
The Prevalence, Risk, and Management of Methicillin-Resistant Staphylococcus aureus Infection in Diverse Populations across Canada: A Systematic Review

Abstract
1. Introduction
2. Results
3. Discussion
3.1. Antibiotic Resistance
3.2. Risk Factors
3.3. Future Directions
4. Materials and Methods
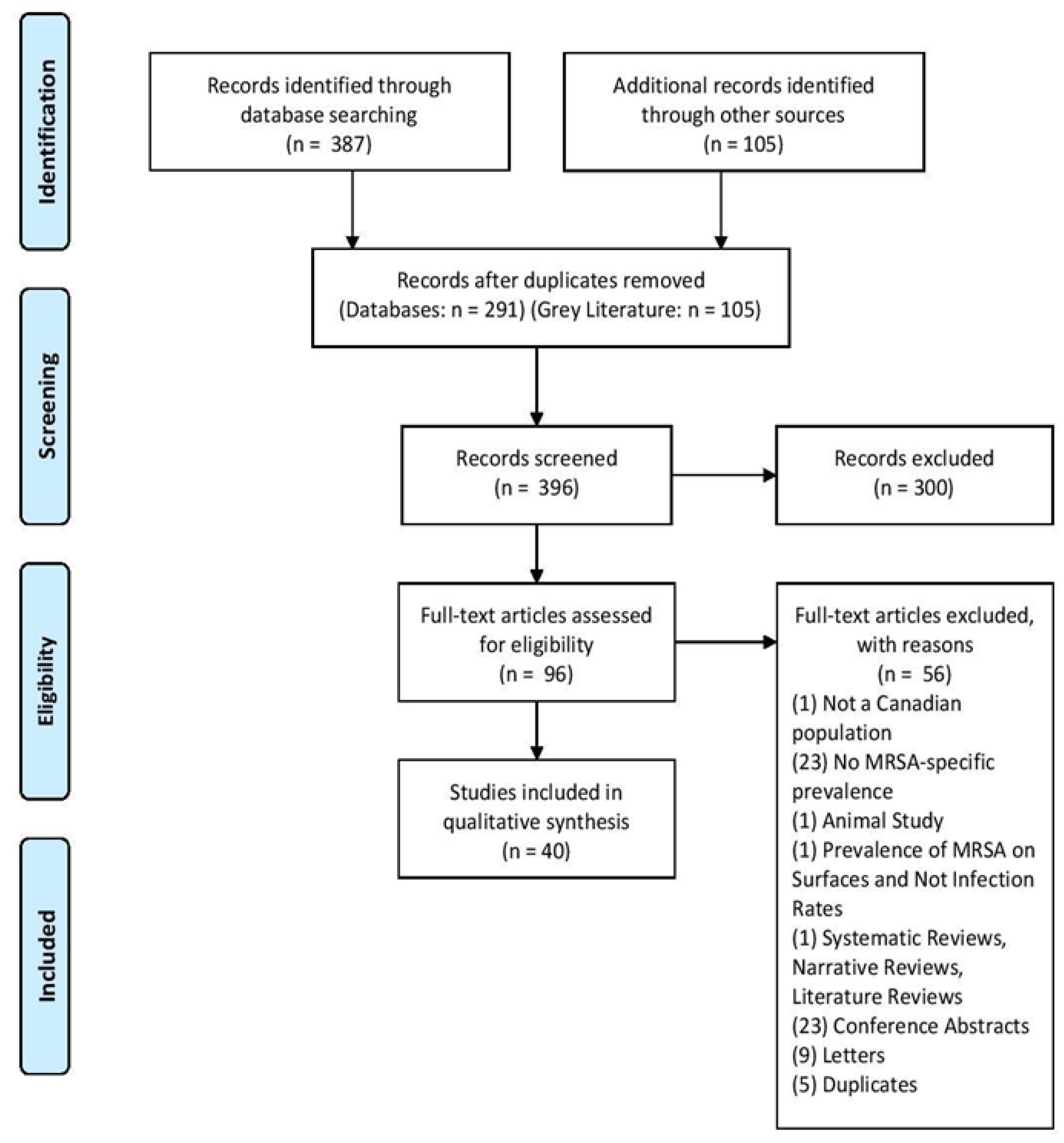
4.1. Search Strategy
4.2. Eligibility Criteria and Selection of Articles
4.3. Data Extraction Process and Synthesis of Evidence
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Key Words | ||
|---|---|---|
| MRSA Keywords | Canada Keywords | Prevalence Keywords |
| Methicillin-Resistant Staphylococcus aureus | Canada | Prevalence |
| MRSA | Canadian | Incidence |
| Alberta | ||
| British Columbia | ||
| Manitoba | ||
| New Brunswick | ||
| Newfoundland | ||
| Labrador | ||
| Northwest Territories | ||
| Nova Scotia | ||
| Nunavut | ||
| Ontario | ||
| Prince Edward Island | ||
| Quebec | ||
| Saskatchewan | ||
| Yukon | ||
| Mesh Terms: | ||
| MRSA Terms | Canada Terms | Prevalence Terms |
| Methicillin-resistant Staphylococcus Aureus | Canada | Prevalence |
| Alberta | Incidence | |
| British Columbia | ||
| Manitoba | ||
| New Brunswick | ||
| “Newfoundland and Labrador” | ||
| Northwest Territories | ||
| Nova Scotia | ||
| Nunavut | ||
| Ontario | ||
| Prince Edward Island | ||
| Quebec | ||
| Saskatchewan | ||
| Yukon Territory | ||
| EMtree Terms: | ||
| MRSA Terms | Canada Terms | Prevalence Terms |
| Methicillin-resistant Staphylococcus aureus | Canada | Epidemiological data |
| Meticillin resistant Staphylococcus aureus | Alberta | Prevalence |
| British Columbia | Infection Rate | |
| Manitoba | Incidence | |
| New Brunswick | ||
| “Newfoundland and Labrador” | ||
| Northwest Territories | ||
| Nova Scotia | ||
| Nunavut | ||
| Ontario | ||
| Prince Edward Island | ||
| Quebec | ||
| Saskatchewan | ||
| Yukon | ||
| First Author, Year | MRSA Prevalence | Year | Region | Population |
|---|---|---|---|---|
| Allard et al., 2008 | (Bacteremia) Prevalence in 1991–1999: 0 per 100,000 2000–2002: 2.6 per 100,000 patients Prevalence in 2002–2005: 7.4/100,000 | 1991–2005 | Quebec | Hospital Patients with at least 1 blood culture positive for S. aureus |
| Simor et al., 2001 | Prevalence (per 1000 admissions): 1995: 0.25 1999:1.11 | 1995–1999 | Across Canada | Hospital Patients |
| Simor et al., 2010 | Prevalence (per 10,000 patient days): 1995: 0.36 2007: 3.43 | 1995–2007 | Across Canada | Hospital Patients |
| Warshawsky et al., 2000 | Prevalence: 37 per 100,000 patients | 1997 | London, ON | Hospital and Clinic Patients |
| Sligl et al., 2007 | Infection Rate: 3.1 per 1000 ICU admissions (overall), Prevalence (per 1000 ICU admissions): 1997: 0.8 1998: 0.8 1999: 3.1 2000: 6.0 2001: 3.8 2002: 0.9 2003: 1.5 2004: 4.7 2005: 7.9 | 1997–2005 | Edmonton, AB | ICU Patients |
| Zoutman et al., 2005 | Prevalence: 2.0 per 1000 admissions | 1999 | Across Canada | Acute care hospital patients |
| First Author, Year | MRSA Prevalence | Year | Region | Population |
|---|---|---|---|---|
| Jones et. al, 2004 | Prevalence: 7.20% | 2000–2002 | Across Canada | 87 hospital sites |
| Al-Rawahi et al., 2008 | Prevalence: 2000: 7.4% 2006: 18.6% | 2000, 2006 | Vancouver | Injection Drug Users |
| Golding et al., 2012 | Prevalence: CA-MRSA 8.2/10,000 | 2001 | Northern Saskatchewan | Northern Health Regions in Saskatchewan |
| Cowie et al., 2005 | Prevalence: 22/408 participants = 5.39% | 2002 | Vancouver, BC | Acute Care Institutions |
| Bracco et al., 2007 | Prevalence: 1.1% | 2002–2004 | Montreal | ICU patients |
| Mitchell et al., 2019 | Prevalence (of all healthcare-associated infections): 2002: 3.9% 2017: 8.5% | 2002, 2017 | Across Canada | Hospital Inpatients |
| Poutanen et al., 2005 | Prevalence: 3.7 per 10,000 patient days | 2003 | Toronto, ON | Hospital Patients |
| Stenstrom et al., 2009 | Prevalence: 54.8% of SSTI patients, 68% after 21 months | 2003–2004 | Vancouver, BC | SSTI patients in ED |
| Wilmer et al., 2014 | Prevalence (in wound isolates, per 10 000 ED visits): 2003: 12.0 2004: 23.0 2005: 40.1 2006: 76.7 2007: 82.2 2008: 68.2 2009: 45.0 2010: 46.3 2011: 34.3 | 2003–2011 | Vancouver, BC | ED Patients |
| Gill et al., 2019 | Prevalence: 22.2/100,000 | 2004 | Calgary | Calgary Laboratory Services Data |
| Li et al., 2014 | Prevalence: 0.32 per 100,000 people | 2005 | Alberta | Individuals living in Alberta |
| Gilbert et al., 2007 | Prevalence (Infection and Colonization): 5.5% among 271 participants | 2005 | Calgary | From five study sites: an outreach needle-exchange van, homeless shelters, detoxification centres and residential substance treatment programs, and inner city medical clinic and new admissions to a local corrections facility |
| First Author, Year | MRSA Prevalence or Incidence | Year | Region | Population |
|---|---|---|---|---|
| Hanselman et al., 2008 | 3.18% (7/220) | 2006 | Toronto | School Teachers in Toronto |
| Szakacs et al. 2007 | Prevalence: 4.5% | 2006 | Ottawa, ON | Inner City Shelter Residents |
| Golding et al., 2011 | Prevalence: 146–482/10,000 | 2006–2008 | North Saskatchewan | 3 Northern Saskatchewan communities |
| Roth et al., 2016 | Prevalence: 46.79 per 100,000 patient days | 2006–2009 | Ottawa, ON | Hospital Patients |
| Li et al., 2017 | Incidence Rate Ratio: 2006–2007: 1.022, April 2007–Jan 2009: 0.989, Jan 2010–Mar 2015: 0.987 | 2006–2015 | Quebec | Teaching Facility Patients |
| Antoniou et al., 2009 | Prevalence: Nasal or Rectal Carriage (CA-MRSA) = 1.6% | 2007 | Toronto | Mainly men who have sex with men |
| Adam et al., 2011 | Prevalence: 356/8228 | 2007–2009 | British Columbia, Alberta, Manitoba, Saskatchewan, Ontario, Quebec, New Brunswick, Nova Scotia | Canadian Hospitals |
| Golding et al., 2012 | Prevalence (2006): 168.1 per 10,000 Prevalence (2008): 142.6 per 10,000 | 2006–2008 | North Saskatchewan | Northern health regions in Saskatchewan |
| Achiam et al., 2011 | Prevalence: 17.1% of all samples taken (13.2% from SSTI infection sites, 10.2% in nares cultures, 5.8% in throat cultures) | 2008 | London, Ontario | ED patients with SSTI infection |
| Zhanel et al., 2010 | Prevalence: 5.1% of all bacterial isolates | 2008 | Across Canada | Hospital Patients |
| Wang et al., 2018 | Prevalence of colonization: 3.13% | 2008–2010 | Ottawa, ON | Hospital Patients |
| Simor et al., 2016 | Prevalence: 0.45 per 1000 admissions (MRSA BSI) | 2008–2012 | Across Canada | Hospital Patients |
| Saito et al., 2013 | Prevalence: 0% | 2009 | Toronto, ON | ER Healthcare Workers |
| Trépanier et al., 2013 | Prevalence (colonization): 0.4% | 2010 | Quebec City, QC | Medical Residents |
| Simor et al., 2013 | Prevalence: 4.2% colonization, 0.3% infection rate | 2010 | All 10 Provinces | Hospital Inpatients |
| William et al., 2015 | Prevalence: 2010: 4.3% 2012: 3.9% | 2010, 2012 | All 10 provinces | Hospital Patients |
| Martin et al., 2018 | Prevalence: 0.7 per 100 inpatients | 2010, 2012, 2016 | Across Canada | Hospital Inpatients |
| First Author, Year | MRSA Prevalence | Year | Region | Population |
|---|---|---|---|---|
| Eman et al., 2014 | Prevalence: 3.0 cases per 100 residents | 2011 | Ontario | Long-term Care Homes in Ontario |
| Muileboom et al., 2013 | Prevalence: 2482 per 100,000 patients | 2011 | NW Ontario | Clinic, Laboratory and Hospital Patients (mainly remote Indigenous communities) |
| Li et al., 2014 | Prevalence: 1.44 per 100,000 people | 2012 | Alberta | Alberta Residents, most infected were Indigenous |
| Jeong et al., 2020 | Prevalence: 14.78% (55/372) | 2012–2013 | AB, SK, MB, ON, QC | Individuals in First Nations Communities Across 5 Provinces with SSTIs |
| Ugarte Torres et al., 2017 | Prevalence (colonization): 1.4% | 2014 | Calgary, AB | STI and Community Clinic Patients |
| Gill et al., 2019 | Prevalence: 81/100,000 | 2014 | Calgary | Calgary Laboratory Services Patients |
References
- Loewen, K.; Schreiber, Y.; Kirlew, M.; Bocking, N.; Kelly, L. Community-associated methicillin-resistant. Can. Fam. Physician 2005, 63, 512–520. [Google Scholar]
- Cimolai, N. Methicillin-resistant Staphylococcus aureus in Canada: A historical perspective and lessons learned. Can. J. Microbiol. 2010, 56, 89–120. [Google Scholar] [CrossRef]
- Methicillin-Resistant Staphylococcus aureus: An Update. (2012, February). Toronto Invasion Bacterial Disease Network. Available online: https://eportal.mountsinai.ca/Microbiology/research/tibdn/tibdnnews/TIBDN_Newsletter_16.pdf (accessed on 21 March 2021).
- Wang, R.; Braughton, K.R.; Kretschmer, D.; Bach, T.H.; Queck, S.Y.; Li, M.; Otto, M. Identification of novel cytolytic peptides as key virulence determinants for community-associated MRSA. Nat. Med. 2007, 13, 1510–1514. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Canadian Nosocomial Infection Surveillance Program. (Cnisp): Summary Report of Healthcare Associated Infection (Hai), Antimicrobial Resistance (Amr) and Antimicrobial Use (Amu) Surveillance Data from 1 January 2013 to 31 December 2017. Available online: https://www.canada.ca/en/public-health/services/publications/science-research-data/summary-report-healthcare-associated-infection-antimicrobial-resistance-antimicrobial-use-surveillance-data-2013-2017.html#a4.2. (accessed on 21 March 2021).
- Simor, A.E.; Williams, V.; McGeer, A.; Raboud, J.; Larios, O.; Weiss, K.; Hirji, Z.; Laing, F.; Moore, C.; Gravel, D. Prevalence of colonization and infection with methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus and of Clostridium difficile infection in Canadian hospitals. Infect. Control. Hosp. Epidemiol. 2013, 34, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Fortin, E.; Tremblay, C.; Ngenda-Muadi, M.; Garenc, C.; Moisan, D.; Villeneuve, J.; Quach, C. Hospital-Acquired Methicillin-Resistant Staphylococcus aureus Bloodstream Infections in Québec: Impact of Guidelines. Infect. Control. Hosp. Epidemiol. 2017, 38, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Simor, A.E.; Ofner-Agostini, M.; Bryce, E.; Green, K.; McGeer, A.; Mulvey, M.; The Canadian Nosocomial Infection Surveillance Program, Health Canada. The evolution of methicillin-resistant Staphylococcus aureus in Canadian hospitals: 5 years of national surveillance. CMAJ 2001, 165, 21–26. [Google Scholar] [PubMed]
- Sligl, W.; Taylor, G.; Gibney, R.N.; Rennie, R.; Chui, L. Methicillin-resistant Staphylococcus aureus in a Canadian intensive care unit: Delays in initiating effective therapy due to the low prevalence of infection. Can. J. Infect. Dis. Med. Microbiol 2007, 18, 139–143. [Google Scholar] [CrossRef]
- Saito, G.; Thom, J.; Wei, Y.; Gnanasuntharam, P.; Kreiswirth, N.; Willey, B.; Borgundvaag, B. Methicillin-resistant Staphylococcus aureus colonization among health care workers in a downtown emergency department in Toronto, Ontario. Can. J. Infect. Dis. Med. Microbiol 2013, 24, 57–60. [Google Scholar] [CrossRef]
- Golding, G.R.; Levett, P.N.; McDonald, R.R.; Irvine, J.; Quinn, B.; Nsungu, M.; Partnership, N.A.R. High rates of Staphylococcus aureus USA400 infection, Northern Canada. Emerg. Infect. Dis. 2011, 17, 722–725. [Google Scholar] [CrossRef]
- Golding, G.R.; Quinn, B.; Bergstrom, K.; Stockdale, D.; Woods, S.; Nsungu, M.; Partnership, N.A.R. Community-based educational intervention to limit the dissemination of community-associated methicillin-resistant Staphylococcus aureus in Northern Saskatchewan, Canada. BMC Public Health 2012, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Jeong, D.; Nguyen, H.N.T.; Tyndall, M.; Schreiber, Y.S. Antibiotic use among twelve Canadian First Nations communities: A retrospective chart review of skin and soft tissue infections. BMC Infect. Dis. 2020, 20, 118. [Google Scholar] [CrossRef]
- Allard, C.; Carignan, A.; Bergevin, M.; Boulais, I.; Tremblay, V.; Robichaud, P.; Pepin, J. Secular changes in incidence and mortality associated with Staphylococcus aureus bacteraemia in Quebec, Canada, 1991–2005. Clin. Microbiol. Infect. 2008, 14, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Warshawsky, B.; Hussain, Z.; Gregson, D.B.; Alder, R.; Austin, M.; Bruckschwaiger, D.; Schiedel, L. Hospital- and community-based surveillance of methicillin-resistant Staphylococcus aureus: Previous hospitalization is the major risk factor. Infect. Control. Hosp. Epidemiol. 2000, 21, 724–727. [Google Scholar] [CrossRef] [PubMed]
- Zoutman, D.E.; Ford, B.D. The relationship between hospital infection surveillance and control activities and antibiotic-resistant pathogen rates. Am. J. Infect. Control. 2005, 33, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.E.; Karlowsky, J.A.; Draghi, D.C.; Thornsberry, C.; Sahm, D.F.; Bradley, J.S. Rates of antimicrobial resistance among common bacterial pathogens causing respiratory, blood, urine, and skin and soft tissue infections in pediatric patients. Eur. J. Clin. Microbiol. Infect. Dis. 2004, 23, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Cowie, S.E.; Ma, I.; Lee, S.K.; Smith, R.M.; Hsiang, Y.N. Nosocomial MRSA infection in vascular surgery patients: Impact on patient outcome. Vasc. Endovasc. Surg. 2005, 39, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Gill, V.C.; Ma, I.; Guo, M.; Gregson, D.B.; Naugler, C.; Church, D.L. Sociodemographic and geospatial associations with community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA) infections in a large Canadian city: An 11 year retrospective study. BMC Public Health 2019, 19, 914. [Google Scholar] [CrossRef]
- Poutanen, S.M.; Vearncombe, M.; McGeer, A.J.; Gardam, M.; Large, G.; Simor, A.E. Nosocomial acquisition of methicillin-resistant Staphylococcus aureus during an outbreak of severe acute respiratory syndrome. Infect. Control. Hosp. Epidemiol. 2005, 26, 134–137. [Google Scholar] [CrossRef]
- Li, V.; Chui, L.; Simmonds, K.; Nguyen, T.; Golding, G.R.; Yacoub, W.; Louie, M. Emergence of new CMRSA7/USA400 methicillin-resistant Staphylococcus aureus spa types in Alberta, Canada, from 2005 to 2012. J. Clin. Microbiol. 2014, 52, 2439–2446. [Google Scholar] [CrossRef]
- Bracco, D.; Dubois, M.J.; Bouali, R.; Eggimann, P. Single rooms may help to prevent nosocomial bloodstream infection and cross-transmission of methicillin-resistant Staphylococcus aureus in intensive care units. Intensive Care Med. 2007, 33, 836–840. [Google Scholar] [CrossRef]
- Al-Rawahi, G.N.; Schreader, A.G.; Porter, S.D.; Roscoe, D.L.; Gustafson, R.; Bryce, E.A. Methicillin-resistant Staphylococcus aureus nasal carriage among injection drug users: Six years later. J. Clin. Microbiol. 2008, 46, 477–479. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, M.; Macdonald, J.; Louie, M.; Gregson, D.; Zhang, K.; Elsayed, S.; Conly, J. Prevalence of USA300 colonization or infection and associated variables during an outbreak of community-associated methicillin-resistant Staphylococcus aureus in a marginalized urban population. Can. J. Infect. Dis. Med. Microbiol. 2007, 18, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Stenstrom, R.; Grafstein, E.; Romney, M.; Fahimi, J.; Harris, D.; Hunte, G.; Christenson, J. Prevalence of and risk factors for methicillin-resistant Staphylococcus aureus skin and soft tissue infection in a Canadian emergency department. CJEM 2009, 11, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Szakacs, T.A.; Toye, B.; Turnbull, J.M.; Muckle, W.; Roth, V.R. Prevalence of methicillin-resistant Staphylococcus aureus in a Canadian inner-city shelter. Can. J. Infect. Dis. Med. Microbiol. 2007, 18, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Hanselman, B.A.; Kruth, S.A.; Rousseau, J.; Weese, J.S. Methicillin-resistant Staphylococcus aureus colonization in schoolteachers in Ontario. Can. J. Infect. Dis. Med. Microbiol. 2008, 19, 405–408. [Google Scholar] [CrossRef]
- Trépanier, P.; Tremblay, C.; Ruest, A. Methicillin-resistant Staphylococcus aureus colonization among medical residents. Can. J. Infect. Dis. Med. Microbiol. 2013, 24, 148937. [Google Scholar] [CrossRef]
- Mitchell, R.; Taylor, G.; Rudnick, W.; Alexandre, S.; Bush, K.; Forrester, L.; Program, C.N.I.S. Trends in health care-associated infections in acute care hospitals in Canada: An analysis of repeated point-prevalence surveys. CMAJ 2019, 191, E981–E988. [Google Scholar] [CrossRef]
- Wilmer, A.; Lloyd-Smith, E.; Romney, M.G.; Champagne, S.; Wong, T.; Zhang, W.; Hull, M.W. Reduction in community-onset methicillin-resistant Staphylococcus aureus rates in an urban Canadian hospital setting. Epidemiol. Infect. 2014, 142, 463–467. [Google Scholar] [CrossRef]
- Achiam, C.C.; Fernandes, C.M.; McLeod, S.L.; Salvadori, M.I.; John, M.; Seabrook, J.A.; Hussain, Z. Methicillin-resistant Staphylococcus aureus in skin and soft tissue infections presenting to the Emergency Department of a Canadian Academic Health Care Center. Eur. J. Emerg. Med. 2011, 18, 2–8. [Google Scholar] [CrossRef]
- Adam, H.J.; DeCorby, M.; Rennie, R.; Karlowsky, J.A.; Hoban, D.J.; Zhanel, G.G.; The Canadian Antimicrobial Resistance Alliance (CARA). Prevalence of antimicrobial resistant pathogens from blood cultures from Canadian hospitals: Results of the CANWARD 2007–2009 study. Diagn. Microbiol. Infect. Dis. 2011, 69, 307–313. [Google Scholar] [CrossRef]
- Antoniou, T.; Devlin, R.; Gough, K.; Mulvey, M.; Katz, K.C.; Zehtabchi, M.; Loutfy, M.R. Prevalence of community-associated methicillin-resistant Staphylococcus aureus colonization in men who have sex with men. Int. J. STD AIDS 2009, 20, 180–183. [Google Scholar] [CrossRef]
- Martin, P.; Chakra, C.N.A.; Williams, V.; Bush, K.; Dyck, M.; Hirji, Z.; Kiss, A.; Larios, O.E.; McGeer, A.; Moore, C.; et al. Prevalence of antibiotic-resistant organisms in Canadian Hospitals. Comparison of point-prevalence survey results from 2010, 2012, and 2016. Infect. Control. Hosp. Epidemiol. 2019, 40, 53–59. [Google Scholar] [CrossRef]
- Roth, V.R.; Longpre, T.; Taljaard, M.; Coyle, D.; Suh, K.N.; Muldoon, K.A.; Forster, A. Universal vs risk factor screening for methicillin-resistant staphylococcus aureus in a large multicenter tertiary care facility in Canada. Infect. Control. Hosp. Epidemiol. 2016, 37, 41–48. [Google Scholar] [CrossRef]
- Simor, A.E.; Pelude, L.; Golding, G.; Fernandes, R.; Bryce, E.; Frenette, C.; Program, C.N.I.S. Determinants of outcome in hospitalized patients with methicillin-resistant staphylococcus aureus bloodstream infection: Results from national surveillance in Canada, 2008–2012. Infect. Control. Hosp. Epidemiol. 2016, 37, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Suh, K.N.; Muldoon, K.A.; Oake, N.; Forster, A.; Ramotar, K.; Roth, V.R. Risk factors for methicillin-resistant staphylococcus aureus (mrsa) colonization among patients admitted to obstetrical units: A nested case-control study. J. Obstet. Gynaecol. Can. 2018, 40, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Williams, V.; Simor, A.E.; Kiss, A.; McGeer, A.; Hirji, Z.; Larios, O.E.; Moore, C.; Weiss, K. Is the prevalence of antibiotic-resistant organisms changing in Canadian hospitals? Comparison of point-prevalence survey results in 2010 and 2012. Clin. Microbiol. Infect. 2015, 21, 553–559. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhanel, G.G.; DeCorby, M.; Adam, H.; Mulvey, M.R.; McCracken, M.; Lagacé-Wiens, P.; Alliance, C.A.R. Prevalence of antimicrobial-resistant pathogens in Canadian hospitals: Results of the Canadian Ward Surveillance Study (CANWARD 2008). Antimicrob. Agents Chemother. 2010, 54, 4684–4693. [Google Scholar] [CrossRef] [PubMed]
- Ugarte Torres, A.; Chu, A.; Read, R.; MacDonald, J.; Gregson, D.; Louie, T.; Conly, J. The epidemiology of Staphylococcus aureus carriage in patients attending inner city sexually transmitted infections and community clinics in Calgary, Canada. PLoS ONE 2017, 12, e0178557. [Google Scholar] [CrossRef]
- El Emam, K.; Arbuckle, L.; Essex, A.; Samet, S.; Eze, B.; Middleton, G.; Earle, C. Secure surveillance of antimicrobial resistant organism colonization or infection in Ontario long term care homes. PLoS ONE 2014, 9, e93285. [Google Scholar] [CrossRef]
- Muileboom, J.; Hamilton, M.; Parent, K.; Makahnouk, D.; Kirlew, M.; Saginur, R.; Kelly, L. Community-associated methicillin-resistant Staphylococcus aureus in northwest Ontario: A five-year report of incidence and antibiotic resistance. Can. J. Infect. Dis. Med. Microbiol. 2013, 24, e42–e44. [Google Scholar] [CrossRef]
- Kim, J.; Ferrato, C.; Golding, G.R.; Mulvey, M.R.; Simmonds, K.A.; Svenson, L.W.; Louie, M. Changing epidemiology of methicillin-resistant Staphylococcus aureus in Alberta, Canada: Population-based surveillance, 2005–2008. Epidemiol. Infect. 2011, 139, 1009–1018. [Google Scholar] [CrossRef]
- Laupland, K.B.; Ross, T.; Gregson, D.B. Staphylococcus aureus bloodstream infections: Risk factors, outcomes, and the influence of methicillin resistance in Calgary, Canada, 2000–2006. J. Infect. Dis. 2008, 198, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Laupland, K.B.; Lyytikäinen, O.; Søgaard, M.; Kennedy, K.J.; Knudsen, J.D.; Ostergaard, C.; Collaborative, I.B.S. The changing epidemiology of Staphylococcus aureus bloodstream infection: A multinational population-based surveillance study. Clin. Microbiol. Infect. 2013, 19, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Simor, A.E.; Gilbert, N.L.; Gravel, D.; Mulvey, M.R.; Bryce, E.; Loeb, M.; Program, C.N.I.S. Methicillin-resistant Staphylococcus aureus colonization or infection in Canada: National surveillance and changing epidemiology, 1995–2007. Infect. Control. Hosp. Epidemiol. 2010, 31, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shammer, L.; Clarke, M. Preferred reporting items for systematic reviews and meta-analyses protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitevska, E.; Wong, B.; Surewaard, B.G.J.; Jenne, C.N. The Prevalence, Risk, and Management of Methicillin-Resistant Staphylococcus aureus Infection in Diverse Populations across Canada: A Systematic Review. Pathogens 2021, 10, 393. https://doi.org/10.3390/pathogens10040393
Mitevska E, Wong B, Surewaard BGJ, Jenne CN. The Prevalence, Risk, and Management of Methicillin-Resistant Staphylococcus aureus Infection in Diverse Populations across Canada: A Systematic Review. Pathogens. 2021; 10(4):393. https://doi.org/10.3390/pathogens10040393
Chicago/Turabian StyleMitevska, Elena, Britney Wong, Bas G. J. Surewaard, and Craig N. Jenne. 2021. "The Prevalence, Risk, and Management of Methicillin-Resistant Staphylococcus aureus Infection in Diverse Populations across Canada: A Systematic Review" Pathogens 10, no. 4: 393. https://doi.org/10.3390/pathogens10040393
APA StyleMitevska, E., Wong, B., Surewaard, B. G. J., & Jenne, C. N. (2021). The Prevalence, Risk, and Management of Methicillin-Resistant Staphylococcus aureus Infection in Diverse Populations across Canada: A Systematic Review. Pathogens, 10(4), 393. https://doi.org/10.3390/pathogens10040393