.; et al. Peritoneal dialysis-related peritonitis treatment recommendations: 1996 update. Perit. Dial. Int. 1996, 16, 557–573. [Google Scholar] [CrossRef]
- Keane, W.F.; Bailie, G.R.; Boeschoten, E.; Gokal, R.; Golper, T.A.; Holmes, C.J.; Kawaguchi, Y.; Piraino, B.; Riella, M.; Vas, S. International Society for Peritoneal Dialysis. Adult peritoneal dialysis-related peritonitis treatment recommendations: 2000 update. Perit. Dial. Int. 2000, 20, 396–411, Erratum in Perit. Dial. Int. 2000, 20, 828–829. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, M.; Thodis, E.; Ikonomopoulos, D.; Vidgen, E.; Chu, M.; Bargman, J.M.; Vas, S.I.; Oreopoulos, D.G. Predictor of outcome following bacterial peritonitis in peritoneal dialysis. Perit. Dial. Int. 2002, 22, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Stinghen, A.E.; Barretti, P.; Pecoits-Filho, R. Factors contributing to the differences in peritonitis rates between centers and regions. Perit. Dial. Int. 2007, 27, 281–285. [Google Scholar] [CrossRef]
- Prasad, K.N.; Singh, K.; Rizwan, A.; Mishra, P.; Tiwari, D.; Prasad, N.; Gupta, A. Microbiology and outcomes of peritonitis in northern India. Perit. Dial. Int. 2014, 34, 188–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernardini, J.; Piraino, B.; Sorkin, M. Analysis of continuous ambulatory peritoneal dialysis-related Pseudomonas aeruginosa infections. Am. J. Med. 1987, 83, 829–832. [Google Scholar] [CrossRef]
- Lanotte, P.; Watt, S.; Mereghetti, L.; Dartiguelongue, N.; Rastegar-Lari, A.; Goudeau, A.; Quentin, R. Genetic features of Pseudomonas aeruginosa isolates from cystic fibrosis patients compared with those of isolates from other origins. J. Med. Microbiol. 2004, 53, 73–81. [Google Scholar] [CrossRef]
- Gonçalves, I.R.; Dantas, R.C.C.; Ferreira, M.L.; Batistão, D.W.D.F.; Gontijo-Filho, P.P.; Ribas, R.M. Carbapenem-resistant Pseudomonas aeruginosa: Association with virulence genes and biofilm formation. Braz. J. Microbiol. 2017, 48, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Martins, V.V.; Pitondo-Silva, A.; Manço, L.D.M.; Falcão, J.P.; Freitas, S.D.S.; da Silveira, W.D.; Stehling, E.G. Pathogenic potential and genetic diversity of environmental and clinical isolates of Pseudomonas aeruginosa. APMIS 2014, 122, 92–100. [Google Scholar] [CrossRef]
- Juan, C.; Peña, C.; Oliver, A. Host and Pathogen Biomarkers for Severe Pseudomonas aeruginosa Infections. J. Infect. Dis. 2017, 215 (Suppl. 1), S44–S51. [Google Scholar] [CrossRef]
- Taylor, P.K.; Yeung, A.T.; Hancock, R.E. Antibiotic resistance in Pseudomonas aeruginosa biofilms: Towards the development of novel anti-biofilm therapies. J. Biotechnol. 2014, 191, 121–130. [Google Scholar] [CrossRef]
- Martins, M.; Rodrigues, A.; Pedrosa, J.M.; Carvalho, M.J.; Cabrita, A.; Oliveira, R. Update on the challenging role of biofilms in peritoneal dialysis. Biofouling 2013, 29, 1015–1027. [Google Scholar] [CrossRef] [PubMed]
- Dijkshoorn, L.; Nemec, A.; Seifert, H. An increasing threat in hospitals: Multidrug-resistant Acinetobacter baumannii. Nat. Rev. Microbiol. 2007, 5, 939–951. [Google Scholar] [CrossRef] [PubMed]
- Visca, P.; Seifert, H.; Towner, K.J. Acinetobacter infection—An emerging threat to human health. IUBMB Life 2011, 63, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Li, P.H.; Cheng, V.C.; Yip, T.; Yap, D.Y.; Lui, S.L.; Lo, W.K. Epidemiology and Clinical Characteristics of Acinetobacter Peritoneal Dialysis-Related Peritonitis in Hong Kong-With a Perspective on Multi-Drug and Carbapenem Resistance. Perit. Dial. Int. 2017, 37, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Lee, S.Y.; Yang, W.S.; Chen, H.W.; Fang, C.C.; Yen, C.J.; Chiang, C.K.; Hung, K.Y.; Huang, J.W. Acinetobacter peritoneal dialysis peritonitis: A changing landscape over time. PLoS ONE 2014, 9, e110315. [Google Scholar] [CrossRef] [PubMed]
- Dubois, D.; Grare, M.; Prere, M.F.; Segonds, C.; Marty, N.; Oswald, E. Performances of the Vitek MS matrix-assisted laser desorption ionization-time of flight mass spectrometry system for rapid identification of bacteria in routine clinical microbiology. J. Clin. Microbiol. 2012, 50, 2568–2576. [Google Scholar] [CrossRef] [Green Version]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing. In CLSI Supplement M100S, 29th ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- Stepanovic, S.; Vukovic, D.; Dakic, I.; Savic, B.; Svabic-Vlahovic, M. A modified microtiter-plate test for quantification of staphylococcal biofilm formation. J. Microbiol. Methods 2000, 40, 175–179. [Google Scholar] [CrossRef]
- Durmaz, R.; Otlu, B.; Koksal, F.; Hosoglu, S.; Ozturk, R.; Ersoy, Y.; Aktas, E.; Gursoy, N.C.; Caliskan, A. The optimization of a rapid pulsed-field gel electrophoresis protocol for the typing of Acinetobacter baumannii, Escherichia coli and Klebsiella spp. Jpn. J. Infect. Dis. 2009, 62, 372–377. [Google Scholar]


{kind=link}
{kind=link}
| Patient Data | |||||
|---|---|---|---|---|---|
| Sample Number | Species | Year of Isolation | Age (Years) | Gender | Dialysis * |
| H 1196 | Acinetobacter ursingii | 1997 | 46 | M | CAPD |
| H 829 | Pseudomonas aeruginosa | 1998 | 14 | M | CAPD |
| H 1467 | Pseudomonas aeruginosa | 1998 | 24 | M | CAPD |
| H 2635 | Pseudomonas aeruginosa | 1998 | 54 | F | CAPD |
| H 167 | Pseudomonas aeruginosa | 1999 | 51 | F | CAPD |
| H 636 | Pseudomonas aeruginosa | 1999 | 9 | M | CAPD |
| H 2624 | Pseudomonas aeruginosa | 1999 | 73 | F | CAPD |
| H 3343 | Pseudomonas aeruginosa | 1999 | 6 | M | CAPD |
| H 3379 | Acinetobacter haemolyticus | 1999 | 29 | F | CAPD |
| H 35 | Acinetobacter baumannii | 2000 | 65 | F | DPA |
| H 1961 | Acinetobacter baumannii | 2000 | 40 | M | CAPD |
| H 2008 | Acinetobacter baumannii | 2001 | 69 | M | CAPD |
| H 1682 | Acinetobacter baumannii | 2002 | 81 | F | DPA |
| H 2337 | Burkholderia gladioli | 2002 | 74 | M | CAPD |
| H 3076 | Pseudomonas aeruginosa | 2002 | 43 | M | CAPD |
| H 3108 | Acinetobacter baumannii | 2002 | 66 | M | CAPD |
| S 22813 | Acinetobacter haemolyticus | 2003 | 52 | M | DPA |
| S 23517 | Pseudomonas aeruginosa | 2003 | 21 | F | DPA |
| S 22270 | Acinetobacter ursingii | 2004 | 49 | F | CAPD |
| S 20514 | Pseudomonas pútida | 2005 | 44 | M | CAPD |
| S 1045 | Achromobacter denitrificans | 2006 | 56 | F | DPA |
| S 1063 | Pseudomonas aeruginosa | 2006 | 42 | F | DPA |
| S 1518 | Pseudomonas aeruginosa | 2006 | 62 | M | CAPD |
| S 1541 | Acinetobacter baumannii | 2006 | 54 | M | DPA |
| S 3007 | Pseudomonas aeruginosa | 2006 | 35 | M | CAPD |
| S 3920 | Pseudomonas aeruginosa | 2006 | 65 | M | CAPD |
| S 6344 | Pseudomonas aeruginosa | 2006 | 2 | F | DPA |
| S 6430 | Pseudomonas aeruginosa | 2006 | 46 | M | DPA |
| S 6757 | Pseudomonas aeruginosa | 2006 | 33 | F | DPA |
| S 7122 | Acinetobacter haemolyticus | 2006 | 35 | F | DPA |
| S 2797 | Achromobacter denitrificans | 2007 | 24 | M | DPA |
| S 3620 | Acinetobacter baumannii | 2007 | 61 | M | CAPD |
| S 4411 | Pseudomonas putida | 2007 | 54 | M | CAPD |
| S 5215 | Burkholderia cepacia | 2007 | 53 | M | DPA |
| S 98 | Acinetobacter baumannii | 2008 | 91 | F | CAPD |
| S 3040 | Acinetobacter baumannii | 2008 | 32 | F | DPA |
| S 3265 | Pseudomonas aeruginosa | 2008 | 78 | F | DPA |
| S 4661 | Achromobacter denitrificans | 2008 | 22 | F | DPA |
| s 4845 | Acinetobacter haemolyticus | 2008 | 26 | M | CAPD |
| S 500 | Acinetobacter haemolyticus | 2009 | 27 | M | DPA |
| S 4506 | Pseudomonas aeruginosa | 2009 | 36 | M | CAPD |
| S 56765 | Stenotrophomonas maltophilia | 2009 | 42 | M | DPA |
| S 983 | Pseudomonas aeruginosa | 2010 | 54 | M | DPA |
| S 1489 | Acinetobacter baumannii | 2010 | 46 | F | DPA |
| S 335984 | Acinetobacter baumannii | 2013 | 66 | F | DPA |
| S 736033 | Pseudomonas aeruginosa | 2014 | 15 | F | DPA |
| S 1257017 | Pseudomonas aeruginosa | 2015 | 30 | F | DPA |
| S 1471199 | Pseudomonas aeruginosa | 2015 | 64 | M | DPA |
| Pseudomonas spp. (n = 24) | Acinetobacter spp. (n = 18) | Achromobacter spp. (n = 3) | B. gladioli (n = 1) | B. cepacia (n = 1) | Stenotrophomonas spp. (n = 1) | NF-GNB (n = 48) | |
|---|---|---|---|---|---|---|---|
| Susceptibility n (%) | Susceptibility n (%) | Susceptibility n (%) | Susceptibility n (%) | Susceptibility n (%) | Susceptibility n (%) | Susceptibility n (%) | |
| Amikacin | 20 (83.3) 1,2 | 7 (38.9) | 1 (33.3) | 1 (100) | - | - | 29 (60.4) |
| Ciprofloxacin | 17 (70.1) 1 | 7 (38.9) | 2 (66.7) | 0 (0.0) | - | - | 26 (54.1) |
| Ceftazidime | 21 (87.3) 1 | 8 (44.4) | 3 (100) | 0 (0.0) | 1 (100.0) | 1 (100.0) | 34 (70.8) |
| Cefepime | 20 (83.3) 1,2 | 7 (38.9) | 1 (33.3) | 0 (0.0) | - | - | 27 (56.2) |
| Imipenem | 20 (83.3) | 16 (88.9) | 3 (100) | 0 (0.0) | - | - | 39 (81.2) |
| Cluster | Similarity | Sample | Year | Antimicrobial Profile * | Biofilm Production | Virulence Genes ** | |
|---|---|---|---|---|---|---|---|
| Sensibility | Resistance | ||||||
| A | 93.3% | S-1063 | 2006 | IPM | AMI, CAZ, COM and CIP | Strong producer | algD, exoS, plcH, plcN, toxA, aprA, lasB, e rhlAB |
| S-3920 | 2006 | - | AMI, CAZ, CPM, CIP and IPM | Strong producer | |||
| B | 86.4% | S-4506 | 2009 | AMI, CAZ, CPM, CIP and IPM | - | Strong producer | algD, exoS, plcH, plcN, toxA, aprA, lasB, e rhlAB |
| S-1257017 | 2015 | AMI, CAZ, CPM, CIP and IPM | - | Moderate producer | |||
| C | 82.9% | S-1518 | 2006 | AMI, CAZ and CPM | CIP and IPM | Moderate producer | algD, plcH, plcN, toxA, aprA, lasB, e rhlAB |
| S-6344 | 2006 | CAZ, CPM and IPM | CIP and AMI | Moderate producer | |||
| Cluster | Similarity | Sample | Year | Antimicrobial Profile * | Biofilm Production | |
|---|---|---|---|---|---|---|
| Sensibility | Resistance | |||||
| A | 82.1% | S-1961 | 2000 | IPM | AMI, CAZ, CPM, and CIP | Weak producer |
| S-2008 | 2001 | IPM | AMI, CAZ, CPM, and CIP | Weak producer | ||
| S-1682 | 2002 | IPM | AMI, CAZ, CPM, and CIP | No producer | ||
| S-3108 | 2002 | IPM and CPM | AMI, CAZ, and CIP | Weak producer | ||
| S-3040 | 2008 | IPM and CPM | AMI, CAZ, and CIP | No producer | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moro Lima dos Santos, A.C.; Monteiro, A.C.M.; Barbosa, T.A.; Riboli, D.F.M.; Camargo, C.H.; Ferreira, A.M.; Mondelli, A.L.; Montelli, A.C.; Hernandes, R.T.; Ribeiro de Souza da Cunha, M.d.L.; et al. Phenotypic and Molecular Characterization of Nonfermenting Gram-Negative Bacilli Causing Peritonitis in Peritoneal Dialysis Patients. Pathogens 2022, 11, 218. https://doi.org/10.3390/pathogens11020218
Moro Lima dos Santos AC, Monteiro ACM, Barbosa TA, Riboli DFM, Camargo CH, Ferreira AM, Mondelli AL, Montelli AC, Hernandes RT, Ribeiro de Souza da Cunha MdL, et al. Phenotypic and Molecular Characterization of Nonfermenting Gram-Negative Bacilli Causing Peritonitis in Peritoneal Dialysis Patients. Pathogens. 2022; 11(2):218. https://doi.org/10.3390/pathogens11020218
Chicago/Turabian StyleMoro Lima dos Santos, Ana Cláudia, Aydir Cecília Marinho Monteiro, Thaís Alves Barbosa, Danilo Flávio Moraes Riboli, Carlos Henrique Camargo, Adriano Martison Ferreira, Alessandro Lia Mondelli, Augusto Cezar Montelli, Rodrigo Tavanelli Hernandes, Maria de Lourdes Ribeiro de Souza da Cunha, and et al. 2022. "Phenotypic and Molecular Characterization of Nonfermenting Gram-Negative Bacilli Causing Peritonitis in Peritoneal Dialysis Patients" Pathogens 11, no. 2: 218. https://doi.org/10.3390/pathogens11020218
APA StyleMoro Lima dos Santos, A. C., Monteiro, A. C. M., Barbosa, T. A., Riboli, D. F. M., Camargo, C. H., Ferreira, A. M., Mondelli, A. L., Montelli, A. C., Hernandes, R. T., Ribeiro de Souza da Cunha, M. d. L., & Barretti, P. (2022). Phenotypic and Molecular Characterization of Nonfermenting Gram-Negative Bacilli Causing Peritonitis in Peritoneal Dialysis Patients. Pathogens, 11(2), 218. https://doi.org/10.3390/pathogens11020218