
The Causal Factors of Elevator Maintenance: A Perspective from Saudi Arabia Healthcare Facility Management




Abstract
:1. Introduction
2. Literature Review
3. Materials and Methods
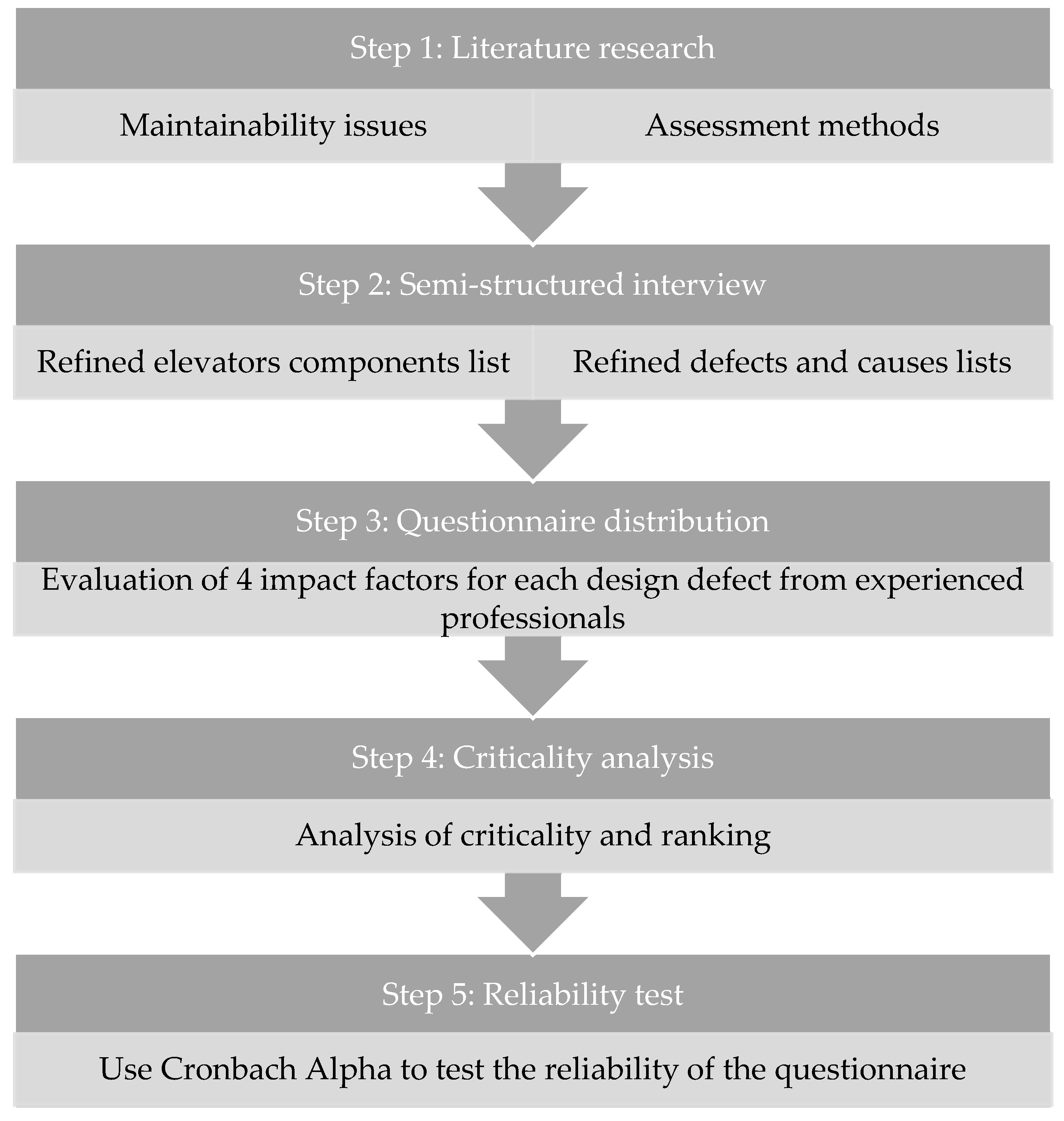
- Step 1.
- Research was conducted that reviewed the literature regarding elevator maintenance defects and their causes in order to analyze their criticality. Since this study focuses on design-caused maintenance issues, the selection process for defects and causes verified that design decisions regarding the specifics of an elevator component lead to the occurrence of said defects. This included research on the assessment methodology to be utilized. Guided by the maintainability assessment and checklist presented by Das and Chew, four elements were chosen for evaluation in this study for each defect, i.e., hygienic, health, and safety impact; cost impact; performance impact; and defect frequency [24]. These elements added additional factors focused on health and safety in order to respond to the nature of healthcare facilities, compared to the impact factors employed by Das and Chew [24].
- Step 2.
- Semi-structured interviews were conducted with a representative sample of experts in elevator maintenance to collect data on the elements mentioned above and to critique the research content of the literature. A total of 62 elevator maintenance issues were discussed with each expert. The interviews involved discussing each issue in light of two essential elements: the extent to which a defect was design-caused, and healthcare relatedness. There were anomalies in the feedback from the selected 6 participants. To avoid bias or inconsistency, the results from all participants were cross-checked during interviews. This step resulted in a refined list of 35 defects as a final list of maintenance issues caused by design decisions as agreed upon by most interviewees. The targeted interviewees were professionals with a proven record of experience with healthcare facility management. Since some experts may not have dealt with elevator systems directly, experience in elevator maintenance was a prerequisite. Whether in a public or private healthcare facility, the level of experience required of the interviewees was at least 15 years. Table 3 lists the responses collected from the interviewees after cross-checking the literature review data of each elevator defect and its cause.
- Step 3.
- A questionnaire was distributed among facility management experts in Saudi Arabia, asking them to evaluate the list generated in Step 2 based on a 5-point Likert scale. This questionnaire adopted convenience sampling, which is a non-probability sampling technique that selects a sample of participants from a population based on convenient accessibility of the data sources [25]. Failure mode, effects, and criticality analysis (FMECA) was used to reflect upon the perspectives of the interviewees to produce their evaluations. The targeted experts were required to have more than ten years of experience in a public or private healthcare facility. All the respondents had to disclose whether their professional background included elevator maintenance experience in healthcare facilities.
- Step 4.
- Criticality analysis was applied to the results that reflected the most severe design decisions, leading to the determination of the most common elevator maintenance issues.
- Step 5.
- We performed a reliability test on the questionnaire, utilizing Cronbach’s alpha (α).
FMECA Assessment
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ciarapica, F.E.; Giacchetta, G.; Paciarotti, C. Facility management in the healthcare sector: Analysis of the Italian situation. Prod. Plan. Control 2008, 19, 327–341. [Google Scholar] [CrossRef]
- Hosking, J.E.; Jarvis, R.J. Developing a replacement facility strategy: Lessons from the healthcare sector. J. Facil. Manag. 2003, 2, 214–228. [Google Scholar] [CrossRef]
- Chotipanich, S. Positioning facility management. Facilities 2004, 22, 364–372. [Google Scholar] [CrossRef]
- Shohet, I.M.; Lavy-Leibovich, S.; Bar-On, D. Integrated maintenance monitoring of hospital buildings. Constr. Manag. Econ. 2003, 21, 219–228. [Google Scholar] [CrossRef]
- Shohet, I.M. Key performance indicators for strategic healthcare facilities maintenance. J. Constr. Eng. Manag. 2006, 132, 345–352. [Google Scholar] [CrossRef]
- Mohammed, M.A.; Hassanain, M.A. Towards improvement in facilities operation and maintenance through feedback to the design team. Built Hum. Environ. Rev. 2010, 3, 72–87. [Google Scholar]
- Seeley, L.H. Building Maintenance; MacMillan Press Ltd.: London, UK, 1976. [Google Scholar]
- Arditi, D.; Nawakorawit, M. Designing buildings for maintenance: Designers’ perspective. J. Archit. Eng. 1999, 5, 107–116. [Google Scholar] [CrossRef]
- Dunston, P.S.; Williamson, C.E. Incorporating maintainability in constructability review process. J. Manag. Eng. 1999, 15, 56–60. [Google Scholar] [CrossRef]
- Meier, J.R.; Russell, J.S. Model process for implementing maintainability. J. Constr. Eng. Manag. 2000, 126, 440–450. [Google Scholar] [CrossRef]
- de Silva, N.; Dulaimi, M.F.; Ling, F.Y.; Ofori, G. Improving the maintainability of buildings in Singapore. Build. Environ. 2004, 39, 1243–1251. [Google Scholar] [CrossRef]
- Al-Hammad, A.; Assaf, S.; Al-Shihah, M. The effect of faulty design on building maintenance. J. Qual. Maint. Eng. 1997, 3, 29–39. [Google Scholar] [CrossRef]
- BCA (Building and Construction Authority). Design for Maintainability Checklist Version 1.3; BCA: Singapore, 2016. Available online: https://www.bca.gov.sg/BCA_Consultation/others/DfM_Checklist_3_Sep2016.pdf (accessed on 1 March 2019).
- The National Committee for Legislation and Standardization of Operation and Maintenance. The Committee Final Report; The National Committee for Legislation and Standardization of Operation and Maintenance: Riyadh, Saudi Arabia, 2016. [Google Scholar]
- Pati, D.; Park, C.S.; Augenbroe, G. Facility maintenance performance perspective to target strategic organizational objectives. J. Perform. Constr. Facil. 2010, 24, 180–187. [Google Scholar] [CrossRef]
- Clemente, J.; Cachadinha, N. BIM-Lean synergies in the management on MEP works in public facilities of intensive use—A case study. In Proceedings of the 21th Annual Conference of the International Group for Lean Construction, Fortaleza, Brazil, 29 July–2 August 2013; pp. 751–759. [Google Scholar]
- Gelnay, B. Facility management and the design of Victoria public hospitals. In Proceedings of the CIB Working Commission 70: Facilities Management and Maintenance Global Symposium, Glasgow, Scotland, 18–20 September 2002; pp. 525–545. [Google Scholar]
- Beckmann, U.; Gillies, D.M.; Berenholtz, S.M.; Wu, A.W.; Pronovost, P. Incidents relating to the intra-hospital transfer of critically ill patients. Intensive Care Med. 2004, 30, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Siti, N.A.; Asmone, A.S.; Chew, M.Y.L. An assessment of maintainability of elevator system to improve facilities management knowledge-base. IOP Conf. Ser. Earth Environ. Sci. 2018, 117, 012025. [Google Scholar] [CrossRef]
- Chew, M.L.; Das, S.; Sulaiman, N.H. Quantifying maintainability parameters for vertical transport system. In Proceedings of the 11th International Conference on Durability of Building Materials & Components, Istanbul Technical University, Istanbul, Turkey, 11–14 May 2008; pp. 11–14. [Google Scholar]
- De Silva, N.; Ranasinghe, M.; De Silva, C.R. Risk analysis in maintainability of high-rise buildings under tropical conditions using ensemble neural network. Facilities 2016, 34, 2–27. [Google Scholar] [CrossRef]
- de Silva, N.; Ranasinghe, M. Maintainability risks of condominiums in Sri Lanka. J. Financ. Manag. Prop. Constr. 2010, 15, 41–60. [Google Scholar] [CrossRef]
- Hassanain, M.A.; Al-Hammad, A.M.; Fatayer, F. Assessment of defects in HVAC systems caused by lack of maintenance feedback to the design team. Archit. Sci. Rev. 2014, 57, 188–195. [Google Scholar] [CrossRef]
- Das, S.; Chew, M.Y. Generic method of grading building defects using FMECA to improve maintainability decisions. J. Perform. Constr. Facil. 2011, 25, 522–533. [Google Scholar] [CrossRef]
- Salkind, N.J. Encyclopedia of Research Design; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2010; Volume 1. [Google Scholar]
- Gliem, J.A.; Gliem, R.R. Calculating, interpreting, and reporting Cronbach’s alpha reliability coefficient for Likert-type scales. In Proceedings of the Midwest Research-to-Practice Conference in Adult, Continuing, and Community Education, The Ohio State University, Columbus, OH, USA, 8–10 October 2003. [Google Scholar]
- Yang, J.B.; Ou, S.F. Using structural equation modeling to analyze relationships among key causes of delay in construction. Can. J. Civ. Eng. 2008, 35, 321–332. [Google Scholar] [CrossRef]
- Ihsan, B.; Alshibani, A. Factors affecting operation and maintenance cost of hotels. Prop. Manag. 2018, 36, 296–313. [Google Scholar] [CrossRef]
- Hassanain, M.A.; Assaf, S.; Al-Ofi, K.; Al-Abdullah, A. Factors affecting maintenance cost of hospital facilities in Saudi Arabia. Prop. Manag. 2013, 31, 297–310. [Google Scholar] [CrossRef]
- Mohammadpour, A.; Anumba, C.J.; Bulbul, T.; Messner, J.; Singh, G.; Singh, R. Impact analysis of facility failures on healthcare delivery process: Use case-driven approach. J. Perform. Constr. Facil. 2015, 30, 04015093. [Google Scholar] [CrossRef]
- Salah, M.; Osman, H.; Hosny, O. Performance-based reliability-centered maintenance planning for hospital facilities. J. Perform. Constr. Facil. 2017, 32, 04017113. [Google Scholar] [CrossRef]
- Patton, J.D. Maintainability and Maintenance Management, 3rd ed.; Instrument Society of America: Research Triangle Park, NC, USA, 1994. [Google Scholar]
- Talon, A.; Chevalier, J.L.; Hans, J. Failure Modes Effects and Criticality Analysis Research for and Application to the Building Domain, CIB Report; International Council for Research and Innovation in Building and Construction (CIB): Rotterdam, The Netherlands, 2006. [Google Scholar]
- El-Haram, M.A.; Horner, R.M.W. Application of the principles of ILS to the development of cost effective maintenance strategies for existing building stock. Constr. Manag. Econ. 2003, 21, 283–296. [Google Scholar] [CrossRef]
- Mecca, S.; Masera, M. Technical risk analysis in construction by means of FMEA methodology. In Proceedings of the 15th Annual ARCOM Conference, Liverpool, UK, 15–17 September 1999. [Google Scholar]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef]

{kind=link}
| Authors | Building Type | Location | Elevators Defects | Impact Factors of Defects | Comparison |
|---|---|---|---|---|---|
| Siti et al. [19] | General buildings | Singapore | 26 | Not stated | This study provided a framework for an elevator maintainability evaluation and sought to understand maintainability issues via a questionnaire distributed among practitioners. |
| Chew et al. [20] | High-rise commercial buildings | Singapore | 114 | This study analyzed elevators’ economic defects, system performance, safety, and comfort impact. | This study focused on commercial buildings, and the impact of defects did not consider healthcare-related building use. It includes defects that occurred during the construction and operation stages. |
| De Silva et al., 2016 [21] | High-rise Building | Sri Lanka | - | 10 risk factors | This study followed a risk-based framework that can measure maintainability by listing. It used an artificial neural network (ANN) tool to forecast maintainability in the early stage of a building. It serves as a decision tool to reduce maintenance costs. |
| De Silva and Ranasinghe [22] | Condominium | Sri Lanka | - | - | This study followed a risk-based maintainability assessment by investigating defects and problems. Although building service defects were the most serious maintainability issues, this study did not specify the defects of the elevator system. |
| Hassanain et al., 2014 [23] | Higher education | Saudi Arabia | - | - | This study investigated the defects of the heating, ventilating, air-conditioning, and cooling (HVAC) systems from maintenance professionals’ point of view. It presented evaluated maintainability lists built to help designers avoid common maintenance issues. |
| Siti et al. [19] | Chew et al. [20] | Das and Chew [21] |
|---|---|---|
| Traveling performance Machine rooms Hoistway and elevator pit Elevator car Elevator lobby | Components: Machine room Lift hoistway Lift car Lift pit Lift landing Sub-components: controller, governor machine, machine room, traction machine, traction motor, brake assembly, guide rail, wire rope, shaft, car interior, car door, car top, car bottom, door operator, travelling, landing door, lift landing, and smoke detector | Machine room and equipment Lift car Car and lobby door Hoistway Ropes Landing Lift pit |
| Sn | Component | Defect | Causes |
|---|---|---|---|
| 1 | Elevator general performance | Long waiting time for elevator to come | Design consideration for traffic load is improper |
| 2 | Elevator car vibrations | Overloading when counterweight ropes are not perfectly matched, especially if less than three, or poor machine room and hoistway building tightness, which allows dust in | |
| 3 | Elevator car jams | Limit switch placement is near the governor rope, which causes the car to stop | |
| 4 | Machine room | Existence of debris and lubricants | Dust from finished or window AC usage or inadequate space and clearance around equipment in the machine room |
| 5 | Falling on machines while performing maintenance or being hit by them | Inadequate space in the machine room, hoistway, or pit, or water or lubricant spills forming slippery working surfaces | |
| 6 | Insufficient lighting level | Inadequate lighting level or short-lamp-life design | |
| 7 | Poor air quality | No air conditioning or proper ventilation, or high humidity coming from water leaks in the wall or ceiling without proper drainage | |
| 8 | Controller | Dirt or noise | Not configured for the environment of the area, i.e., cold versus arid environments and weather conditions, and Ingress Protection (IP) rating does not match |
| 9 | Voltage mismatch | The voltage of imported controllers may differ under many circumstances, allowing a potential voltage mismatch | |
| 10 | Traction machine | Dirt and oil on the traction machine | Insufficient accessibility and limited space to allow adequate general cleaning or spillage removal during lubrication |
| 11 | Wearing marks on ropes | Selection of the rope is mismatched and improper for long sustainment of friction, and possible tension unevenness or improper sheave geometry and design, allowing fast sheave wear that damages ropes | |
| 12 | Noise and vibrations | Insufficient specs for traction machine strength, leading to faster inner wearing, or a proper machine bed rubber is unavailable to absorb vibrations and add more durability | |
| 13 | Speed governor machine | Dirt or noise | High friction due to unsuitable components and rope selection, or inadequate accessibility causing insufficient cleaning for dirt and spillages |
| 14 | Sudden stops | Improper selection, sizing, and specifications of the tripping mechanism | |
| 15 | Elevator car | Maintenance working conditions unsafe | Insufficient clearances, low overhead above, guards unavailable, or lighting is poor or unavailable |
| 16 | Noisy traveling cable | Cable selection does not secure proper acoustic performance | |
| 17 | Darkness or low lighting level | No guard for lights, which may become damaged | |
| 18 | Poor air quality | Inadequate air conditioning or ventilation | |
| 19 | Noisy interior | Finished materials for the car have poor acoustical design; low specs are selected; ventilation fan is noisy due to low quality; trapdoor lock design allows minor movement, thus making sounds | |
| 20 | Car Operating Panel (COP) button not working | Nondurable design for buttons allowing faster damage | |
| 21 | Damaged flooring | Nondurable flooring materials are selected | |
| 22 | Hoistway | Noise and vibration | Guide rail specifications are poorly selected, which may lead to denting |
| 23 | Dirt and dust | Materials selected to build the hoistway generate dust | |
| 24 | Poor air quality | Inadequate ventilation inside the hoistway, walls allow for water seepage, no existing waterproofing | |
| 25 | Roping system | Corroded wires | Rope materials are not rust-resistant and are thus susceptible to corrosion, or poor pulley geometry or grooves causing wires to undergo repetitive bending or excessive friction |
| 26 | Rope vibrations | Deep dust accumulations in pulleys | |
| 27 | Car door | Frequent door closing while users step in | Poor sensing system design, such as single-point photoelectric eyes sensors, that allows such performance |
| 28 | Car doors remain open | COP buttons are nondurable and become unable to function properly without intervention and second attempts | |
| 29 | Noisy doors and abnormal operation | The door roller shoe is poorly designed, and its materials are not adequately selected with rubber lining | |
| 30 | The front frame (jamb) is rusty or damaged | Poor material selection in terms of durability and corrosion resistance | |
| 31 | Lobby and Landing | Button damage | Poor material selection for nondurable buttons that cannot withstand heavy use |
| 32 | The in-car service switch is jammed/broken | Inadequate design to protect the switch from possible vandalism | |
| 33 | Lift pit | Wet and dirt issues | Inaccessible pits or limited access for cleaning, or seepage through structural members with no proper waterproofing |
| 34 | Poor lighting | The lighting is either not provided by the design or not adequately guarded, or the selected lighting level is insufficient | |
| 35 | Falling on or being hit by an adjacent machine while performing maintenance | The pit does not include a partition when accommodating more than one car |
| Sn | Component | Defect | Number of Responses | Severity (Sv) | Criticality (Cr) | Defect Rank | Avg Component Criticality | Component Rank | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | D | ||||||||
| 1 | Elevator general performance | Long waiting time for elevator to come | 27 | 27 | 27 | 27 | 3.5432 | 0.4462 | 10 | 0.4703 | 1 |
| 2 | Elevator car vibrations | 27 | 27 | 27 | 27 | 3.6049 | 0.4700 | 4 | |||
| 3 | Elevator car jams | 27 | 27 | 27 | 27 | 3.6296 | 0.4947 | 1 | |||
| 4 | Machine room | Existence of debris and lubricants | 27 | 27 | 27 | 27 | 3.2593 | 0.3959 | 28 | 0.4074 | 3 |
| 5 | Falling on machines while performing maintenance or being hit by them | 27 | 27 | 27 | 27 | 3.4938 | 0.4296 | 17 | |||
| 6 | Insufficient lighting level | 27 | 27 | 27 | 27 | 3.4074 | 0.3988 | 26 | |||
| 7 | Poor air quality | 27 | 27 | 27 | 27 | 3.4198 | 0.4053 | 25 | |||
| 8 | Controller | Dirt or noise | 15 | 25 | 25 | 25 | 3.4133 | 0.4260 | 19 | 0.4359 | 2 |
| 9 | Voltage mismatch | 25 | 25 | 25 | 25 | 3.6667 | 0.4459 | 11 | |||
| 10 | Traction machine | Dirt and oil on traction machine | 25 | 25 | 25 | 25 | 3.2400 | 0.4199 | 20 | 0.4124 | 2 |
| 11 | Wearing marks on ropes | 25 | 25 | 25 | 25 | 3.1467 | 0.3877 | 32 | |||
| 12 | Noise and vibrations | 25 | 25 | 25 | 25 | 3.4000 | 0.4298 | 15 | |||
| 13 | Speed governor machine | Dirt or noise | 25 | 25 | 25 | 25 | 3.5067 | 0.4657 | 5 | 0.4701 | 1 |
| 14 | Sudden stops | 25 | 25 | 25 | 24 | 3.5733 | 0.4745 | 3 | |||
| 15 | Elevator car | Maintenance working conditions unsafe | 25 | 25 | 25 | 25 | 3.6667 | 0.4928 | 2 | 0.4167 | 3 |
| 16 | Noisy traveling cable | 25 | 25 | 25 | 25 | 3.4400 | 0.3963 | 27 | |||
| 17 | Darkness or low lighting level | 25 | 25 | 25 | 25 | 3.2667 | 0.4077 | 23 | |||
| 18 | Poor air quality | 25 | 25 | 25 | 25 | 3.0667 | 0.3925 | 30 | |||
| 19 | Noisy interior | 25 | 25 | 25 | 25 | 3.0400 | 0.3843 | 33 | |||
| 20 | Car Operating Panel (COP) button not working | 25 | 25 | 25 | 25 | 3.3733 | 0.4480 | 9 | |||
| 21 | Damaged flooring | 25 | 25 | 25 | 25 | 3.2933 | 0.3952 | 29 | |||
| 22 | Hoistway | Noise and vibration | 25 | 25 | 25 | 25 | 3.5067 | 0.4096 | 22 | 0.3772 | 4 |
| 23 | Dirt and dust | 25 | 25 | 25 | 25 | 3.1600 | 0.3741 | 34 | |||
| 24 | Poor air quality | 25 | 25 | 25 | 25 | 3.2933 | 0.3478 | 35 | |||
| 25 | Roping system | Corroded wires | 25 | 25 | 25 | 25 | 3.4400 | 0.4293 | 18 | 0.4097 | 3 |
| 26 | Rope vibrations | 25 | 25 | 25 | 25 | 3.3867 | 0.3901 | 31 | |||
| 27 | Car door | Frequent door closing while users step in | 25 | 25 | 25 | 25 | 3.4267 | 0.4331 | 12 | 0.4387 | 2 |
| 28 | Car doors remain open | 25 | 25 | 25 | 25 | 3.5067 | 0.4601 | 7 | |||
| 29 | Noisy doors and abnormal operation | 25 | 25 | 25 | 25 | 3.4000 | 0.4298 | 15 | |||
| 30 | Front frame (jamb) is rusty or damaged | 25 | 25 | 25 | 25 | 3.3733 | 0.4318 | 14 | |||
| 31 | Lobby and landing | Button damage | 25 | 25 | 25 | 25 | 3.2400 | 0.4510 | 8 | 0.4330 | 2 |
| 32 | In-car service switch is jammed/broken | 25 | 25 | 25 | 25 | 3.4133 | 0.4151 | 21 | |||
| 33 | Lift pit | Wet and dirt issues | 25 | 25 | 25 | 25 | 3.3333 | 0.4320 | 13 | 0.4333 | 2 |
| 34 | Poor lighting | 25 | 25 | 25 | 25 | 3.3067 | 0.4074 | 24 | |||
| 35 | Falling on or being hit by an adjacent machine while performing maintenance | 25 | 25 | 25 | 25 | 3.4667 | 0.4604 | 6 | |||
| Sn | Elevator Component | Notes |
|---|---|---|
| 1 | Elevator general performance | Contains the highest weight of overly critical maintenance issues. The major critical design-caused defect is elevator car jams caused by the limit switch placement in elevators near the governor rope, making the elevator car stop moving. |
| 2 | Machine room | Comes tenth among the overall less-critical components. The defects associated with the machine room are pertinent to other systems and mostly focus on accessibility and cleanliness obstacles. |
| 3 | Controller | Includes the most critical design-caused defect seen in the area experts worked in, i.e., the voltage mismatch of controllers. Since controllers are mostly imported from abroad, there are frequent cases of voltage mismatch, which could be avoided if additional measures were taken at the design stage. |
| 4 | Traction machine | The most critical defect within the traction machine category is the noise and vibrations caused by insufficient specifications for traction machine strength, leading to faster inner wearing. A proper machine bed rubber is unavailable to absorb vibrations and add more durability. |
| 5 | Over-speed governor machine | This component comes second among all others for two primary defects, i.e., dirt or noise, caused by high friction due to unsuitable components and rope selection, or is otherwise caused by inadequate accessibility causing insufficient cleaning of dirt and spillages. The second is a sudden stop due to the improper selection, sizing, or specifications of the tripping mechanism. |
| 6 | Elevator car | The primary defect that causes maintenance issues is unsafe working conditions caused by a low overhead above the elevator car or poor or unavailable lighting. |
| 7 | Hoistway | From inside the hoistway or shafts, host elevators have a moderate critical defect affecting their maintenance. The primary design-caused defects rated for this component are noise and vibration, dirt and dust, and low air quality. |
| 8 | Roping system | Corrosion is the primary defect that affects this component caused by non-rust-resistant rope materials, which are thus susceptible to corrosion, poor pulley geometry, or grooves, causing the wire to undergo repetitive bending or excessive friction. |
| 9 | Car door | Overall, this component comes third compared to other components. Its primary defect is that the doors may remain open because the car’s operating panel (COP) buttons are nondurable and become unable to function appropriately without intervention and second attempts. |
| 10 | Lobby and landing | The in-car service switch being jammed or broken is the most critical defect for lobby and landing components. This is caused mostly by inadequate designs to protect the switch from possible vandalism. |
| 11 | Lift pit | As a component, this is among the components that are second in criticality. The most critical defect, ranked eleventh among all component defects, is the possibility of falling on or being hit by an adjacent machine while performing maintenance. The reason for this is that some elevator pits do not include a partition when accommodating more than one car. |
| Number of Questions | Sum of Variances | The Variance of Total Scores | Cronbach’s Alpha, α |
|---|---|---|---|
| 140 | 129.35 | 12,564.74 | 0.9968 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alassafi, H.; Al-Gahtani, K.; Almohsen, A.; Alfalah, G. The Causal Factors of Elevator Maintenance: A Perspective from Saudi Arabia Healthcare Facility Management. Buildings 2022, 12, 532. https://doi.org/10.3390/buildings12050532
Alassafi H, Al-Gahtani K, Almohsen A, Alfalah G. The Causal Factors of Elevator Maintenance: A Perspective from Saudi Arabia Healthcare Facility Management. Buildings. 2022; 12(5):532. https://doi.org/10.3390/buildings12050532
Chicago/Turabian StyleAlassafi, Hassan, Khalid Al-Gahtani, Abdulmohsen Almohsen, and Ghasan Alfalah. 2022. "The Causal Factors of Elevator Maintenance: A Perspective from Saudi Arabia Healthcare Facility Management" Buildings 12, no. 5: 532. https://doi.org/10.3390/buildings12050532
APA StyleAlassafi, H., Al-Gahtani, K., Almohsen, A., & Alfalah, G. (2022). The Causal Factors of Elevator Maintenance: A Perspective from Saudi Arabia Healthcare Facility Management. Buildings, 12(5), 532. https://doi.org/10.3390/buildings12050532