
Synergistic Combination of AS101 and Azidothymidine against Clinical Isolates of Carbapenem-Resistant Klebsiella pneumoniae

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Antimicrobial Susceptibility Testing
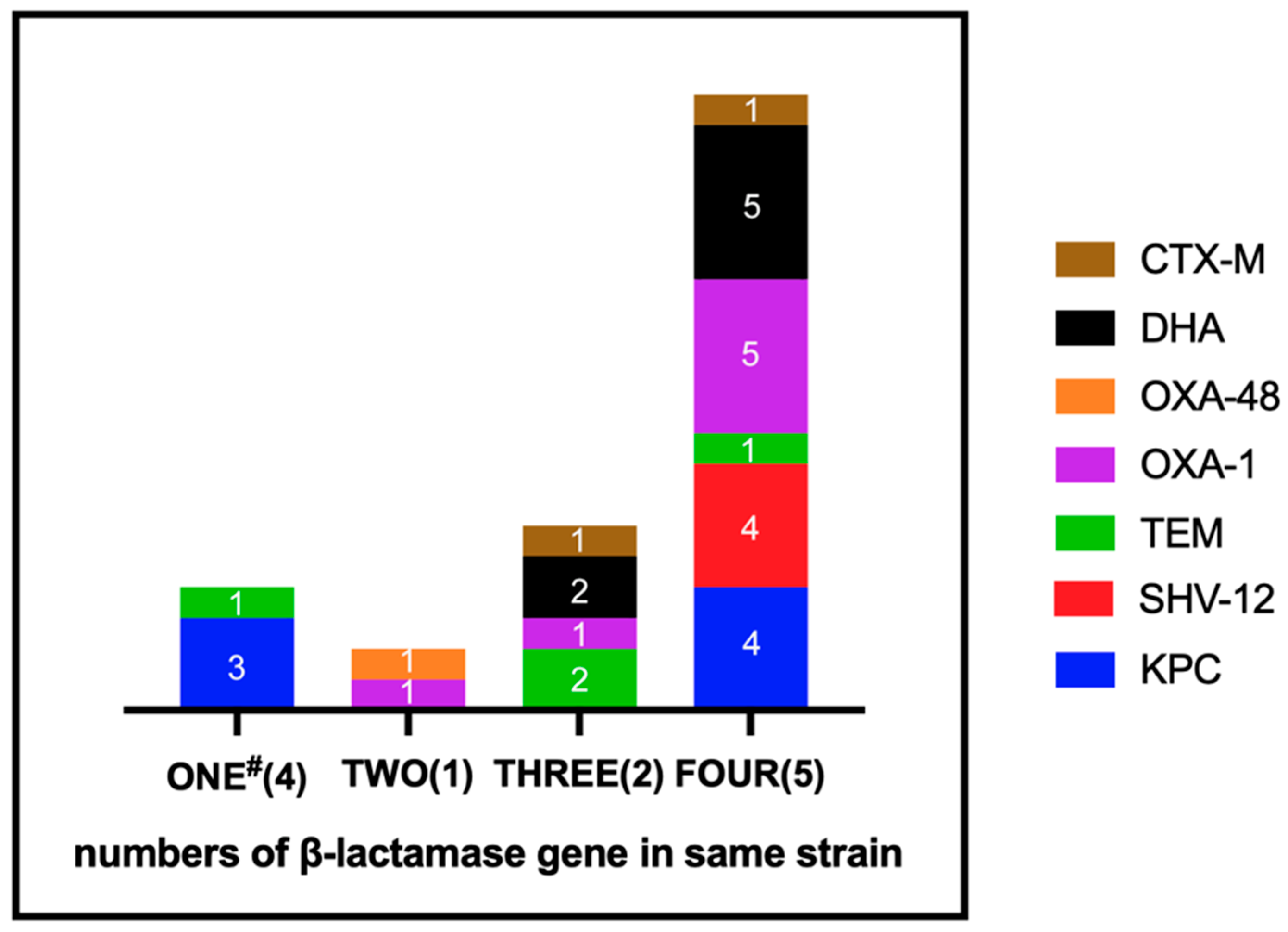
2.2. Detection of Resistance Gene
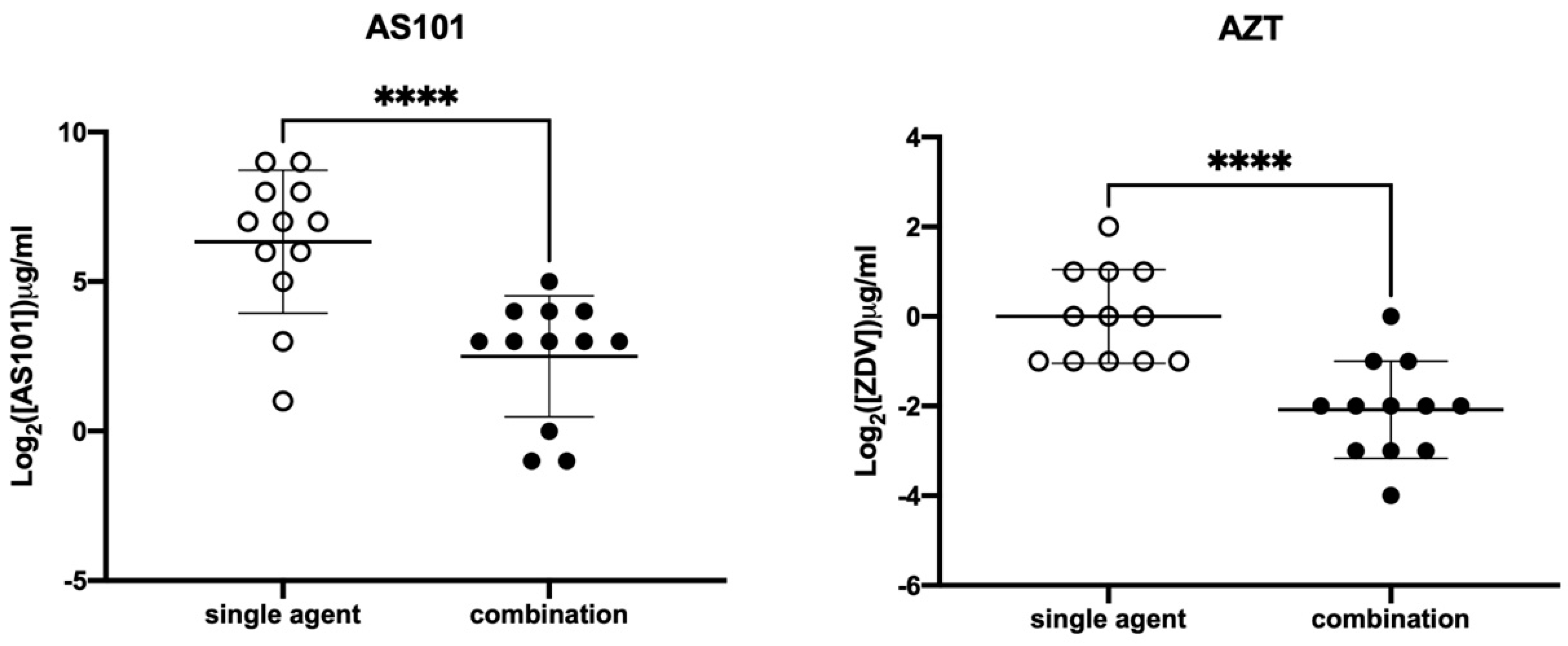
2.3. Evaluation of Synergistic Effects
3. Discussion
4. Materials and Methods
4.1. Bacteria Isolates
4.2. Antimicrobial Susceptibility
4.3. Synergistic Analysis
4.4. Polymerase Chain Reaction Detection
4.5. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery and Development of New Antibiotics. Available online: https://www.who.int/medicines/publications/WHO-PPL-Short_Summary_25Feb-ET_NM_WHO.pdf (accessed on 10 September 2021).
- Tiri, B.; Sensi, E.; Marsiliani, V.; Cantarini, M.; Priante, G.; Vernelli, C.; Martella, L.A.; Costantini, M.; Mariottini, A.; Andreani, P.; et al. Antimicrobial Stewardship Program, COVID-19, and Infection Control: Spread of Carbapenem-Resistant Klebsiella Pneumoniae Colonization in ICU COVID-19 Patients. What Did Not Work? J. Clin. Med. 2020, 9, 2744. [Google Scholar] [CrossRef]
- Nordmann, P.; Poirel, L. Epidemiology and Diagnostics of Carbapenem Resistance in Gram-negative Bacteria. Clin. Infect. Dis. 2019, 69, S521–S528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization; European Centre for Disease Prevention and Control. Antimicrobial Resistance in the EU/EEA (EARS-Net)—Annual Epidemiological Report 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2019#copy-to-clipboard (accessed on 10 September 2021).
- Mendes, R.; Mendoza, M.; Singh, K.K.B.; Castanheira, M.; Bell, J.M.; Turnidge, J.D.; Lin, S.S.F.; Jones, R.N. Regional Resistance Surveillance Program Results for 12 Asia-Pacific Nations (2011). Antimicrob. Agents Chemother. 2013, 57, 5721–5726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.-L.; Lu, M.-C.; Shao, P.-L.; Lu, P.-L.; Chen, Y.-H.; Cheng, S.-H.; Ko, W.-C.; Lin, C.-Y.; Wu, T.-S.; Yen, M.-Y.; et al. Nationwide surveillance of antimicrobial resistance among clinically important Gram-negative bacteria, with an emphasis on carbapenems and colistin: Results from the Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART) in 2018. Int. J. Antimicrob. Agents 2019, 54, 318–328. [Google Scholar] [CrossRef]
- Novelli, A.; Del Giacomo, P.; Rossolini, G.M.; Tumbarello, M. Meropenem/vaborbactam: A next generation β-lactam β-lactamase inhibitor combination. Expert Rev. Anti-Infect. Ther. 2020, 18, 643–655. [Google Scholar] [CrossRef]
- Lai, C.-C.; Chen, C.-C.; Tang, H.-J. Meropenem-Vaborbactam in the Treatment of Acute Bacterial Infections. J. Clin. Med. 2019, 8, 1650. [Google Scholar] [CrossRef] [Green Version]
- Pogue, J.; Bonomo, R.A.; Kaye, K.S. Ceftazidime/Avibactam, Meropenem/Vaborbactam, or Both? Clinical and Formulary Considerations. Clin. Infect. Dis. 2018, 68, 519–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhanel, G.G.; Lawrence, C.; Adam, H.; Schweizer, F.; Zelenitsky, S.; Zhanel, M.; Lagacé-Wiens, P.; Walkty, A.; Denisuik, A.; Golden, A.; et al. Imipenem–Relebactam and Meropenem–Vaborbactam: Two Novel Carbapenem-β-Lactamase Inhibitor Combinations. Drugs 2017, 78, 65–98. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, Y.; Coates, A. Azidothymidine Produces Synergistic Activity in Combination with Colistin against Antibiotic-Resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2019, 63, e01630-18. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.-T.; Yang, T.-Y.; Lu, P.-L.; Lin, S.-Y.; Wang, L.-C.; Wang, S.-F.; Hsieh, Y.-J.; Tseng, S.-P. Combination of Colistin and Azidothymidine Demonstrates Synergistic Activity against Colistin-Resistant, Carbapenem-Resistant Klebsiella pneumoniae. Microorganisms 2020, 8, 1964. [Google Scholar] [CrossRef]
- Antonello, R.M.; Di Bella, S.; Betts, J.; La Ragione, R.; Bressan, R.; Principe, L.; Morabito, S.; Gigliucci, F.; Tozzoli, R.; Busetti, M.; et al. Zidovudine in synergistic combination with fosfomycin: An in vitro and in vivo evaluation against multidrug-resistant Enterobacterales. Int. J. Antimicrob. Agents 2021, 58, 106362. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, N.; Chuachoowong, R.; Mock, P.A.; Bhadrakom, C.; Siriwasin, W.; Young, N.L.; Chotpitayasunondh, T.; Chearskul, S.; Roongpisuthipong, A.; Chinayon, P.; et al. Short-course zidovudine for perinatal HIV-1 transmission in Bangkok, Thailand: A randomised controlled trial. Lancet 1999, 353, 773–780. [Google Scholar] [CrossRef]
- Loose, M.; Naber, K.G.; Hu, Y.; Coates, A.; Wagenlehner, F.M. Urinary bactericidal activity of colistin and azidothymidine combinations against mcr-1-positive colistin-resistant Escherichia coli. Int. J. Antimicrob. Agents 2019, 54, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Shahbazi, F.; Dashti-Khavidaki, S. Colistin: Efficacy and safety in different populations. Expert Rev. Clin. Pharmacol. 2015, 8, 423–448. [Google Scholar] [CrossRef] [PubMed]
- Sredni, B.; Caspi, R.; Klein, A.; Kalechman, Y.; Danziger, Y.; BenYa’Akov, M.; Tamari, T.; Shalit, F.; Albeck, M. A new immunomodulating compound (AS-101) with potential therapeutic application. Nature 1987, 330, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Vázquez-Tato, M.P.; Mena-Menéndez, A.; Feás, X.; Seijas, J.A. Novel Microwave-Assisted Synthesis of the Immunomodulator Organotellurium Compound Ammonium Trichloro(dioxoethylene-O,O′)tellurate (AS101). Int. J. Mol. Sci. 2014, 15, 3287–3298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halpert, G.; Sredni, B. The effect of the novel tellurium compound AS101 on autoimmune diseases. Autoimmun. Rev. 2014, 13, 1230–1235. [Google Scholar] [CrossRef]
- Vonsover, A.; Loya, S.; Sredni, B.; Albeck, M.; Gotlieb-Stematsky, T.; Araf, O.; Hizi, A. Inhibition of the Reverse Transcriptase Activity and Replication of Human Immunodeficiency Virus Type 1 by AS 101 In Vitro. AIDS Res. Hum. Retrovir. 1992, 8, 613–623. [Google Scholar] [CrossRef]
- Indenbaum, V.; Bin, H.; Makarovsky, D.; Weil, M.; Shulman, L.; Albeck, M.; Sredni, B.; Mendelson, E. In vitro and in vivo activity of AS101 against West Nile virus (WNV). Virus Res. 2012, 166, 68–76. [Google Scholar] [CrossRef]
- Yang, T.-Y.; Tseng, S.-P.; Dlamini, H.N.; Lu, P.-L.; Lin, L.; Wang, L.-C.; Hung, W.-C. In Vitro and In Vivo Activity of AS101 against Carbapenem-Resistant Acinetobacter baumannii. Pharmaceuticals 2021, 14, 823. [Google Scholar] [CrossRef]
- Yang, T.-Y.; Kao, H.-Y.; Lu, P.-L.; Chen, P.-Y.; Wang, S.-C.; Wang, L.-C.; Hsieh, Y.-J.; Tseng, S.-P. Evaluation of the Organotellurium Compound AS101 for Treating Colistin- and Carbapenem-Resistant Klebsiella pneumoniae. Pharmaceuticals 2021, 14, 795. [Google Scholar] [CrossRef]
- Daniel-Hoffmann, M.; Albeck, M.; Sredni, B.; Nitzan, Y. A potential antimicrobial treatment against ESBL-producing Klebsiella pneumoniae using the tellurium compound AS101. Arch. Microbiol. 2009, 191, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Daniel-Hoffmann, M.; Sredni, B.; Nitzan, Y. Bactericidal activity of the organo-tellurium compound AS101 against Enterobacter cloacae. J. Antimicrob. Chemother. 2012, 67, 2165–2172. [Google Scholar] [CrossRef]
- Patel, G.; Huprikar, S.; Factor, S.H.; Jenkins, S.G.; Calfee, D.P. Outcomes of Carbapenem-Resistant Klebsiella pneumoniae Infection and the Impact of Antimicrobial and Adjunctive Therapies. Infect. Control. Hosp. Epidemiol. 2008, 29, 1099–1106. [Google Scholar] [CrossRef]
- Antibiotic Resistance Threats in the United States. 2013. Available online: https://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf (accessed on 10 September 2021).
- Chiu, S.-K.; Ma, L.; Chan, M.-C.; Lin, Y.-T.; Fung, C.-P.; Wu, T.-L.; Chuang, Y.-C.; Lu, P.-L.; Wang, J.-T.; Lin, J.-C.; et al. Carbapenem Nonsusceptible Klebsiella pneumoniae in Taiwan: Dissemination and Increasing Resistance of Carbapenemase Producers During 2012–2015. Sci. Rep. 2018, 8, 8468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Duin, D.; Perez, F.; Rudin, S.D.; Cober, E.; Hanrahan, J.; Ziegler, J.; Webber, R.; Fox, J.; Mason, P.; Richter, S.S.; et al. Surveillance of Carbapenem-Resistant Klebsiella pneumoniae: Tracking Molecular Epidemiology and Outcomes through a Regional Network. Antimicrob. Agents Chemother. 2014, 58, 4035–4041. [Google Scholar] [CrossRef] [Green Version]
- Han, J.H.; Goldstein, E.J.; Wise, J.; Bilker, W.B.; Tolomeo, P.; Lautenbach, E. Epidemiology of Carbapenem-Resistant Klebsiella pneumoniae in a Network of Long-Term Acute Care Hospitals. Clin. Infect. Dis. 2016, 64, 839–844. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, N.; Rezaee, M.A.; Kafil, H.S.; Hasani, A.; Barhaghi, M.H.S.; Milani, M.; Sefidan, F.Y.; Memar, M.Y.; Lalehzadeh, A.; Ghotaslou, R. Evaluation of Resistance Mechanisms in Carbapenem-Resistant Enterobacteriaceae. Infect. Drug Resist. 2020, 13, 1377–1385. [Google Scholar] [CrossRef]
- Elshamy, A.A.; Aboshanab, K.M. A review on bacterial resistance to carbapenems: Epidemiology, detection and treatment options. Futur. Sci. OA 2020, 6, FSO438. [Google Scholar] [CrossRef] [Green Version]
- Codjoe, F.S.; Donkor, E.S. Carbapenem Resistance: A Review. Med. Sci. 2017, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- David, S.; Reuter, S.; Harris, S.R.; Glasner, C.; Feltwell, T.; Argimon, S.; Abudahab, K.; Goater, R.; Giani, T.; Errico, G.; et al. Epidemic of carbapenem-resistant Klebsiella pneumoniae in Europe is driven by nosocomial spread. Nat. Microbiol. 2019, 4, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- Doi, Y. Treatment Options for Carbapenem-resistant Gram-negative Bacterial Infections. Clin. Infect. Dis. 2019, 69, S565–S575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Thirtieth Informational Supplement; Document M100-S130 CLSI; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2020. [Google Scholar]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and Zone Diameters. Version 11.0, 2021. Available online: http://www.eucast.org (accessed on 10 September 2021).
- Tseng, S.-P.; Wang, S.-F.; Ma, L.; Wang, T.-Y.; Yang, T.-Y.; Siu, L.K.; Chuang, Y.-C.; Lee, P.-S.; Wang, J.-T.; Wu, T.-L.; et al. The plasmid-mediated fosfomycin resistance determinants and synergy of fosfomycin and meropenem in carbapenem-resistant Klebsiella pneumoniae isolates in Taiwan. J. Microbiol. Immunol. Infect. 2017, 50, 653–661. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Antimicrobial Agent | Antibiotic Susceptibility 1 | ||
|---|---|---|---|
| S | I | R | |
| Amikacin | 66.7% | 0.0% | 33.3% |
| Ampicillin | 0.0% | 0.0% | 100.0% |
| Aztreonam | 16.7% | 0.0% | 83.3% |
| Ceftazidime | 0.0% | 8.3% | 91.7% |
| Cefazolin | 0.0% | 0.0% | 100.0% |
| Ciprofloxacin | 0.0% | 0.0% | 100.0% |
| Cefepime | 0.0% | 16.7% | 83.3% |
| Cefoxitin | 0.0% | 0.0% | 100.0% |
| Ceftriaxone | 0.0% | 0.0% | 100.0% |
| Cefotaxime | 8.3% | 0.0% | 91.7% |
| Gentamicin | 41.7% | 0.0% | 58.3% |
| Imipenem | 0.0% | 0.0% | 100.0% |
| Levofloxacin | 0.0% | 0.0% | 100.0% |
| Meropenem | 0.0% | 0.0% | 100.0% |
| Trimethoprim/Sulfamethoxazole | 8.3% | 0.0% | 91.7% |
| Piperacillin–Tazobactam | 8.3% | 0.0% | 91.7% |
| Ertapenem | 0.0% | 0.0% | 100.0% |
| Tigecycline | 91.7% | 8.3% | 0.0% |
| Doripenem | 0.0% | 0.0% | 100.0% |
| Agent | MIC Alone * (μg/mL) | MIC in Combination # (μg/mL) | ||||||
|---|---|---|---|---|---|---|---|---|
| Range | MIC50 | MIC75 | MIC90 | Range | MIC50 | MIC75 | MIC90 | |
| AS101 | 2–512 | 128 | 256 | 512 | 0.5–32 | 8 | 16 | 16 |
| AZT | 0.5–4 | 1 | 2 | 2 | 0.0625–1 | 0.25 | 0.25 | 0.5 |
| Strains | MIC Alone * (μg/mL) | MIC in Combination # (μg/mL) | FICI | Interpretation | ||
|---|---|---|---|---|---|---|
| AS101 | AZT | AS101 | AZT | (AS101, AZT) | ||
| CRE-918 | 128 | 0.5 | 0.5 | 0.25 | 0.5 | synergistic |
| CRE-949 | 256 | 1 | 8 | 0.25 | 0.28 | synergistic |
| CRE-1017 | 64 | 2 | 8 | 0.5 | 0.38 | synergistic |
| CRE-1038 | 256 | 0.5 | 16 | 0.125 | 0.31 | synergistic |
| CRE-1044 | 512 | 0.5 | 16 | 0.0625 | 0.16 | synergistic |
| CRE-1085 | 32 | 2 | 8 | 0.25 | 0.38 | synergistic |
| CRE-1086 | 128 | 2 | 16 | 0.5 | 0.38 | synergistic |
| CRE-1125 | 2 | 1 | 0.5 | 0.25 | 0.5 | synergistic |
| CRE-1136 | 128 | 1 | 32 | 0.25 | 0.5 | synergistic |
| CRE-1290 | 64 | 0.5 | 8 | 0.125 | 0.38 | synergistic |
| CRE-1382 | 512 | 0.5 | 8 | 0.125 | 0.27 | synergistic |
| CRE-1536 | 8 | 4 | 1 | 1 | 0.38 | synergistic |
| Isolation Source | No. of Isolates (%) |
|---|---|
| Abscess | 1 (8.3) |
| Blood | 1 (8.3) |
| Sputum | 4 (33.3) |
| Urine | 5 (41.7) |
| Deep wound | 1 (8.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, C.-L.; Hung, W.-C.; Lu, P.-L.; Lin, L.; Wang, L.-C.; Yang, T.-Y.; Tseng, S.-P. Synergistic Combination of AS101 and Azidothymidine against Clinical Isolates of Carbapenem-Resistant Klebsiella pneumoniae. Pathogens 2021, 10, 1552. https://doi.org/10.3390/pathogens10121552
Sung C-L, Hung W-C, Lu P-L, Lin L, Wang L-C, Yang T-Y, Tseng S-P. Synergistic Combination of AS101 and Azidothymidine against Clinical Isolates of Carbapenem-Resistant Klebsiella pneumoniae. Pathogens. 2021; 10(12):1552. https://doi.org/10.3390/pathogens10121552
Chicago/Turabian StyleSung, Chung-Lin, Wei-Chun Hung, Po-Liang Lu, Lin Lin, Liang-Chun Wang, Tsung-Ying Yang, and Sung-Pin Tseng. 2021. "Synergistic Combination of AS101 and Azidothymidine against Clinical Isolates of Carbapenem-Resistant Klebsiella pneumoniae" Pathogens 10, no. 12: 1552. https://doi.org/10.3390/pathogens10121552
APA StyleSung, C.-L., Hung, W.-C., Lu, P.-L., Lin, L., Wang, L.-C., Yang, T.-Y., & Tseng, S.-P. (2021). Synergistic Combination of AS101 and Azidothymidine against Clinical Isolates of Carbapenem-Resistant Klebsiella pneumoniae. Pathogens, 10(12), 1552. https://doi.org/10.3390/pathogens10121552