
Positive Effects of Advanced Daylight Supply of Buildings on Schoolchildren—A Controlled, Single-Blinded, Longitudinal, Clinical Trial with Real Constructive Implementation

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
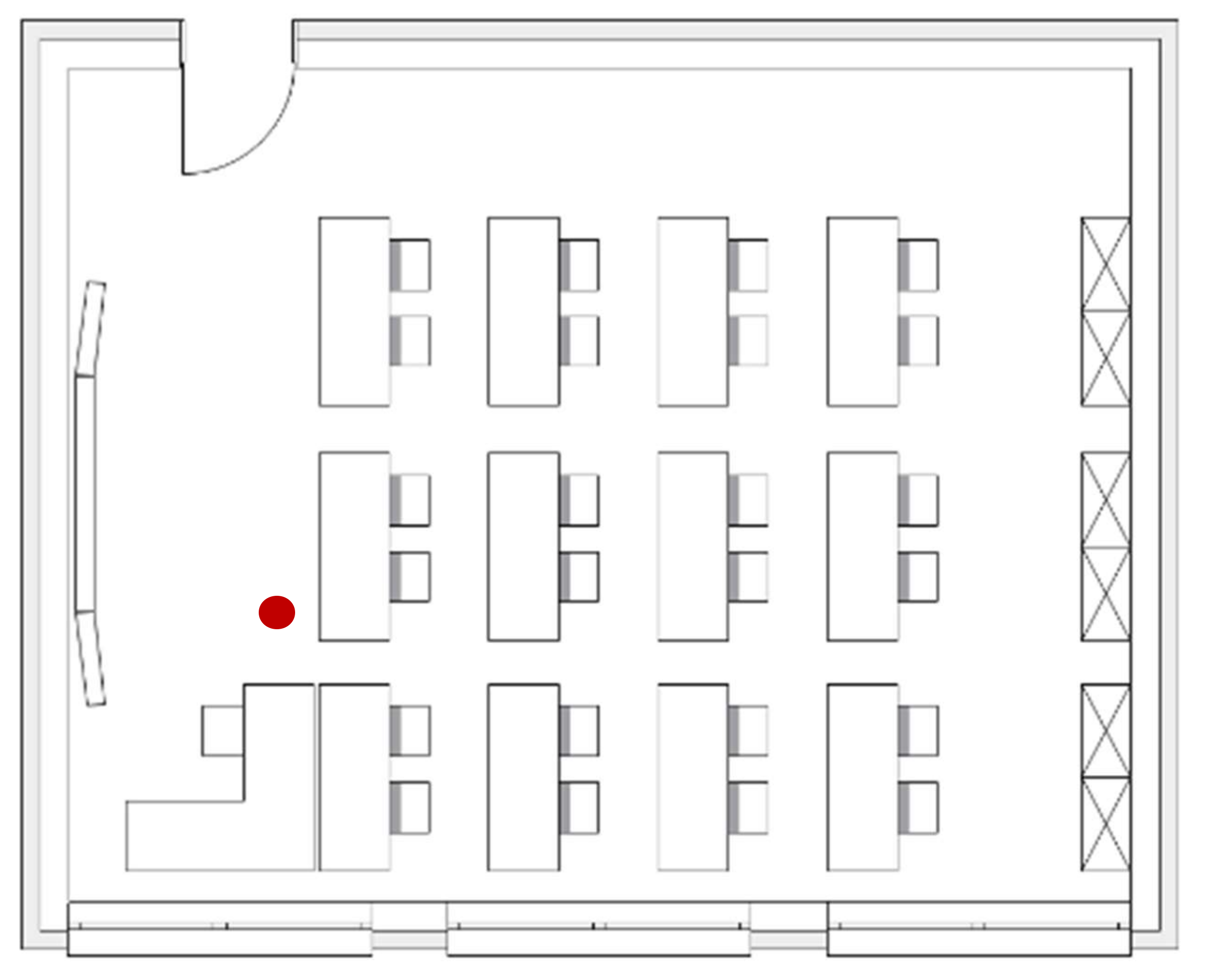
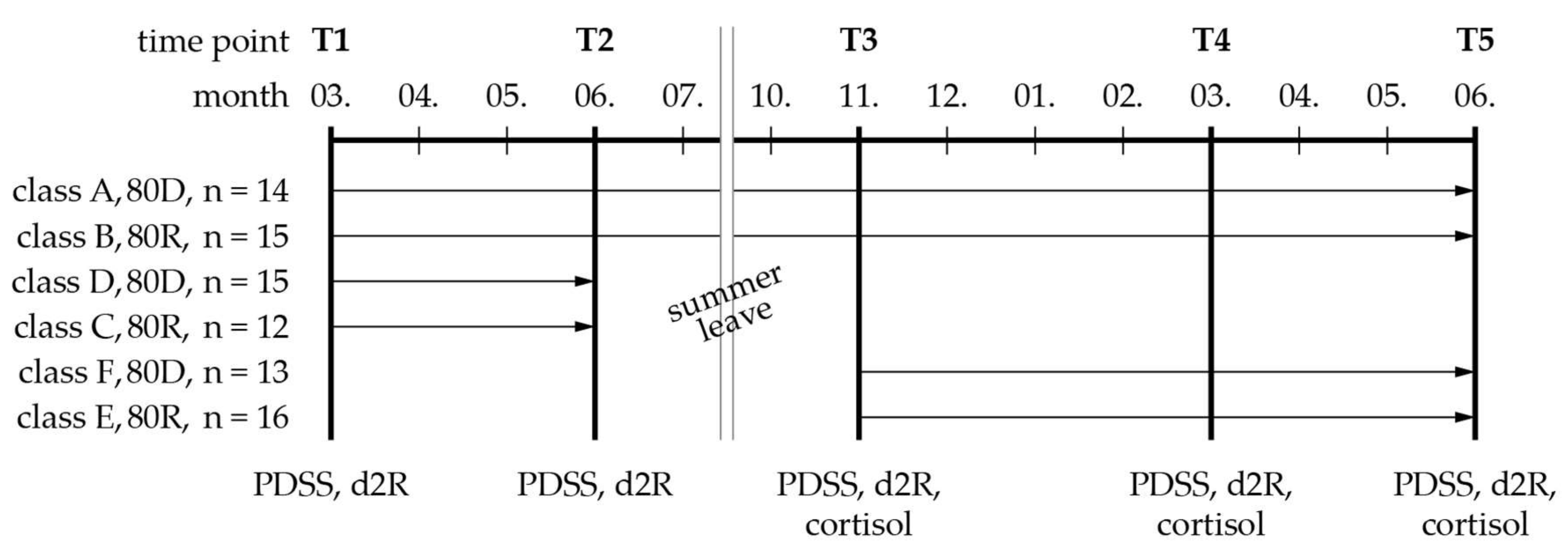
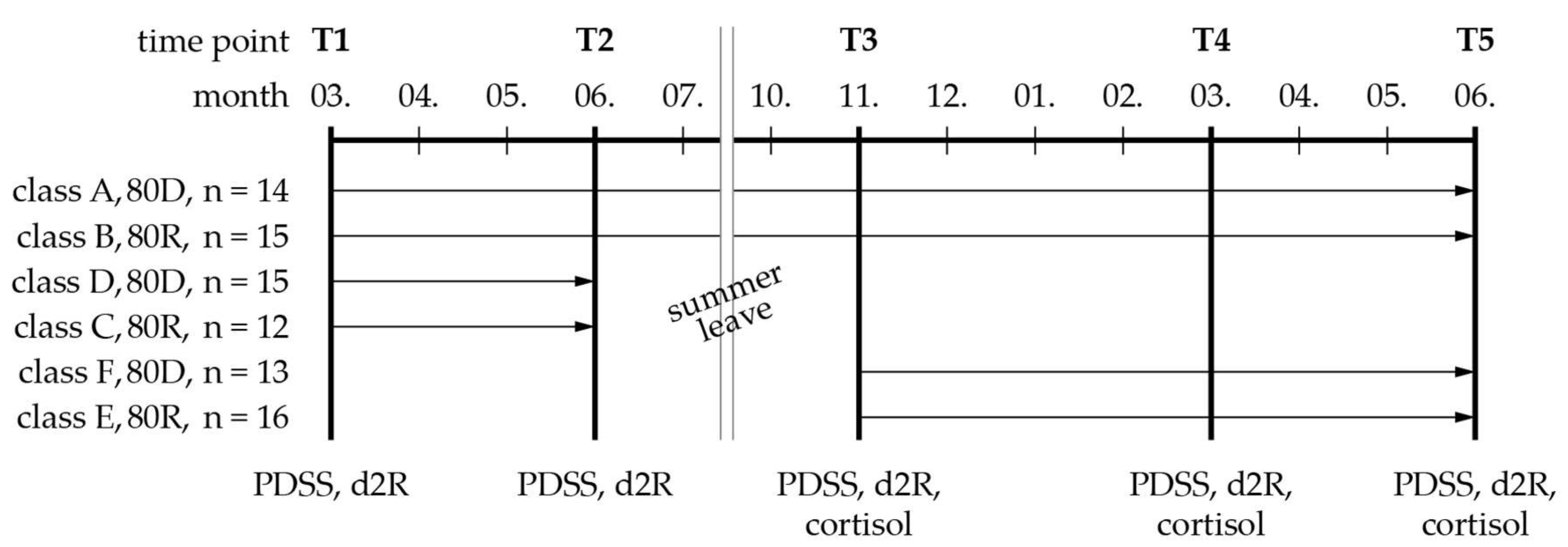
2.1. Study Design and Setting
2.2. Study Population
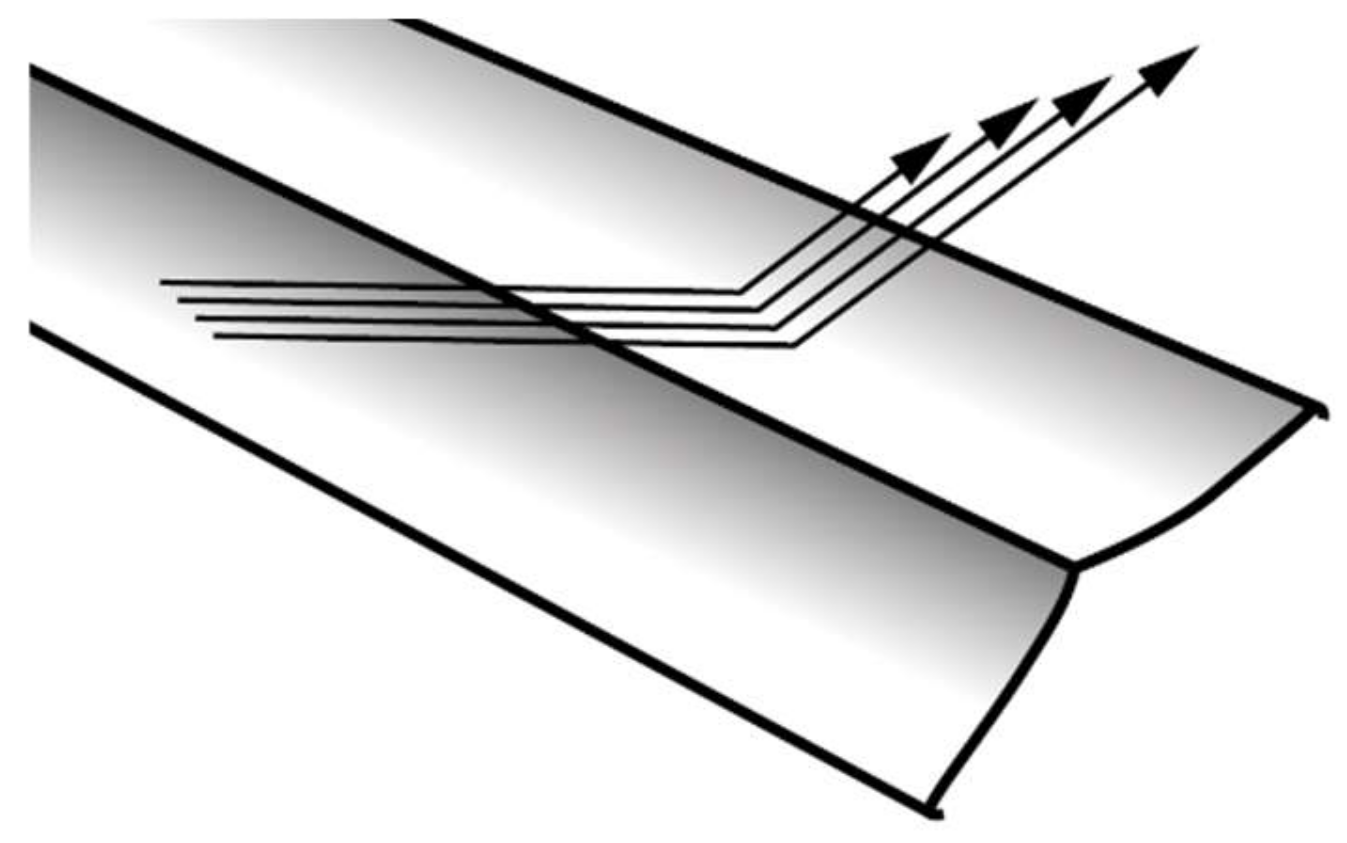
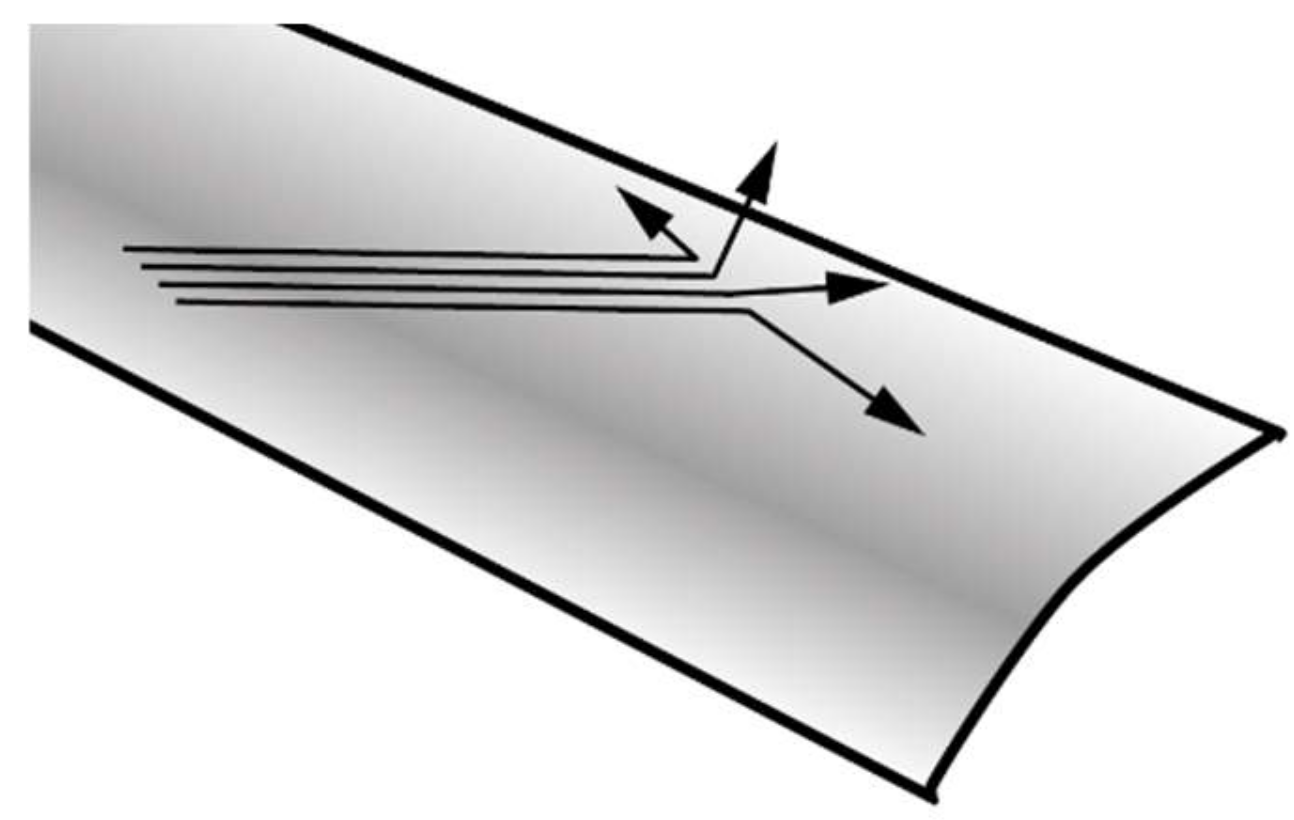
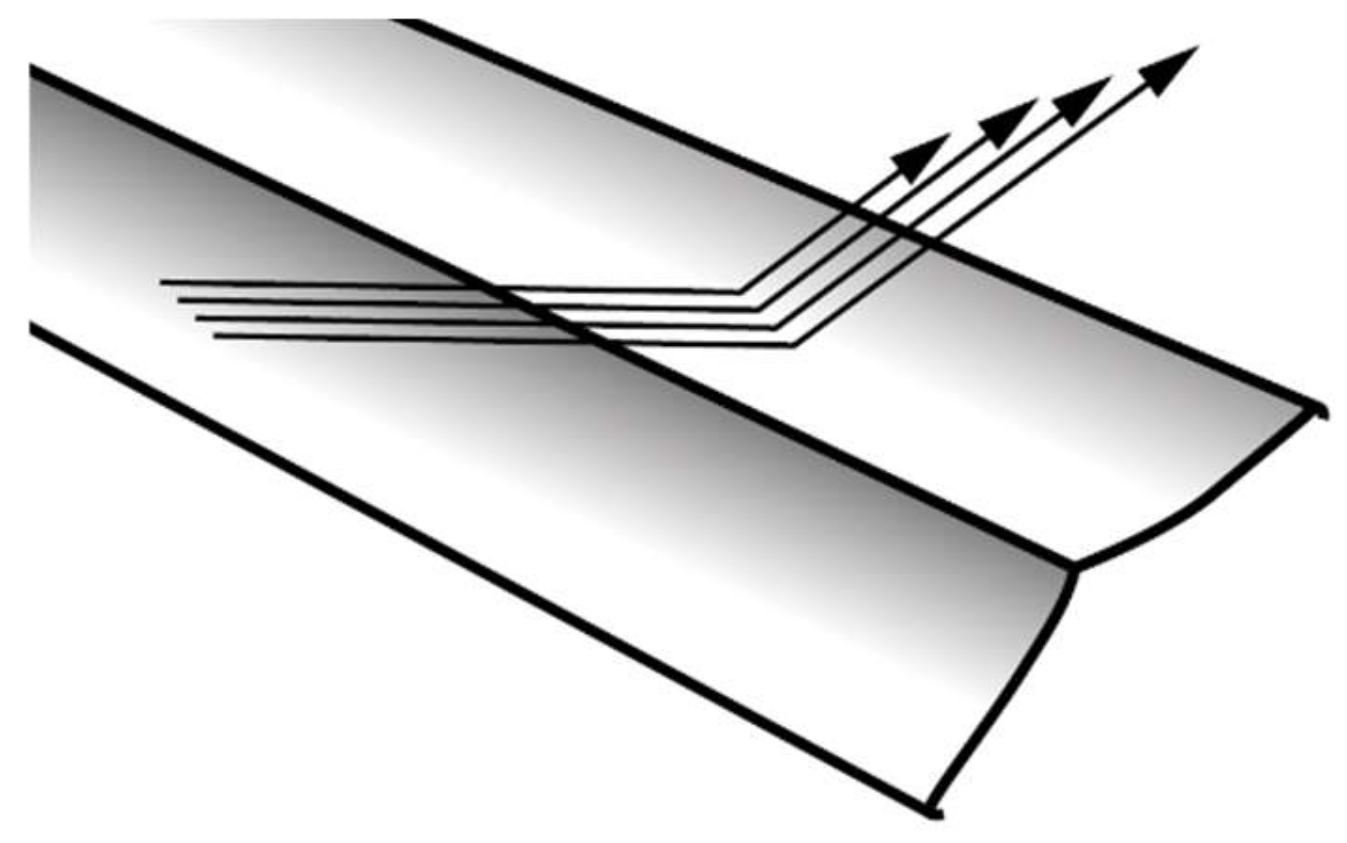
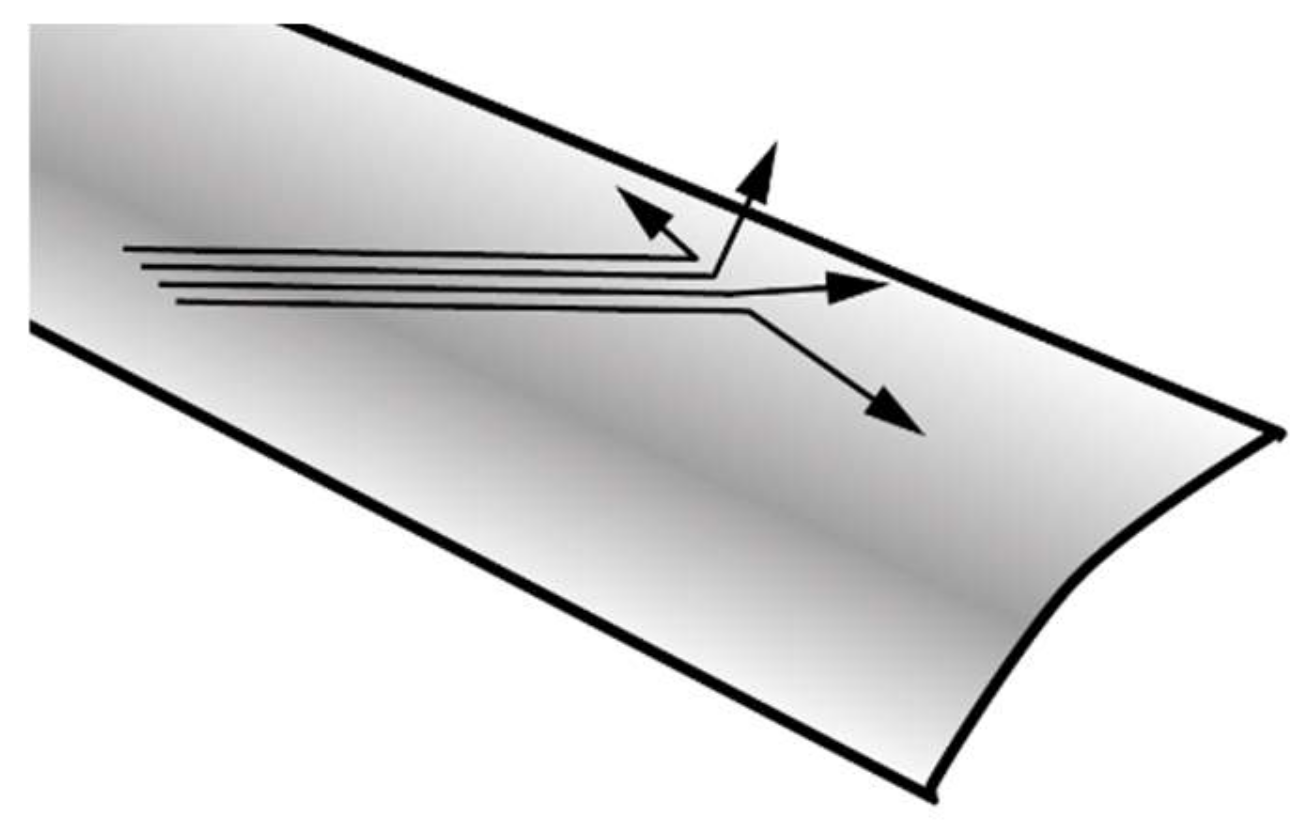
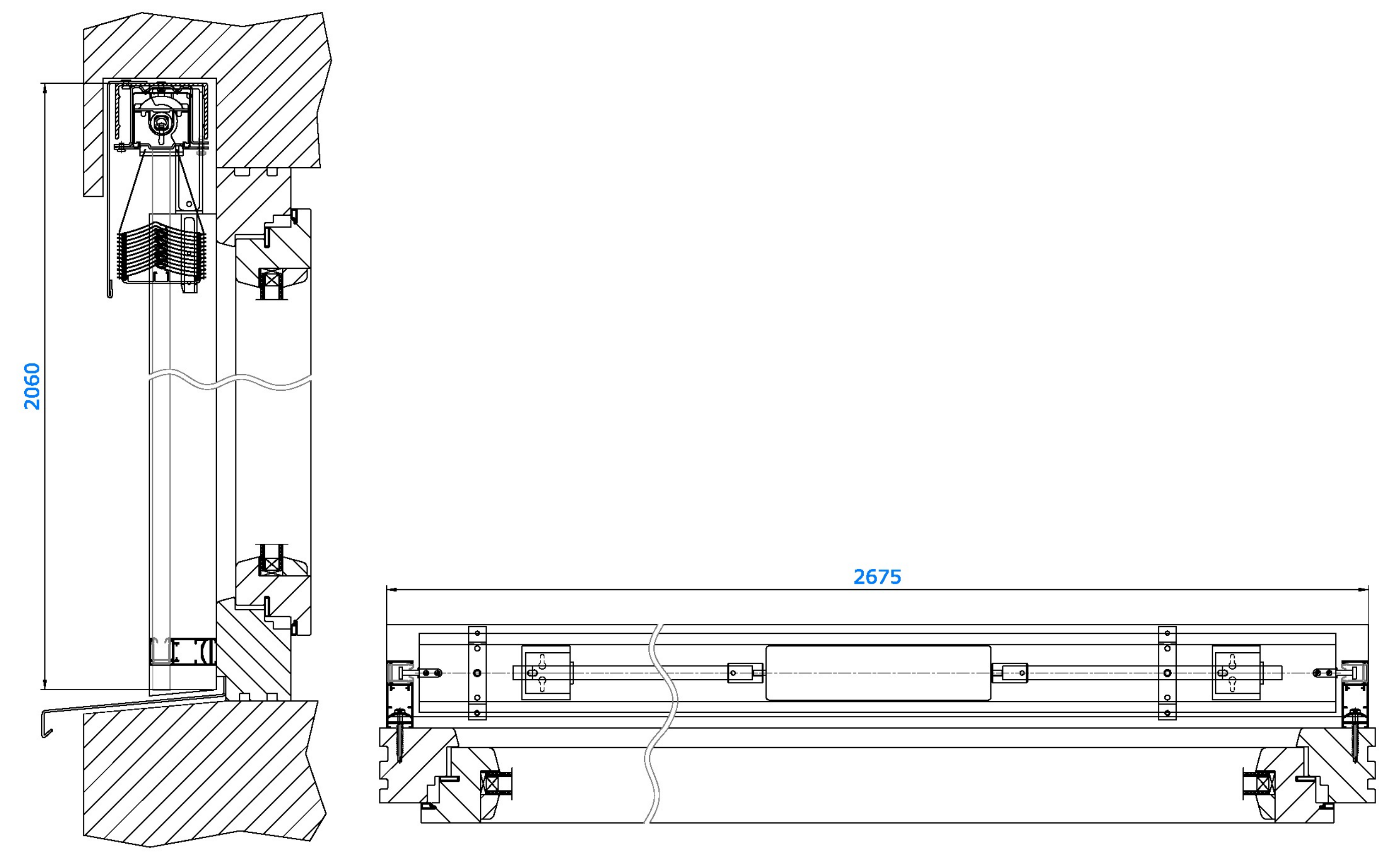
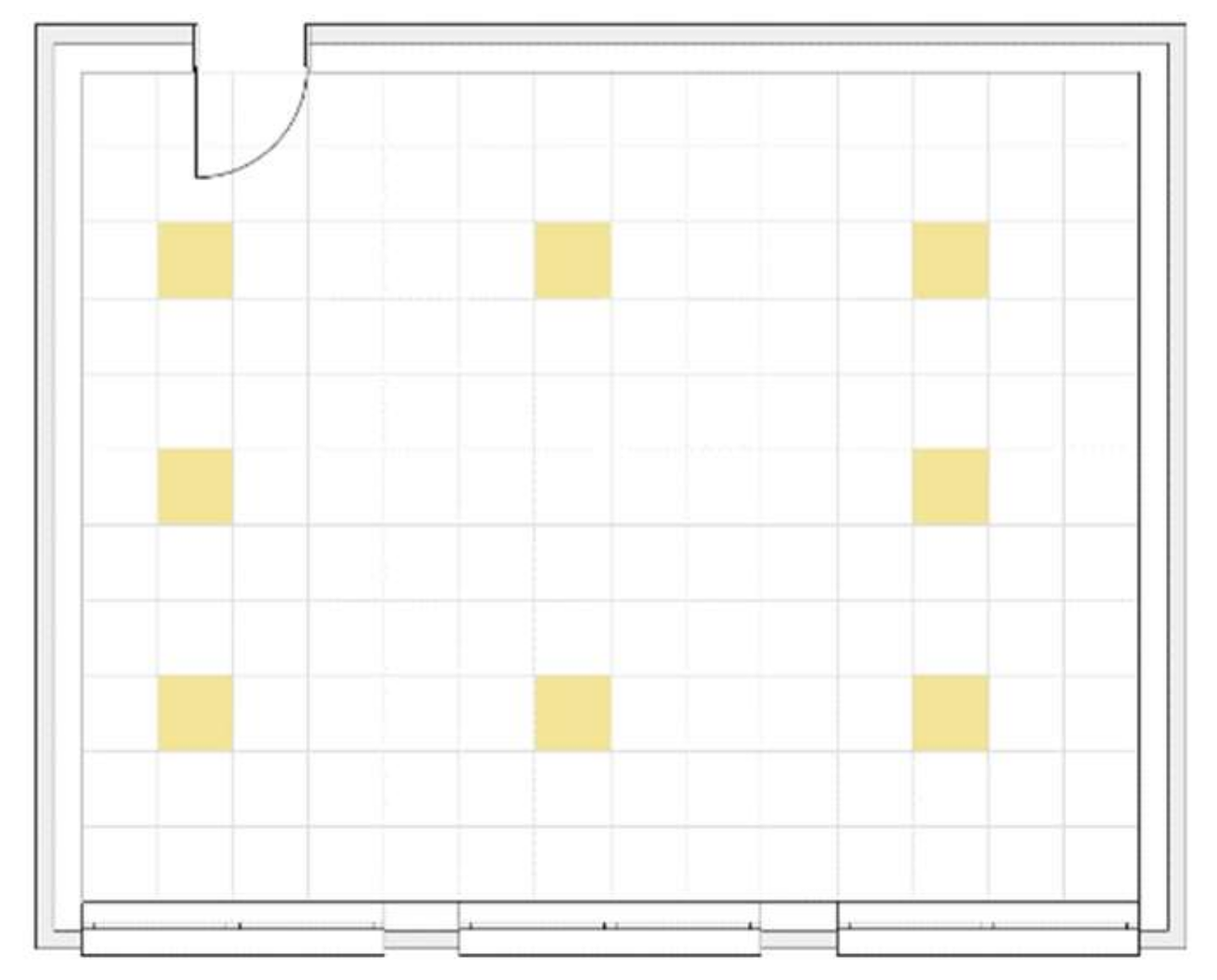
2.3. Intervention
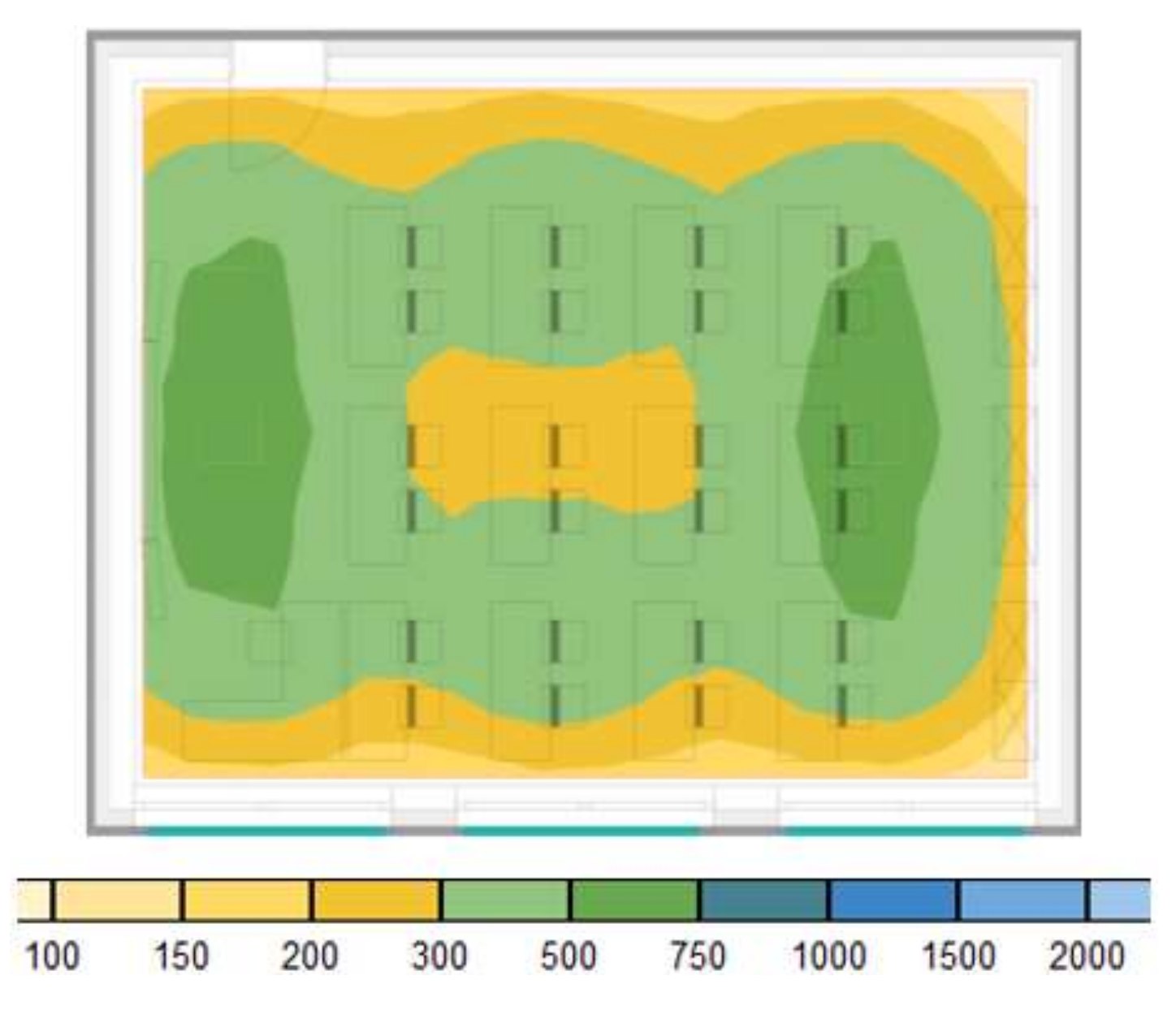
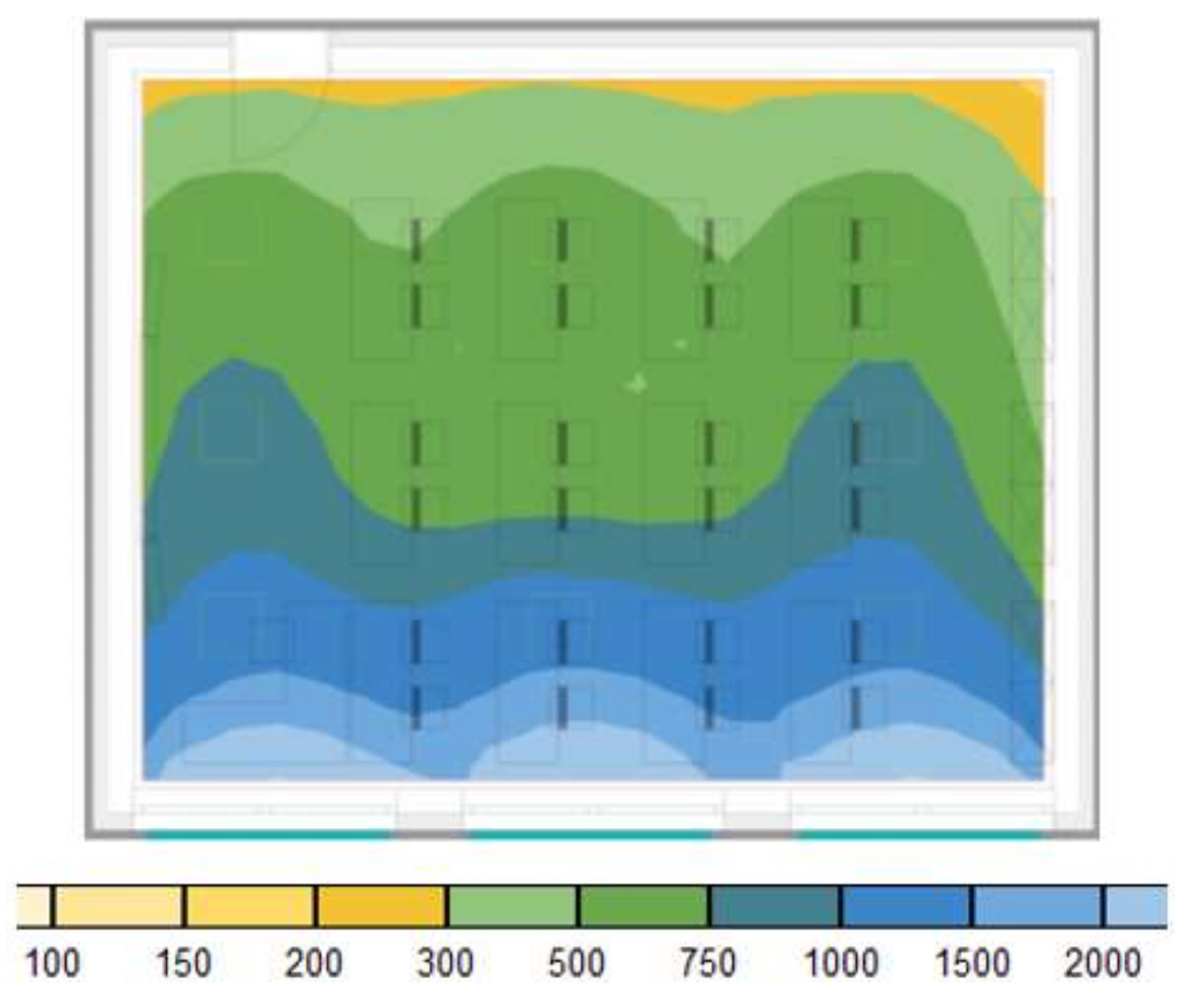
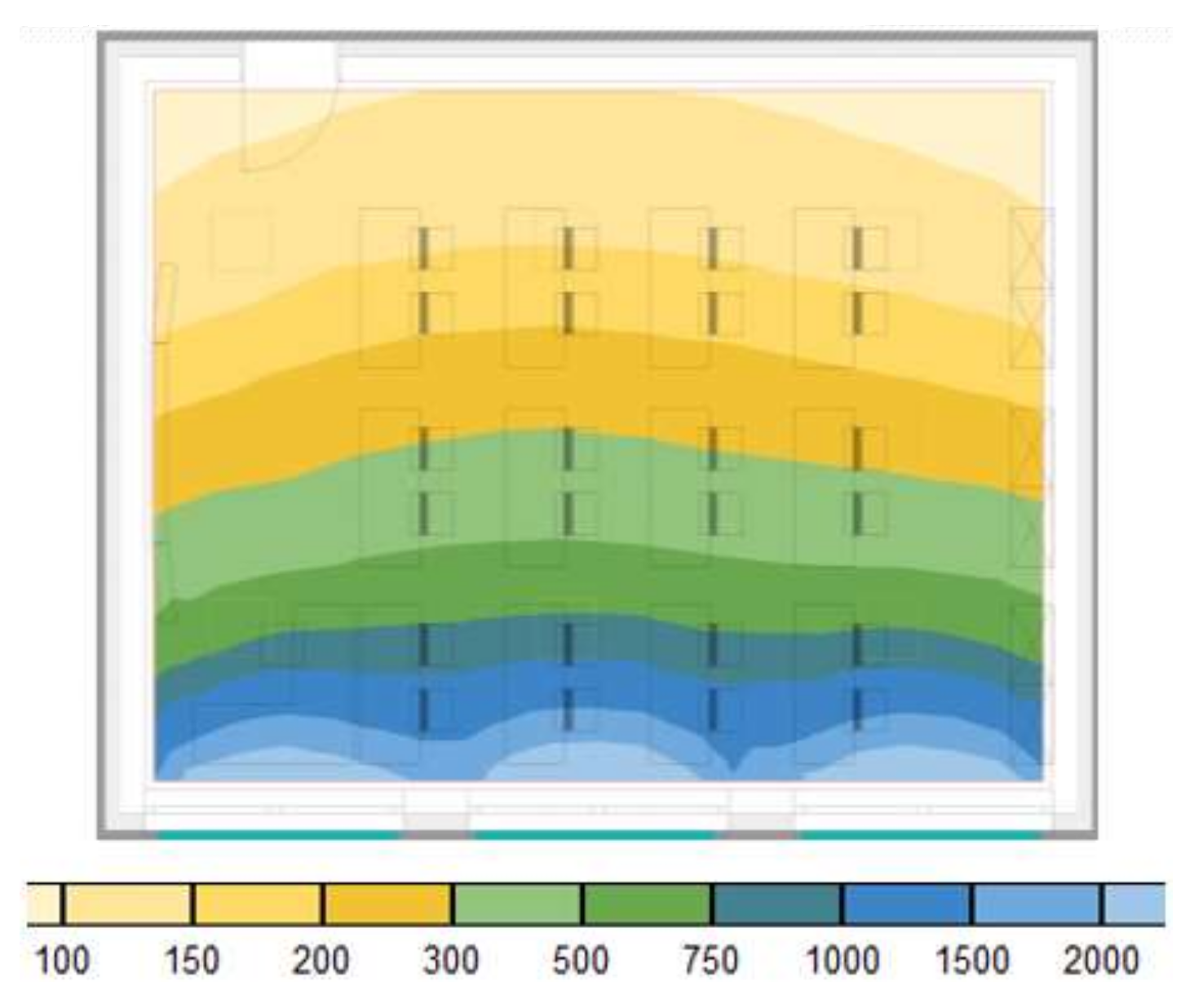
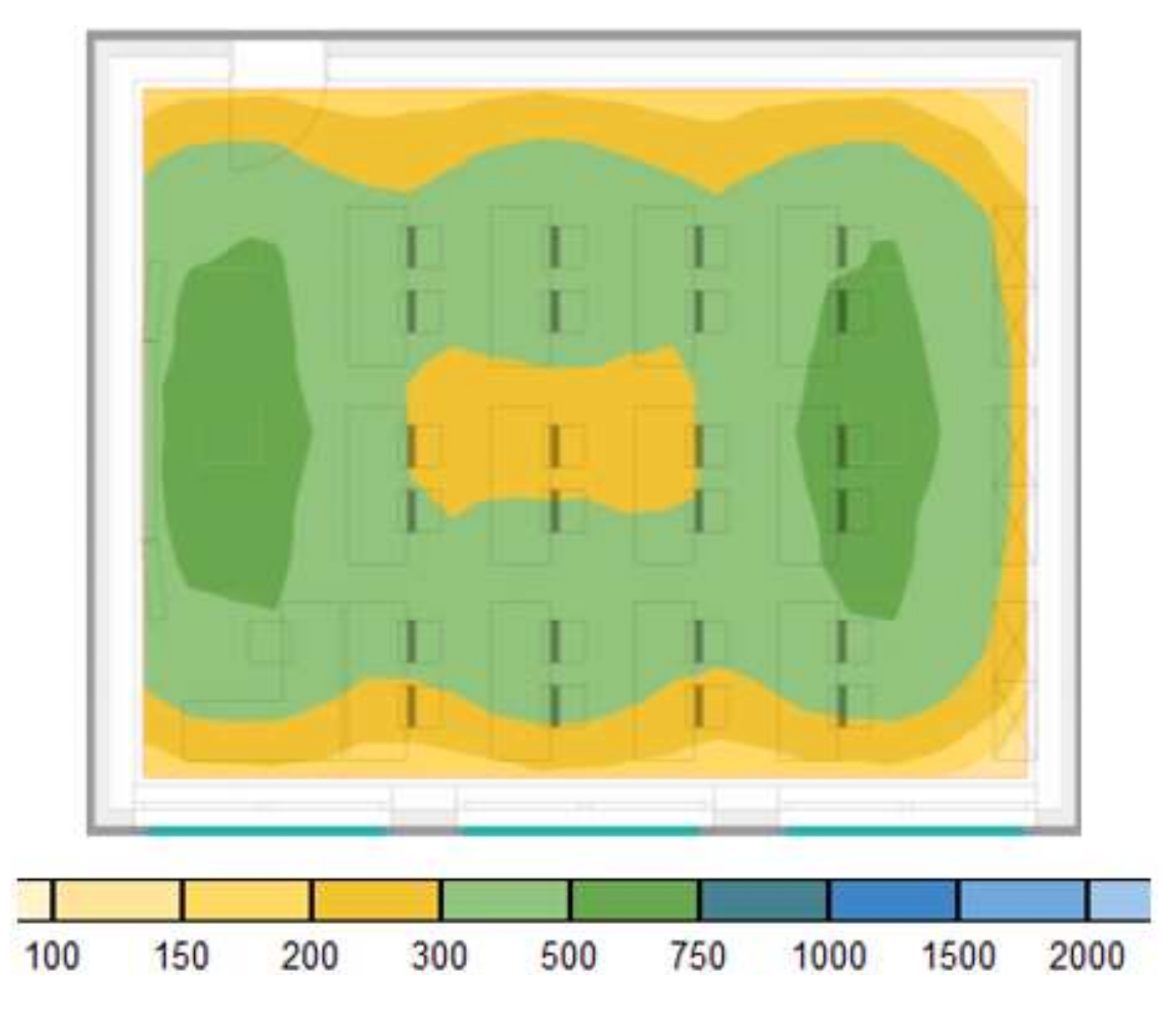
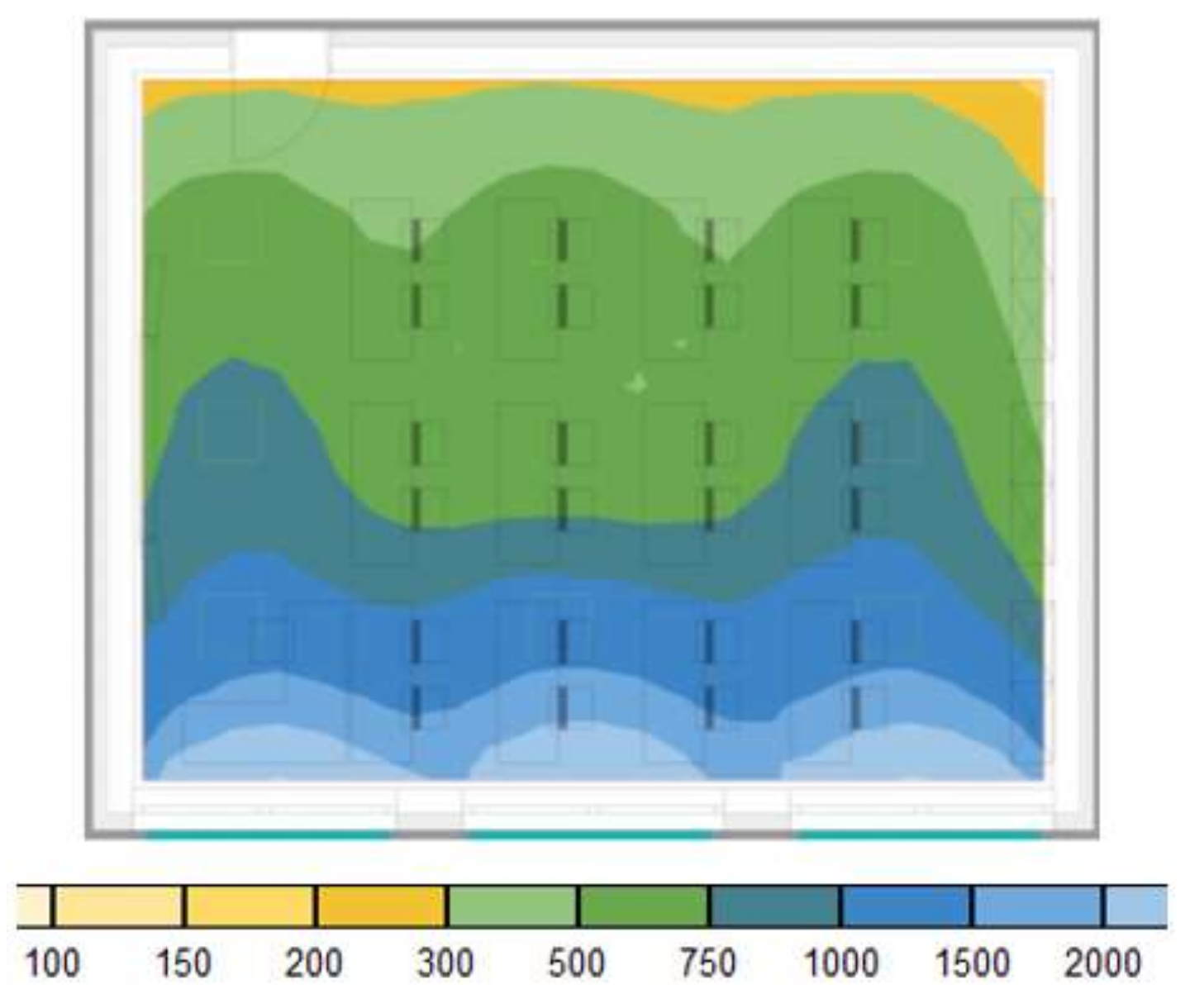
- 8% to 33% at the back of the room;
- −10% to 47% at the front of the room;
- 53% to 63% at the room’s ceiling.
2.4. Building Specifications
2.5. Outcomes
2.5.1. Data Collection
2.5.2. Salivary Cortisol
2.5.3. Sleepiness and Sleep Duration
2.5.4. Concentration
2.5.5. Visual Analogue Scales
2.6. Sample Size, Randomization, and Blinding
2.7. Statistical Methods
3. Results
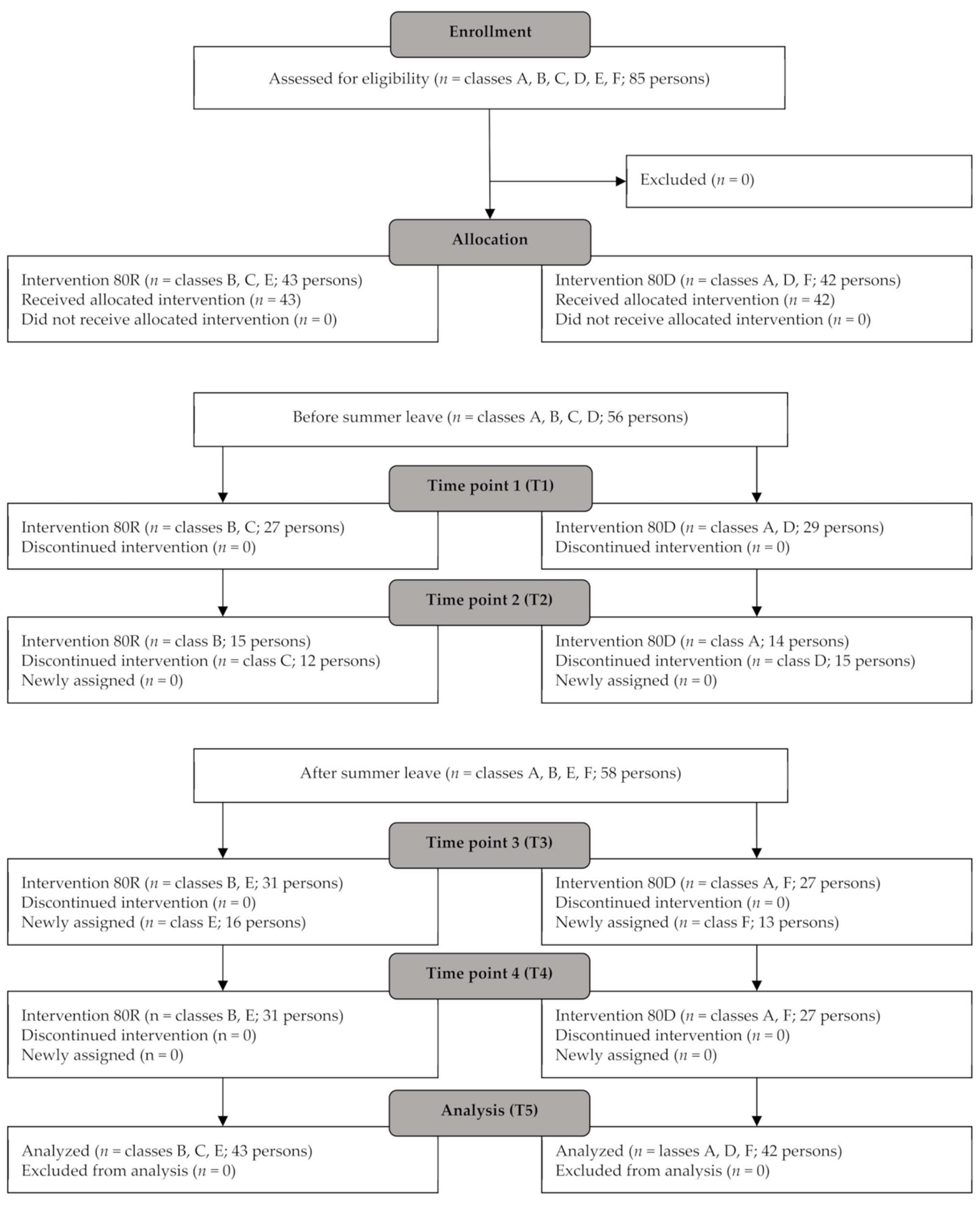
3.1. Study Participants, Baseline Characteristics, and CONSORT Flow Diagram
3.2. Indoor Air Quality
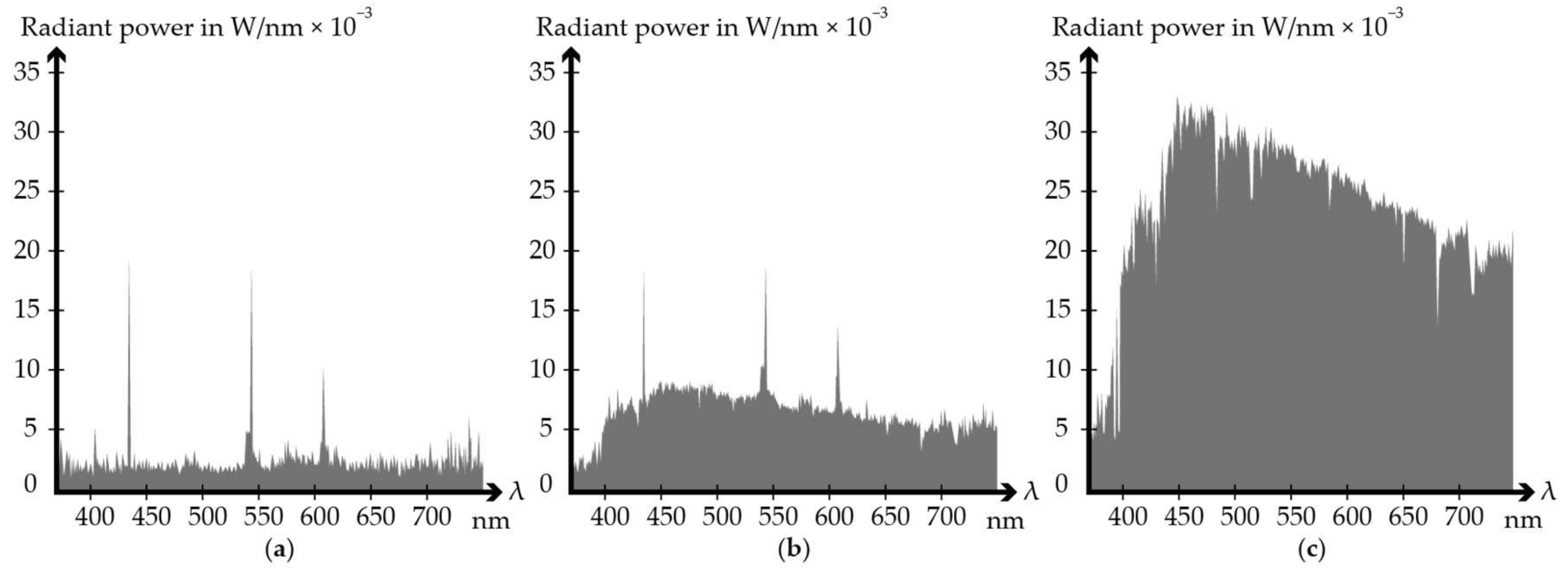
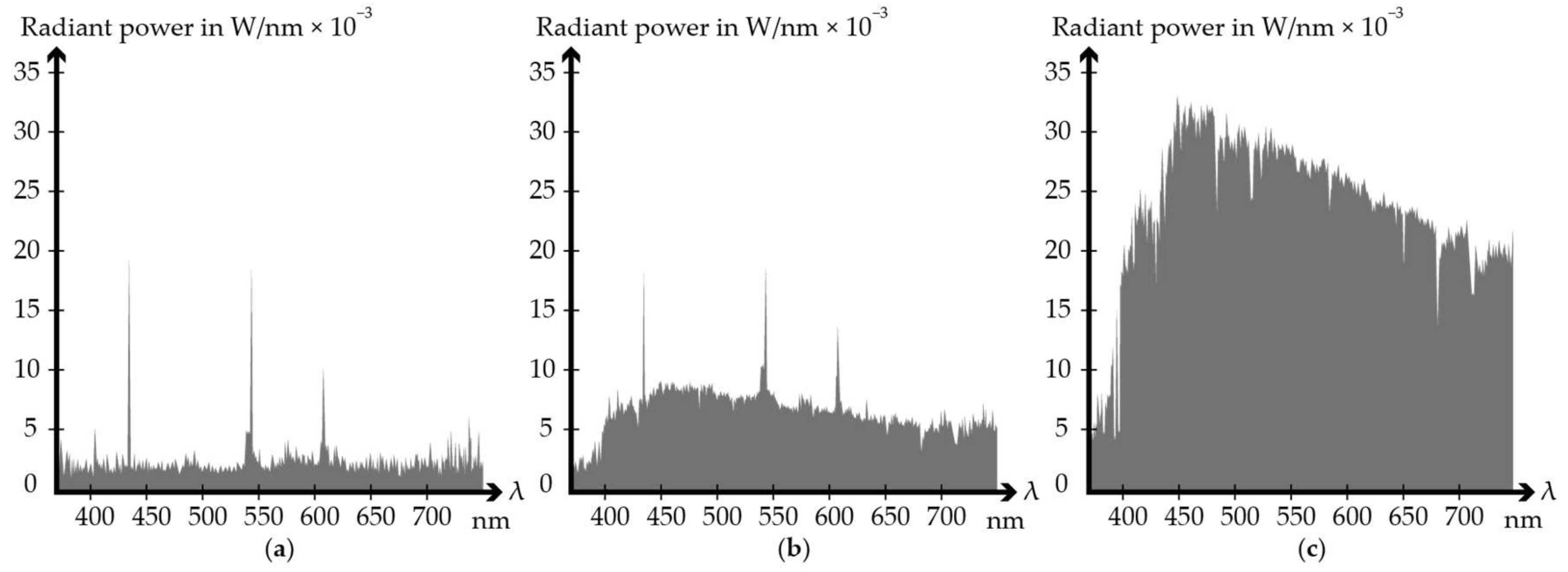
3.3. Artificial lighting
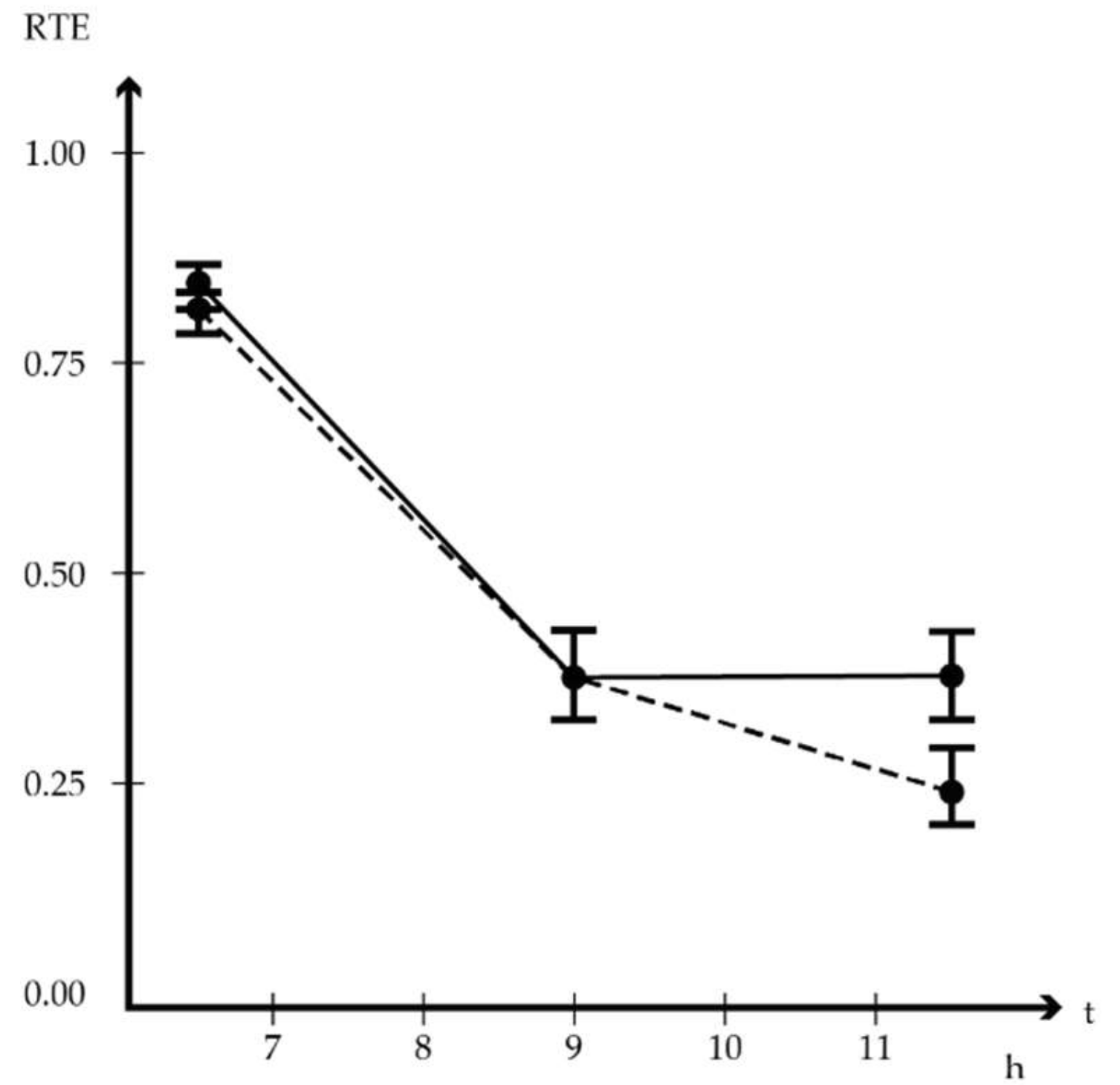
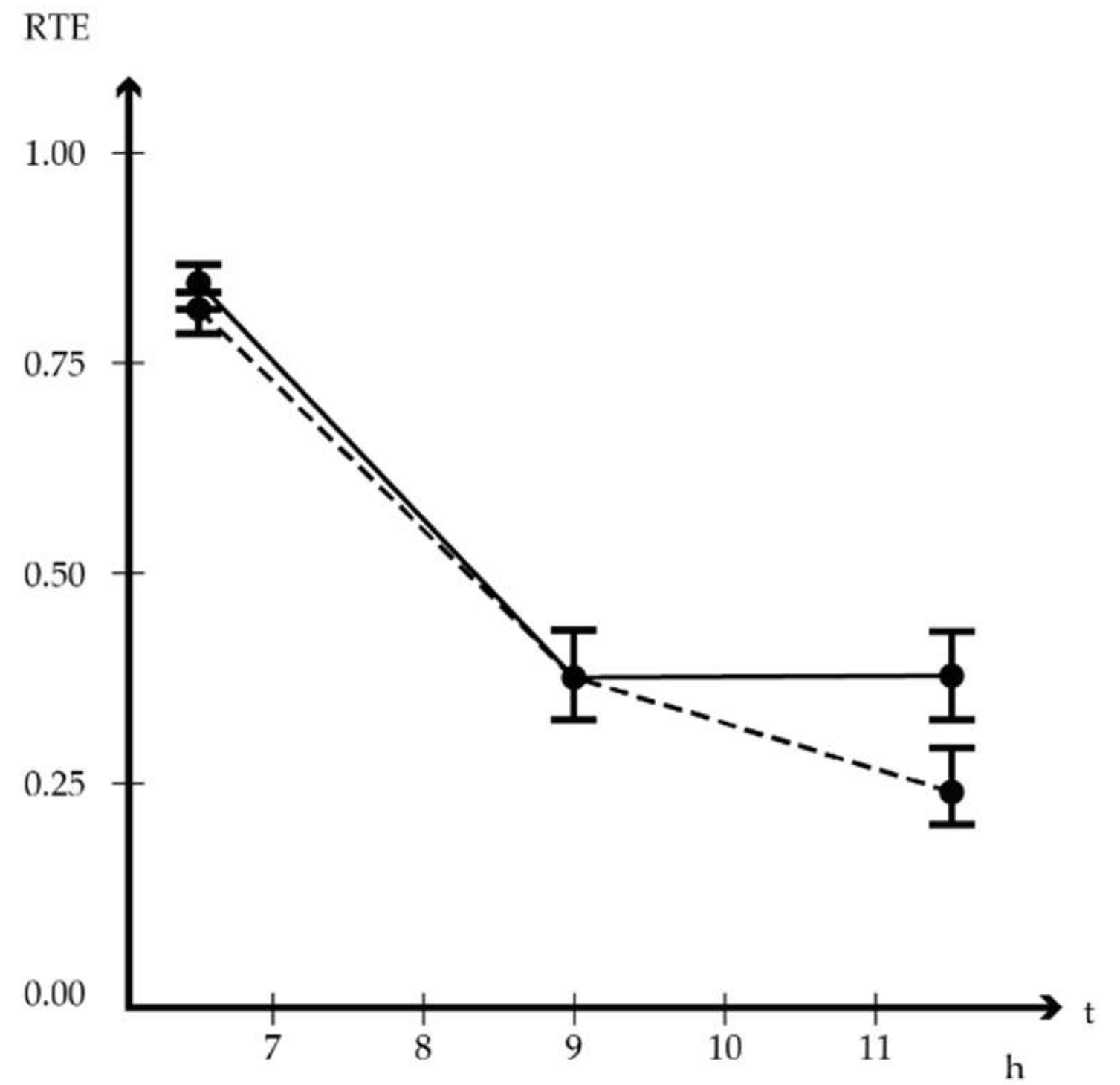
3.4. Cortisol
3.5. PDSS Pediatric Daytime Sleepiness Questionnaire, Sleep Duration, and d-2R Concentration
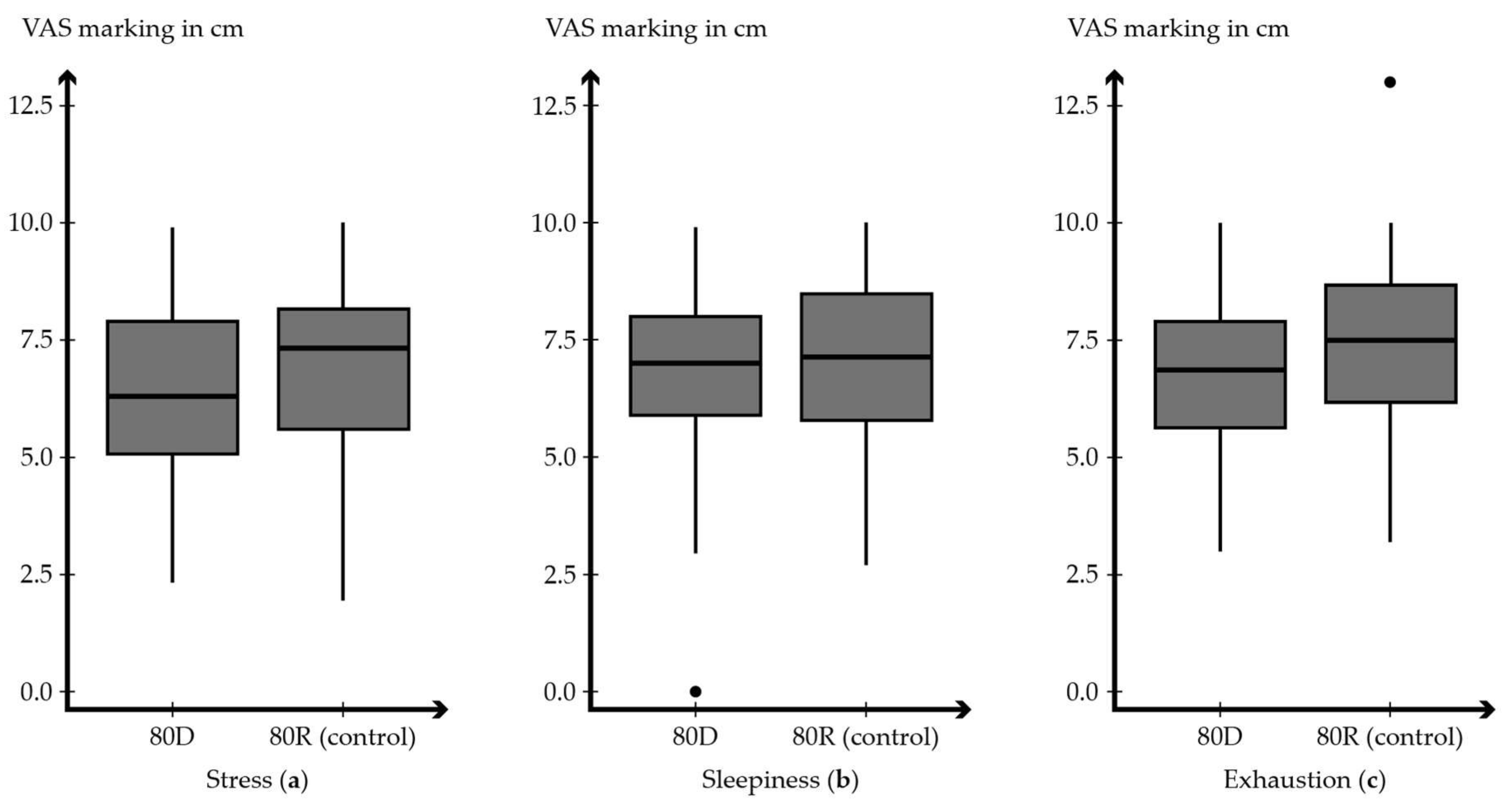
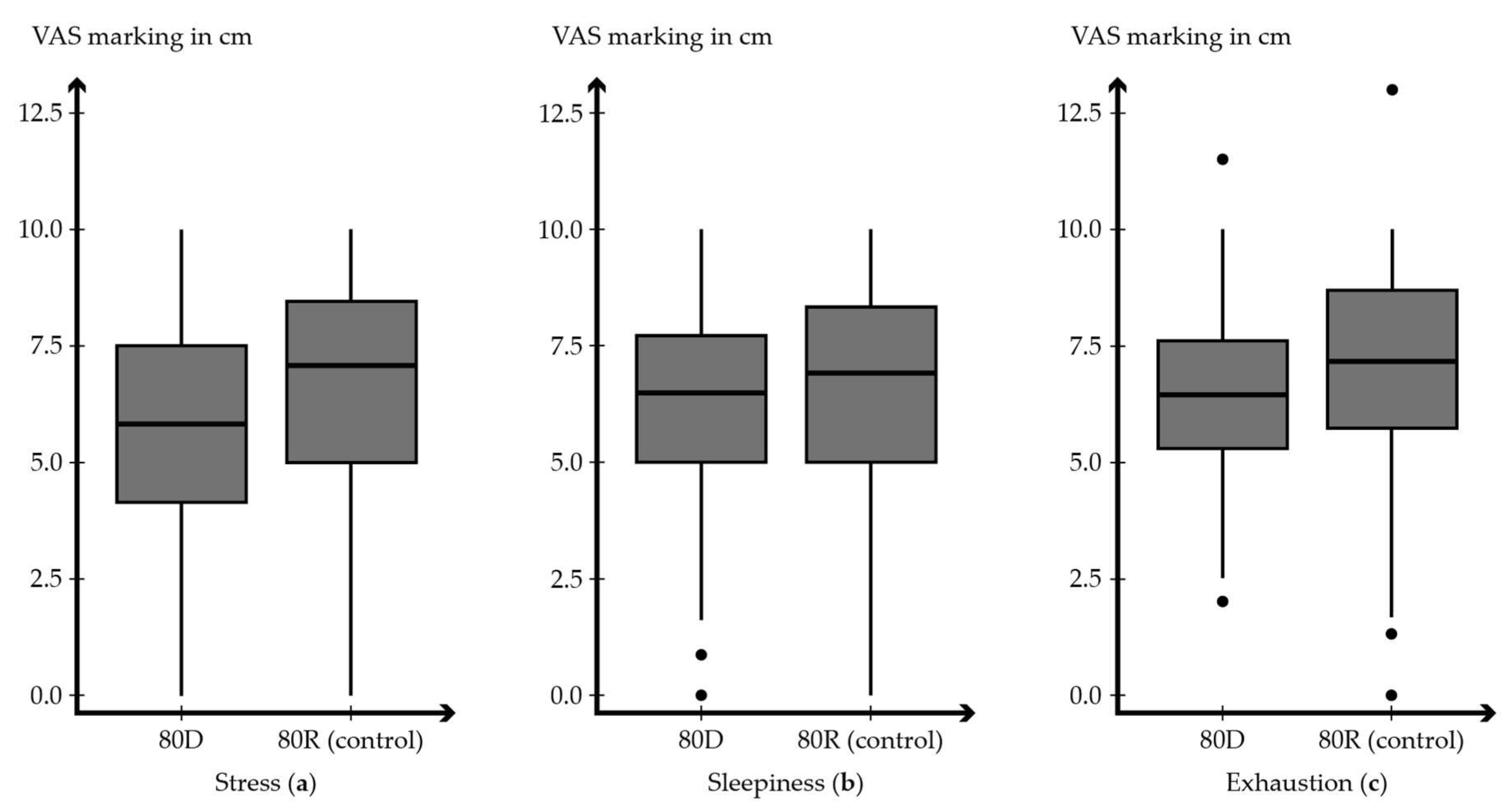
3.6. Visual Analogue Scales
4. Discussion
Limitations
5. Conclusions
- Advanced daylight supply can improve cortisol balance in schoolchildren.
- Providing more natural light can lower daytime sleepiness, even if sleep duration decreases.
- Indoors, the benefits of natural light can be obtained by utilizing innovative technology.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Houser, K.; Boyce, P.; Zeitzer, J.; Herf, M. Human-centric lighting: Myth, Magic or Metaphor? Lighting Res. Technol. 2020, 53, 97–118. [Google Scholar] [CrossRef]
- Elverson, C.A.; Wilson, M.E. Cortisol: Circadian Rhythm and Response to a Stressor. Newborn Infant Nurs. Rev. 2005, 5, 159–169. [Google Scholar] [CrossRef]
- Arendt, D. Evolution of eyes and photoreceptor cell types. Int. J. Dev. Biol. 2003, 47, 563–571. [Google Scholar]
- Hernández-Andrés, J.; Romero, J.; Nieves, J.L.; Lee, R.L. Color and spectral analysis of daylight in southern Europe. J. Opt. Soc. Am. A 2001, 18, 1325. [Google Scholar] [CrossRef]
- Judd, D.B.; MacAdam, D.L.; Wyszecki, G.; Budde, H.W.; Condit, H.R.; Henderson, S.T.; Simonds, J.L. Spectral Distribution of Typical Daylight as a Function of Correlated Color Temperature. J. Opt. Soc. Am. 1964, 54, 1031. [Google Scholar] [CrossRef]
- Brainard, G.C.; Hanifin, J.P.; Greeson, J.M.; Byrne, B.; Glickman, G.; Gerner, E.; Rollag, M.D. Action Spectrum for Melatonin Regulation in Humans: Evidence for a Novel Circadian Photoreceptor. J. Neurosci. 2001, 21, 6405–6412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thapan, K.; Arendt, J.; Skene, D.J. An action spectrum for melatonin suppression: Evidence for a Novel Non-Rod, Non-Cone Photoreceptor System in Humans. J. Physiol. 2001, 535, 261–267. [Google Scholar] [CrossRef]
- Lucas, R.J.; Peirson, S.N.; Berson, D.M.; Brown, T.M.; Cooper, H.M.; Czeisler, C.A.; Figueiro, M.G.; Gamlin, P.D.; Lockley, S.W.; O’Hagan, J.B.; et al. Measuring and using light in the melanopsin age. Trends Neurosci. 2014, 37, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Stevens, R.G. Circadian Disruption and Breast Cancer: From Melatonin to Clock Genes. Epidemiology 2005, 16, 254–258. [Google Scholar] [CrossRef]
- Sephton, S.; Spiegel, D. Circadian disruption in cancer: A Neuroendocrine-Immune Pathway from Stress to Disease? Brain Behav. Immun. 2003, 17, 321–328. [Google Scholar] [CrossRef]
- Fasciani, I.; Petragnano, F.; Aloisi, G.; Marampon, F.; Rossi, M.; Coppolino, M.F.; Rossi, R.; Longoni, B.; Scarselli, M.; Maggio, R. A New Threat to Dopamine Neurons: The Downside of Artificial Light. Neuroscience 2020, 432, 216–228. [Google Scholar] [CrossRef] [PubMed]
- Moriske, H.-J. (Ed.) Stellungnahme der Kommission Innenraumlufthygiene am Umweltbundesamt; Umweltbundesamt: Dessau-Roßlau, Germany, 2020. [Google Scholar]
- al horr, Y.; Arif, M.; Katafygiotou, M.; Mazroei, A.; Kaushik, A.; Elsarrag, E. Impact of indoor environmental quality on occupant well-being and comfort: A Review of the Literature. Int. J. Sustain. Built Environ. 2016, 5, 1–11. [Google Scholar] [CrossRef]
- Gudipudi, R.; Fluschnik, T.; Ros, A.G.C.; Walther, C.; Kropp, J.P. City density and CO2 efficiency. Energy Policy 2016, 91, 352–361. [Google Scholar] [CrossRef]
- Maller, C.; Townsend, M.; Pryor, A.; Brown, P.; Leger, L.S. Healthy nature healthy people: ‘contact with nature’ as an upstream health promotion intervention for populations. Health Promot. Int. 2006, 21, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DIN EN 17037:2019; Daylight in Buildings. German Institute for Standardisation: Berlin, Germany, 2019.
- Gasparella, A.; Pernigotto, G.; Cappelletti, F.; Romagnoni, P.; Baggio, P. Analysis and modelling of window and glazing systems energy performance for a well insulated residential building. Energy Build. 2011, 43, 1030–1037. [Google Scholar] [CrossRef]
- Wacker, M.; Holick, M.F. Sunlight and Vitamin D: A Global Perspective for Health. Derm. Endocrinol. 2013, 5, 51–108. [Google Scholar] [CrossRef] [Green Version]
- DIN EN ISO 7730:2006; Ergonomics of the Thermal Environment—Analytical Determination and Interpretation of Thermal Comfort Using Calculation of the PMV and PPD Indices and Local Thermal Comfort Criteria. German Institute for Standardisation: Berlin, Germany, 2006.
- Bartlett, D.J.; Biggs, S.N.; Armstrong, S.M. Circadian rhythm disorders among adolescents: Assessment and Treatment Options. Med. J. Aust. 2013, 199, S16–S20. [Google Scholar] [CrossRef]
- Klepeis, N.E.; Nelson, W.C.; Ott, W.R.; Robinson, J.P.; Tsang, A.M.; Switzer, P.; Behar, J.V.; Hern, S.C.; Engelmann, W.H. The National Human Activity Pattern Survey (NHAPS): A Resource for Assessing Exposure to Environmental Pollutants. J. Expo Sci. Environ. Epidemiol. 2001, 11, 231–252. [Google Scholar] [CrossRef] [Green Version]
- Committee on Environmental Health. Ambient Air Pollution: Health Hazards to Children. Pediatrics 2004, 114, 1699–1707. [Google Scholar] [CrossRef] [Green Version]
- Mors, S.T.; Hensen, J.L.M.; Loomans, M.G.L.C.; Boerstra, A.C. Adaptive thermal comfort in primary school classrooms: Creating and Validating PMV-Based Comfort Charts. Build. Environ. 2011, 46, 2454–2461. [Google Scholar] [CrossRef] [Green Version]
- Yun, H.; Nam, I.; Kim, J.; Yang, J.; Lee, K.; Sohn, J. A field study of thermal comfort for kindergarten children in Korea: An Assessment of Existing Models and Preferences of Children. Build. Environ. 2014, 75, 182–189. [Google Scholar] [CrossRef]
- Turunen, M.; Toyinbo, O.; Putus, T.; Nevalainen, A.; Shaughnessy, R.; Haverinen-Shaughnessy, U. Indoor environmental quality in school buildings, and the health and wellbeing of students. Int. J. Hyg. Environ. Health 2014, 217, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M. The Impact of School Daily Schedule on Adolescent Sleep. Pediatrics 2005, 115, 1555–1561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- mpfs, Welche Freizeitaktivitäten übst Du Täglich oder Wöchentlich Aus? 2019. Available online: https://de.statista.com/statistik/daten/studie/29982/umfrage/regelmaessige-freizeitaktivitaeten-von-kindern/ (accessed on 23 November 2020).
- Samiou, A.I.; Doulos, L.T.; Zerefos, S. Daylighting and artificial lighting criteria that promote performance and optical comfort in preschool classrooms. Energy Build. 2022, 258, 111819. [Google Scholar] [CrossRef]
- Booysen, M.J.; Samuels, J.A.; Grobbelaar, S.S. LED there be light: The Impact of Replacing Lights at Schools in South Africa. Energy Build. 2021, 235, 110736. [Google Scholar] [CrossRef]
- Tahsildoost, M.; Zomorodian, Z.S. Indoor environment quality assessment in classrooms: An Integrated Approach. J. Build. Phys. 2018, 42, 336–362. [Google Scholar] [CrossRef]
- World Bank; UN DESA. Urbanisierungsgrad: Anteil der Stadtbewohner an der Gesamtbevölkerung in Deutschland in den Jahren von 2000 bis 2019. Statista. 2020. Available online: https://de.statista.com/statistik/daten/studie/662560/umfrage/urbanisierung-in-deutschland/ (accessed on 25 June 2021).
- RETROLux 80D Tageslichtlenkung. 2020. Available online: www.schlotterer.com/de/produkte/retrolux-80d (accessed on 12 April 2021).
- Meyer, C.; Junior, G.J.F.; Barbosa, D.G.; Andrade, R.D.; Pelegrini, A.; Felden, É.P.G. Analysis of daytime sleepiness in adolescents by the Pediatric daytime sleepiness scale: A Systematic Review. Rev. Paul. De Pediatr. 2017, 35, 351–360. [Google Scholar] [CrossRef] [Green Version]
- Brickenkamp, R. d2–Aufmerksamkeits-Belastungstest; Hogrefe: Göttingen, Germany, 2002. [Google Scholar]
- DIN German Institute for Standardization, DIN EN 13211 Air Quality—Stationary Source Emissions—Manual Method of Determination of the Concentration of Total Mercury; German Version EN 13211:2001. 2001. Available online: https://www.perinorm.com/document.aspx?hitnr=0&q=AC:DE45757898 (accessed on 26 April 2021).
- Association of Engineers, VDI 2078 Calculation of Thermal Loads and Room Temperatures (Design Cooling Load and Annual Simulation). 2015. Available online: https://www.perinorm.com/document.aspx?hitnr=0&q=AC:DE88185767 (accessed on 26 April 2021).
- rgb Photonics User Manual. 2020. Available online: https://www.rgb-photonics.com/fileadmin/user_upload/downloads/manuals/Qmini_1_Spectrometer.pdf (accessed on 14 October 2021).
- Brickenkamp, R.; Schmidt-Atzert, L.; Liepmann, D. d2-R–Aufmerksamkeits-und Konzentrationstest; Hogrefe Verlag: Göttingen, Germany, 2010. [Google Scholar]
- Lazor, T.; Tigelaar, L.; Pole, J.D.; de Souza, C.; Tomlinson, D.; Sung, L. Instruments to measure anxiety in children, adolescents, and young adults with cancer: A Systematic Review. Support. Care Cancer 2017, 25, 2921–2931. [Google Scholar] [CrossRef]
- von Baeyer, C.L. Children’s Self-Reports of Pain Intensity: Scale Selection, Limitations and Interpretation. Pain Res. Manag. 2006, 11, 157–162. [Google Scholar] [CrossRef]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. nparLD: An R Software Package for the Nonparametric Analysis of Longitudinal Data in Factorial Experiments. J. Stat. Softw. 2012, 50, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Weinfurt, K.P. Repeated measures analysis: Anova, Manova, and Hlm. In Reading and Understanding More Multivariate Statistics; American Psychological Association: Washington, DC, USA, 2000; pp. 317–361. [Google Scholar]
- Zeitzer, J.M. When is a proxy not a proxy? The foibles of studying non-image forming light. J. Physiol. 2018, 596, 2029–2030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vetter, C.; Pattison, P.M.; Houser, K.; Herf, M.; Phillips, A.J.K.; Wright, K.P.; Skene, D.J.; Brainard, G.C.; Boivin, D.B.; Glickman, G. A Review of Human Physiological Responses to Light: Implications for the Development of Integrative Lighting Solutions. Leukos 2021, 18, 1–28. [Google Scholar] [CrossRef]
- Vetter, C. Circadian disruption: What Do We Actually Mean? Eur. J. Neurosci. 2020, 51, 531–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rossi, M. Conclusions and Possible Guidelines for Circadian Lighting Design. In Circadian Lighting Design in the LED Era; Springer International Publishing: Cham, Switzerland, 2019; pp. 257–277. [Google Scholar] [CrossRef]
- Safranek, S.; Collier, J.M.; Wilkerson, A.; Davis, R.G. Energy impact of human health and wellness lighting recommendations for office and classroom applications. Energy Build. 2020, 226, 110365. [Google Scholar] [CrossRef]
- DIN/TS 5031-100:2021; Optical Radiation Physics and Illuminating Engineering—Melanopic Effects of Ocular Light on Human Beings—Quantities, Symbols and Action Spectra. German Institute for Standardisation: Berlin, Germany, 2021.
- CIE TN 003:2015; Report on the First International Workshop on Circadian and Neurophysiological Photometry. International Commission on Illumination: Vienna, Austria, 2015.
- Hellhammer, D.H.; Wüst, S.; Kudielka, B.M. Salivary cortisol as a biomarker in stress research. Psychoneuroendocrinology 2009, 34, 163–171. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participation | 1 Semester Starting at T1 | 2 Semesters Starting at T3 | Whole Study | |||
|---|---|---|---|---|---|---|
| Group | 80D | 80R (Control) | 80D | 80R (Control) | 80D | 80R (Control) |
| Number | 29 | 27 | 27 | 31 | 56 | 58 |
| Sex—male | 14 | 19 | 15 | 13 | 34 | 27 |
| Sex—female | 15 | 8 | 16 | 14 | 24 | 29 |
| Age (years) | 10.83 ± 0.66 | 10.63 ± 0.63 | 10.59 ± 0.57 | 10.45 ± 0.51 | 10.71 ± 0.62 | 10.53 ± 0.57 |
| Cortisol * (ng/mL) | N/A | N/A | 12.07 ± 6.5 | 9.75 ± 6.23 | 13.6 ± 6.67 | 9.76 ± 5.68 |
| PDSS total score | 11.76 ± 4.26 | 12.26 ± 5.82 | 11.56 ± 3.85 | 11.61 ± 5.1 | 11.66 ± 4.03 | 11.91 ± 5.41 |
| Sleep duration (h) | 8.67 ± 0.78 | 8.44 ± 1.14 | 8.15 ± 0.96 | 8.56 ± 1.12 | 8.42 ± 0.9 | 8.51 ± 1.12 |
| Months | Time Point | CO2 (ppm) | Air Humidity (%) | Air Temperature (°C) | |||
|---|---|---|---|---|---|---|---|
| 80D | 80R (Control) | 80D | 80R (Control) | 80D | 80R (Control) | ||
| March–May | 1 | 982.68 ± 424.77 | 896.54 ± 409.74 | 35.98 ± 5.92 | 36.97 ± 6.39 | 24.84 ± 1.42 | 24.82 ± 1.72 |
| June | 2 | 674.38 ± 278.43 | 839.91 ± 443.49 | 44.68 ± 3.16 | 42.83 ± 4.82 | 26.66 ± 1.12 | 25.39 ± 1.80 |
| October–November | 3 | 1066.52 ± 485.65 | 1054.97 ± 420.87 | 39.30 ± 5.24 | 36.09 ± 4.98 | 24.04 ± 1.02 | 24.21 ± 0.99 |
| December–February | 3 | 1293.62 ± 462.28 | 1070.96 ± 466.21 | 35.46 ± 5.10 | 37.06 ± 6.01 | 24.03 ± 1.05 | 24.67 ± 1.26 |
| March–May | 4 | 982.68 ± 424.77 | 896.54 ± 409.74 | 35.98 ± 5.92 | 36.97 ± 6.39 | 24.84 ± 1.42 | 24.82 ± 1.72 |
| June | 5 | 674.38 ± 278.43 | 839.91 ± 443.49 | 44.68 ± 3.16 | 42.83 ± 4.82 | 26.66 ± 1.12 | 25.39 ± 1.80 |
| Months | Time Point | 80D | 80R (Control) | ||
|---|---|---|---|---|---|
| Mean ± SD | Median ± IQR | Mean ± SD | Median ± IQR | ||
| March–May | 1 | 24.90 ± 31.15 | 0.00 ± 45.46 | 31.81 ± 32.47 | 28.57 ± 55.67 |
| June | 2 | 26.08 ± 32.88 | 0.00 ± 54.55 | 29.93 ± 32.15 | 10.00 ± 56.00 |
| October–November | 3 | 40.10 ± 29.89 | 41.88 ± 0.92 | 31.19 ± 30.80 | 30.95 ± 55.56 |
| December–February | 3 | 55.27 ± 27.66 | 59.17 ± 40.63 | 48.96 ± 34.37 | 55.05 ± 52.14 |
| March–May | 4 | 24.90 ± 31.15 | 0.00 ± 45.46 | 31.81 ± 32.47 | 28.57 ± 55.67 |
| June | 5 | 26.08 ± 32.88 | 0.00 ± 54.55 | 29.93 ± 32.15 | 10.00 ± 56.00 |
| F1-LD-F1 Pretest for Equal Baseline Values | Relative Treatment Effects (RTE) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p-Value 1 | Time Point | 80D | 80R (Control) | ||||||
| Cortisol at 6:30 AM | Treatment | 1.35 (1.00, ∞) | 0.245 | n.s. | 80D | 0.54 | Control | 0.47 | ||
| Semester 2–3 | Time | 1.68 (1.96, ∞) | 0.188 | n.s. | T3 | 0.48 | 80D × T3 | 0.49 | 80R × T3 | 0.48 |
| Treat. × Time | 0.89 (1.96, ∞) | 0.408 | n.s. | T4 | 0.55 | 80D × T4 | 0.58 | 80R × T4 | 0.51 | |
| T5 | 0.47 | 80D × T5 | 0.54 | 80R × T5 | 0.41 | |||||
| F1-LD-F1 Model for Cortisol Decrease | Relative Treatment Effects (RTE) | |||||||||
| F | p-Value 1 | Time of Day | 80D | 80R (Control) | ||||||
| Cortisol decreases | Treatment | 4.60 (1.00, ∞) | 0.032 | * | 80D | 0.48 | Control | 0.53 | ||
| 6:30 AM–11:30 AM | Time | 253.43 (1.91, ∞) | 0.000 | *** | 06:30 | 0.83 | 80D × 06:30 | 0.81 | 80R × 06:30 | 0.84 |
| Treat. × Time | 3.91 (1.91, ∞) | 0.022 | * | 09:00 | 0.38 | 80D × 09:00 | 0.37 | 80R × 09:00 | 0.38 | |
| Treat. × 09:00 | 0.96 (1.00, ∞) | 0.353 | n.s. | 11:30 | 0.31 | 80D × 11:30 | 0.24 | 80R × 11:30 | 0.38 | |
| Treat. × 11:30 | 1.83 (1.00, ∞) | 0.353 | n.s. | |||||||
| F1-LD-F1 Model | Relative Treatment Effects (RTE) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| F | p-Value 1 | Time Point | 80D | 80R (Control) | ||||||
| Daytime sleepiness Semester 1 | Treatment | 0.244 | 0.622 | n.s. | 80D | 0.483 | Control | 0.518 | ||
| Time | 0.002 | 0.963 | n.s. | T1 | 0.501 | 80D × T1 | 0.478 | 80R × T1 | 0.524 | |
| Treat × Time | 0.104 | 0.747 | n.s. | T2 | 0.500 | 80D × T2 | 0.487 | 80R × T2 | 0.512 | |
| Daytime sleepiness Semester 2–3 | Treatment | 1.392 | 0.238 | n.s. | 80D | 0.460 | Control | 0.535 | ||
| Time | 2.468 | 0.085 | . | T3 | 0.520 | 80D × T3 | 0.497 | 80R × T3 | 0.507 | |
| Treat × Time | 2.147 | 0.117 | n.s. | T4 | 0.458 | 80D × T4 | 0.424 | 80R × T4 | 0.492 | |
| T5 | 0.532 | 80D × T5 | 0.458 | 80R × T5 | 0.606 | |||||
| Sleep duration (h) Semester 1 | Treatment | 0.107 | 0.741 | n.s. | 80D | 0.490 | Control | 0.510 | ||
| Time | 5.564 | 0.018 | * | T1 | 0.549 | 80D × T1 | 0.595 | 80R × T1 | 0.503 | |
| Treat × Time | 7.410 | 0.006 | ** | T2 | 0.452 | 80D × T2 | 0.385 | 80R × T2 | 0.518 | |
| Sleep duration (h) Semester 2–3 | Treatment | 0.012 | 0.913 | n.s. | 80D | 0.497 | Control | 0.503 | ||
| Time | 11.193 | 0.000 | *** | T3 | 0.595 | 80D × T3 | 0.544 | 80R × T3 | 0.647 | |
| Treat × Time | 1.869 | 0.158 | n.s. | T4 | 0.514 | 80D × T4 | 0.533 | 80R × T4 | 0.495 | |
| T5 | 0.391 | 80D × T5 | 0.414 | 80R × T5 | 0.367 | |||||
| d-2R concentration Semester 1 | Treatment | 0.020 | 0.887 | n.s. | 80D | 0.505 | Control | 0.495 | ||
| Time | 64.155 | 0.000 | *** | T1 | 0.396 | 80D × T1 | 0.423 | 80R × T1 | 0.369 | |
| Treat × Time | 2.965 | 0.085 | . | T2 | 0.603 | 80D × T2 | 0.586 | 80R × T2 | 0.621 | |
| d-2R concentration Semester 2–3 | Treatment | 0.812 | 0.368 | n.s. | 80D | 0.535 | Control | 0.470 | ||
| Time | 23.970 | 0.000 | *** | T3 | 0.395 | 80D × T3 | 0.431 | 80R × T3 | 0.359 | |
| Treat × Time | 0.360 | 0.549 | n.s. | T4 | 0.499 | 80D × T4 | 0.526 | 80R × T4 | 0.472 | |
| T5 | 0.613 | 80D × T5 | 0.647 | 80R × T5 | 0.578 | |||||
| VAS Scale | Time Point | Simple Comparison | ||
|---|---|---|---|---|
| Wilcoxon Rank Sum | p-Value 1 | |||
| Stress | T1–T2 | 7351 | 0.025 | * |
| T3–T5 | 33,607 | 0.000 | *** | |
| Sleepiness | T1–T2 | 6927.5 | 0.171 | n.s. |
| T3–T5 | 28,178 | 0.333 | n.s. | |
| Exhaustion | T1–T2 | 7640.5 | 0.005 | ** |
| T3–T5 | 30,312 | 0.014 | * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neberich, M.; Gerner, N.; Romodow, C.; Freidl, J.; Huber, D.; Weisböck-Erdheim, R.; Pichler, C.; Hartl, A. Positive Effects of Advanced Daylight Supply of Buildings on Schoolchildren—A Controlled, Single-Blinded, Longitudinal, Clinical Trial with Real Constructive Implementation. Buildings 2022, 12, 600. https://doi.org/10.3390/buildings12050600
Neberich M, Gerner N, Romodow C, Freidl J, Huber D, Weisböck-Erdheim R, Pichler C, Hartl A. Positive Effects of Advanced Daylight Supply of Buildings on Schoolchildren—A Controlled, Single-Blinded, Longitudinal, Clinical Trial with Real Constructive Implementation. Buildings. 2022; 12(5):600. https://doi.org/10.3390/buildings12050600
Chicago/Turabian StyleNeberich, Marcel, Nathalie Gerner, Carina Romodow, Johanna Freidl, Daniela Huber, Renate Weisböck-Erdheim, Christina Pichler, and Arnulf Hartl. 2022. "Positive Effects of Advanced Daylight Supply of Buildings on Schoolchildren—A Controlled, Single-Blinded, Longitudinal, Clinical Trial with Real Constructive Implementation" Buildings 12, no. 5: 600. https://doi.org/10.3390/buildings12050600
APA StyleNeberich, M., Gerner, N., Romodow, C., Freidl, J., Huber, D., Weisböck-Erdheim, R., Pichler, C., & Hartl, A. (2022). Positive Effects of Advanced Daylight Supply of Buildings on Schoolchildren—A Controlled, Single-Blinded, Longitudinal, Clinical Trial with Real Constructive Implementation. Buildings, 12(5), 600. https://doi.org/10.3390/buildings12050600