
Study of the Plasma and Buffy Coat in Patients with SARS-CoV-2 Infection—A Preliminary Report

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinical Findings
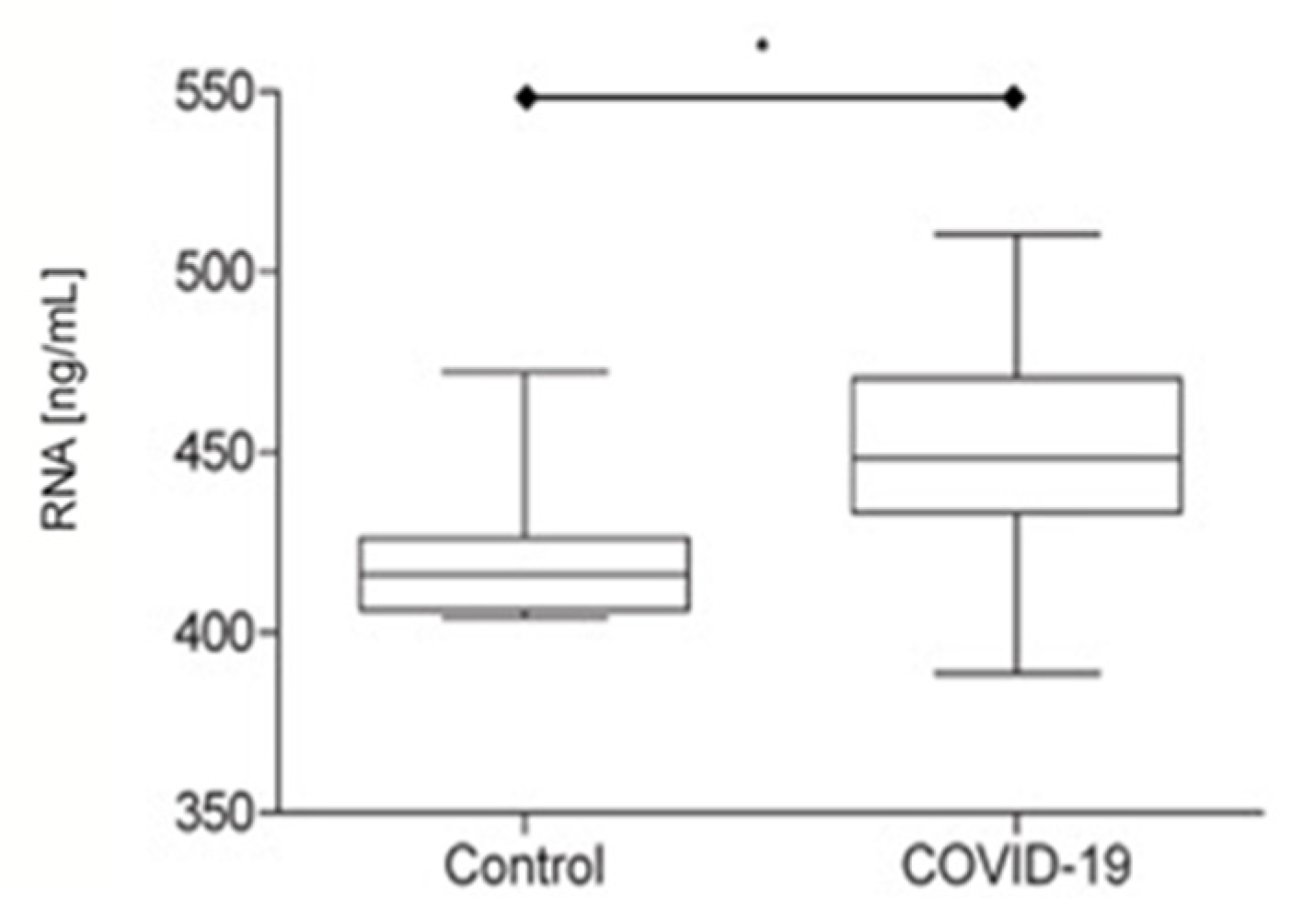
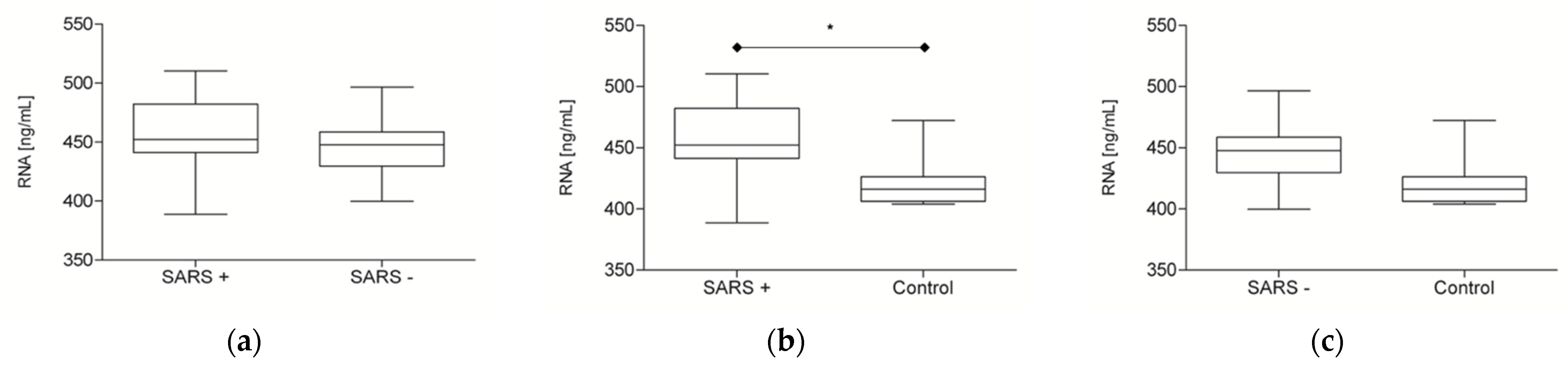
2.2. RNA Plasma Findings
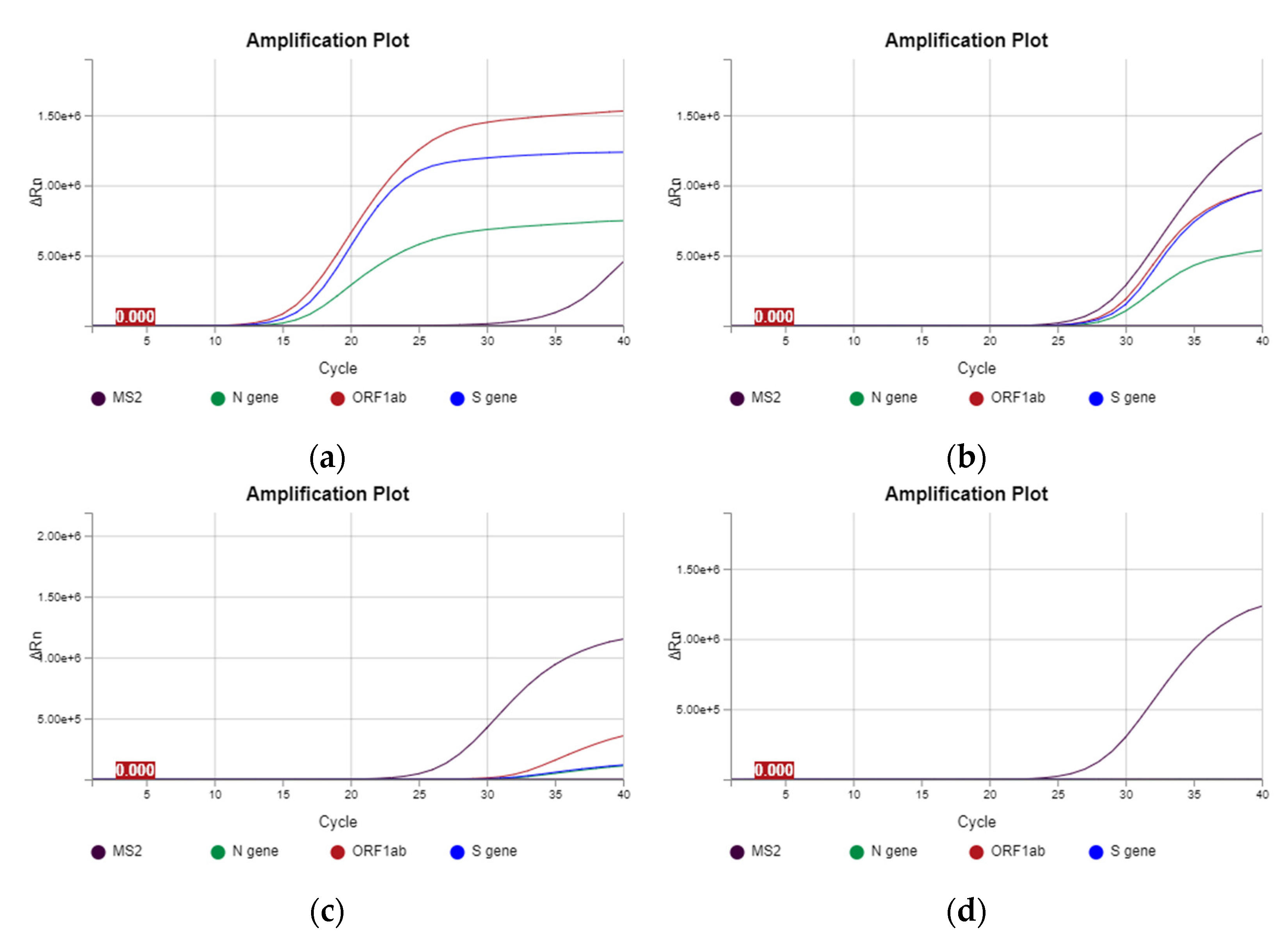
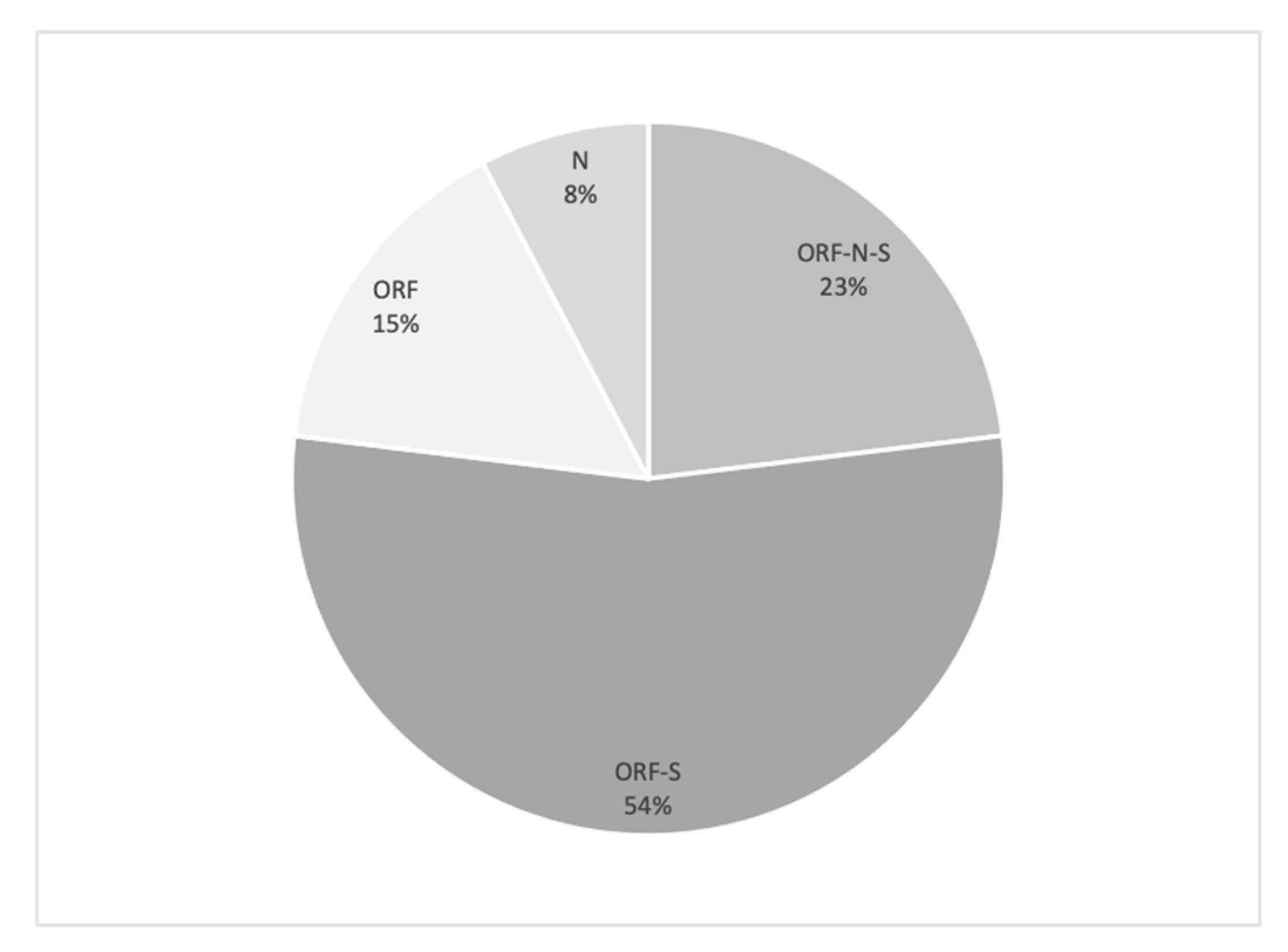
2.3. RNA Buffy Coat Findings
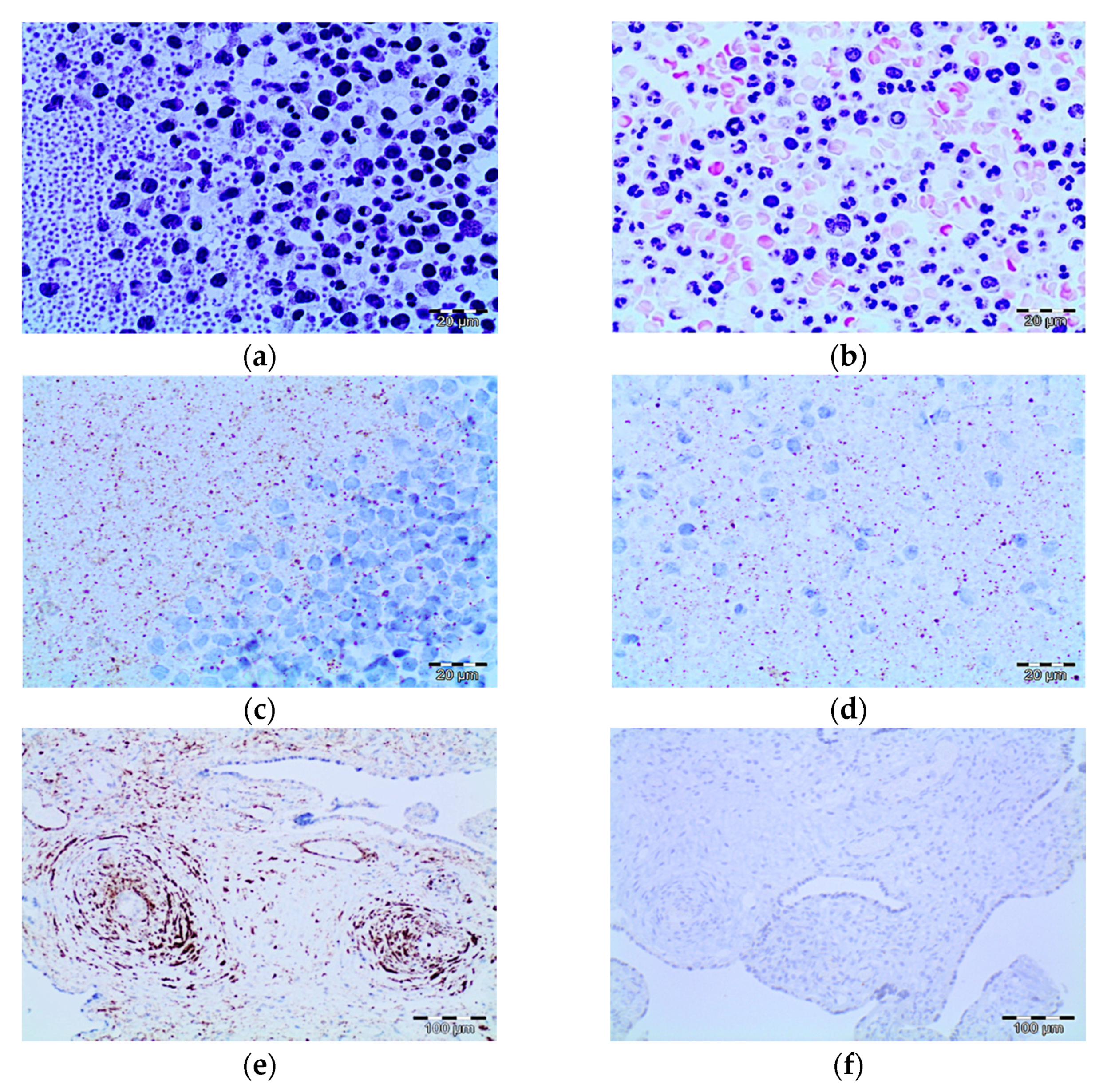
2.4. Morphological and Immunohistochemical Buffy Coat Findings
2.4.1. Morphological Study
2.4.2. Immunohistochemical Study
3. Discussion
4. Materials and Methods
4.1. Study Design and Patient Cohort
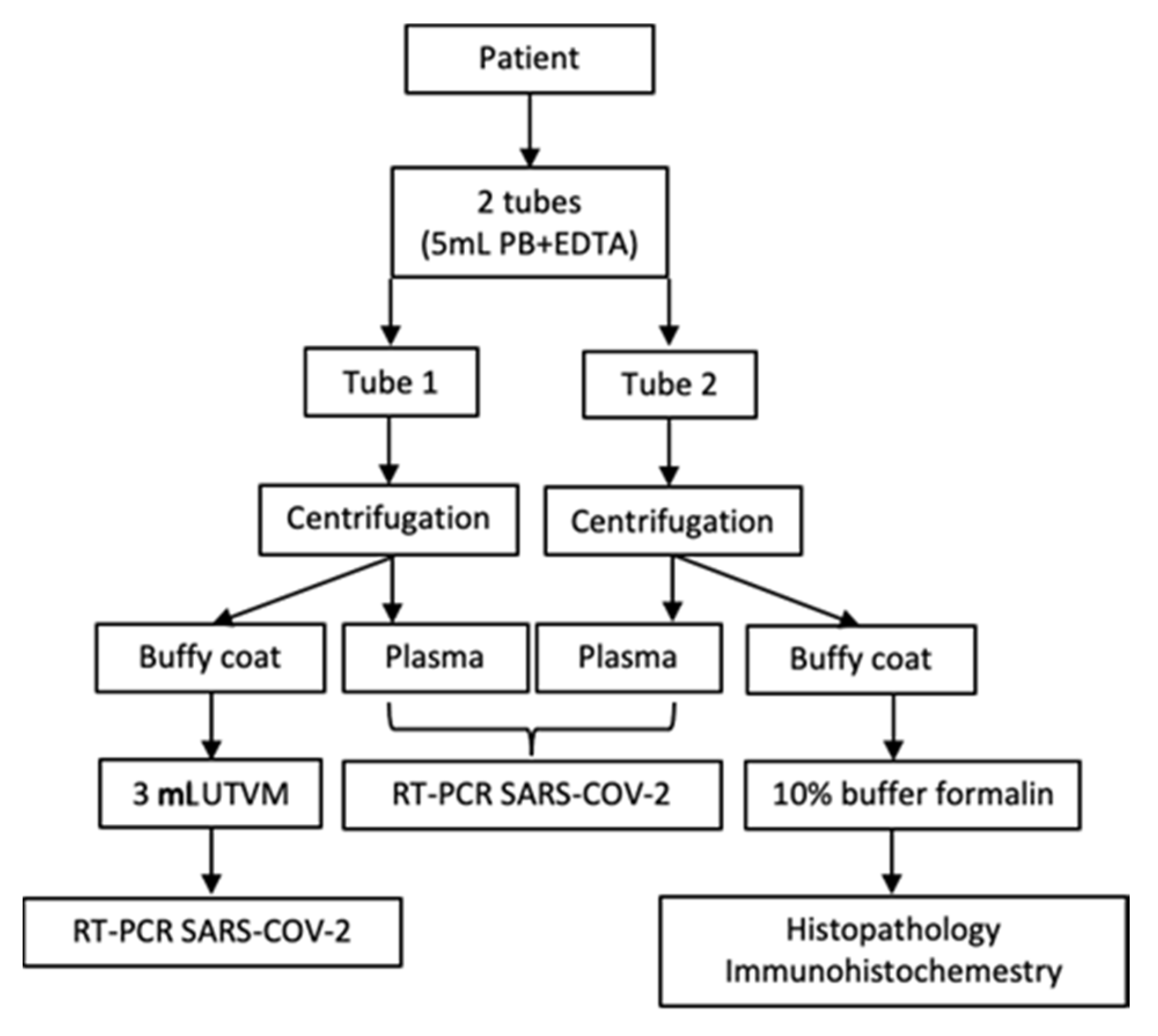
4.2. Blood Samples
4.3. RNA Plasma Extraction
4.4. RNA Buffy Coat Extraction
4.5. Histopathological Preparation of the Buffy Coat
4.6. Immunohistochemistry Study of the Buffy Coat
4.7. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Sun, P.; Lu, X.; Xu, C.; Sun, W.; Pan, B. Understanding of COVID-19 based on current evidence. J. Med. Virol. 2020, 92, 548–551. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2020, 6, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.Z.; Holmes, E.C. A Genomic Perspective on the Origin and Emergence of SARS-CoV-2. Cell 2020, 181, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Liu, J.; Xu, W.; Luo, Q.; Chen, D.; Lei, Z.; Huang, Z.; Li, X.; Deng, K.; Lin, B.; et al. SARS-CoV-2 can be detected in urine, blood, anal swabs, and oropharyngeal swabs specimens. J. Med. Virol. 2020, 92, 1676–1680. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Zhao, B.; Qu, Y.; Chen, Y.; Xiong, J.; Feng, Y.; Men, D.; Huang, Q.; Liu, Y.; Yang, B.; et al. Detectable Serum Severe Acute Respiratory Syndrome Coronavirus 2 Viral Load (RNAemia) Is Closely Correlated with Drastically Elevated Interleukin 6 Level in Critically Ill Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 5, 1937–1942. [Google Scholar] [CrossRef]
- Zhang, W.; Du, R.H.; Li, B.; Zheng, X.S.; Yang, X.L.; Hu, B.; Wang, Y.Y.; Xiao, G.F.; Yan, B.; Shi, Z.L. Molecular and serological investigation of 2019-nCoV infected patients: Implication of multiple shedding routes. Emerg. Microbes Infect. 2020, 9, 386–389. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Lan, Y.; Yuan, X.; Deng, X.; Li, Y.; Cai, X.; Li, L.; He, R.; Tan, Y.; Deng, X.; et al. DetecTable 2019-nCoV viral RNA in blood is a strong indicator for the further clinical severity. Emerg. Microbes Infect. 2020, 9, 469–473. [Google Scholar] [CrossRef] [Green Version]
- Hogan, C.A.; Stevens, B.A.; Sahoo, M.K.; Huang, C.; Garamani, N.; Gombar, S.; Yamamoto, F.; Murugesan, K.; Kurzer, J.; Zehnder, J.; et al. High Frequency of SARS-CoV-2 RNAemia and Association with Severe Disease. Clin. Infect. Dis. 2020, ciaa1054. [Google Scholar] [CrossRef] [PubMed]
- Hagman, K.; Hedenstierna, M.; Gille-Johnson, P.; Hammas, B.; Grabbe, M.; Dillner, J.; Ursing, J. SARS-CoV-2 RNA in serum as predictor of severe outcome in COVID-19: A retrospective cohort study. Clin. Infect. Dis. 2020, ciaa1285. [Google Scholar] [CrossRef]
- Eberhardt, K.A.; Meyer-Schwickerath, C.; Heger, E.; Knops, E.; Lehmann, C.; Rybniker, J.; Schommers, P.; Eichenauer, D.A.; Kurth, F.; Ramharter, M.; et al. RNAemia Corresponds to Disease Severity and Antibody Response in Hospitalized COVID-19 Patients. Viruses 2020, 12, 1045. [Google Scholar] [CrossRef]
- Veyer, D.; Kernéis, S.; Poulet, G.; Wack, M.; Robillard, N.; Taly, V.; L’Honneur, A.S.; Rozenberg, F.; Laurent-Puig, P.; Bélec, L.; et al. Highly sensitive quantification of plasma SARS-CoV-2 RNA shelds light on its potential clinical value. Clin. Infect. Dis. 2020, ciaa1196. [Google Scholar] [CrossRef]
- Colagrossi, L.; Antonello, M.; Renica, S.; Merli, M.; Matarazzo, E.; Travi, G.; Vecchi, M.; Colombo, J.; Muscatello, A.; Grasselli, G.; et al. SARS-CoV-2 RNA in plasma samples of COVID-19 affected individuals: A cross-sectional proof-of-concept study. BMC Infect. Dis. 2021, 21, 184. [Google Scholar] [CrossRef]
- Azghandi, M.; Kerachian, M.A. Detection of novel coronavirus (SARS-CoV-2) RNA in peripheral blood specimens. J. Transl. Med. 2020, 18, 412. [Google Scholar] [CrossRef]
- Huang, Z.; Ning, B.; Yang, H.S.; Youngquist, B.M.; Niu, A.; Lyon, C.J.; Beddingfield, B.J.; Fears, A.C.; Monk, C.H.; Murrell, A.E.; et al. Sensitive tracking of circulating viral RNA through all stages of SARS-CoV-2 infection. J. Clin. Investig. 2021, 131, e146031. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wo, J.; Shao, J.; Zhu, H.; Wu, N.; Li, M.; Yao, H.; Hu, M.; Dennin, R.H. SARS-coronavirus replicates in mononuclear cells of peripheral blood (PBMCs) from SARS patients. J. Clin. Virol. 2003, 28, 239–244. [Google Scholar] [CrossRef]
- Yilla, M.; Harcourt, B.H.; Hickman, C.J.; McGrew, M.; Tamin, A.; Goldsmith, C.S.; Bellini, W.J.; Anderson, L.J. SARS-coronavirus replication in human peripheral monocytes/macrophages. Virus Res. 2005, 107, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Zini, G.; Bellesi, S.; Ramundo, F.; d’Onofrio, G. Morphological anomalies of circulating blood cells in COVID-19. Am. J. Hematol. 2020, 95, 870–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzaid, F.; Julla, J.B.; Diedisheim, M.; Potier, C.; Potier, L.; Velho, G.; Gaborit, B.; Manivet, P.; Germain, S.; Vidal-Trecan, T.; et al. Monocytopenia, monocyte morphological anomalies and hyperinflammation characterise severe COVID-19 in type 2 diabetes. EMBO Mol. Med. 2020, 12, e13038. [Google Scholar] [CrossRef] [PubMed]
- Kaur, G.; Sandeep, F.; Olayinka, O.; Gupta, G. Morphologic Changes in Circulating Blood Cells of COVID-19 Patients. Cureus 2021, 13, e13416. [Google Scholar] [CrossRef] [PubMed]
- Harris, C.K.; Hung, Y.P.; Nielsen, G.P.; Stone, J.R.; Ferry, J.A. Bone Marrow and Peripheral Blood Findings in Patients Infected by SARS-CoV-2. Am. J. Clin. Pathol. 2021, 155, 627–637. [Google Scholar] [CrossRef]
- Pozdnyakova, O.; Connell, N.T.; Battinelli, E.M.; Connors, J.M.; Fell, G.; Kim, A.S. Clinical Significance of CBC and WBC Morphology in the Diagnosis and Clinical Course of COVID-19 Infection. Am. J. Clin. Pathol. 2021, 155, 364–375. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | N | % |
|---|---|---|
| Male | 18 | 75 |
| Female | 6 | 25 |
| Symptoms | 22 | 91.67 |
| Dry cough | 21 | 95.45 |
| Fever | 21 | 95.45 |
| Dyspnea | 20 | 90.91 |
| Odynophagia | 15 | 68.18 |
| Anosmia | 6 | 68.18 |
| GI symptoms | 1 | 4.55 |
| Asymptomatic | 2 | 8.33 |
| Intensive care unit | ||
| Required | 13 | 54.17 |
| Not required | 11 | 45.83 |
| Lived | 16 | 66.67 |
| Died | 8 | 33.33 |
| Patient | Gender | Age (Years) | Comorbidities | Symptoms | SARS-CoV-2 ** | Initial O2 Sat. (%) | C-Reactive Protein (mg/dL) | X-ray Diagnostic (Lung) | Evolution |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Male | 69 | DLP, CRCa | Cough, Fever, Dyspnea | Positive | 91 | 12.78 | Bilateral basal condensation | Live |
| 2 | Female | 77 | SAH | Cough, Fever, Dyspnea | Positive | 95 | 22.2 | Left basal condensation | Died |
| 3 | Male | 51 | Hyperglycemia | Fever, Dyspnea | Positive | 94 | 17.6 | Bilateral basal condensation | Live |
| 4 | Male | 54 | SAH, T2DM, DLP | Cough, Fever | Positive | 95 | 15.7 | Bilateral alveolar infiltrates | Live |
| 5 | Female | 58 | BRCa | Cough, Fever, Dyspnea | Positive | 90 | 30 | Bilateral peripheral infiltrates | Live |
| 6 | Female | 54 | Hypothyroidism | Cough, Fever, Dyspnea | Positive | 87 | 14.72 | Bilateral interstitial infiltrates | Live |
| 7 | Male | 72 | SAH, T2DM, DLP | Cough, Dyspnea | Positive | 95 | 28 | Bilateral interstitial infiltrates | Died |
| 8 | Male | 78 | SAH | Cough, Fever, Dyspnea | Positive | 93 | 4.85 | Bilateral interstitial infiltrates | Died |
| 9 | Male | 63 | T2DM | Fever, Dyspnea | Positive | 70 | 11 | Bilateral basal condensation | Live |
| 10 | Female | 73 | SAH, DLP | Cough, Fever, Dyspnea | Positive | 98 | NR | Bilateral interstitial infiltrates | Live |
| 11 | Male | 62 | SAH, T2DM, DLP | Fever, Dyspnea | Positive | 85 | 22 | Bilateral interstitial infiltrates | Died |
| 12 | Male | 62 | SAH, T2DM, CRI | Cough, Fever, Dyspnea | Positive | 90 | 18.7 | Bilateral interstitial infiltrates | Died |
| 13 | Male | 57 | SAH, DLP | Cough, Dyspnea | Positive | 65.8 | 13 | Bilateral interstitial infiltrates | Live |
| 14 | Male | 69 | SAH, DLP | Cough, Dyspnea | Positive | 65 | 16 | Bilateral basal condensation | Live |
| 15 | Male | 61 | No | Cough, Fever, Dyspnea | Positive | 75 | 25 | Bilateral basal condensation | Live |
| 16 | Male | 54 | DLP | Cough, Fever, Dyspnea | Positive | 92 | 6.31 | Bilateral interstitial infiltrates | Live |
| 17 | Male | 69 | No | Cough, Fever, Dyspnea | Positive | 90 | 14.3 | Bilateral basal condensation | Live |
| 18 | Female | 76 | CRI | Diarrhea | Positive | 97 | 10 | Right basal condensation | Died |
| 19 | Male | 82 | SAH, DLP | Cough, Dyspnea | Positive | 88 | 4.2 | Bilateral interstitial infiltrates | Died |
| 20 | Female | 63 | SAH, T2DM, DLP | Cough, Fever, Dyspnea | Positive | 90 | 16.93 | Bilateral basal condensation | Live |
| 21 | Male | 53 | SAH, DLP | Asymptomatic | Positive | 98 | NR | No infiltrates. No consolidations | Live |
| 22 | Male | 54 | SAH, Obesity | Asymptomatic | Positive | 98 | NR | No infiltrates. No consolidations | Live |
| 23 | Male | 51 | DLP | Cough, Fever, Dyspnea | Positive | 94 | 13 | Bilateral interstitial infiltrates | Live |
| 24 | Male | 77 | SHA, DLP | Cough, Fever, Dyspnea | Positive | 88 | 6.14 | Bilateral basal condensation | Died |
| Control | |||||||||
| 1 | Male | 72 | CRCa | Asymptomatic | Negative | - | - | - | Live |
| 2 | Male | 52 | LCa | Asymptomatic | Negative | - | - | - | Live |
| 3 | Male | 51 | LCa | Asymptomatic | Negative | - | - | - | Live |
| 4 | Female | 62 | CRCa | Asymptomatic | Negative | - | - | - | Live |
| 5 | Female | 62 | LCa | Asymptomatic | Negative | - | - | - | Live |
| 6 | Male | 75 | CRCa | Asymptomatic | Negative | - | - | - | Live |
| 7 | Female | 64 | CRCa | Asymptomatic | Negative | - | - | - | Live |
| 8 | Female | 68 | LCa | Asymptomatic | Negative | - | - | - | Live |
| Case | Age | Sex | Gene Plasma | Gene Buffy Coat | Evolution |
|---|---|---|---|---|---|
| 2 | 77 | F | ORF, S, N | ORF, N | Died |
| 4 | 54 | M | N | N | Live |
| 5 | 58 | F | ORF, S | Negative | Live |
| 6 | 54 | F | ORF, N, S | N, S | Live |
| 7 | 72 | M | ORF | Negative | Died |
| 8 | 78 | M | ORF, S | Negative | Died |
| 9 | 63 | M | ORF, S | Negative | Live |
| 13 | 57 | M | ORF, S | Negative | Live |
| 14 | 69 | M | ORF, S | Negative | Live |
| 17 | 69 | M | ORF, N, S | ORF, N | Live |
| 18 | 76 | F | ORF | Negative | Died |
| 19 | 82 | M | ORF, S | Negative | Live |
| 23 | 77 | M | ORF, S | Negative | Died |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña, K.B.; Riu, F.; Gumà, J.; Guilarte, C.; Pique, B.; Hernandez, A.; Àvila, A.; Parra, S.; Castro, A.; Rovira, C.; et al. Study of the Plasma and Buffy Coat in Patients with SARS-CoV-2 Infection—A Preliminary Report. Pathogens 2021, 10, 805. https://doi.org/10.3390/pathogens10070805
Peña KB, Riu F, Gumà J, Guilarte C, Pique B, Hernandez A, Àvila A, Parra S, Castro A, Rovira C, et al. Study of the Plasma and Buffy Coat in Patients with SARS-CoV-2 Infection—A Preliminary Report. Pathogens. 2021; 10(7):805. https://doi.org/10.3390/pathogens10070805
Chicago/Turabian StylePeña, Karla B., Francesc Riu, Josep Gumà, Carmen Guilarte, Berta Pique, Anna Hernandez, Alba Àvila, Sandra Parra, Antoni Castro, Conxita Rovira, and et al. 2021. "Study of the Plasma and Buffy Coat in Patients with SARS-CoV-2 Infection—A Preliminary Report" Pathogens 10, no. 7: 805. https://doi.org/10.3390/pathogens10070805
APA StylePeña, K. B., Riu, F., Gumà, J., Guilarte, C., Pique, B., Hernandez, A., Àvila, A., Parra, S., Castro, A., Rovira, C., Cueto, P., Vallverdu, I., & Parada, D. (2021). Study of the Plasma and Buffy Coat in Patients with SARS-CoV-2 Infection—A Preliminary Report. Pathogens, 10(7), 805. https://doi.org/10.3390/pathogens10070805