
The Subgingival Plaque Microbiome, Systemic Antibodies against Bacteria and Citrullinated Proteins following Periodontal Therapy

 , , ,
, , ,  and
and 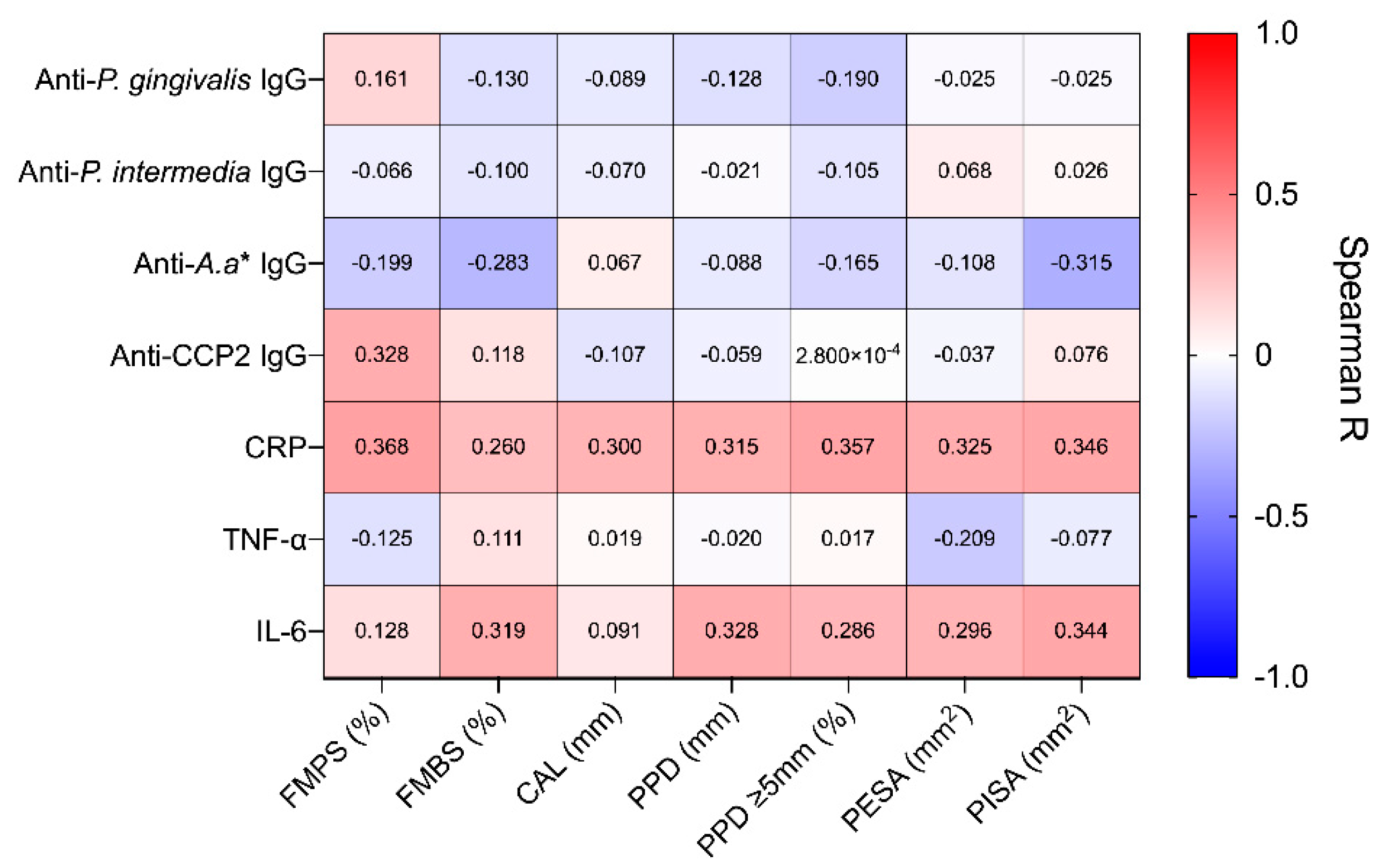{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Results
2.1. Study Cohort and Clinical Improvement
2.2. Association between Clinical Parameters and Systemic Markers
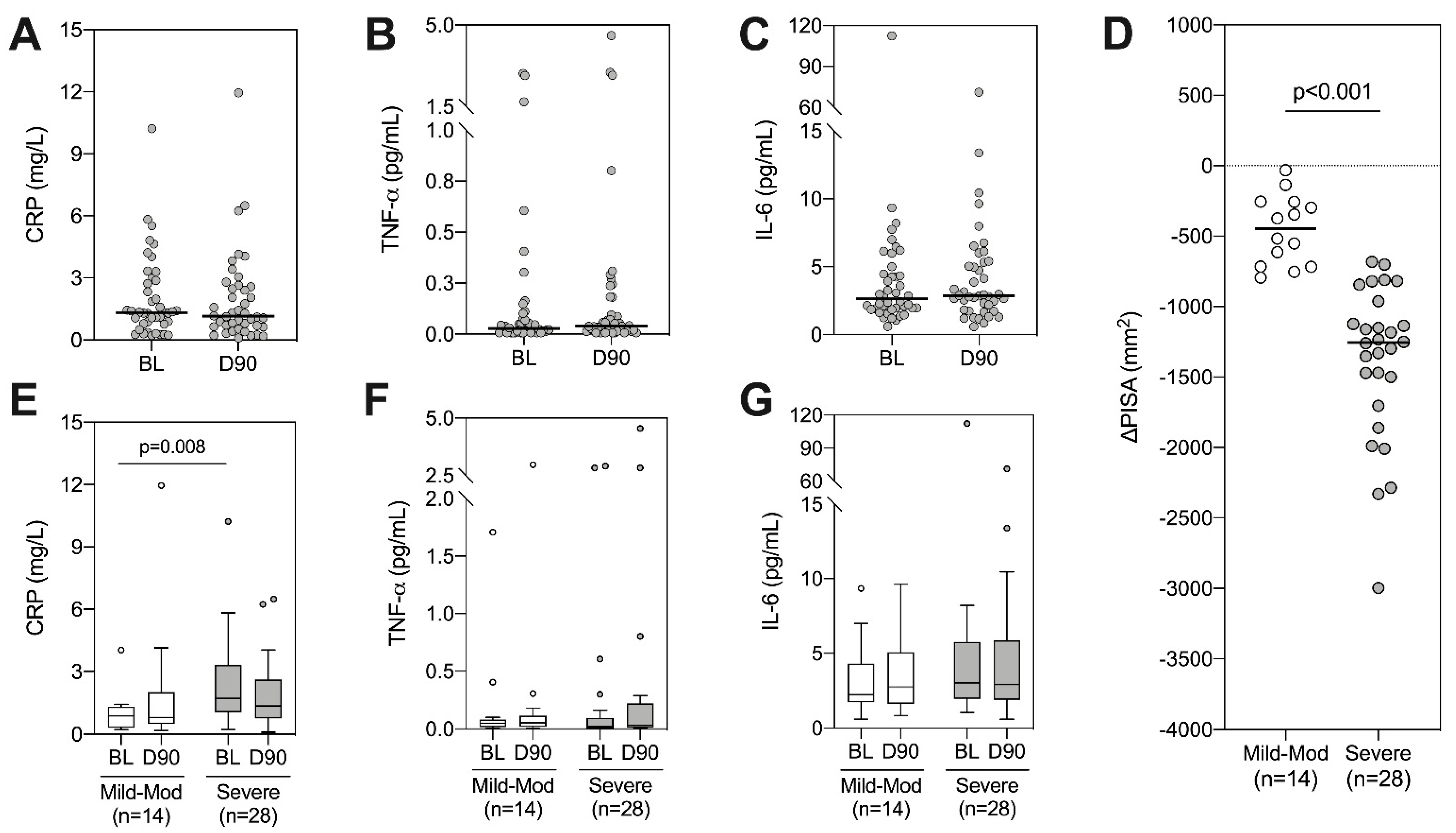
2.3. Longitudinal Alterations in Systemic Inflammatory Markers
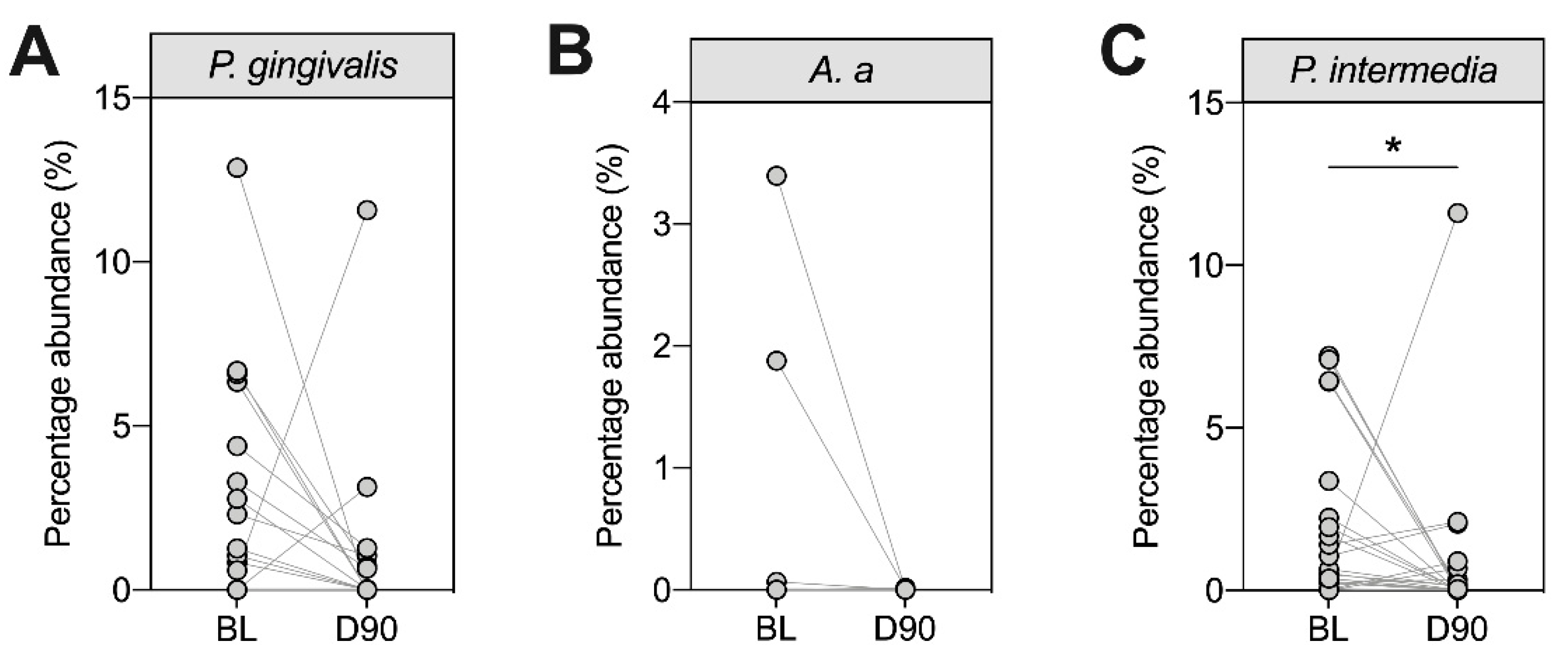
2.4. Subgingival Plaque Colonisation by P. gingivalis, A. actinomycetemcomitans and P. intermedia
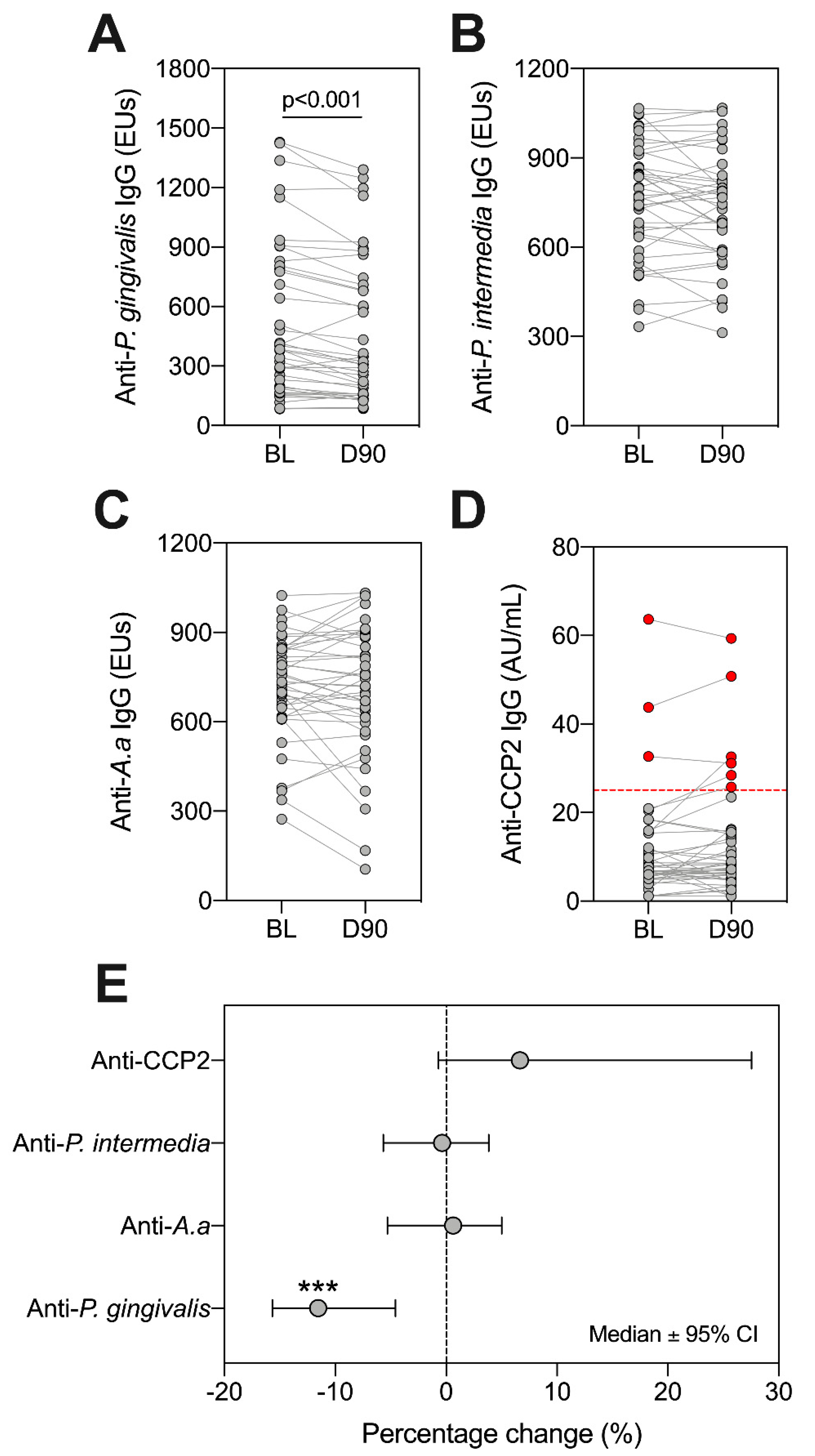
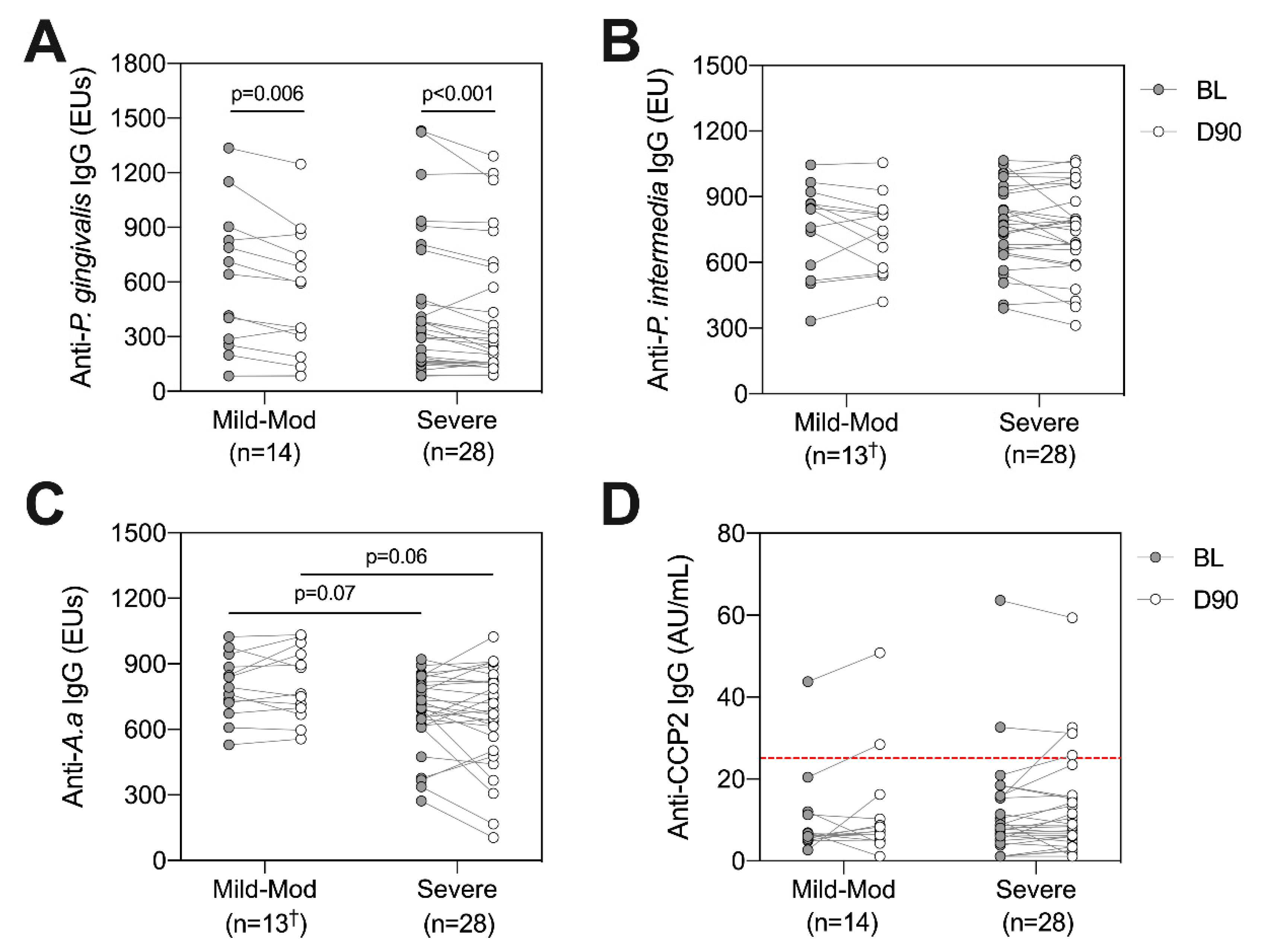
2.5. Longitudinal Alterations in Antibody Titres
2.6. Anti-Bacterial Antibodies and ACPAs according to Periodontal Disease Severity
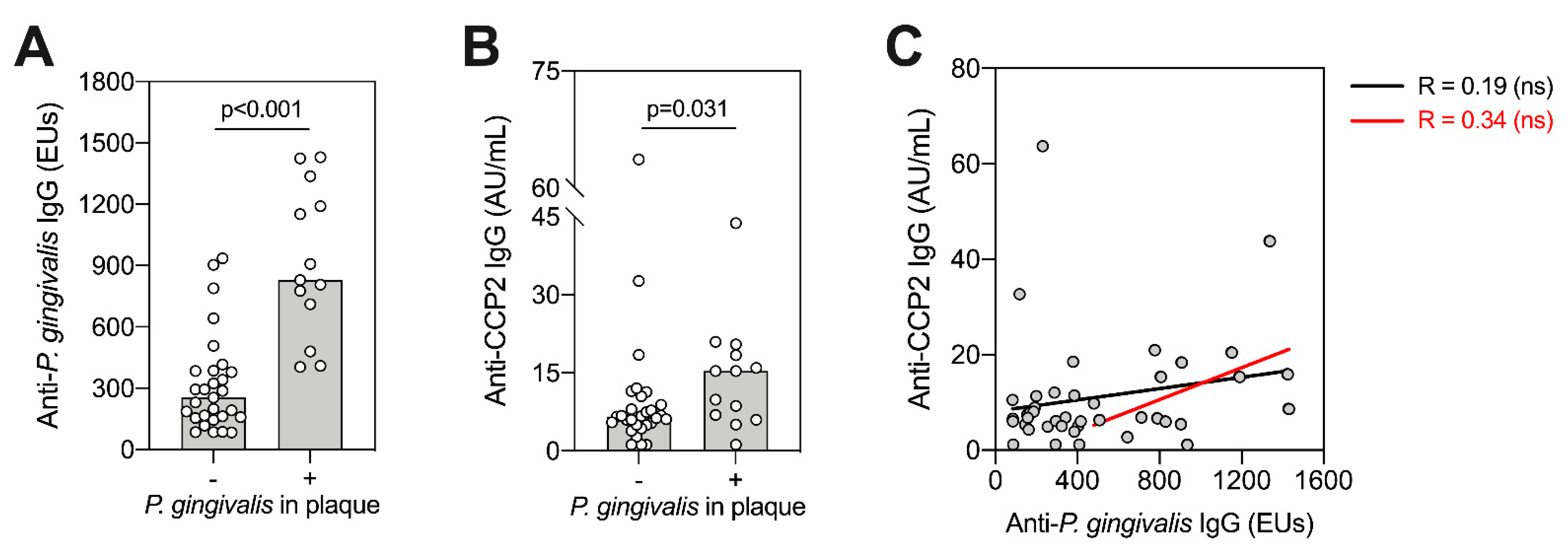
2.7. P. gingivalis Colonisation and Antibody Titres
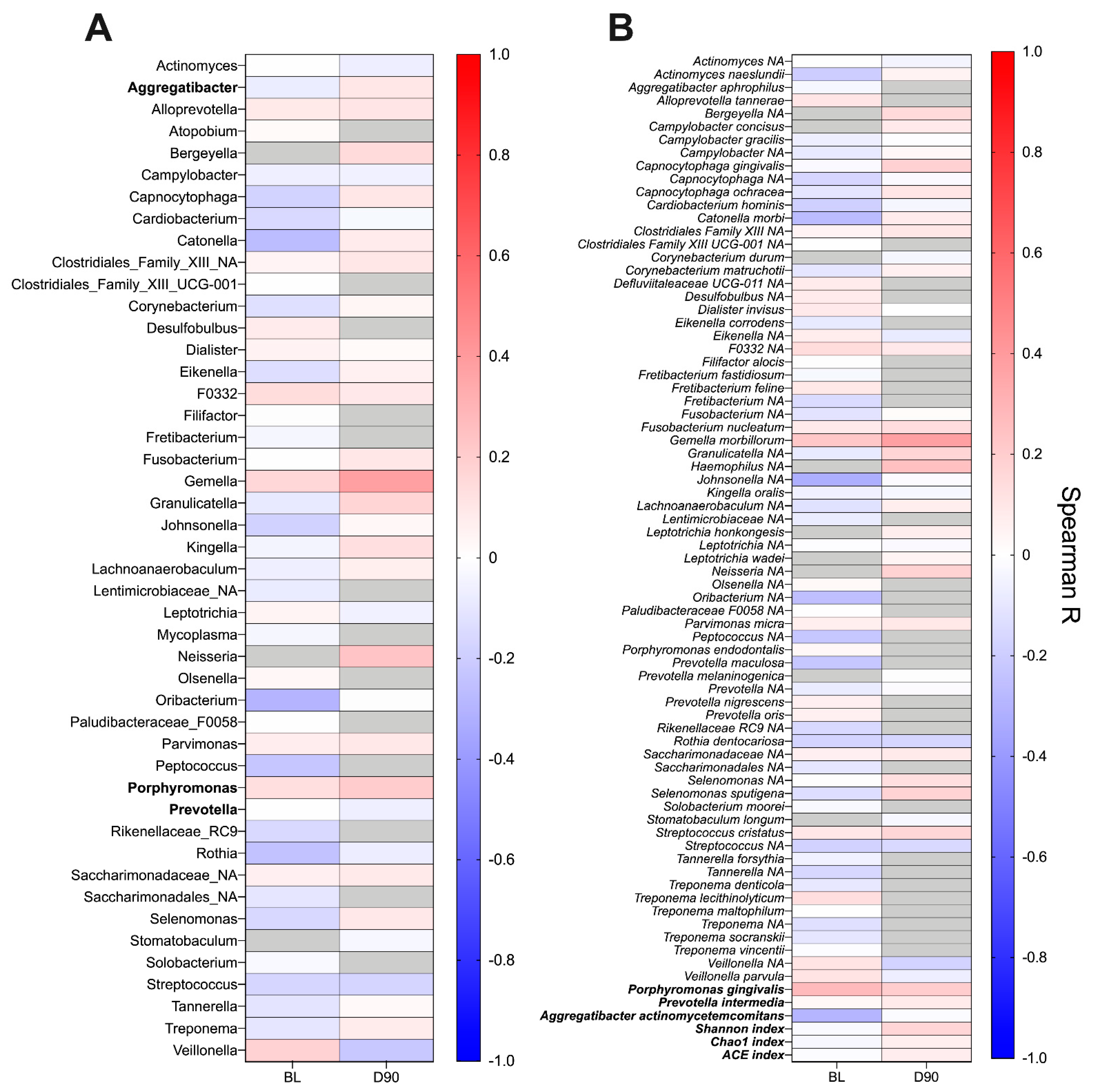
2.8. ACPA Association with Subgingival Plaque Microbiome
3. Discussion
4. Materials and Methods
4.1. Study Population, Treatment and Clinical Examination
4.2. Sample Collection and Processing
4.3. CCP2 ELISA
4.4. Anti-Bacterial Antibody Titres
4.5. Analysis of Inflammatory Markers
4.6. Bacterial 16S rRNA Sequencing
4.7. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Del Castillo, A.M.; Jepsen, S.; Gonzalez-Juanatey, J.R.; D’Aiuto, F.; Bouchard, P.; Chapple, I.; Dietrich, T.; Gotsman, I.; Graziani, F.; et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [Google Scholar] [CrossRef] [PubMed]
- Potempa, J.; Mydel, P.; Koziel, J. The case for periodontitis in the pathogenesis of rheumatoid arthritis. Nat. Rev. Rheumatol. 2017, 13, 606–620. [Google Scholar] [CrossRef]
- Ide, R.; Hoshuyama, T.; Wilson, D.; Takahashi, K.; Higashi, T. Periodontal Disease and Incident Diabetes. J. Dent. Res. 2010, 90, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Mira, A.; Simon-Soro, A.; Curtis, M.A. Role of microbial communities in the pathogenesis of periodontal diseases and caries. J. Clin. Periodontol. 2017, 44, S23–S38. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Darveau, R.P.; Curtis, M.A. The keystone-pathogen hypothesis. Nat. Rev. Microbiol. 2012, 10, 717–725. [Google Scholar] [CrossRef]
- Hoek, J.V.D.; Boshuizen, H.C.; Roorda, L.D.; Tijhuis, G.J.; Nurmohamed, M.T.; Bos, G.A.M.V.D.; Dekker, J. Mortality in patients with rheumatoid arthritis: A 15-year prospective cohort study. Rheumatol. Int. 2017, 37, 487–493. [Google Scholar] [CrossRef]
- Culshaw, S.; McInnes, I.; Liew, F.Y. What can the periodontal community learn from the pathophysiology of rheumatoid arthritis? J. Clin. Periodontol. 2011, 38, 106–113. [Google Scholar] [CrossRef]
- Anderson, J.; Caplan, L.; Yazdany, J.; Robbins, M.L.; Neogi, T.; Michaud, K.; Saag, K.G.; O’Dell, J.R.; Kazi, S. Rheumatoid arthritis disease activity measures: American College of Rheumatology recommendations for use in clinical practice. Arthritis Rheumatol. 2012, 64, 640–647. [Google Scholar] [CrossRef]
- Firestein, G.S.; McInnes, I.B. Immunopathogenesis of Rheumatoid Arthritis. Immunity 2017, 46, 183–196. [Google Scholar] [CrossRef]
- Rocha, S.D.B.; Baldo, D.C.; Andrade, L.E.C. Clinical and pathophysiologic relevance of autoantibodies in rheumatoid arthritis. Adv. Rheumatol. 2019, 59, 2. [Google Scholar] [CrossRef]
- Bizzaro, N.; Bartoloni, E.; Morozzi, G.; Manganelli, S.; Riccieri, V.; Sabatini, P.; Filippini, M.; Tampoia, M.; Afeltra, A.; Sebastiani, G.D.; et al. Anti-cyclic citrullinated peptide antibody titer predicts time to rheumatoid arthritis onset in patients with undifferentiated arthritis: Results from a 2-year prospective study. Arthritis Res. Ther. 2013, 15, R16. [Google Scholar] [CrossRef]
- Dahlqvist, S.R.; De Jong, B.A.W.; Berglin, E.; Hallmans, G.; Wadell, G.; Stenlund, H.; Sundin, U.; Van Venrooij, W.J. Antibodies against cyclic citrullinated peptide and IgA rheumatoid factor predict the development of rheumatoid arthritis. Arthritis Rheumatol. 2003, 48, 2741–2749. [Google Scholar] [CrossRef]
- Guo, Q.; Wang, Y.; Xu, D.; Nossent, J.; Pavlos, N.J.; Xu, J. Rheumatoid arthritis: Pathological mechanisms and modern pharmacologic therapies. Bone Res. 2018, 6, 1–14. [Google Scholar] [CrossRef]
- Nesse, W.; Westra, J.; Van Der Wal, J.E.; Abbas, F.; Nicholas, A.P.; Vissink, A.; Brouwer, E. The periodontium of periodontitis patients contains citrullinated proteins which may play a role in ACPA (anti-citrullinated protein antibody) formation. J. Clin. Periodontol. 2012, 39, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Wegner, N.; Wait, R.; Sroka, A.; Eick, S.; Nguyen, K.-A.; Lundberg, K.; Kinloch, A.; Culshaw, S.; Potempa, J.; Venables, P.J. Peptidylarginine deiminase from Porphyromonas gingivalis citrullinates human fibrinogen and α-enolase: Implications for autoimmunity in rheumatoid arthritis. Arthritis Rheumatol. 2010, 62, 2662–2672. [Google Scholar] [CrossRef] [PubMed]
- Konig, M.F.; Abusleme, L.; Reinholdt, J.; Palmer, R.J.; Teles, R.P.; Sampson, K.; Rosen, A.; Nigrovic, P.A.; Sokolove, J.; Giles, J.T.; et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci. Transl. Med. 2016, 8, 369ra176. [Google Scholar] [CrossRef] [PubMed]
- McGraw, W.T.; Potempa, J.; Farley, D.; Travis, J. Purification, Characterization, and Sequence Analysis of a Potential Virulence Factor from Porphyromonas gingivalis, Peptidylarginine Deiminase. Infect. Immun. 1999, 67, 3248–3256. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Neiderud, A.-M.; Papadimitriou, A.; Sandros, J.; Dahlén, G. “Checkerboard” Assessments of Periodontal Microbiota and Serum Antibody Responses: A Case-Control Study. J. Periodontol. 2000, 71, 885–897. [Google Scholar] [CrossRef]
- Pussinen, P.J.; Könönen, E.; Paju, S.; Hyvärinen, K.; Gursoy, U.K.; Huumonen, S.; Knuuttila, M.; Suominen, A.L. Periodontal pathogen carriage, rather than periodontitis, determines the serum antibody levels. J. Clin. Periodontol. 2011, 38, 405–411. [Google Scholar] [CrossRef]
- Vlachojannis, C.; Dye, B.A.; Herrera-Abreu, M.; Pikdöken, L.; Lerche-Sehm, J.; Pretzl, B.; Celenti, R.; Papapanou, P.N. Determinants of serum IgG responses to periodontal bacteria in a nationally representative sample of US adults. J. Clin. Periodontol. 2010, 37, 685–696. [Google Scholar] [CrossRef]
- Dye, B.A.; Herrera-Abreu, M.; Lerche-Sehm, J.; Vlachojannis, C.; Pikdöken, L.; Pretzl, B.; Schwartz, A.; Papapanou, P.N. Serum Antibodies to Periodontal Bacteria as Diagnostic Markers of Periodontitis. J. Periodontol. 2009, 80, 634–647. [Google Scholar] [CrossRef]
- Suvan, J.; Leira, Y.; Moreno, F.; Graziani, F.; Derks, J.; Tomasi, C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J. Clin. Periodontol. 2019, 47, 155–175. [Google Scholar] [CrossRef]
- Chen, C.; Hemme, C.; Beleno, J.; Shi, Z.J.; Ning, D.; Qin, Y.; Tu, Q.; Jorgensen, M.; He, Z.; Wu, L.; et al. Oral microbiota of periodontal health and disease and their changes after nonsurgical periodontal therapy. ISME J. 2018, 12, 1210–1224. [Google Scholar] [CrossRef] [PubMed]
- Shi, B.; Chang, M.; Martin, J.; Mitreva, M.; Lux, R.; Klokkevold, P.; Sodergren, E.; Weinstock, G.M.; Haake, S.K.; Li, H. Dynamic Changes in the Subgingival Microbiome and Their Potential for Diagnosis and Prognosis of Periodontitis. MBio 2015, 6. [Google Scholar] [CrossRef]
- Leira, Y.; Martín-Lancharro, P.; Blanco, J. Periodontal inflamed surface area and periodontal case definition classification. Acta Odontol. Scand. 2017, 76, 195–198. [Google Scholar] [CrossRef]
- Lappin, D.F.; Apatzidou, D.; Quirke, A.-M.; Oliver-Bell, J.; Butcher, J.P.; Kinane, D.F.; Riggio, M.P.; Venables, P.; McInnes, I.B.; Culshaw, S. Influence of periodontal disease, Porphyromonas gingivalis and cigarette smoking on systemic anti-citrullinated peptide antibody titres. J. Clin. Periodontol. 2013, 40, 907–915. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Payne, J.B.; Yu, F.; Thiele, G.M.; Reynolds, R.J.; Cannon, G.W.; Markt, J.; McGowan, D.; Kerr, G.S.; Redman, R.S.; et al. Periodontitis andPorphyromonas gingivalisin Patients with Rheumatoid Arthritis. Arthritis Rheumatol. 2014, 66, 1090–1100. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Thiele, G.M.; Deane, K.D.; Payne, J.B.; O’Dell, J.R.; Yu, F.; Sayles, H.; Weisman, M.H.; Gregersen, P.K.; Buckner, J.H.; et al. Porphyromonas gingivalisand disease-related autoantibodies in individuals at increased risk of rheumatoid arthritis. Arthritis Rheumatol. 2012, 64, 3522–3530. [Google Scholar] [CrossRef]
- Okada, M.; Kobayashi, T.; Ito, S.; Yokoyama, T.; Abe, A.; Murasawa, A.; Yoshie, H. Periodontal Treatment Decreases Levels of Antibodies toPorphyromonas gingivalisand Citrulline in Patients with Rheumatoid Arthritis and Periodontitis. J. Periodontol. 2013, 84, e74–e84. [Google Scholar] [CrossRef]
- Shimada, A.; Kobayashi, T.; Ito, S.; Okada, M.; Murasawa, A.; Nakazono, K.; Yoshie, H. Expression of anti-Porphyromonas gingivalis peptidylarginine deiminase immunoglobulin G and peptidylarginine deiminase-4 in patients with rheumatoid arthritis and periodontitis. J. Periodontal Res. 2016, 51, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Yang, N.-Y.; Wang, C.; Chyuan, I.-T.; Wu, K.-J.; Tu, Y.-K.; Chang, C.-W.; Hsu, P.N.; Kuo, M.Y.-P.; Chen-Ying, W. Significant association of rheumatoid arthritis-related inflammatory markers with non-surgical periodontal therapy. J. Formos. Med. Assoc. 2018, 117, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Hensvold, A.H.; Frisell, T.; Magnusson, P.K.E.; Holmdahl, R.; Askling, J.; Catrina, A.I. How well do ACPA discriminate and predict RA in the general population: A study based on 12 590 population-representative Swedish twins. Ann. Rheum. Dis. 2016, 76, 119–125. [Google Scholar] [CrossRef]
- Teeuw, W.J.; Slot, D.E.; Susanto, H.; Gerdes, V.E.A.; Abbas, F.; D’Aiuto, F.; Kastelein, J.J.P.; Loos, B.G. Treatment of periodontitis improves the atherosclerotic profile: A systematic review and meta-analysis. J. Clin. Periodontol. 2014, 41, 70–79. [Google Scholar] [CrossRef]
- Loutan, L.; Alpízar-Rodríguez, D.; Courvoisier, D.S.; Finckh, A.; Mombelli, A.; Giannopoulou, C. Periodontal status correlates with anti-citrullinated protein antibodies in first-degree relatives of individuals with rheumatoid arthritis. J. Clin. Periodontol. 2019, 46, 690–698. [Google Scholar] [CrossRef]
- Bender, P.; Bürgin, W.B.; Sculean, A.; Eick, S. Serum antibody levels against Porphyromonas gingivalis in patients with and without rheumatoid arthritis—A systematic review and meta-analysis. Clin. Oral Investig. 2017, 21, 33–42. [Google Scholar] [CrossRef]
- Seror, R.; Le Gall-David, S.; Bonnaure-Mallet, M.; Schaeverbeke, T.; Cantagrel, A.; Minet, J.; Gottenberg, J.-E.; Chanson, P.; Ravaud, P.; Mariette, X. Association of Anti-Porphyromonas gingivalisAntibody Titers with Nonsmoking Status in Early Rheumatoid Arthritis: Results from the Prospective French Cohort of Patients with Early Rheumatoid Arthritis. Arthritis Rheumatol. 2015, 67, 1729–1737. [Google Scholar] [CrossRef]
- Fisher, A.B.; Cartwright, A.; Quirke, A.-M.; De Pablo, P.; Romaguera, D.; Panico, S.; Mattiello, A.; Gavrila, D.; Navarro, C.; Sacerdote, C.; et al. Smoking, Porphyromonas gingivalis and the immune response to citrullinated autoantigens before the clinical onset of rheumatoid arthritis in a Southern European nested case–control study. BMC Musculoskelet. Disord. 2015, 16, 1–11. [Google Scholar] [CrossRef]
- Horibe, M.; Watanabe, H.; Ishikawa, I. Effect of periodontal treatments on serum IgG antibody titers against periodontopathic bacteria. J. Clin. Periodontol. 1995, 22, 510–515. [Google Scholar] [CrossRef]
- Kudo, C.; Naruishi, K.; Maeda, H.; Abiko, Y.; Hino, T.; Iwata, M.; Mitsuhashi, C.; Murakami, S.; Nagasawa, T.; Nagata, T.; et al. Assessment of the Plasma/Serum IgG Test to Screen for Periodontitis. J. Dent. Res. 2012, 91, 1190–1195. [Google Scholar] [CrossRef]
- Darby, I.B.; Mooney, J.; Kinane, D.F. Changes in subgingival microflora and humoral immune response following periodontal therapy. J. Clin. Periodontol. 2001, 28, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Lange, L.; Thiele, G.M.; McCracken, C.E.; Wang, G.; Ponder, L.A.; Angeles-Han, S.T.; Rouster-Stevens, K.A.; Hersh, A.O.; Vogler, L.B.; Bohnsack, J.F.; et al. Symptoms of periodontitis and antibody responses to Porphyromonas gingivalis in juvenile idiopathic arthritis. Pediatr. Rheumatol. 2016, 14, 8. [Google Scholar] [CrossRef]
- Lakio, L.; Antinheimo, J.; Paju, S.; Buhlin, K.; Pussinen, P.J.; Alfthan, G. Tracking of plasma antibodies againstAggregatibacter actinomycetemcomitansandPorphyromonas gingivalisduring 15 years. J. Oral Microbiol. 2009, 1, 1. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Okuda, K.; Takazoe, I.; Watanabe, H.; Ishikawa, I. The Relationship between Serum IgG Levels to Subgingival Gram-negative Bacteria and Degree of Periodontal Destruction. J. Dent. Res. 1985, 64, 1306–1310. [Google Scholar] [CrossRef]
- Damgaard, C.; Reinholdt, J.; Enevold, C.; Fiehn, N.-E.; Nielsen, C.H.; Holmstrup, P. Immunoglobulin G antibodies against Porphyromonas gingivalis or Aggregatibacter actinomycetemcomitans in cardiovascular disease and periodontitis. J. Oral Microbiol. 2017, 9, 1374154. [Google Scholar] [CrossRef]
- Kharlamova, N.; Jiang, X.; Sherina, N.; Potempa, B.; Israelsson, L.; Quirke, A.-M.; Eriksson, K.; Yucel-Lindberg, T.; Venables, P.J.; Potempa, J.; et al. Antibodies toPorphyromonas gingivalisIndicate Interaction Between Oral Infection, Smoking, and Risk Genes in Rheumatoid Arthritis Etiology. Arthritis Rheumatol. 2016, 68, 604–613. [Google Scholar] [CrossRef]
- Sjöström, K.; Ou, J.; Whitney, C.; Johnson, B.; Darveau, R.; Engel, D.; Page, R.C.; Myers, B.; Pharmaceutical, S. Effect of Treatment on Titer, Function, and Antigen Recognition of Serum Antibodies to Actinobacillus Actinomycetemcomitans in Patients with Rapidly Progressive Periodontitis. Inject. Immun. 1994, 62, 145–151. [Google Scholar] [CrossRef]
- Nesse, W.; Abbas, F.; Van Der Ploeg, I.; Spijkervet, F.K.L.; Dijkstra, P.U.; Vissink, A. Periodontal inflamed surface area: Quantifying inflammatory burden. J. Clin. Periodontol. 2008, 35, 668–673. [Google Scholar] [CrossRef]
- Johnston, W.; Rosier, B.T.; Artacho, A.; Paterson, M.; Piela, K.; Delaney, C.; Brown, J.L.; Ramage, G.; Mira, A.; Culshaw, S. Mechanical biofilm disruption causes microbial and immunological shifts in periodontitis patients. Sci. Rep. 2021. Under Review. [Google Scholar]
- Mooney, J.; Adonogianaki, E.; Kinane, D.F. Relative avidity of serum antibodies to putative periodontopathogens in periodontal disease. J. Periodontal Res. 1993, 28, 444–450. [Google Scholar] [CrossRef]
- Rosier, B.T.; Buetas, E.; Moya-Gonzalvez, E.M.; Artacho, A.; Mira, A. Nitrate as a Potential Prebiotic for the Oral Microbiome. Sci. Rep. 2020, 10, 12895. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Davison, E.; Johnston, W.; Piela, K.; Rosier, B.T.; Paterson, M.; Mira, A.; Culshaw, S. The Subgingival Plaque Microbiome, Systemic Antibodies against Bacteria and Citrullinated Proteins following Periodontal Therapy. Pathogens 2021, 10, 193. https://doi.org/10.3390/pathogens10020193
Davison E, Johnston W, Piela K, Rosier BT, Paterson M, Mira A, Culshaw S. The Subgingival Plaque Microbiome, Systemic Antibodies against Bacteria and Citrullinated Proteins following Periodontal Therapy. Pathogens. 2021; 10(2):193. https://doi.org/10.3390/pathogens10020193
Chicago/Turabian StyleDavison, Emily, William Johnston, Krystyna Piela, Bob T. Rosier, Michael Paterson, Alex Mira, and Shauna Culshaw. 2021. "The Subgingival Plaque Microbiome, Systemic Antibodies against Bacteria and Citrullinated Proteins following Periodontal Therapy" Pathogens 10, no. 2: 193. https://doi.org/10.3390/pathogens10020193
APA StyleDavison, E., Johnston, W., Piela, K., Rosier, B. T., Paterson, M., Mira, A., & Culshaw, S. (2021). The Subgingival Plaque Microbiome, Systemic Antibodies against Bacteria and Citrullinated Proteins following Periodontal Therapy. Pathogens, 10(2), 193. https://doi.org/10.3390/pathogens10020193