


Assessment of Households’ Perceptions of Health Co-Benefits in Relation to the Willingness to Undertake Energy Retrofits in Barcelona



Abstract
1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Supporting Literature | Impact Subcategory | Causes | Physical Indicator | Method Used |
|---|---|---|---|---|
| Vandentorren et al. (2003) [9] France | High interior temperatures | Heat waves Living in a penthouse Lack of thermal insulation | Additional deaths Respiratory diseases Cardiovascular diseases | A case study in four different areas in France (where the heat wave was strongest) |
| Kampa and Castanas (2008) [10] | Indoor air quality | Particulate matter (PM10 and PM2.5). Nitrogen dioxide (NO2). Sulfur dioxide (SO2) emissions of Sox and NOx CO2 and ozone (O3) | Mortality Respiratory problems (asthma and chronic bronchitis) Cardiovascular problems Lung cancer | Avoided costs approach Contingent valuation method Willingness to pay (WTP) |
| Ortiz, J. and Salom, J. (2016) [6] Spain | Cold temperatures in winter | Age of the dwelling Existence and characteristics of the heating system Price of energy (heating) | Self-perceived health Respiratory diseases (asthma and chronic bronchitis) Cardiovascular diseases Mortality and morbidity | Characterise the housing stock in Spain Characterise dwellings that do not guarantee comfort conditions in winter Describe people’s health |
| Chapman et al. (2003) [11] United States | Condensations (dampness and fungus) | Warm climates | Irritation, allergies, infections, and asthma | Meta-analysis |
| Bjørner, T. (2004) [12] Denmark Copenhague | Noise exposure | Road and air traffic Ambient noise above 55 dB | Cardiovascular diseases Cognitive impairment in children Sleep disturbance Tinnitus Increased mortality Irritation or anger | Contingent valuation and questionnaire Willingness to pay (WTP) |
| Martin Jakob (2004) [7] Swiss. Residential sector | Thermal comfort | n.a. | n.a. | * Avoided cost approach * Cost–benefit analysis |
| Barón Rodríguez, A. (2017) [13] Spain | Co-benefits Thermal comfort | n.a. | n.a. | * Survey * Descriptive statistical analysis |
| Biere Arenas, R. et al. (2023). [14] Barcelonés | Pecuniary benefits Co-benefits | n.a. | n.a. | * Survey * Multivariate analysis of results * Principal components |
| Marmolejo et al. (2020) [15] Spain | Co-benefits Thermal comfort | n.a. | n.a. | * Survey * Descriptive statistical analysis * Regression model |
| Larger scale; exterior housing | ||||
| Arellano, B. Et al. (2022) [23] Spain. Barcelona | Heat island | * Torrid temperatures | * Respiratory diseases * Cardiovascular diseases * Morbidity and mortality | * Individualised analysis for the four weather stations * Linear ordinary least squares regression (OLS) |
2. Research Methodology
3. Method and Materials
3.1. Survey Design
3.2. Validity and Reliability of the Survey
3.3. Population and Sample
3.4. Data Collection
3.5. Survey Improvement and Respondents Recruiting
4. Statistical Analysis
5. Results and Discussion
5.1. Descriptive Analysis
5.1.1. Socio-Demographic Characteristics
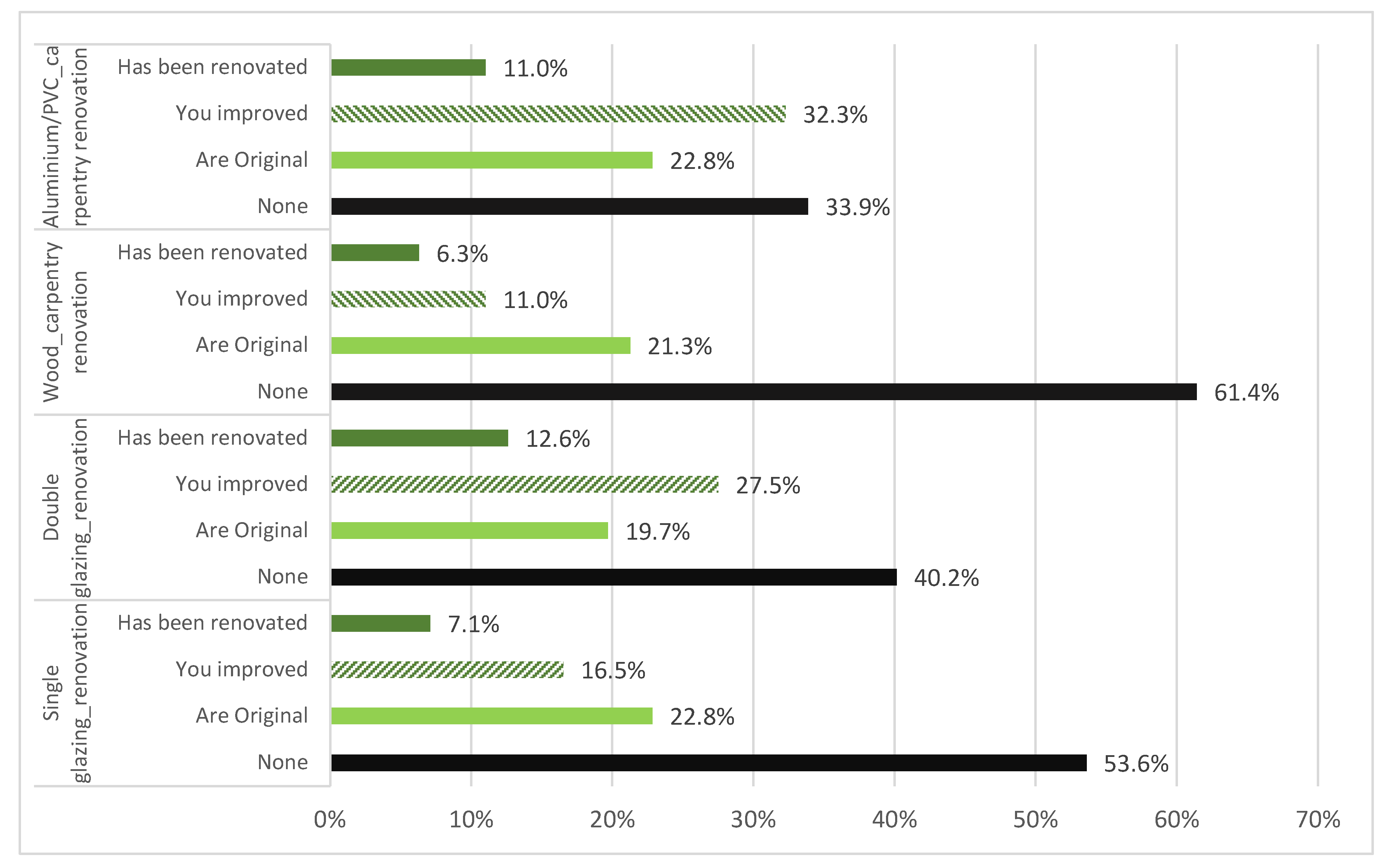
5.1.2. Housing Conditions and Attributes
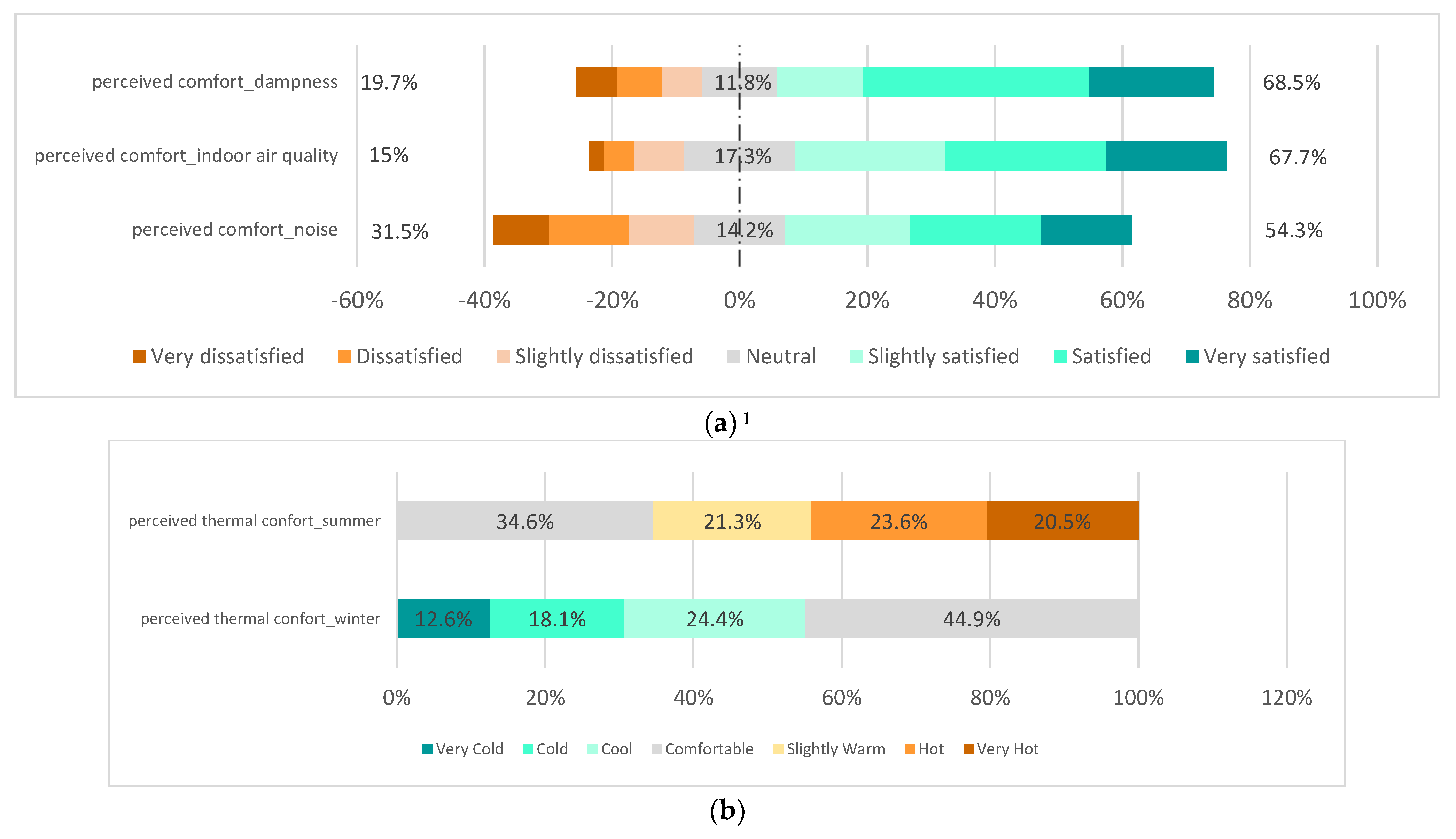
5.1.3. Perception of Indoor Comfort Conditions
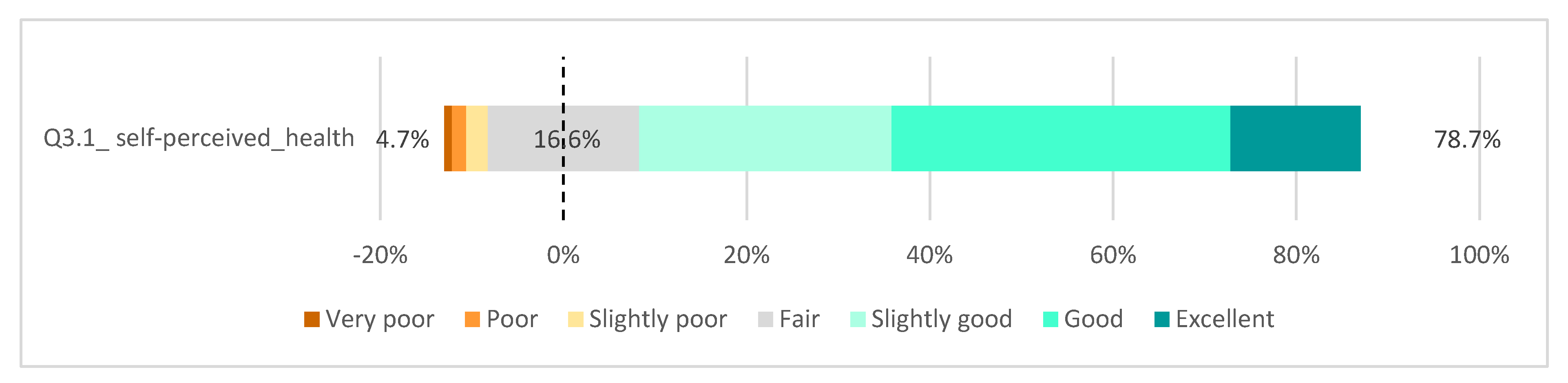
5.1.4. Self-Perception of Health
5.1.5. Awareness of the Health Co-Benefits of Housing Conditions
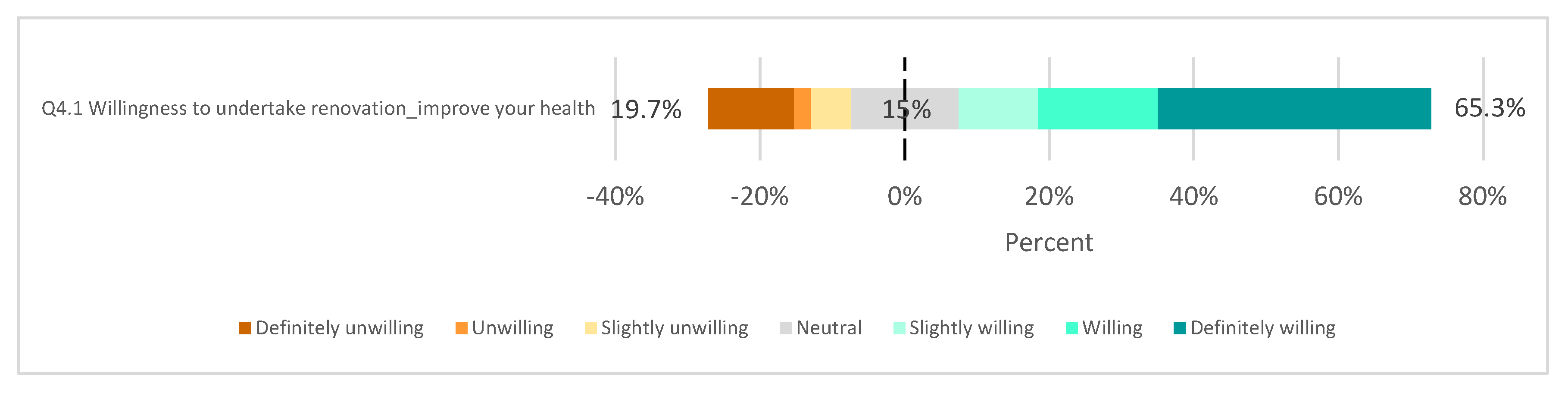
5.1.6. Willingness to Undertake an Energy Retrofit
5.2. Segmented Analysis
- -
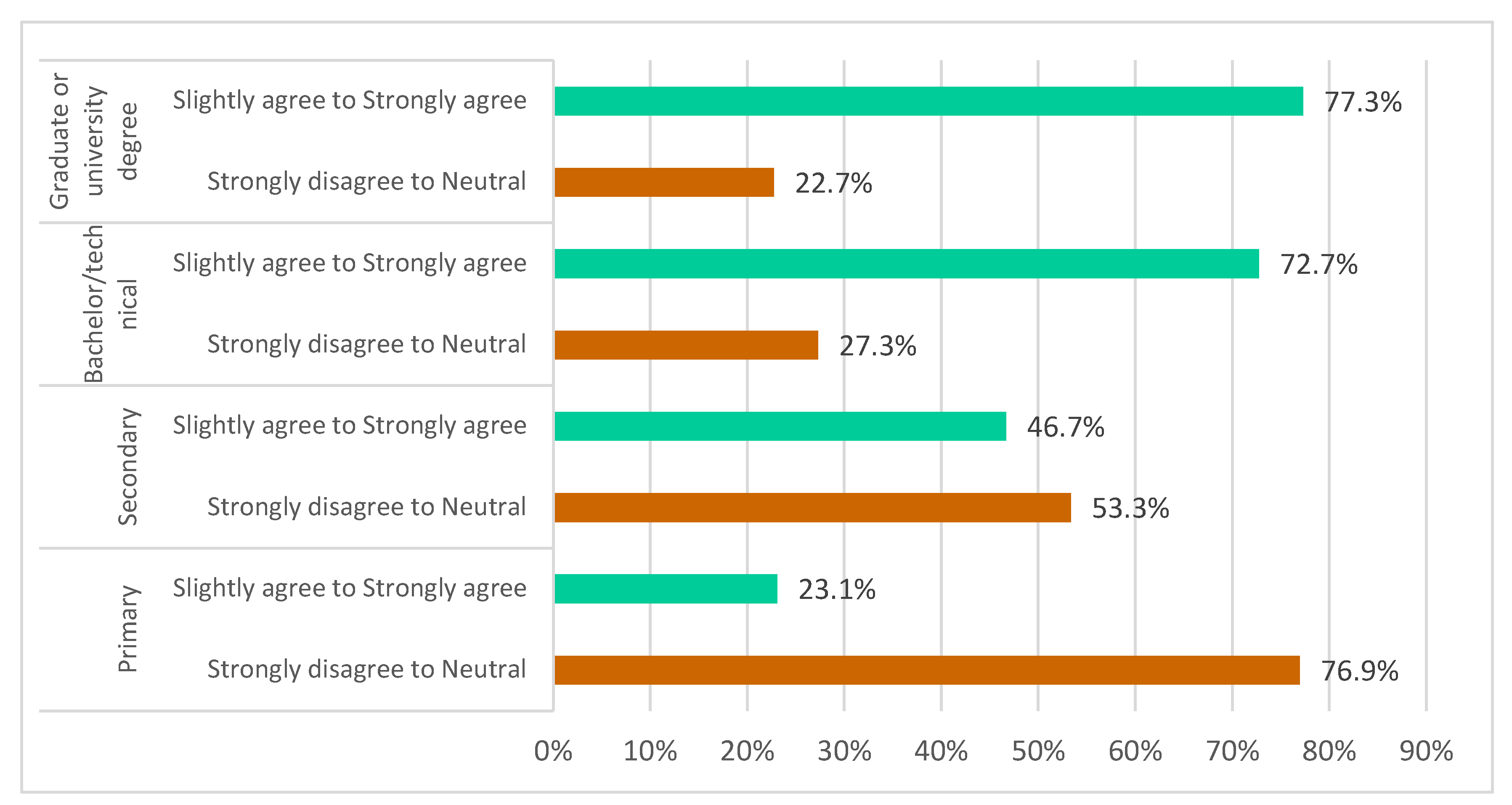
- Relationship between awareness of health co-benefits and educational attainment
- -
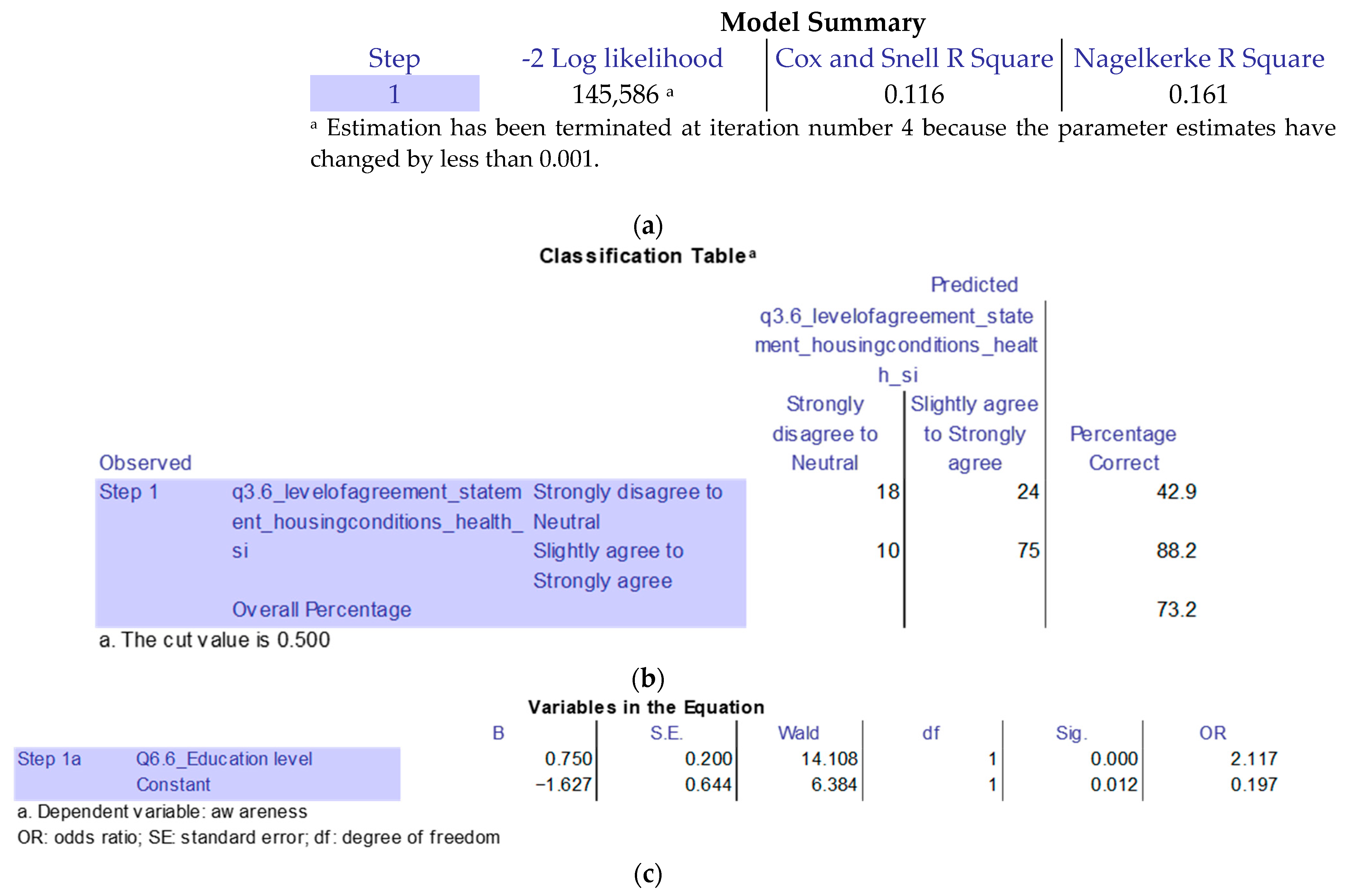
- Explanatory model for awareness
- -
- Relationship between respiratory diseases and dampness
- -
- Relationship between willingness to undertake energy retrofits and housing conditions
- -
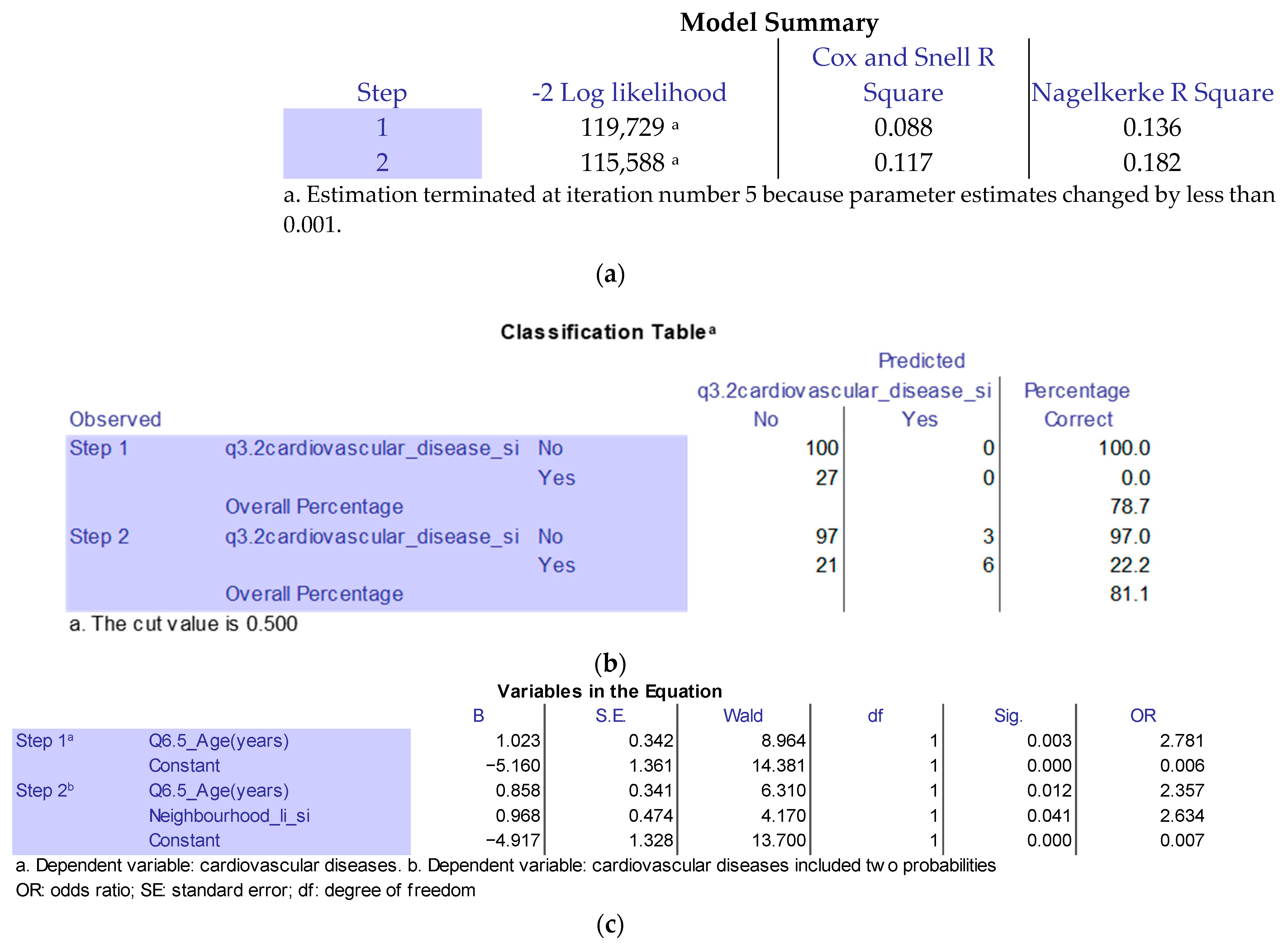
- Relationship between cardiovascular diseases and neighbourhood (income)
6. Conclusions
Discussion, Limitations of the Study, and Future Research
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- WWF. Potencial de Ahorro Energético y de Reducción de Emisiones de CO2 del Parque Residencial Existente en España en 2020; WWF: Madrid, Spain, 2010; Available online: https://wwfes.awsassets.panda.org/downloads/resumen_wwf.pdf?40760/Potencial-de-Ahorro-Energtico-y-de-Reduccin-de-Emisiones-de-CO2-del-Parque-Residencial-existente-en-Espaa-en-2020 (accessed on 10 January 2024).
- Ajuntament de Barcelona. Energia Barcelona. Available online: https://www.energia.barcelona/es/ahorrar-energia-en-el-hogar-y-en-el-trabajo (accessed on 2 June 2023).
- Agencias. Destinados 17,8 Millones de Fondos Europeos a Rehabilitar 1.933 Viviendas en Barcelona, 20–22. Available online: https://www.lavanguardia.com/vida/20230602/9015609/destinados-17-8-millones-fondos-europeos-rehabilitar-1-933-viviendas-barcelona.html (accessed on 2 June 2023).
- European Commission. Directive 2010/31/EU of the European Parliament and of the Council of 19 May 2010 on the Energy Performance of Buildings (Recast). 2018. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A02010L0031-20210101 (accessed on 10 January 2024).
- Directive (EU) 2023/1791 of the European Parliament and of the Council of 13 September 2023 on Energy Efficiency and Amending Regulation (EU) 2023/955 (Recast) (Text with EEA Relevance). Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ%3AJOL_2023_231_R_0001 (accessed on 10 January 2024).
- Ortiz, J.; Salom, J. Estimación del Efecto de la Rehabilitación Energética en la Salud de las Personas. In Eficiencia Energética: Sistemas, Edificios y Comunidades; Institut de Recerca en Energia de Catalunya, Barcelona, Spain. 2016. Available online: http://www.lacasaqueahorra.org/documentos/estimacionEfectoRehabilitacionSalud.pdf (accessed on 30 September 2023).
- Jakob, M. Marginal costs and co-benefits of energy efficiency investments: The case of the Swiss residential sector. Energy Policy 2006, 34, 172–187. [Google Scholar] [CrossRef]
- Dell’Anna, F.; Becchio, C.; Bottero, M.; Corgnati Stefano, P. Evaluating Health Benefits of Urban Energy Retrofitting: An Application for the City of Turin. In Smart and Sustainable Planning for Cities and Regions; Springer International Publishing: Cham, Switzerland, 2019; pp. 281–304. [Google Scholar] [CrossRef]
- Barón Rodríguez, A.; Ortíz Roncallo, M.; Larrea Eguiguren, A.; Ampudia Farías, A.; Marmolejo Duarte, C.R.; Garcia-Almirall, M.P. Study of the perception of thermal comfort, Residetial Satisfaction and management model, of the residents of the conservation and energy Rehabilitation Area in the Poroneos Street, Santa Coloma de Gramenet, Spain. In Proceedings of the International Congress Virtual City and Territory (XII CTV)—Intelligent Cities and Territories (CTV 2018), Mendoza, Argentina, 5–7 September 2018; CPSV: Barcelona, Spain, 2018; pp. 303–318. [Google Scholar]
- Biere Arenas, R.; Marmolejo Duarte, C.; Crespo Sánchez, E.; Onecha Pérez, B. Percepción de beneficios y co-beneficios de las viviendas energéticamente eficientes. Un análisis para Barcelona. Rev. INVI 2023, 38, 260–290. [Google Scholar] [CrossRef]
- Sánchez, E.C.; Berrio, S.S.; Perez, B.O.; Marmolejo-Duarte, C. Perceived Benefits of Energy Efficiency in the Spanish Residential Market and Their Relation to Sociodemographic and Living Conditions. Appl. Sci. 2021, 11, 875. [Google Scholar] [CrossRef]
- Vandentorren, S.; Bretin, P.; Zeghnoun, A.; Mandereau-Bruno, L.; Croisier, A.; Cochet, C.; Ribéron, J.; Siberan, I.; Declercq, B.; Ledrans, M. August 2003 Heat Wave in France: Risk Factors for Death of Elderly People Living at Home. Eur. J. Public Health 2006, 16, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Chapman, J.A.; Terr, A.I.; Jacobs, R.L.; Charlesworth, E.N.; Bardana, E.J., Jr. Toxic mold: Phantom risk vs science. Ann. Allergy Asthma Immunol. 2003, 91, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Bjørner, T. Combining socio-acoustic and contingent valuation surveys to value noise reduction. Transp. Res. Part D Transp. Environ. 2004, 9, 341–356. [Google Scholar] [CrossRef]
- Toman, M. Special Section: Forum on Valuation of Ecosystem Services: Why not to calculate the value of the world’s ecosystem services and natural capital. Ecol. Econ. 1998, 25, 57–60. [Google Scholar] [CrossRef]
- Amecke, H. The Impact of Energy Performance Certificates: A Survey of German Home Owners. Energy Policy 2012, 46, 4–14. [Google Scholar] [CrossRef]
- Marmolejo-Duarte, C.; Spairani Berrio, S.; Moral-Ávila, D.; Méndez, L.D. The Relevance of EPC Labels in the Spanish Residential Market: The Perspective of Real Estate Agents. Building 2020, 10, 27. [Google Scholar] [CrossRef]
- Pachauri, R.K.; Allen, M.; Barros, V.; Broome, J.; Cramer, W.; Christ, R.; Church, J.; Clarke, L.; Dahe, Q.; Dasgupta, P. IPCC, 2014: Climate Change 2014: Synthesis Report. In Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2014; p. 151. [Google Scholar]
- Gao, J.; Xu, G.; Ma, W.; Zhang, Y.; Woodward, A.; Vardoulakis, S.; Kovats, S.; Wilkinson, P.; He, T.; Lin, H.; et al. Perceptions of Health Co-Benefits in Relation to Greenhouse Gas Emission Reductions: A Survey among Urban Residents in Three Chinese Cities. Int. J. Environ. Res. Public Health 2017, 14, 298. [Google Scholar] [CrossRef] [PubMed]
- Haines, A. Health benefits of a low carbon economy. Public Health 2012, 126 (Suppl. S1), S33–S39. [Google Scholar] [CrossRef] [PubMed]
- Vardoulakis, S.; Dear, K.; Wilkinson, P. Challenges and opportunities for urban environmental health and sustainability: The healthy-polis initiative. Environ. Health Glob. Access Sci. Source 2016, 15 (Suppl. S1), 30. [Google Scholar] [CrossRef] [PubMed]
- Ramos, B.A.; Cladera, J.R.; Cladera, J.R.; de Larrocha, C.S.; de Larrocha, C.S.; Santafé, M.D.M.; Santafé, M.D.M.; Arenas, R.M.B.; Arenas, R.M.B. Olas de Calor en la ciudad de Barcelona: 1971–2020. ACE Archit. City Environ. 2022, 17, 11684. [Google Scholar] [CrossRef]
- Ürge-Vorsatz, D.; Herrero, S.T.; Dubash, N.K.; Lecocq, F. Measuring the Co-Benefits of Climate Change Mitigation. Annu. Rev. Environ. Resour. 2014, 39, 549–582. [Google Scholar] [CrossRef]
- ANSI/ASHRAE Standard 55:2017; Thermal Environmental Conditions for Human Occupancy. ASHRAE: Atlanta, GA, USA, 2017.
- UNE-EN ISO 10551:2019; Ergonomics of the Physical Environment—Subjective Judgement Scales for Assessing Physical Environments. European Committee for Standardization: Brussels, Belgium, 2019.
- INE. National Institute of Statistics. Number of Households (Main Dwellings) in the 2021 Census. Available online: https://www.ine.es (accessed on 29 September 2023).
- Escofet i Figueras, J. Obtenció d’un Indicador Microterritoal de Renda Familiar Disponible a Partir de Dades Macroterritorials Contrastació Empírica a Nivel de Sección Censal: El cas de Terrasa. Ph.D. Thesis, Universitat Politècnica de Catalunya, Barcelona, Spain, 2016. Available online: https://upcommons.upc.edu/handle/2117/105137 (accessed on 2 June 2023).
- Wang, J.; Guan, Y.; Wu, L.; Guan, X.; Cai, W.; Huang, J.; Dong, W.; Zhang, B. Changing Lengths of the Four Seasons by Global Warming. Geophys. Res. Lett. 2021, 48, e2020GL091753. [Google Scholar] [CrossRef]
- Larson, R.B. Co Controlling Social Desirability Bias. Int. J. Mark. Res. 2018, 61, 534–547. [Google Scholar] [CrossRef]





| No | In-Depth Interview Topic | Interviewee | Date, Roll, and Affiliation |
|---|---|---|---|
| 1 | Introduction to co-benefits and cost-effectiveness assessment | Federico Dell’Anna | 31 April 2022 Research Professor—Polytechnic University of Turin |
| Summary: To understand different methods to quantify the co-benefits of improved building efficiency. | |||
| 2 | Review of previous surveys | Tian Weijia | 21 December 2022 Research Professor—Tongji University |
| Summary: Review the advance and critique of the method and analysis of the prior epidemiological survey, Health Survey of Catalonia—ESCA in Spanish—2022. | |||
| 3 | Review of survey draft | Deng Linshuang | 23 February 2023 Post-Doctor Researcher–Tongji University |
| Summary: Categorise the five topics in the survey based on the hypothesis and research question. | |||
| 4 | Review of survey draft | Joana Aina Ortiz Ferra | 23 February 2023 Deputy Head of Thermal Energy and Building Performance—Fundació Institut de Recerca en l’Energia de Catalunya (IREC) |
| Summary: Apply the survey based on the ASHRAE 55 standard that measures comfort. | |||
| 5 | Review of survey draft | Belen Onecha Perez | 24 February 2023 Research Professor—Polytechnic University of Catalonia |
| Qualitative Study Technical Sheet | Structure of the Survey Request | Answer Format | Statistical Reliability (Cronbach’s Alpha) | |
|---|---|---|---|---|
| Research scope | Barcelona municipality | 1.1 Which floor do you live on? | Closed, multiple choice | n.a. |
| Type of study | Primary qualitative descriptive and segmented study | 1.2 Typology of your apartment | Closed, single option | n.a. |
| Research technique | Face-to-face and online surveys | 1.3 Main orientation of your apartment | Closed, multiple choice | n.a. |
| Data collection instrument | A survey using ten closed-response Likert-scale questions, five closed-response single-choice questions, eight closed-response multiple-choice questions, three open-response free-text questions, and two matrix questions | 1.4 Period of construction of your apartment | Closed, multiple choice | n.a. |
| Type of sample survey | Consecutive and stratified by sex and socio-professional in order to be accessible and representative of the study group | 1.5 How much, on average, is your monthly electricity bill? | Open, free option | n.a. |
| Survey sample size | A total of 127 valid cases have been collected in the 10 districts of Barcelona, Spain, with a response rate of 9% from the neighbourhood associations | 1.6 How much, on average, is your monthly gas bill? | Open, free option | n.a. |
| Survey error level | A total of 7% for global data in the assumed simple random sampling at a 90% confidence level, and p-q-0.5 | 1.7. Does your dwelling have external wall insulation? | Closed, single option | n.a. |
| Data collection period | 25 March 2023 to 31 July 2023 | 1.8 Specify whether your exterior window glasses are original or whether you have upgraded them. | Matrix option | n.a. |
| Research | EnerValor 2 research project | 1.9 Specify whether your window frames are original or whether you have upgraded them. | Matrix option | n.a. |
| 1.10 Do you have a heating system in your apartment? | Closed, single option | n.a. | ||
| 1.11 What type of heating system is installed in your apartment? | Closed, multiple-choice | n.a. | ||
| 1.12 Do you have air conditioning installed in your apartment? | Closed, single option | n.a. | ||
| 2.1 How satisfied are you with the level of external street noise? | Closed, Likert scale | 0.489 | ||
| 2.2 How satisfied are you with the indoor air quality in your apartment? | Closed, Likert scale | 0.721 | ||
| 2.3 How satisfied are you with dampness problems, such as leaks or condensation? | Closed, Likert scale | 0.524 | ||
| 2.4 How do you perceive thermal comfort in summer? | Closed, Likert scale | 0.401 | ||
| 2.5 How do you perceive thermal comfort in winter? | Closed, Likert scale | 0.462 | ||
| 2.6 Please indicate any other problems in your apartment. | Free text | n.a. | ||
| 3.1 What would you say your general health is like? | Closed, Likert scale | n.a. | ||
| 3.2 Have you had any cardiovascular disease? | Closed multiple choice | n.a. | ||
| 3.3 Have you ever had a respiratory illness? | Closed multiple choice | n.a. | ||
| 3.4 Housing conditions have an impact on cardio/respiratory diseases? | Closed, Likert scale | 0.821 | ||
| 3.5 Housing conditions have an impact on mental health? (depression, etc.) | Closed, Likert scale | 0.876 | ||
| 3.6 Do housing conditions have an impact on your health? | Closed, Likert scale | 0.861 | ||
| 4.1 Are you willing to undertake energy retrofit in your apartment? | Closed, Likert scale | n.a. | ||
| 4.2 Which of these aspects of your dwelling would you be willing to... | Closed, single option | n.a. | ||
| 4.3 If you were to carry out an energy retrofit, which would you… | Closed, multiple choice | n.a. | ||
| 4.4 What makes it difficult for you to carry out an energy retrofit? | Closed, multiple choice | n.a. | ||
| Items | Study Participants (N, %) | Target Population (%) |
|---|---|---|
| Barcelona municipality | 127 | 1.63 million (in 2022) |
| Gender | ||
| Male | 54 (42.5%) | 47.59% |
| Female | 73 (57.5%) | 52.41% |
| Idem | Features | Inputs |
|---|---|---|
| KE-1 | Woman; 44 years old; Spanish; architect and professor. A resident of the Sant Gervasi neighbourhood; an expert in insulation and thermal materials. | Point 1.3. The east and west façade is added. Point 1.9. The iron carpentry is changed to steel. Point 6.8. It is specified that it is net per month. |
| KE-2 | Female; 37 years old; Spanish. Deputy Director of Thermal Energy and Building Performance. | Design comfort questions are based on the ASHRAE 55 standard. |
| KE-3 | Female; 21 years old; Spanish; law student. | Point 6.2. Ownership regime. A section is added with others to specify children who are living in the parents’ house and do not own or rent. In addition, persons living in a concession of the use of the building. |
| KE-4 | Male; 35 years old; Spanish. Neighbour and president of the AAVV Verneda. He has lived in the neighbourhood all his life. | Understanding technical terms to simplify them and other problems with housing such as asbestos, aluminosis, or leaks. |
| KE-5 | Male; 38 years old; British. Comedian; 29 years in Spain. Resident of Sant Antoni. | Points 3.4, 3.5, and 3.6. Replace “The conditions of your dwelling …” with “the conditions of the dwelling in general...”. |
| KE-6 | Male; 45 years old; Spanish. Engineer. Resident of Parc Vall d’Hebron. | Point 1.10. The term “aerothermal” heat pump is changed to just “heat pump”. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benites-Aguilar, C.; Marmolejo-Duarte, C. Assessment of Households’ Perceptions of Health Co-Benefits in Relation to the Willingness to Undertake Energy Retrofits in Barcelona. Buildings 2024, 14, 236. https://doi.org/10.3390/buildings14010236
Benites-Aguilar C, Marmolejo-Duarte C. Assessment of Households’ Perceptions of Health Co-Benefits in Relation to the Willingness to Undertake Energy Retrofits in Barcelona. Buildings. 2024; 14(1):236. https://doi.org/10.3390/buildings14010236
Chicago/Turabian StyleBenites-Aguilar, Carlos, and Carlos Marmolejo-Duarte. 2024. "Assessment of Households’ Perceptions of Health Co-Benefits in Relation to the Willingness to Undertake Energy Retrofits in Barcelona" Buildings 14, no. 1: 236. https://doi.org/10.3390/buildings14010236
APA StyleBenites-Aguilar, C., & Marmolejo-Duarte, C. (2024). Assessment of Households’ Perceptions of Health Co-Benefits in Relation to the Willingness to Undertake Energy Retrofits in Barcelona. Buildings, 14(1), 236. https://doi.org/10.3390/buildings14010236