
The Influence of Thermal History and Air Conditioner Use Behavior Under Different Cooling Set Point Temperature Modes on Health



Abstract
1. Introduction
1.1. Energy-Saving Policy and Health
1.2. Indoor Thermal History and Thermoregulatory Capacity
1.3. Behavior and IAQ
1.4. Study Aims
2. Methods
2.1. Experimental Scheme
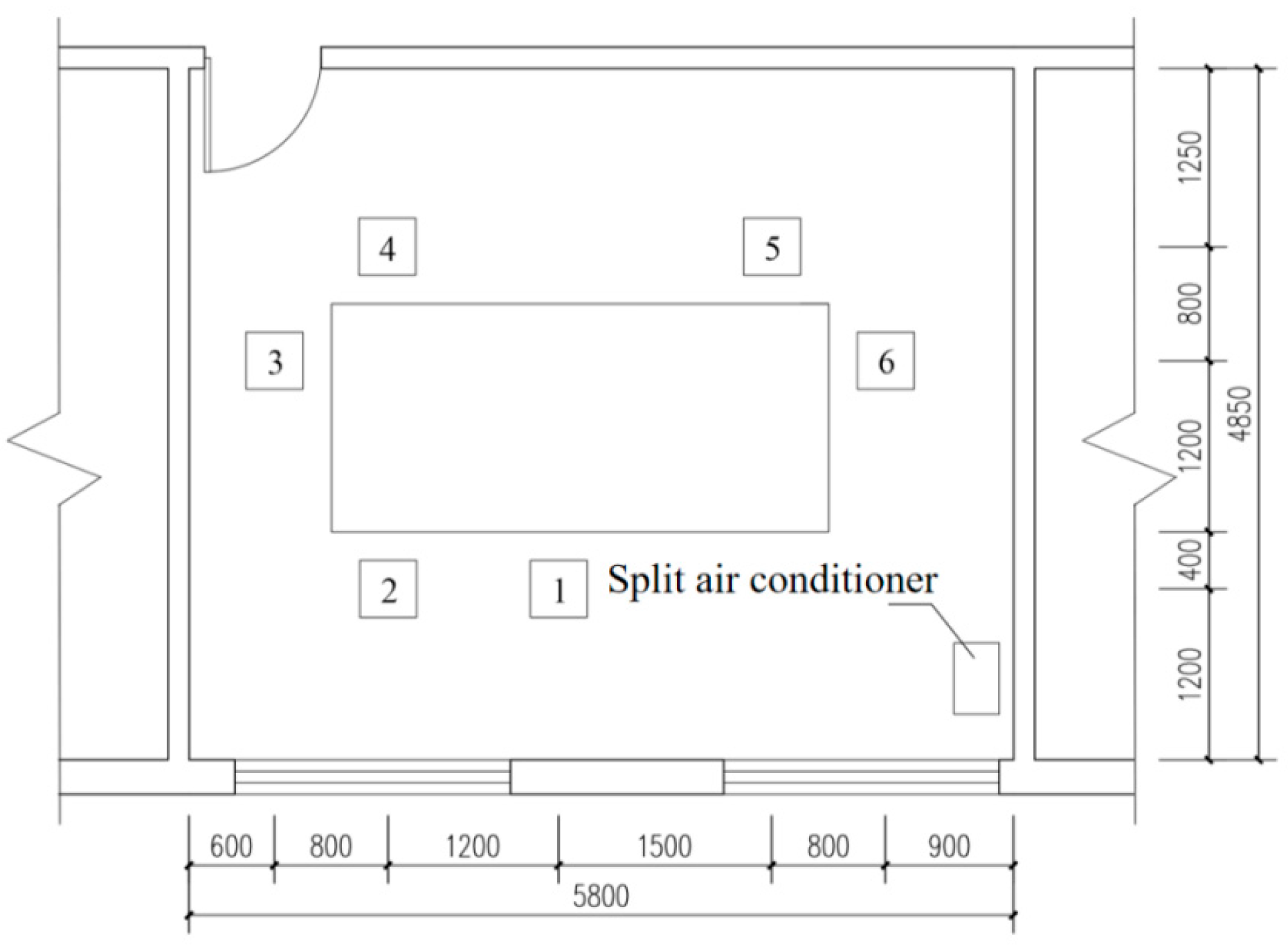
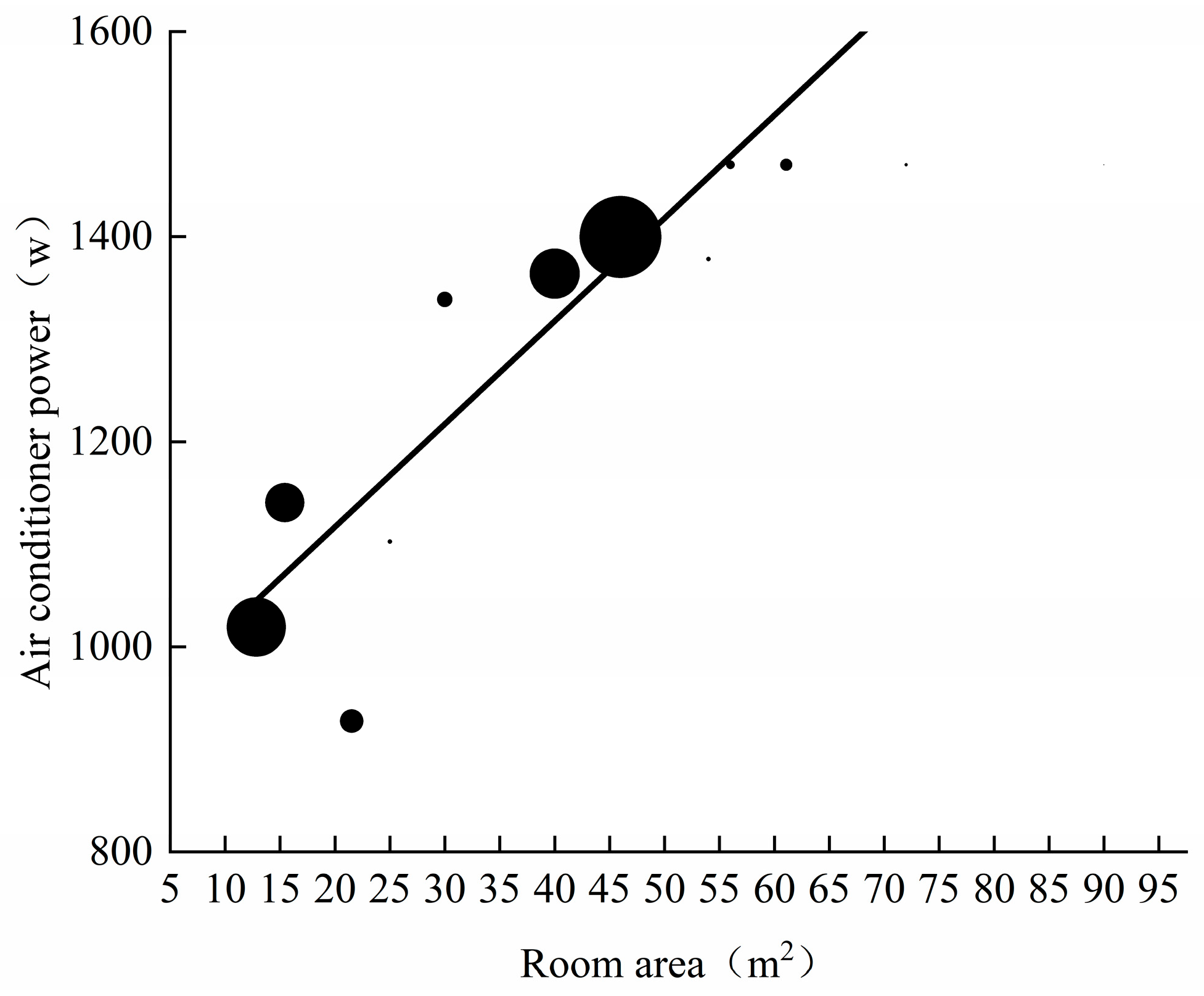
2.1.1. Experimental Room
2.1.2. Subject Information
2.1.3. Test Content and Instrument
Environmental Parameter Measurement
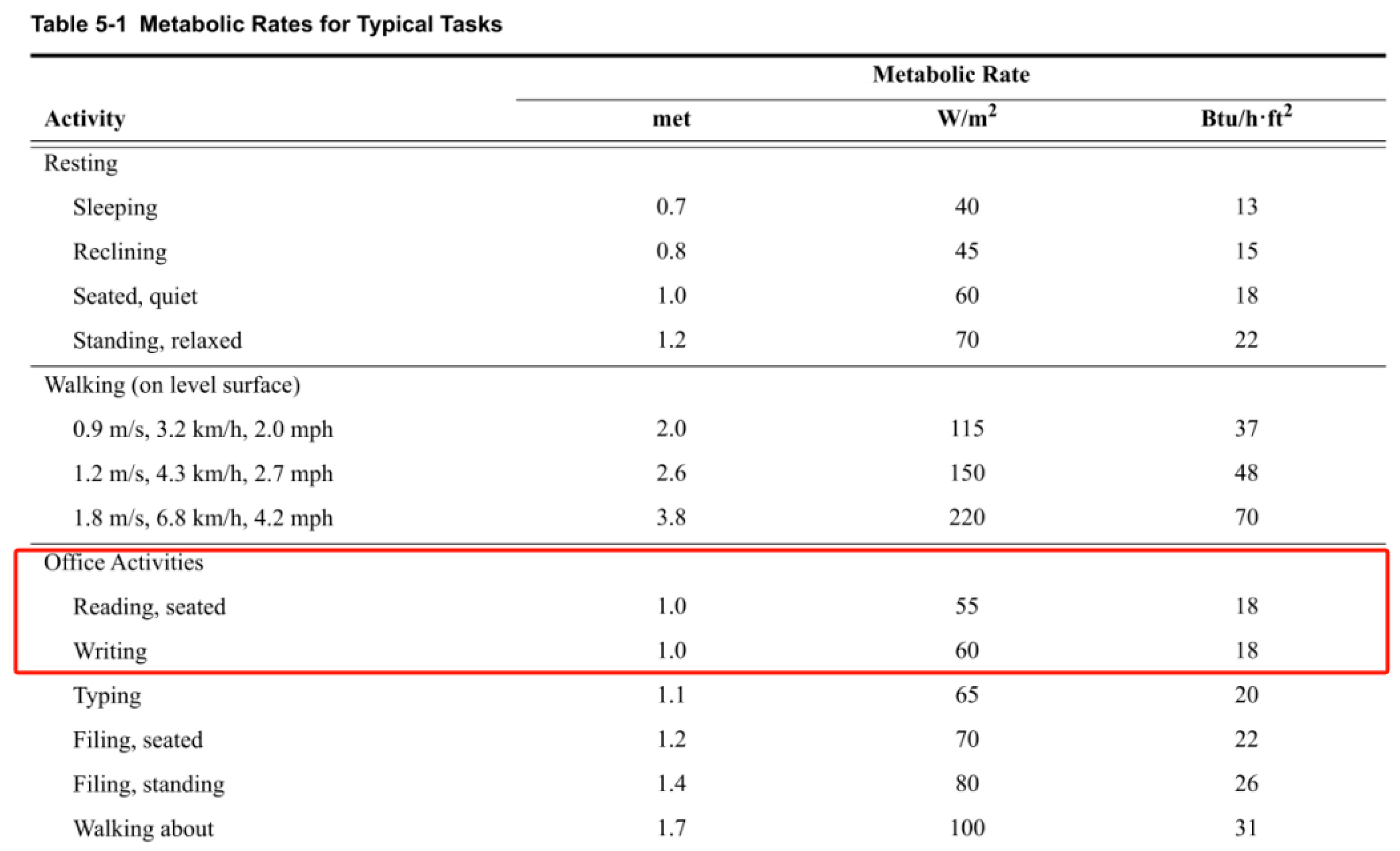
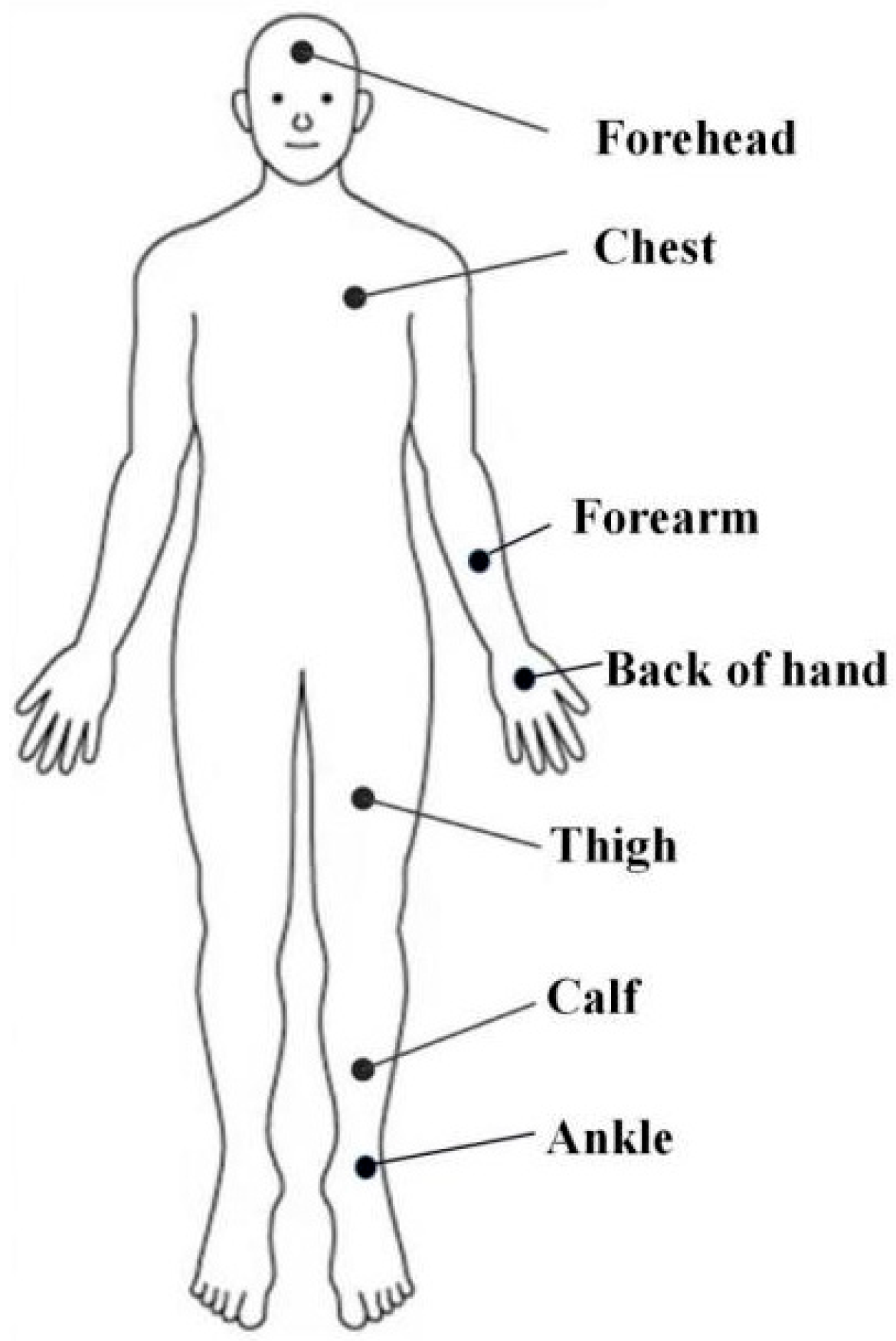
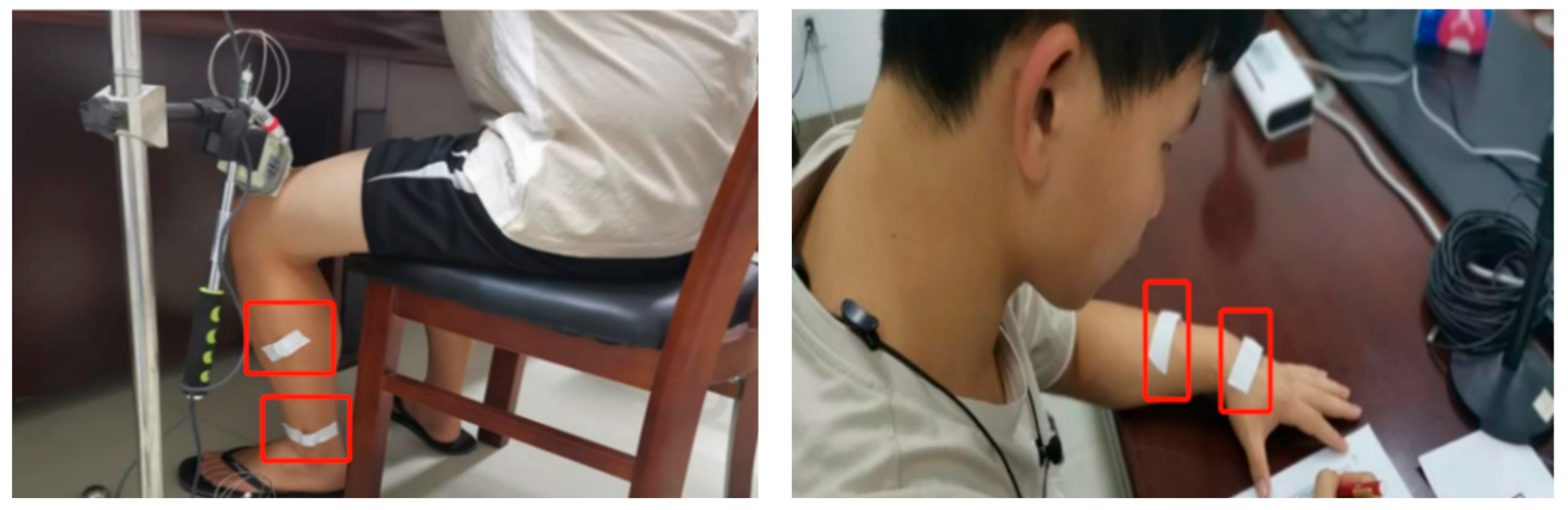
Physiological Parameter Measurement
2.1.4. Experimental Design
Experimental Conditions
Experimental Procedure
2.2. Field Investigation Scheme
2.2.1. Buildings and Subjects
2.2.2. Investigation Content and Instruments
2.2.3. Data Collection
2.3. Data Processing
3. Results
3.1. Experimental Results: Thermal History and Thermal Responses
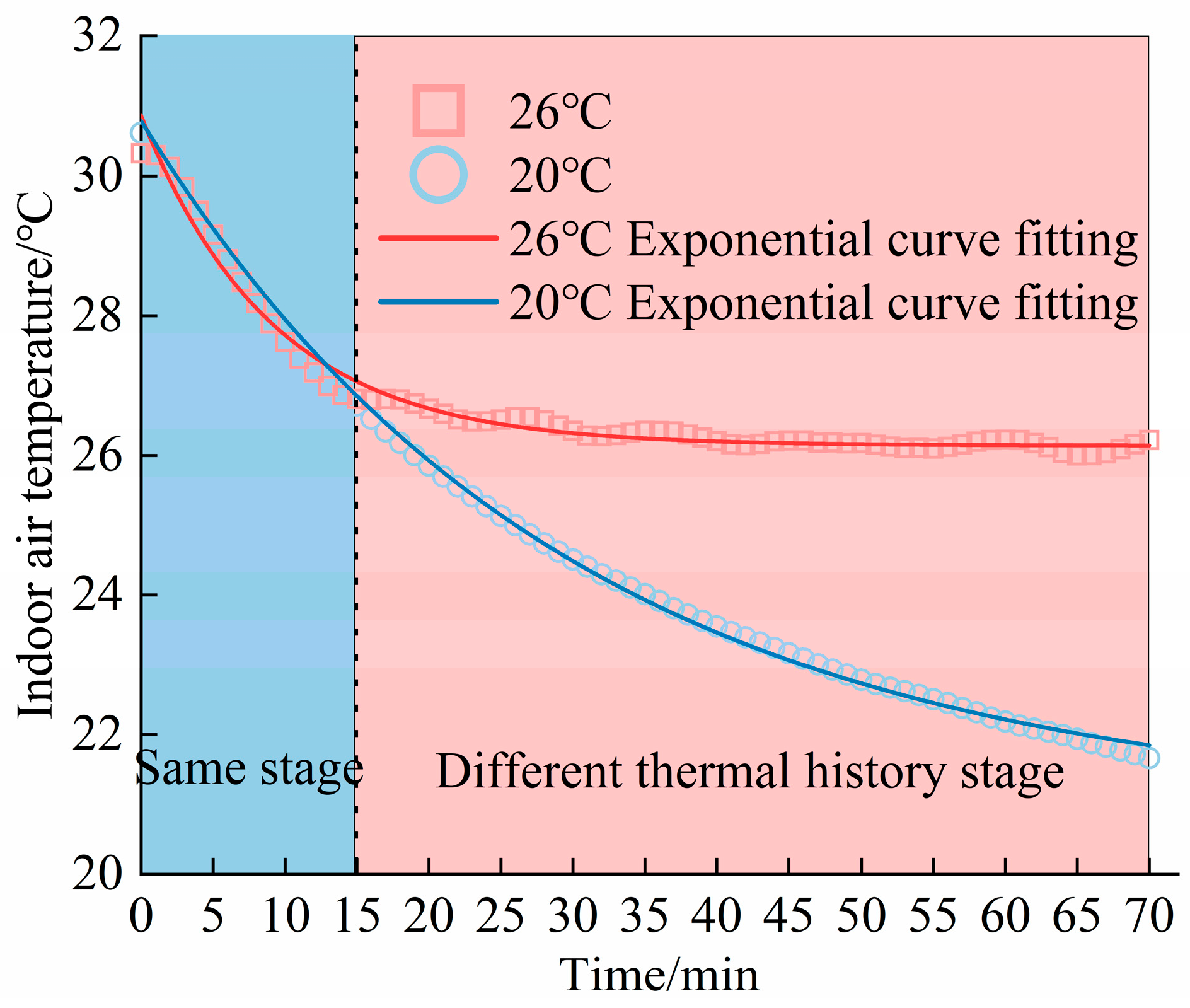
3.1.1. Thermal History
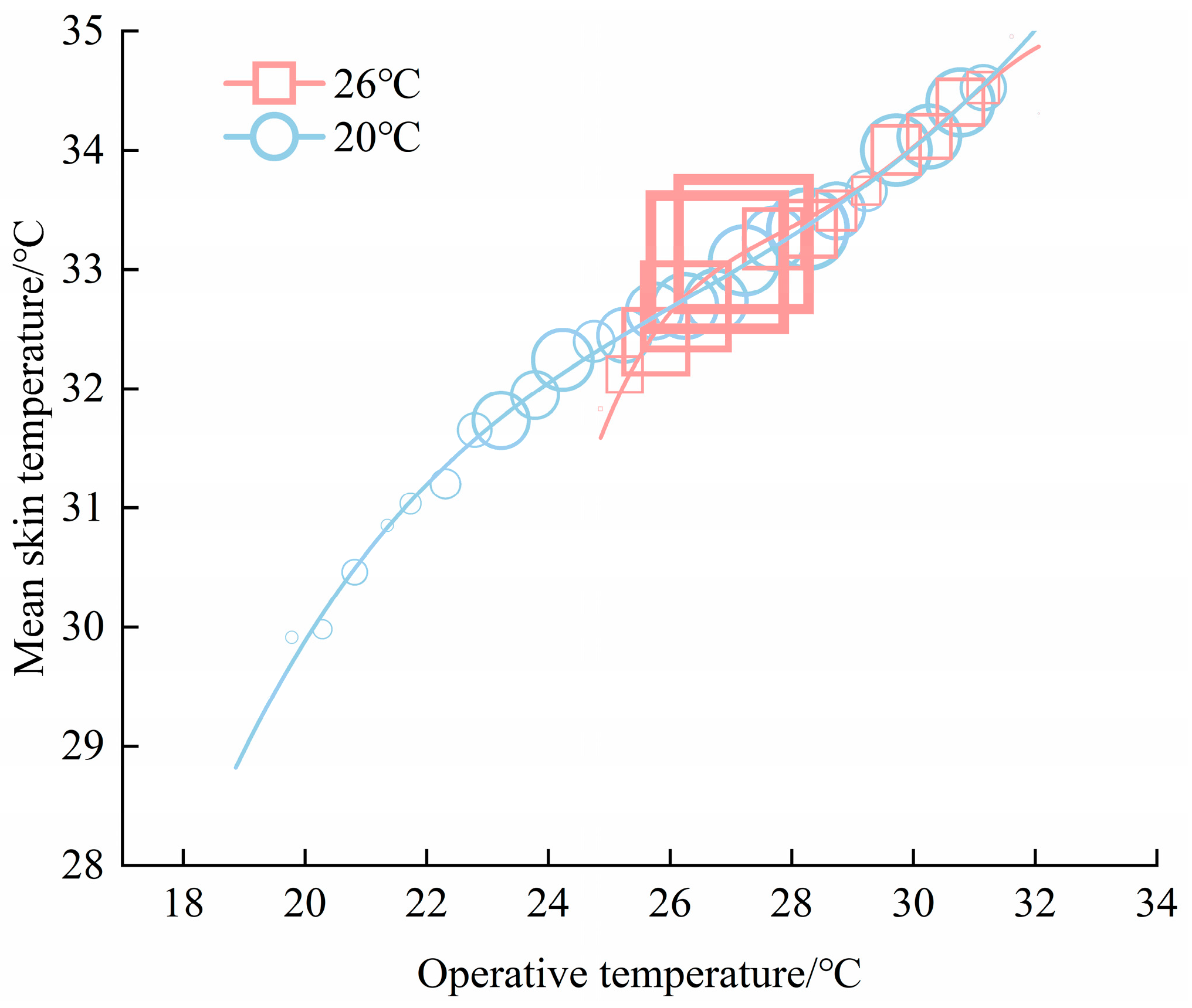
3.1.2. Physiological Responses
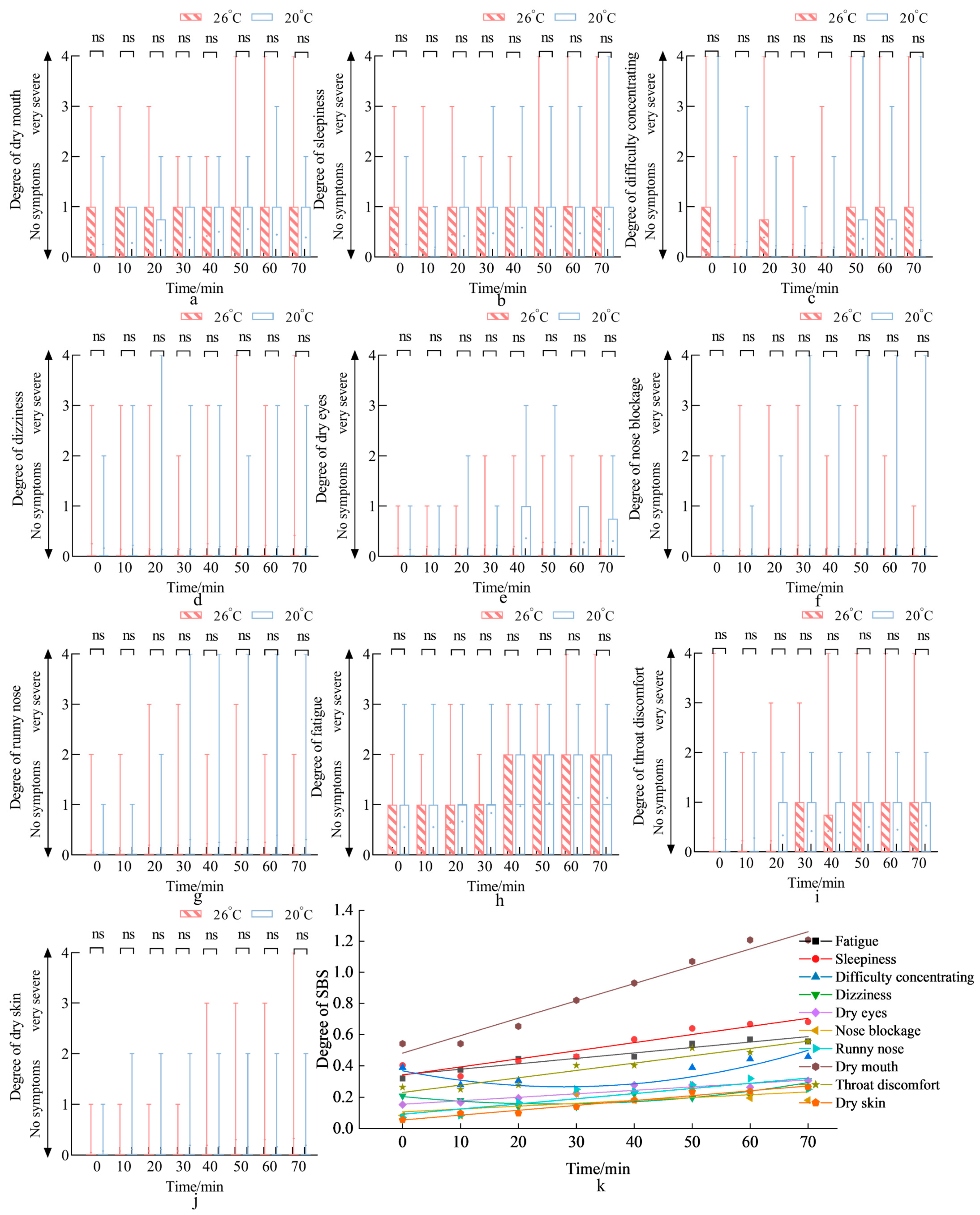
3.1.3. Sick Building Syndrome (SBS)
3.2. Field Investigation Results: Air Conditioner Use Behavior and IAQ
3.2.1. Air Conditioner Use Behavior
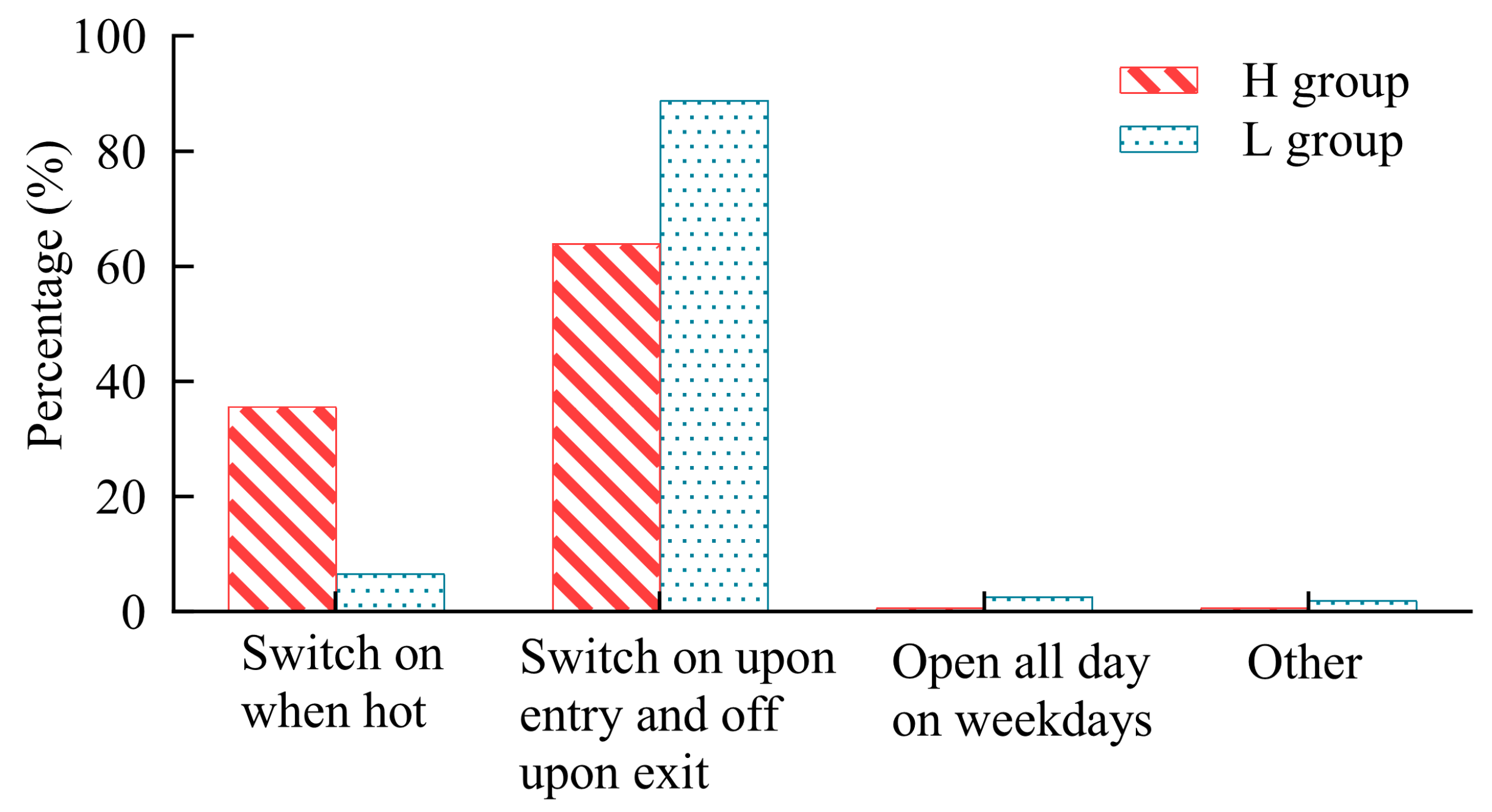
Air Conditioner Use Modes
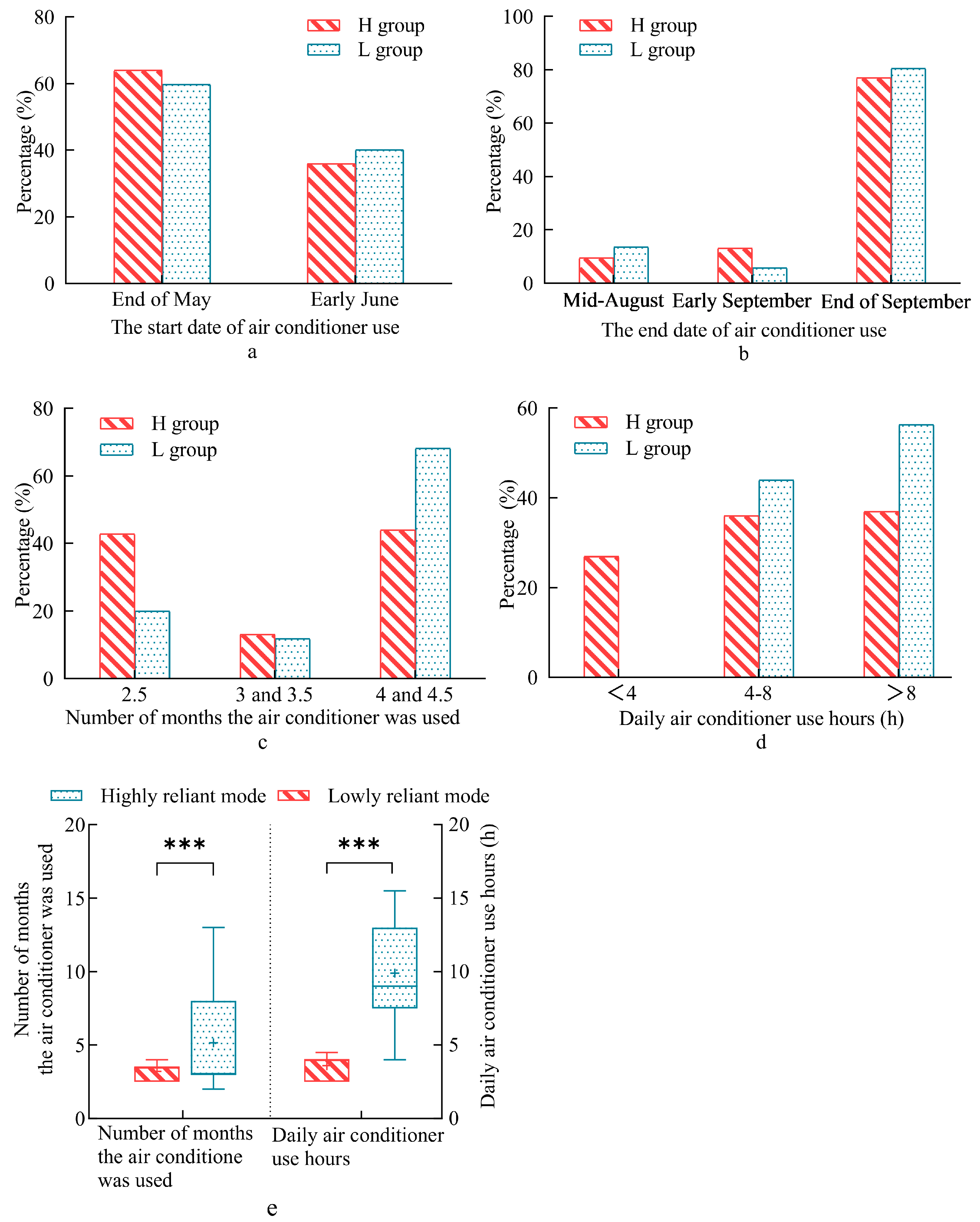
Air Conditioner Use Time
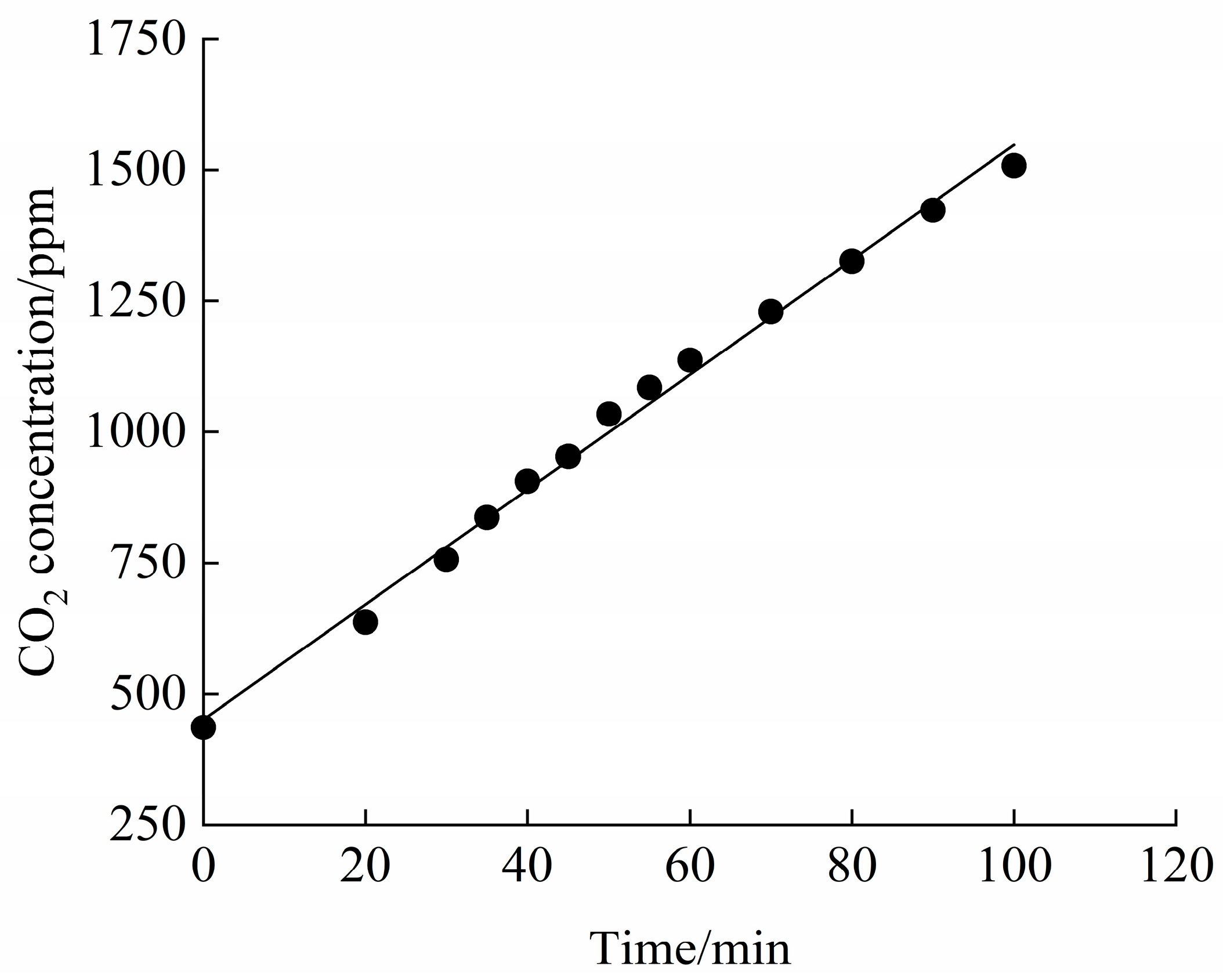
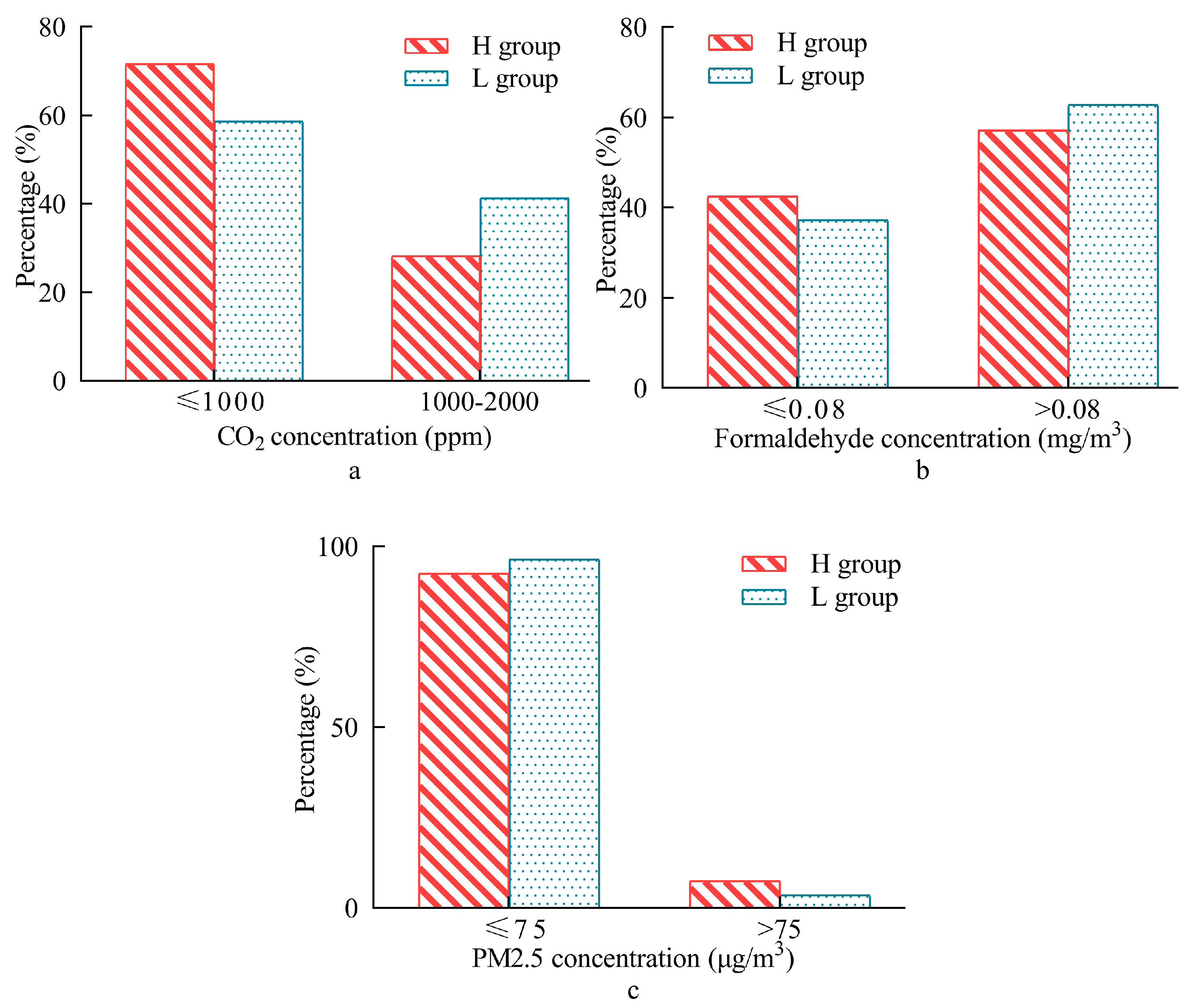
3.2.2. Differences in IAQ
3.2.3. Health Risk Assessment of Formaldehyde Exposure
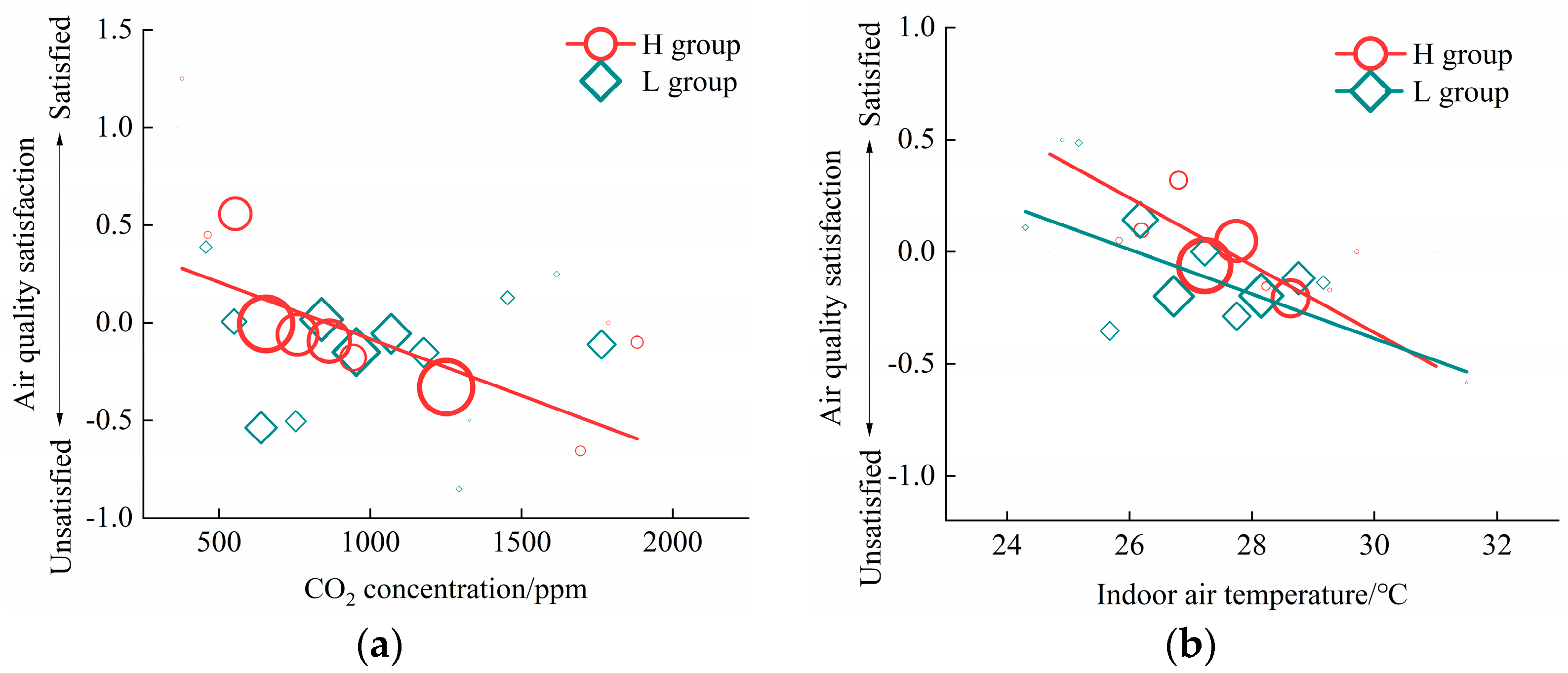
3.2.4. Air Quality Satisfaction
4. Discussion
4.1. Influence of Thermal History of Different SPT Modes on Physiology
4.2. Influence of Air Conditioner Use Behavior of Different SPT Modes on IAQ
4.3. Influence of Long-Term Thermal and Air History of Different SPT Modes on Air Quality Perception
4.4. Influence and Mechanisms of Different SPT Modes on Health
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- China Building Energy Efficiency Association; Chongqing University. Research Report on Carbon Emissions from Urban and Rural Construction in China, 2024th ed.; China Building Energy Efficiency Association; Chongqing University: Chongqing, China, 2025. [Google Scholar]
- Zhuang, X.; Wu, C. Saving Energy when Using Air Conditioners in Offices—Behavioral Pattern and Design Indications. Energy Build. 2014, 76, 661–668. [Google Scholar] [CrossRef]
- Yan, H.; Shi, F.; Sun, Z.; Yuan, G.; Wang, M.; Dong, M. Thermal Adaptation of Different Set Point Temperature Modes and Energy Saving Potential in Split Air-Conditioned Office Buildings during Summer. Build. Environ. 2022, 225, 109565. [Google Scholar] [CrossRef]
- Zhou, X.; Xu, L.; Xie, J.; He, L.; Zhang, J.; Wu, Z.; Pan, Y. Personnel Movement and Air Conditioner Usage Behavior for a University Office in Shanghai. Build. Sci. 2020, 36, 1–7+73. (In Chinese) [Google Scholar]
- Bae, C.; Chun, C. Research on Seasonal Indoor Thermal Environment and Residents’ Control Behavior of Cooling and Heating Systems in Korea. Build. Environ. 2009, 44, 2300–2307. [Google Scholar] [CrossRef]
- Yu, J.; Ouyang, Q.; Zhu, Y.; Shen, H.; Cao, G.; Cui, W. A Comparison of the Thermal Adaptability of People Accustomed to Air-Conditioned Environments and Naturally Ventilated Environments. Indoor Air 2012, 22, 110–118. [Google Scholar] [CrossRef]
- Wu, Z.; Li, N.; Wargocki, P.; Peng, J.; Li, J.; Cui, H. Field Study on Thermal Comfort and Energy Saving Potential in 11 Split Air-Conditioned Office Buildings in Changsha, China. Energy 2019, 182, 471–482. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, Y.; Khan, A. Thermal Comfort of People from Two Types of Air-Conditioned Buildings—Evidences from Chamber Experiments. Build. Environ. 2019, 162, 106287. [Google Scholar] [CrossRef]
- Kravchenko, I.; Velashjerdi Farahani, A.; Kosonen, R.; Kilpeläinen, S.; Saranko, O.; Fortelius, C. Effect of the Urban Microenvironment on the Indoor Air Temperature of the Residential Building Stock in the Helsinki Region. Build. Environ. 2023, 246, 110971. [Google Scholar] [CrossRef]
- Guo, F.; Ham, S.W.; Kim, D.; Moon, H.J. Deep Reinforcement Learning Control for Co-Optimizing Energy Consumption, Thermal Comfort, and Indoor Air Quality in an Office Building. Appl. Energy 2025, 377, 124467. [Google Scholar] [CrossRef]
- Poulin, P.; Marchand, A.; Lévesque, B.; Dubé, M.; Aubin, D.; Ouazia, B.; Duchaine, C.; Brisson, M. Impact of Improved Indoor Air Quality in Nunavik Homes on Children’s Respiratory Health. Indoor Air 2022, 32, e13009. [Google Scholar] [CrossRef]
- Lovas, S.; Pál, L.; Kovács, N.; Diószegi, J.; McKee, M.; Szűcs, S. Dataset on Concentrations of Volatile Organic Compounds in Indoor Environments of Offices, Educational and Residential Buildings in the European Union between 2010 and 2023. Data Brief 2024, 57, 111070. [Google Scholar] [CrossRef] [PubMed]
- Ge, B.; Tieskens, K.; Vyas, P.; Botana Martinez, M.P.; Yuan, Y.; Walsh, K.H.; Main, L.; Bolton, L.; Yajima, M.; Fabian, M.P. Decision Tools for Schools Using Continuous Indoor Air Quality Monitors: A Case Study of CO2 in Boston Public Schools. Lancet Reg. Health–Am. 2025, 48, 101148. [Google Scholar] [CrossRef]
- Jung, D.; Choe, Y.; Shin, J.; Kim, E.; Min, G.; Kim, D.; Cho, M.; Lee, C.; Choi, K.; Woo, B.L.; et al. Risk Assessment of Indoor Air Quality and Its Association with Subjective Symptoms among Office Workers in Korea. Int. J. Environ. Res. Public Health 2022, 19, 2446. [Google Scholar] [CrossRef]
- Sérafin, G.; Blondeau, P.; Mandin, C. Indoor Air Pollutant Health Prioritization in Office Buildings. Indoor Air 2020, 31, 646–659. [Google Scholar] [CrossRef]
- Salthammer, T. Formaldehyde Sources, Formaldehyde Concentrations and Air Exchange rates in European Housings. Build. Environ. 2019, 150, 219–232. [Google Scholar] [CrossRef]
- Nielsen, G.D.; Larsen, S.T.; Wolkoff, P. Recent Trend in Risk Assessment of Formaldehyde Exposures from Indoor Air. Arch. Toxicol. 2013, 87, 73–98. [Google Scholar] [CrossRef]
- Kulshreshtha, P.; Khare, M.; Seetharaman, P. Indoor Air Quality Assessment in and around Urban Slums of Delhi City, India. Indoor Air 2008, 18, 488–498. [Google Scholar] [CrossRef]
- Azuma, K.; Ikeda, K.; Kagi, N.; Yanagi, U.; Osawa, H. Physicochemical Risk Factors for Building-Related Symptoms in Air-Conditioned Office Buildings: Ambient Particles and Combined Exposure to Indoor Air Pollutants. Sci. Total Environ. 2018, 616–617, 1649–1655. [Google Scholar] [CrossRef]
- Yoon, H.; Shuai, J.F.; Kim, T.; Seo, J.; Jung, D.; Ryu, H.; Yang, W. Micro-Environmental Time Activity Patterns of Weekday and Weekend on Korean Adults. J. Odor. Indoor. Environ. 2017, 16, 182–186. [Google Scholar] [CrossRef]
- Cheng, Z.; Lei, N.; Bu, Z.; Sun, H.; Li, B.; Lin, B. Investigations of Indoor Air Quality for Office Buildings in Different Climate Zones of China by Subjective Survey and Field Measurement. Build. Environ. 2022, 214, 108899. [Google Scholar] [CrossRef]
- Alonso, M.J.; Jørgensen, R.B.; Mathisen, H.M. Short Term Measurements of Indoor Air Quality when Using the Home Office in Norway. E3S Web Conf. 2021, 246, 01002. [Google Scholar] [CrossRef]
- Qiu, Y.; Wang, Y.; Tang, Y. Investigation of Indoor Air Quality in Six Office Buildings in Chengdu, China Based on Field Measurements. Build. Simul. 2020, 13, 1009–1020. [Google Scholar] [CrossRef]
- Chiesa, G.; Vigliotti, M. Comparing Mechanical Ventilation Control Strategies for Indoor Air Quality: Monitoring and Simulation Results of a School Building in Northern Italy. Energy Build. 2024, 322, 114665. [Google Scholar] [CrossRef]
- Carrer, P.; De Oliveira Fernandes, E.; Santos, H.; Hänninen, O.; Kephalopoulos, S.; Wargocki, P. On the Development of Health-Based Ventilation Guidelines: Principles and Framework. Int. J. Environ. Res. Public Health 2018, 15, 1360. [Google Scholar] [CrossRef]
- Sekhar, S.C.; Lim, A.H. Indoor Air Quality and Energy Issues of Refrigerant Modulating Air-Conditioning Systems in the Tropics. Build. Environ. 2003, 38, 815–825. [Google Scholar] [CrossRef]
- Licina, D.; Langer, S. Indoor Air Quality Investigation before and after Relocation to WELL-Certified Office Buildings. Build. Environ. 2021, 204, 108182. [Google Scholar] [CrossRef]
- Vergerio, G.; Becchio, C. Pursuing Occupants’ Health and Well-Being in Building Management: Definition of New Metrics Based on Indoor Air Parameters. Build. Environ. 2022, 223, 109447. [Google Scholar] [CrossRef]
- Schweiker, M.; Shukuya, M. Comparison of Theoretical and Statistical Models of Air-Conditioning-Unit Usage Behaviour in a Residential Setting Under Japanese Climatic Conditions. Build. Environ. 2009, 44, 2137–2149. [Google Scholar] [CrossRef]
- Yaglou, C.P.; Riley, E.C.; Coggins, D.I. Ventilation Requirements. ASHVE Trans. 1936, 42, 133–162. [Google Scholar]
- Park, J.; Loftness, V.; Aziz, A.; Wang, T.H. Critical Factors and Thresholds for User Satisfaction on Air Quality in Office Environments. Build. Environ. 2019, 164, 106310. [Google Scholar] [CrossRef]
- Peter, W.; Peter, T.; Ute, M.; Bernhard, D.; Anna, W.; Michael, K.; Hans-Peter, H. Health and Wellbeing of Occupants in Highly Energy Efficient Buildings: A Field Study. Int. J. Environ. Res. Public Health 2017, 14, 314. [Google Scholar] [CrossRef]
- GB 50176; Code for Thermal Design of Civil Building. Ministry of Housing and Urban-Rural Development of the People’s Republic of China: Beijing, China, 2016.
- Lan, L.; Lian, Z. Application of Statistical Power Analysis–How to Determine The Right Sample Size in Human Health, Comfort and Productivity Research. Build. Environ. 2010, 45, 1202–1213. [Google Scholar] [CrossRef]
- ANSI/ASHRAE Standard 55-2023; Thermal Environmental Conditions for Human Occupancy. American Society of Heating, Refrigerating and Air-Conditioning Engineers: Atlanta, GA, USA, 2023.
- ISO 7726; Ergonomics of the Thermal Environment—Instruments for Measuring Physical Quantities. International Organization for Standardization: Geneva, Switzerland, 2001.
- Lin, Y.; Yang, L.; Luo, M. Physiological and Subjective Thermal Responses to Heat Exposure in Northern and Southern Chinese People. Build. Simul. 2021, 14, 1619–1631. [Google Scholar] [CrossRef]
- Yang, Y. Body Temperature and Thermoregulatory Physiology; People’s Military Medical Publishing House: Beijing, China, 2015. [Google Scholar]
- Castellani, J.; Young, A. Human Physiological Responses to Cold Exposure: Acute Responses and Acclimatization to Prolonged Exposure. Auton. Neurosci. 2016, 196, 63–74. [Google Scholar] [CrossRef]
- Choi, J.; Miki, K.; Sagawa, S.; Shiraki, K. Evaluation of Mean Skin Temperature Formulas by Infrared Thermography. Int. J. Biometeorol. 1997, 41, 68–75. [Google Scholar] [CrossRef]
- Mitchell, D.; Wyndham, C. Comparison of Weighting Formulas for Calculating Mean Skin Temperature. J. Appl. Physiol. 1969, 26, 616–622. [Google Scholar] [CrossRef]
- He, Y.; Li, N.; Zhang, H.; Zhou, L. Air-conditioning Use Behaviors when Elevated Air Movement Is Available. Energy Build. 2020, 225, 110370. [Google Scholar] [CrossRef]
- ASHRAE. Handbook of Fundamentals; American Society of Heating, Refrigerating and Air-Conditioning Engineers Inc.: Atlanta, GA, USA, 2017. [Google Scholar]
- Hui, Y.; Tang, Y.; Yang, Q.; Mochida, A. Numerical Study on Influence of Surface Vegetation on Aerodynamics of High-Rise Buildings. Sustain. Cities Soc. 2024, 107, 105407. [Google Scholar] [CrossRef]
- Xu, H. Study on the Night Air Conditioning Thermal Environment of a College Dormitory in Chongqing. Master’s Thesis, Chongqing University, Chongqing, China, 2015. [Google Scholar]
- Zhang, H.; Arens, E.; Kim, D.E.; Buchberger, E.; Bauman, F.; Huizenga, C. Comfort, Perceived Air Quality, and Work Performance in a Low-Power Task–Ambient Conditioning System. Build. Environ. 2010, 45, 29–39. [Google Scholar] [CrossRef]
- GB 50325; Code for Indoor Environmental Pollution Control of Civil Building Engineering. Ministry of Housing and Urban-Rural Development of the People’s Republic of China: Beijing, China, 2020.
- GB/T 18883; Indoor Air Quality Standard. Department of Industry and Transportation. National Standards Commission: Beijing, China, 2002.
- T/CECS 586; Technical Specification for Pollution L of Fine Particulate Matter (PM2.5) in Building. China Academy of Building Research: Beijing, China, 2019.
- USEPA. Risk Assessment Guidance for Superfund Volume I—Human Health Evaluation Manual (Part A); Office of Emergency and Remedial Response: Washington, DC, USA, 1989. [Google Scholar]
- Toftum, J.; Jørgensen, A.S.; Fanger, P.O. Upper Limits of Air Humidity for Preventing Warm Respiratory Discomfort. Energy Build. 1998, 28, 15–23. [Google Scholar] [CrossRef]
- Vecchi, R.D.; Cândido, C.M.; Lamberts, R. Thermal History and Comfort in a Brazilian Subtropical Climate: A ‘Cool’ Addiction Hypothesis. Ambient Constr. 2016, 16, 7–20. [Google Scholar] [CrossRef]
- Liang, W.; Lu, M.; Yang, X. Development of a Physics-Based Model for Analyzing Formaldehyde Emissions from Building Material Under Coupling Effects of Temperature and Humidity. Build. Environ. 2021, 203, 108078. [Google Scholar] [CrossRef]
- Molina, C.; Jones, B.; Hall, I.P.; Sherman, M.H. CHAARM: A Model to Predict Uncertainties in Indoor Pollutant Concentrations, Ventilation and Infiltration Rates, and Associated Energy Demand in Chilean Houses. Energy Build. 2020, 230, 110539. [Google Scholar] [CrossRef]
- Collison, A.K.; Byrne, M.A.; McGrath, J.A. Indoor Air Quality in Naturally Ventilated Classrooms and Offices in Ireland. Build. Environ. 2025, 279, 113023. [Google Scholar] [CrossRef]
- Kim, J.; Hong, T.; Kong, M.; Jeong, K. Building Occupants’ Psycho-Physiological Response to Indoor Climate and CO2 Concentration Changes in Office Buildings. Build. Environ. 2020, 169, 106596. [Google Scholar] [CrossRef]
- Berglund, L.G.; Cain, W.S. Perceived Air Quality and the Thermal Environment. In The Human Equation: Health and Comfort: Proceedings of the ASHRAE/SOEH Conference, IAQ 89, San Diego, CA, USA, 17–20 April 1989; American Society of Heating, Refrigerating, and Air-Conditioning Engineers: Atlanta, GA, USA, 1989; pp. 93–99. [Google Scholar]
- Mui, K.W.H.; Chan, W.T.D. Adaptive Comfort Temperature Model of Air-Conditioned Building in Hong Kong. Build. Environ. 2003, 38, 837–852. [Google Scholar] [CrossRef]
- Fang, L.; Clausen, G.; Fanger, P.O. Impact of Temperature and Humidity on the Perception of Indoor Air Quality. Indoor Air 1998, 8, 276–284. [Google Scholar] [CrossRef]
- Mcfadden, E.R. Respiratory Heat and Water Exchange: Physiological and Clinical Implications. J. Appl. Physiol. 1983, 54, 331–336. [Google Scholar] [CrossRef]
- Drettner, B.; Proctor, D.F.; Andersen, I.B. The Nose: Upper Airway Physiology and the Atmospheric Environment; Elsevier: Amsterdam, The Netherlands, 1982. [Google Scholar]
- Zhang, Y. The Experimental Research into the Influence of Temperature and Carbon Dioxide on Human Comfort in Small Space. Master’s Thesis, Chongqing University, Chongqing, China, 2018. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Age | Height [cm] | Weight [kg] |
|---|---|---|---|
| Male (n = 6) | 21 ± 0.632 | 175.2 ± 6.881 | 77.8 ± 14.496 |
| Female (n = 6) | 21.5 ± 1.761 | 162.7 ± 4.148 | 56.3 ± 3.324 |
| Total (n = 12) | 21.3 ± 1.289 | 168.9 ± 8.450 | 67.0 ± 15.039 |
| Instruments | Test Content | Valid Range | Accuracy |
|---|---|---|---|
| TR-72U, temperature and humidity recorder (manufactured by T&D Corporation, located in Matsumoto, Japan) | Ta | −10–+60 °C | ±0.3 °C |
| RHin | 0–100% | ±5% | |
| WFWZY-1, air velocity (manufactured by Beijing Tianjian Huayi Technology Development Company Limited, located in Beijing, China) | Va | 0.05–30 m/s | ±5% |
| JTR04, temperature of the black globe tester (manufactured by Beijing Century Jiantong Technology Company Limited, located in Beijing, China; diameter: 150 mm) | Tg | 5–120 °C | ±0.5 °C |
| DS1922L iButton, temperature recorder (manufactured by Maxim Integrated Products, Incorporated, located in San Jose, CA, United States) | Tsk | −40–85 °C | ±0.5 °C |
| ST8306, a variety of pollutant monitoring equipment (manufactured by Smart Sensor Instrument Company Limited, located in Shenzhen, China) | CO2 | 0~5000 ppm | ±30 ppm |
| SPT | Age | Height [cm] | Weight [kg] | Metabolic Rate [Met] | |
|---|---|---|---|---|---|
| SPT ≥ 26 °C | Mean | 32.4 | 169.2 | 64.5 | 1.0 |
| Max | 59.0 | 186.0 | 115.0 | 1.2 | |
| Min | 21.0 | 151.0 | 43.0 | 1.0 | |
| Std | ±8.8 | ±7.8 | ±11.3 | ±0.03 | |
| SPT < 26 °C | Mean | 28.6 | 171.4 | 66.8 | 1.0 |
| Max | 56.0 | 189.0 | 118.0 | 1.2 | |
| Min | 20.0 | 153.0 | 43.0 | 0.8 | |
| Std | ±14.2 | ±7.8 | ±12.9 | ±0.02 |
| Instrument | Test Content | Valid Range | Accuracy |
|---|---|---|---|
| ST8306, a variety of pollutant monitoring equipment (manufactured by Smart Sensor Instrument Company Limited, located in Shenzhen, China) | CO2 | 0–5000 ppm | ±30 ppm |
| Formaldehyde | 0–2 ppm | ±0.01 ppm | |
| PM2.5 | 0–500 μg/m3 | ±10% | |
| JT-IAQ, indoor thermal comfort tester (manufactured by Beijing Century Jiantong Technology Company Limited, located in Beijing, China) | Ta | 1–60 °C | ±0.2 °C |
| RHin | 10–98% | ±1.5% | |
| Va | 0.05–5 m/s | ±(0.03 m/s + 2% reading) | |
| Tg | 1–60 °C | ±0.3 °C |
| Time/min | Mean Actual Skin Temperature [°C] | Predicted Mean Skin Temperature [°C] | p |
|---|---|---|---|
| 20 | 32.64 | 32.55 | 0.549 |
| 25 | 32.44 | 32.29 | 0.345 |
| 30 | 32.26 | 31.72 | 0.007 |
| 40 | 32.00 | 31.19 | 0.000 |
| 50 | 31.66 | 30.89 | 0.001 |
| 60 | 31.32 | 30.20 | 0.000 |
| 70 | 31.02 | 29.87 | 0.000 |
| Groups | Min | Max | Mean | Std |
| H group | 0.43 × 10−4 | 4.75 × 10−4 | 1.36 × 10−4 | ±0.60 × 10−4 |
| L group | 0.24 × 10−4 | 10.29 × 10−4 | 1.43 × 10−4 | ±0.91 × 10−4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, F.; Li, N.; Yan, H. The Influence of Thermal History and Air Conditioner Use Behavior Under Different Cooling Set Point Temperature Modes on Health. Buildings 2025, 15, 2211. https://doi.org/10.3390/buildings15132211
Shi F, Li N, Yan H. The Influence of Thermal History and Air Conditioner Use Behavior Under Different Cooling Set Point Temperature Modes on Health. Buildings. 2025; 15(13):2211. https://doi.org/10.3390/buildings15132211
Chicago/Turabian StyleShi, Fangning, Nianping Li, and Haiyan Yan. 2025. "The Influence of Thermal History and Air Conditioner Use Behavior Under Different Cooling Set Point Temperature Modes on Health" Buildings 15, no. 13: 2211. https://doi.org/10.3390/buildings15132211
APA StyleShi, F., Li, N., & Yan, H. (2025). The Influence of Thermal History and Air Conditioner Use Behavior Under Different Cooling Set Point Temperature Modes on Health. Buildings, 15(13), 2211. https://doi.org/10.3390/buildings15132211