
Impact of Resilience Engineering on Physical Symptoms of Construction Workers


Abstract
1. Introduction
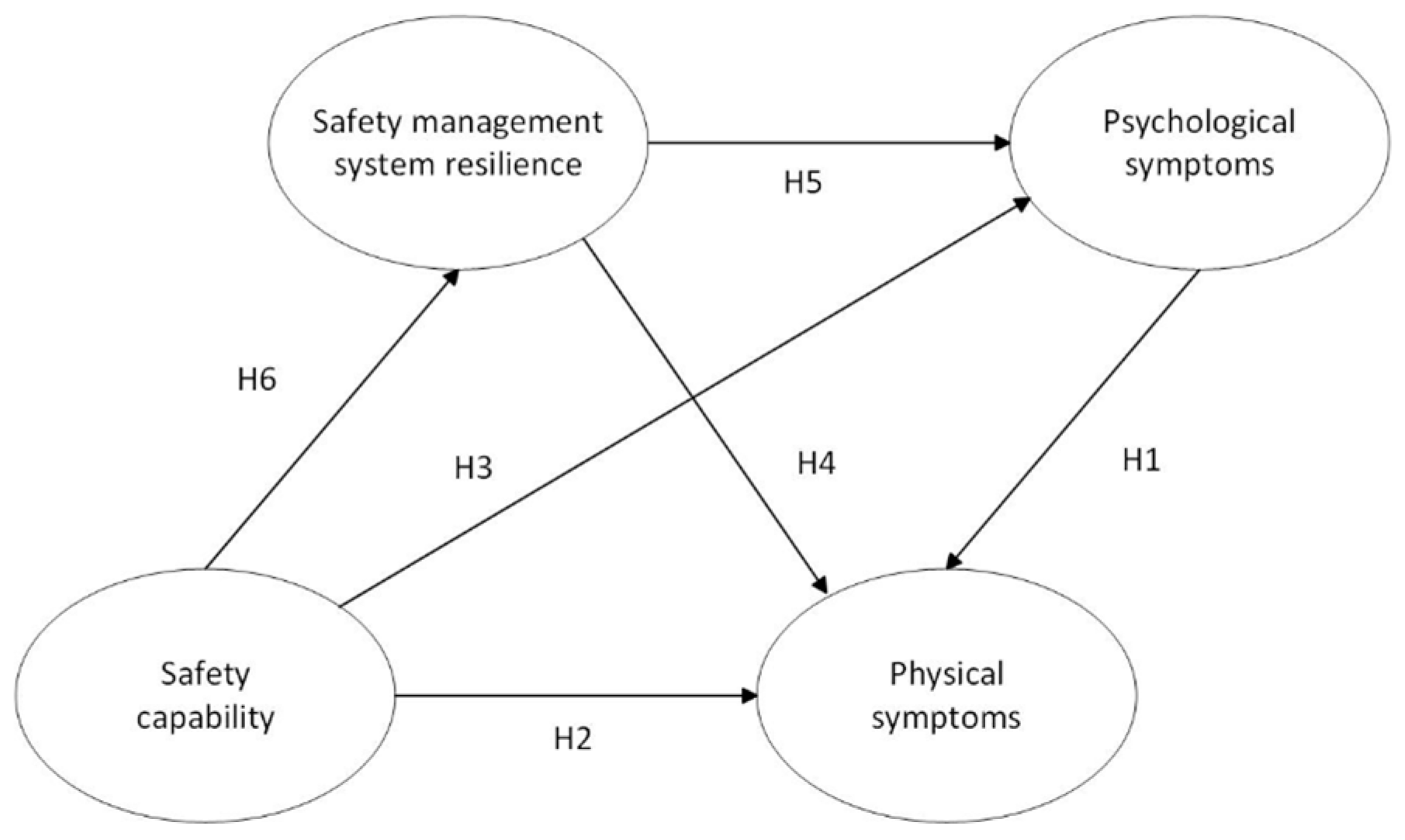
2. Literature Review and Hypotheses
2.1. Safety Capability, Psychological Symptoms, and Physical Symptoms
2.2. Safety Management System Resilience, Psychological Symptoms, and Physical Symptoms
2.3. Safety Capability and Safety Management System Resilience
3. Methods
3.1. Ethical Approval
3.2. Questionnaire Design
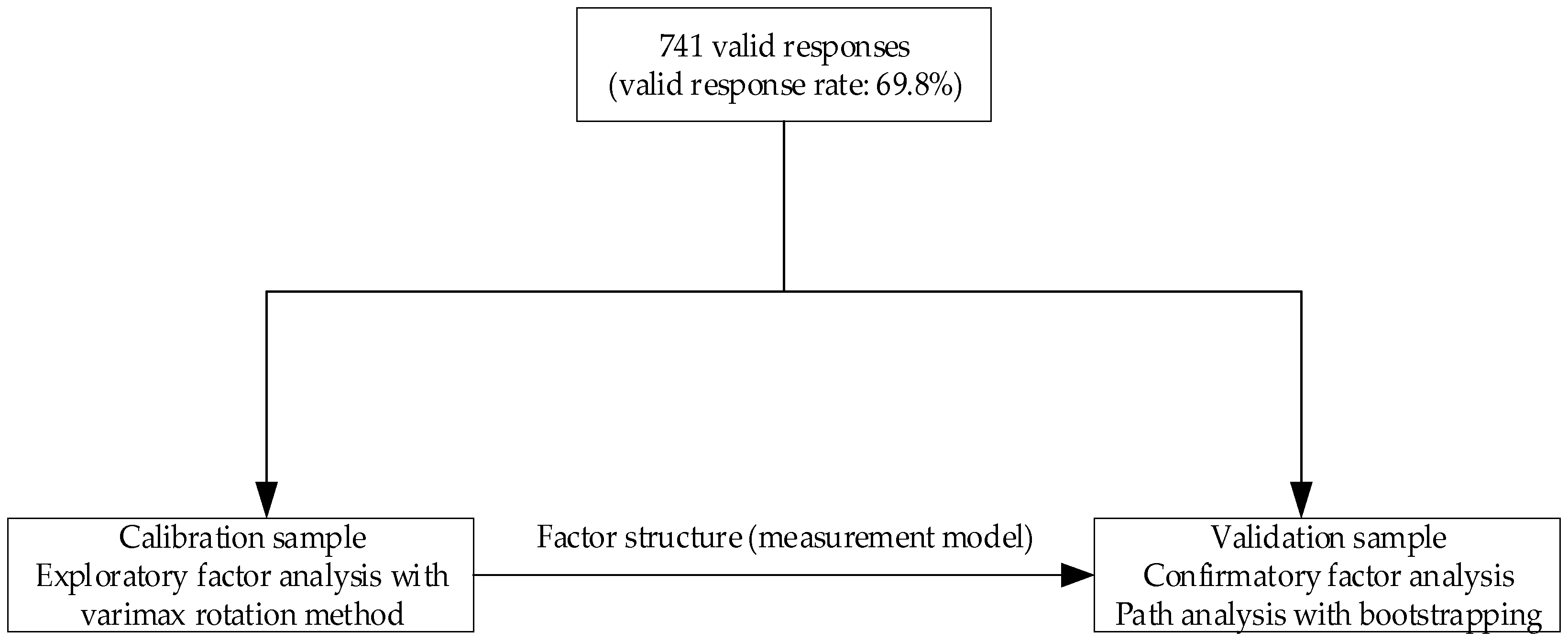
3.3. Data Collection Procedures
3.4. Data Analysis
4. Results
4.1. Exploratory Factor Analysis Results
4.2. Confirmatory Factor Analysis Results
4.2.1. Measurement Model
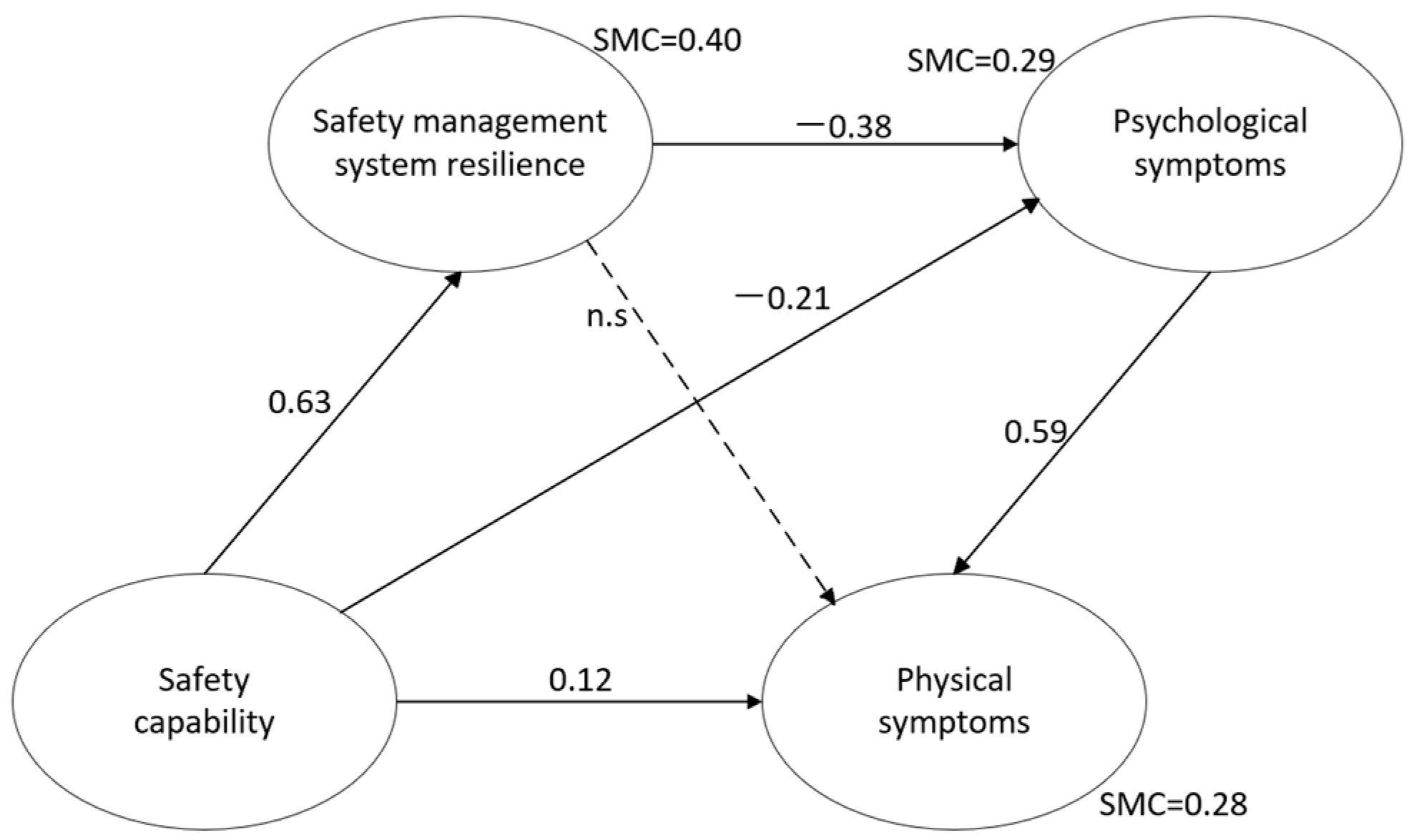
4.2.2. Structural Model
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Giang, D.T.; Pheng, L.S. Role of construction in economic development: Review of key concepts in the past 40 years. Habitat. Int. 2011, 35, 118–125. [Google Scholar] [CrossRef]
- Mitrevska, C.; Mitrevska, E.; Mitrevski, V. Statistical indicators for accidents at work in construction sector. Ann. Fac. Eng. Hunedoara 2022, 20, 87–90. [Google Scholar]
- Boadu, E.F.; Okeke, S.R.; Boadi, C.; Bonsu, E.O.; Addo, I.Y. Work-related respiratory health conditions among construction workers: A systematic narrative review. BMJ Open Respir. Res. 2023, 10, e001736. [Google Scholar] [CrossRef] [PubMed]
- Keer, S.; Brooks, C.; Glass, B.; McLean, D.; Harding, E.; Douwes, J. Respiratory symptoms and use of dust-control measures in New Zealand construction workers: A cross-sectional study. PLoS ONE 2022, 17, e0266668. [Google Scholar] [CrossRef]
- Ringen, K.; Dement, J.; Welch, L.; Dong, X.S.; Bingham, E.; Quinn, P.S. Risks of a lifetime in construction. Part II: Chronic occupational diseases. Am. J. Ind. Med. 2014, 57, 1235–1245. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. Migrant Workers Monitoring Survey Report 2023. Available online: https://www.stats.gov.cn/xxgk/sjfb/zxfb2020/202404/t20240430_1948783.html (accessed on 5 November 2024).
- Lee, Y.-C.; Hong, X.; Man, S.S. Prevalence and associated factors of work-related musculoskeletal disorders symptoms among construction workers: A cross-sectional study in South China. Int. J. Environ. Res. Public Health 2023, 20, 4653. [Google Scholar] [CrossRef]
- Tadesse, S.; Israel, D. Occupational injuries among building construction workers in Addis Ababa, Ethiopia. J. Occup. Med. Toxicol. 2016, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Abbe, O.O.; Harvey, C.M.; Ikuma, L.H.; Aghazadeh, F. Modeling the relationship between occupational stressors, psychosocial/physical symptoms and injuries in the construction industry. Int. J. Ind. Ergon. 2011, 41, 106–117. [Google Scholar] [CrossRef]
- Payne, S.C.; Bergman, M.E.; Beus, J.M.; Rodríguez, J.M.; Henning, J.B. Safety climate: Leading or lagging indicator of safety outcomes? J. Loss Prev. Process Ind. 2009, 22, 735–739. [Google Scholar] [CrossRef]
- Lyu, S.; Hon, C.K.; Chan, A.P.; Wong, F.K.; Javed, A.A. Relationships among safety climate, safety behavior, and safety outcomes for ethnic minority construction workers. Int. J. Environ. Res. Public Health 2018, 15, 484. [Google Scholar] [CrossRef]
- Marín, L.S.; Lipscomb, H.; Cifuentes, M.; Punnett, L. Associations between safety climate and safety management practices in the construction industry. Am. J. Ind. Med. 2017, 60, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Zahoor, H.; Chan, A.P.; Utama, W.P.; Gao, R.; Zafar, I. Modeling the relationship between safety climate and safety performance in a developing construction industry: A cross-cultural validation study. Int. J. Environ. Res. Public Health 2017, 14, 351. [Google Scholar] [CrossRef]
- Ham, D.H. Safety-II and resilience engineering in a nutshell: An introduction guide to their concepts and methods. Saf. Health Work 2021, 12, 10–19. [Google Scholar] [CrossRef]
- Bergström, J.; van Winsen, R.; Henriqson, E. On the rationale of resilience in the domain of safety: A literature review. Reliab. Eng. Syst. Saf. 2015, 141, 131–141. [Google Scholar] [CrossRef]
- Zhou, Z. Understanding the administrative regulation on occupational health and trend in China. J. Occup. Health 2018, 60, 126–131. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Interpretation of the National Program on Prevention and Control of Occupational Diseases (2021–2025). Available online: http://www.nhc.gov.cn/zyjks/zcwj2/202112/7960f4ad8b03466cb34fe537ae7551b5.shtml (accessed on 6 November 2024).
- Peñaloza, G.A.; Wasilkiewicz, K.; Saurin, T.A.; Herrera, I.A.; Formoso, C.T. Safety-I and Safety-II: Opportunities for an integrated approach in the construction industry. In Proceedings of the 8th REA Symposium Embracing Resilience: Scaling up and Speeding up, Kalmar, Sweden, 24–27 June 2019. [Google Scholar]
- Yiu, N.S.N.; Chan, D.W.M.; Shan, M.; Sze, N.N. Implementation of safety management system in managing construction projects: Benefits and obstacles. Saf. Sci. 2019, 117, 23–32. [Google Scholar] [CrossRef]
- Pilanawithana, N.M.; Feng, Y.; London, K.; Zhang, P. Developing resilience for safety management systems in building repair and maintenance: A conceptual model. Saf. Sci. 2022, 152, 105768. [Google Scholar] [CrossRef]
- Li, K.; Wang, D.; Sheng, Z.; Griffin, M.A. A deep dive into worker psychological well-being in the construction industry: A systematic review and conceptual framework. J. Manag. Eng. 2022, 38, 04022051. [Google Scholar] [CrossRef]
- Jefferies, M.; Brewer, G.J.; Gajendran, T. Using a case study approach to identify critical success factors for alliance contracting. Eng. Constr. Archit. Manag. 2014, 21, 465–480. [Google Scholar] [CrossRef]
- Griffin, M.A.; Cordery, J.; Soo, C. Dynamic safety capability. Organ. Psychol. Rev. 2016, 6, 248–272. [Google Scholar] [CrossRef]
- Lyu, Q.; Fu, G.; Wang, Y.; Zhang, R.; Wu, Y.; Xie, X. Cause analysis framework from a safety capability perspective: Application to Tianjiayi hazardous chemical explosion accident. Process Saf. Prog. 2023, 42, 567–577. [Google Scholar] [CrossRef]
- Liu, Q.; Li, X. Modeling and evaluation of the safety control capability of coal mine based on system safety. J. Clean. Prod. 2014, 84, 797–802. [Google Scholar] [CrossRef]
- Yu, C.; Li, A. Evaluation research on safety management capability at construction sites of construction projects. IOP Conf. Ser. Earth Environ. Sci. 2022, 1011, 012037. [Google Scholar] [CrossRef]
- Choudhry, R.M.; Fang, D. Why operatives engage in unsafe work behavior: Investigating factors on construction sites. Saf. Sci. 2008, 46, 566–584. [Google Scholar] [CrossRef]
- Siu, O.; Phillips, D.R.; Leung, T. Safety climate and safety performance among construction workers in Hong Kong: The role of psychological strains as mediators. Accid. Anal. Prev. 2004, 36, 359–366. [Google Scholar] [CrossRef]
- Leung, M.Y.; Liang, Q.; Olomolaiye, P. Impact of job stressors and stress on the safety behavior and accidents of construction workers. J. Manag. Eng. 2016, 32, 04015019. [Google Scholar] [CrossRef]
- Lim, S.; Chi, S.; Lee, J.D.; Lee, H.J.; Choi, H. Analyzing psychological conditions of field-workers in the construction industry. Int. J. Occup. Environ. Health 2017, 23, 261–281. [Google Scholar] [CrossRef]
- Leung, M.; Chan, Y.S.; Yuen, K.W. Impacts of stressors and stress on the injury incidents of construction workers in Hong Kong. J. Constr. Eng. Manag. 2010, 136, 1093–1103. [Google Scholar] [CrossRef]
- Blackhall, I.; Littlemore, M. The impacts of personal stress upon critical project decision making in construction. Built Nat. Environ. Res. Pap. 2010, 3, 7–16. [Google Scholar]
- Sobeih, T.M.; Salem, O.; Daraiseh, N.; Genaidy, A.; Shell, R. Psychosocial factors and musculoskeletal disorders in the construction industry: A systematic review. Theor. Issues Ergon. Sci. 2006, 7, 329–344. [Google Scholar] [CrossRef]
- Jacobsen, H.B.; Caban-Martinez, A.; Onyebeke, L.C.; Sorensen, G.; Dennerlein, J.T.; Reme, S.E. Construction workers struggle with a high prevalence of mental distress and this is associated with their pain and injuries. J. Occup. Environ. Med. 2013, 55, 1197–1204. [Google Scholar] [CrossRef] [PubMed]
- Bernabé, M.; Botia, J.M. Resilience as a mediator in emotional social support’s relationship with occupational psychology health in firefighters. J. Health Psychol. 2016, 21, 1778–1786. [Google Scholar] [CrossRef]
- Holling, C.S. Resilience and stability of ecological systems. Annu. Rev. Ecol. Syst. 1973, 4, 1–23. [Google Scholar] [CrossRef]
- Madni, A.M.; Jackson, S. Towards a conceptual framework for resilience engineering. IEEE Syst. J. 2009, 3, 181–191. [Google Scholar] [CrossRef]
- Pęciłło, M. The resilience engineering concept in enterprises with and without occupational safety and health management systems. Saf. Sci. 2016, 82, 190–198. [Google Scholar] [CrossRef]
- Chen, Y.; McCabe, B.; Hyatt, D. Impact of individual resilience and safety climate on safety performance and psychological stress of construction workers: A case study of the Ontario construction industry. J. Saf. Res. 2017, 61, 167–176. [Google Scholar] [CrossRef]
- Rosa, L.V.; França, J.E.; Haddad, A.N.; Carvalho, P.V. A resilience engineering approach for sustainable safety in green construction. J. Sustain. Dev. Energy Water Environ. Syst. 2017, 5, 480–495. [Google Scholar] [CrossRef]
- Tonetto, M.S.; Formoso, C.T.; Saurin, T.A.; Bonesi De Luca, F.; Lora, F.P.; Lantelme, E. Resilient performance on construction projects in the post-pandemic era: An organizational perspective. Eng. Constr. Archit. Manag. 2023; ahead-of-print. [Google Scholar] [CrossRef]
- Pilanawithana, N.M.; Feng, Y.; London, K.; Zhang, P. Framework for measuring resilience of safety management systems in Australian building repair and maintenance companies. J. Saf. Res. 2023, 85, 405–418. [Google Scholar] [CrossRef] [PubMed]
- Darabont, D.C.; Cioca, L.; Bejinariu, C.; Badea, D.O.; Chivu, O.R.; Chis, T.V. Impact of personal protective equipment use on stress and psychological well-being among firefighters: Systematic review and meta-analysis. Sustainability 2024, 16, 9666. [Google Scholar] [CrossRef]
- Ranasinghe, U.; Jefferies, M.; Davis, P.; Pillay, M. Resilience engineering indicators and safety management: A systematic review. Saf. Health Work 2020, 11, 127–135. [Google Scholar] [CrossRef]
- Nadler, J.T.; Weston, R.; Voyles, E.C. Stuck in the middle: The use and interpretation of mid-points in items on questionnaires. J. Gen. Psychol. 2015, 142, 71–89. [Google Scholar] [CrossRef] [PubMed]
- Revilla, M.A.; Saris, W.E.; Krosnick, J.A. Choosing the number of categories in agree–disagree scales. Sociol. Methods Res. 2014, 43, 73–97. [Google Scholar] [CrossRef]
- Tang, S.; Zhu, K.; Guo, P. Research on quantitative assessment and dynamic reasoning method for emergency response capability in prefabricated construction safety. Buildings 2023, 13, 2311. [Google Scholar] [CrossRef]
- Feng, Y.; Trinh, M.T. Developing resilient safety culture for construction projects. J. Constr. Eng. Manag. 2019, 145, 04019069. [Google Scholar] [CrossRef]
- Guo, Q.; Hao, Q.; Wang, Y.; Wang, J. Subway system resilience evaluation in based on ANP-extension cloud model. J. Syst. Simul. 2021, 33, 943–950. (In Chinese) [Google Scholar]
- Park, J.Y.; Lee, J.H.; Kang, M.Y.; Jang, T.W.; Kim, H.R.; Kim, S.Y.; Lee, J. Development of algorithm for work intensity evaluation using excess overwork index of construction workers with real-time heart rate measurement device. Ann. Occup. Environ. Med. 2023, 35, e24. [Google Scholar] [CrossRef]
- Zahoor, H.; Chan, A.P.; Utama, W.P.; Gao, R.; Memon, S.A. Determinants of safety climate for building projects: SEM-based cross-validation study. J. Constr. Eng. Manag. 2017, 143, 05017005. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 8th ed.; Cengage Learning EMEA: Andover, UK, 2019; p. 746. [Google Scholar]
- Shen, Y.; Koh, T.Y.; Rowlinson, S.; Bridge, A.J. Empirical investigation of factors contributing to the psychological safety climate on construction sites. J. Constr. Eng. Manag. 2015, 141, 04015038. [Google Scholar] [CrossRef]
- Kaiser, H.F. The application of electronic computers to factor analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Cronbach, L.J. Coefficient alpha and the internal structure of tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- Ab Hamid, M.R.; Sami, W.; Sidek, M.M. Discriminant validity assessment: Use of Fornell & Larcker criterion versus HTMT criterion. J. Phys. Conf. Ser. 2017, 890, 012063. [Google Scholar]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Provan, D.J.; Woods, D.D.; Dekker, S.W.; Rae, A.J. Safety II professionals: How resilience engineering can transform safety practice. Reliab. Eng. Syst. Saf. 2020, 195, 106740. [Google Scholar] [CrossRef]
- Patriarca, R.; Bergström, J.; Di Gravio, G.; Costantino, F. Resilience engineering: Current status of the research and future challenges. Saf. Sci. 2018, 102, 79–100. [Google Scholar] [CrossRef]
- Harvey, E.J.; Waterson, P.; Dainty, A.R. Applying HRO and resilience engineering to construction: Barriers and opportunities. Saf. Sci. 2019, 117, 523–533. [Google Scholar] [CrossRef]
- Peñaloza, G.A.; Saurin, T.A.; Formoso, C.T. Monitoring complexity and resilience in construction projects: The contribution of safety performance measurement systems. Appl. Ergon. 2020, 82, 102978. [Google Scholar] [CrossRef] [PubMed]
- Yiu, N.S.; Sze, N.N.; Chan, D.W. Implementation of safety management systems in Hong Kong construction industry: A safety practitioner’s perspective. J. Saf. Res. 2018, 64, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yin, S.; Wu, Y.; Shen, Y.; Rowlinson, S. Development of a classification framework for construction personnel’s safety behavior based on machine learning. Buildings 2023, 13, 43. [Google Scholar] [CrossRef]
- Kolk, A.M.; Hanewald, G.J.; Schagen, S.; van Wijk, C.M.G. A symptom perception approach to common physical symptoms. Soc. Sci. Med. 2003, 57, 2343–2354. [Google Scholar] [CrossRef]
- Kotera, Y.; Green, P.; Sheffield, D. Work-life balance of UK construction workers: Relationship with mental health. Constr. Manag. Econ. 2020, 38, 291–303. [Google Scholar] [CrossRef]
- Rouhanizadeh, B.; Kermanshachi, S. Causes of the mental health challenges in construction workers and their impact on labor productivity. In Proceedings of the Tran-SET 2021, Reston, VA, USA, 3–4 June 2021; pp. 16–26. [Google Scholar]
- Bhattacharjee, K.; Bugalia, N.; Mahalingam, A. An analysis of safety practices for small, medium, and large construction projects: A resilience engineering perspective. Saf. Sci. 2024, 169, 106330. [Google Scholar] [CrossRef]
- Righi, A.W.; Saurin, T.A.; Wachs, P. A systematic literature review of resilience engineering: Research areas and a research agenda proposal. Reliab. Eng. Syst. Saf. 2015, 141, 142–152. [Google Scholar] [CrossRef]
- Pillay, M.; Borys, D.; Else, D.; Tuck, M. Safety culture and resilience engineering-Exploring theory and application in improving gold mining safety. In Proceedings of the Gravity Gold Conference, Melbourne, Australia, 21–22 September 2010. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Category | Frequency | Percentage (%) |
|---|---|---|---|
| Gender | Male | 637 | 86.0% |
| Female | 104 | 14.0% | |
| Age | <25 | 42 | 5.7% |
| 25–30 | 77 | 10.4% | |
| 31–40 | 243 | 32.8% | |
| 41–50 | 275 | 37.1% | |
| >50 | 104 | 14.0% | |
| Educational level | Primary school | 211 | 28.5% |
| Junior middle school | 411 | 55.5% | |
| High school | 89 | 12.0% | |
| College/University | 30 | 4.0% | |
| Work experience (Years) | <5 | 222 | 30.0% |
| 5–10 | 179 | 24.2% | |
| 11–15 | 147 | 19.8% | |
| 16–20 | 133 | 18.0% | |
| 21–25 | 37 | 5.0% | |
| >25 | 23 | 3.0% | |
| Working hours per week (Hours) | <40 | 15 | 2.0% |
| 41–50 | 145 | 19.6% | |
| 51–60 | 309 | 41.7% | |
| 60–70 | 180 | 24.3% | |
| >70 | 92 | 12.4% | |
| Years with the current employer | <1 | 186 | 25.1% |
| 1–2 | 282 | 38.1% | |
| 2–3 | 147 | 19.8% | |
| >3 | 126 | 17.0% |
| Scale Items | SMSR | SC | PSY | PHY |
|---|---|---|---|---|
| SMSR1 | 0.75 | |||
| SMSR2 | 0.85 | |||
| SMSR3 | 0.80 | |||
| SC1 | 0.84 | |||
| SC2 | 0.77 | |||
| SC3 | 0.82 | |||
| SC4 | 0.66 | |||
| SC5 | 0.65 | |||
| SC6 | 0.79 | |||
| SC7 | 0.74 | |||
| SC8 | 0.78 | |||
| PSY1 | 0.58 | |||
| PSY2 | 0.70 | |||
| PSY3 | 0.78 | |||
| PSY4 | 0.83 | |||
| PHY1 | 0.85 | |||
| PHY2 | 0.67 | |||
| PHY3 | 0.65 | |||
| PHY4 | 0.87 | |||
| PHY5 | 0.85 |
| Scale Items | SMCs | |
|---|---|---|
| Estimate | 10,000 Bootstrapping 95% Confidence Interval | |
| SMSR1 | 0.56 | [0.42, 0.67] |
| SMSR2 | 0.72 | [0.66, 0.79] |
| SMSR3 | 0.65 | [0.57, 0.72] |
| SC1 | 0.70 | [0.64, 0.75] |
| SC2 | 0.60 | [0.53, 0.66] |
| SC3 | 0.67 | [0.60, 0.72] |
| SC4 | 0.44 | [0.32, 0.55] |
| SC5 | 0.42 | [0.30, 0.53] |
| SC6 | 0.62 | [0.55, 0.68] |
| SC7 | 0.55 | [0.48, 0.60] |
| SC8 | 0.60 | [0.49, 0.68] |
| PSY1 | 0.34 | [0.24, 0.44] |
| PSY2 | 0.49 | [0.39, 0.59] |
| PSY3 | 0.60 | [0.49, 0.70] |
| PSY4 | 0.68 | [0.57, 0.79] |
| PHY1 | 0.72 | [0.39, 0.90] |
| PHY2 | 0.45 | [0.14, 0.76] |
| PHY3 | 0.42 | [0.14, 0.73] |
| PHY4 | 0.76 | [0.74, 0.91] |
| PHY5 | 0.72 | [0.28, 0.87] |
| Mean | S. D. | Cronbach’s α | SC | SMSR | PSY | PHY | |
|---|---|---|---|---|---|---|---|
| SC | 3.77 | 0.59 | 0.91 | 0.58 | |||
| SMSR | 3.96 | 0.69 | 0.84 | 0.63 *** | 0.64 | ||
| PSY | 1.29 | 0.40 | 0.81 | −0.45 *** | −0.51 *** | 0.53 | |
| PHY | 1.04 | 0.20 | 0.87 | −0.11 *** | −0.17 *** | 0.51 *** | 0.61 |
| Path | Estimate | 95% Confidence Interval (with 10,000 Bootstrap Samples) | Comment | |
|---|---|---|---|---|
| H1: PSY → PHY | 0.59 | [0.44, 0.74] | H1 supported | |
| H2: SC → PHY | 0.12 | [0.05, 0.21] | H2 not supported | |
| H3: SC → PSY | −0.21 | [−0.33, −0.10] | H3 supported | |
| H4: SMSR → PHY | 0.05 | [−0.04, 0.16] | H4 not supported | |
| H5: SMSR → PSY | −0.38 | [−0.51, −0.25] | H5 supported | |
| H6: SC → SMSR | 0.63 | [0.50, 0.74] | H6 supported | |
| Path | Estimate | 95% Confidence Interval (with 10,000 Bootstrap Samples) |
|---|---|---|
| SC → SMSR → PHY | 0.01 | [−0.01, 0.04] |
| SC → PSY → PHY | −0.03 | [−0.09, −0.02] |
| SC → SMSR → PSY → PHY | −0.04 | [−0.10, −0.02] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Z.; Zhong, H.; Li, S.; Li, S.; Shen, Y.; He, C.; Xu, Z. Impact of Resilience Engineering on Physical Symptoms of Construction Workers. Buildings 2024, 14, 4056. https://doi.org/10.3390/buildings14124056
Hu Z, Zhong H, Li S, Li S, Shen Y, He C, Xu Z. Impact of Resilience Engineering on Physical Symptoms of Construction Workers. Buildings. 2024; 14(12):4056. https://doi.org/10.3390/buildings14124056
Chicago/Turabian StyleHu, Zhen, Heng Zhong, Siyuan Li, Siyi Li, Yuzhong Shen, Changquan He, and Zhizhou Xu. 2024. "Impact of Resilience Engineering on Physical Symptoms of Construction Workers" Buildings 14, no. 12: 4056. https://doi.org/10.3390/buildings14124056
APA StyleHu, Z., Zhong, H., Li, S., Li, S., Shen, Y., He, C., & Xu, Z. (2024). Impact of Resilience Engineering on Physical Symptoms of Construction Workers. Buildings, 14(12), 4056. https://doi.org/10.3390/buildings14124056