1. Introduction
Indoor thermal comfort has become an important topic for sustainable building research. Thermal comfort improves the performance of the building, by reducing the energy consumption and greenhouse gas emissions [
1]. Sensing, controlling, and predicting thermal comfort is required to ensure healthy indoor conditions for occupants. Providing an appropriate indoor environment, especially in medico-social institutions, is crucial since patients spend 80–90% of the day indoors and are significantly impacted by variations in hygrothermal parameters. Furthermore, such buildings may experience different hygrothermal conditions depending on patient rooms and building design, not to mention the type of disease. Ensuring a comfortable environment can positively contribute to their treatment and care [
2,
3].
The American Society of Heating, Refrigerating, and Air-Conditioning Engineers (ASHRAE) defined thermal comfort as the state of mind in which satisfaction is expressed with the thermal environment [
4]. Over the years, an extensive amount of research has been carried out on thermal comfort but mainly focused on healthy occupants. However, few studies have explored the thermal sensation of occupants in specific buildings such as medico-social institutions due to the lack of knowledge in this area [
5,
6]. Thermal comfort requirements in medico-social institutions can differ from other types of buildings. Nevertheless, the current ASHRAE standards 55-2017 [
7] and ISO/TS 14415 [
8] lack information on this topic. The standards outline methods to determine the thermal environmental conditions (temperature, humidity, air speed, and radiant effects) for healthy adults. Nevertheless, these standards are not intended to override any health or critical process requirements (see ASHRAE Standards: 55-2017,
Section 2).
For people with limited adaptive opportunities who are recognized as vulnerable people, an acceptable environment to healthy individuals may be considered unacceptable to them [
9]. Assessing thermal comfort in medico-social institutions is therefore challenging. The major challenge is to best meet the thermal comfort needs of different in-situ populations: i.e., medico-social staff and patients.
Among the thermal comfort indices, Fanger’s predicted mean vote (PMV) and predicted percentage of dissatisfied (PPD) are the most applicable [
10]. The PMV-PPD model requires two personal factors—metabolic rate and clothing insulation—and four environmental factors—air temperature, radiant temperature, air velocity, and humidity [
11]. When patients take medications that affect their thermoregulatory system [
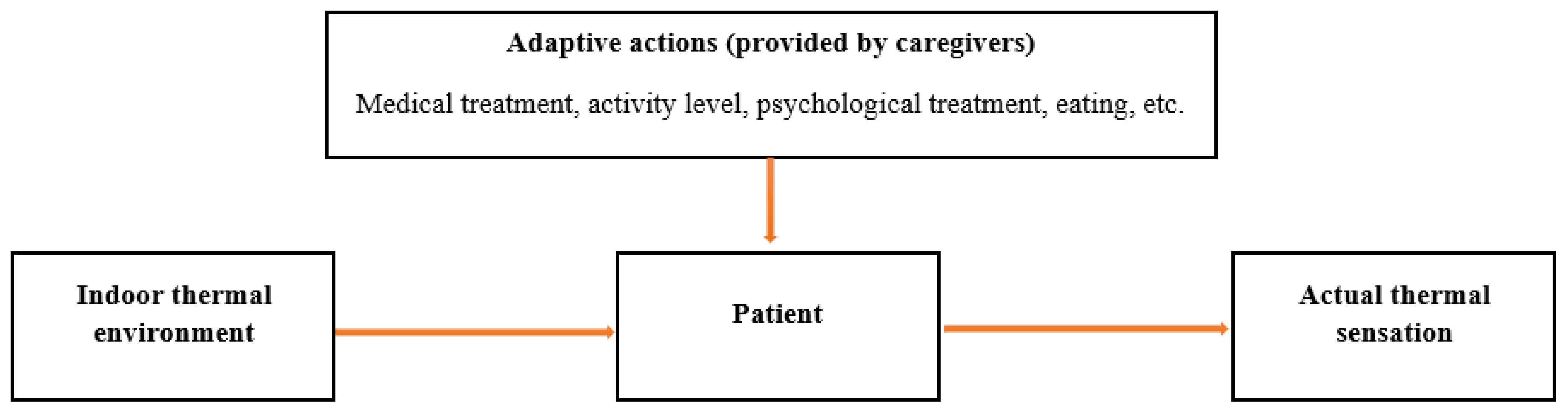
12], the predictability of comfort ratings may be less reliable. Therefore, thermal adaptation can play a key role in evaluating the thermal sensation of patients.
Recently, the adaptive approach to thermal comfort has interested researchers [
13,
14], because it takes into account many factors such as climate, culture, as well as psychological and behavioral adaptations, which play an important role in controlling thermal comfort. This approach could be defined as follows: “If a change occurs such as to produce discomfort, people react in ways which tend to restore their comfort” [
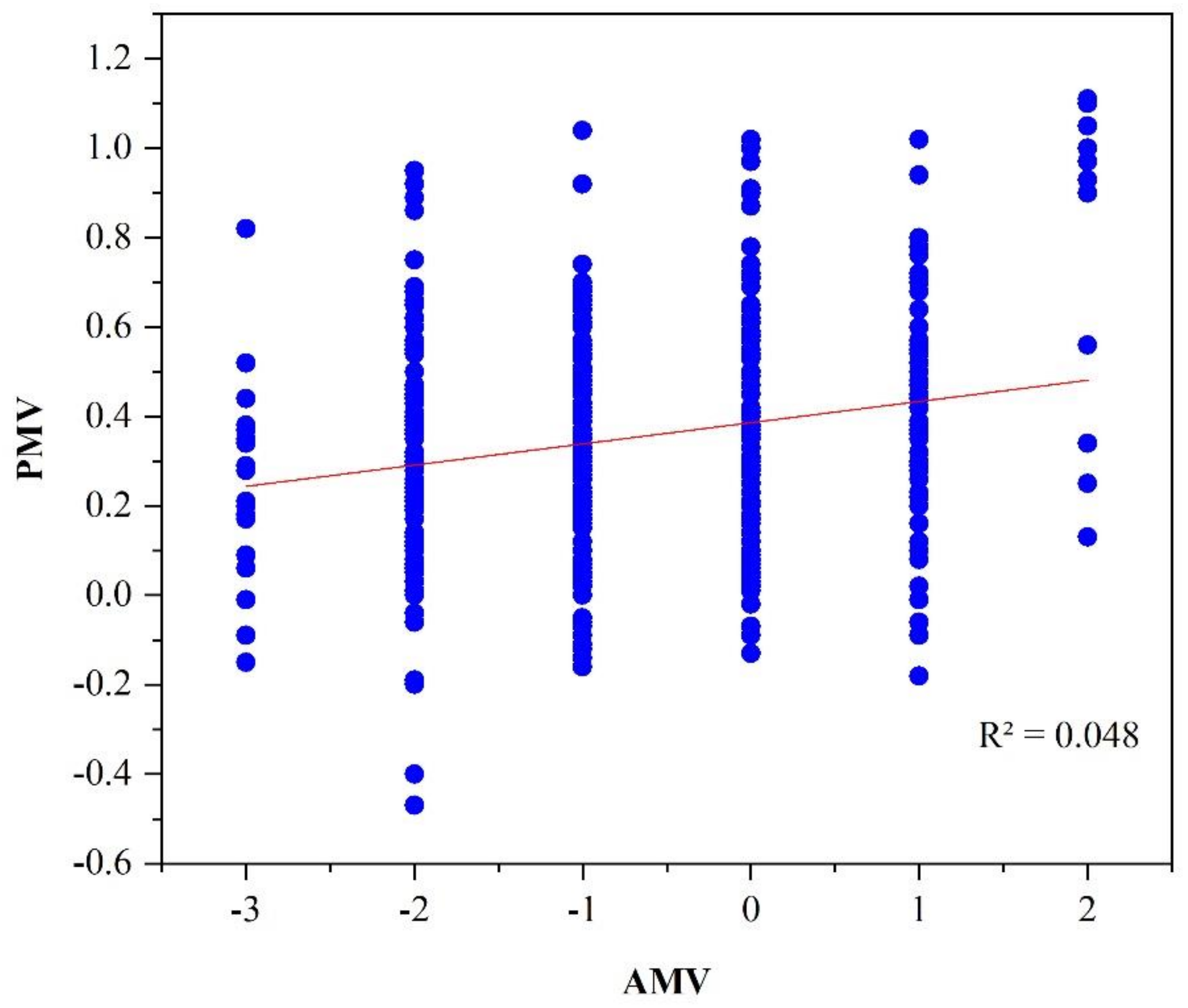
15]. The cultural background is an important parameter in terms of AMV values (subjective approach) and in terms of PMV values (objective approach). The cultural variation and the availability of personal environmental control options, have an important influence on the PMV model accuracy [
16]. Food habit and clothes style, for example, can affect internal thermal energy production and increase the clothing’s factor, respectively. On the other hand, several scientific have highlighted the importance of including the culture influence on thermal comfort, this topic would be important in architect field, by improving the design possibilities [
17]. Pereira et al. [
18] showed that detection of occupant behavior in buildings is an important parameter, which leading to better indoor environment and thermal comfort. Pereira et al. [
19] showed that occupant behavior in buildings is decisive for their hygrothermal performance. Verheyen et al. [
20] investigated the thermal comfort of patients in a Belgian healthcare facility by comparing objective parameters and subjective measures of thermal comfort for different patient groups. They concluded that PMV can adequately predict mean thermal sensation for the majority of patients. On the contrary, Sattayakorn et al. [
21] indicated that the PMV-PPD model was unsuitable for evaluating the thermal comfort of occupants in healthcare facilities in tropical regions. This result was later confirmed by Yau et al. [
22], who indicated that the PMV-PPD model may not be suitable for tropical hospitals as occupants may be more satisfied with a hot indoor environment. In the study of Hashiguchi et al. [
23], a comparison of the thermal comfort of patients and medical staff concluded that most patients were comfortable, while the medical staff were uncomfortable. However, this study did not compare subjective responses and objective measures with PMV predictions, which is of crucial importance in this field.
Skoog et al. [
24] showed little difference in the thermal sensations between staff and patients in Swedish hospitals. In another study by Hill et al. [
25] on patients with physical disabilities, their most frequent request was to be warmer, whereas staff generally wanted to be cooler. In the same context, Khodakarami et al. [
26] highlighted that hospital occupants have different thermal comfort requirements that are difficult to accommodate in the same space, and thus adaptive comfort is recommended for each group. Regarding the management of the indoor environment, Kim et al. [
27] stated that indoor hygrothermal conditions must be carefully managed in healthcare facilities to improve staff satisfaction with their indoor environment. They concluded that the green features implemented by leadership in energy and environmental design (LEED) in healthcare facilities had a good effect on healthcare staff’s level of comfort. Pereira et al. [
28] highlighted that energy efficient and smarter buildings must include the requirements of the occupants, also discussed the importance of occupant behaviour motivations for the design and implementation of smart systems in buildings. Walker et al. [
29] discussed the importance of thermal comfort management in care homes, and the need to distinguish them from other seemingly similar buildings, because the thermal comfort requirements of patients can be associated with health risks.
To manage the indoor environment, Nomura et al. [
30] noted that to bring about positive health outcomes for patients, there must be a minimum of six air changes per hour (ACH), although in spaces with heating, ventilation, and air conditioning (HVAC) systems, this rate may be reduced to 4 ACH. Hwang et al. [
31] reported that patients are more comfortable in warmer and humid indoor environments in Taiwanese hospitals and are insensitive to indoor thermal changes. The study by Kameel et al. [
32] in healthcare settings showed that hygrothermal parameters can activate or deactivate viruses and that low humidity levels can increase susceptibility to respiratory disease. Smith et al. [
33] showed that patients usually preferred air temperatures between 21.5 °C and 22 °C and relative humidity between 30% and 70%. Bouzidi et al. [
34] investigated adaptive thermal comfort during summer in French healthcare buildings, results shows that the adaptive temperature was 25.0 °C with upper and lower limits of 24.7 °C and 25.4 °C. Pereira et al. [
35] reported that the design of the buildings can be improved by consideration of the effects that the spatial and human characteristics have on the indoor environment quality.
Despite the importance of these studies on thermal comfort, the well-being of occupants in specific situations such as medico-social institutions requires further exploration. First, in the case of healthcare buildings, the indoor temperature set-point is usually determined by healthcare staff, meaning that it is not correlated to patients’ thermal sensation. Second, the adaptive approach is essential to ensure thermal comfort in healthcare buildings, although no study conducted in a French climate has determined the adaptive temperatures for patients. Finally, a new thermal comfort index is necessary to correctly assess the thermal conditions of healthcare buildings.
Hence, the main purpose of this field study is to determine the thermal sensation of occupants in order to adapt thermal approaches to vulnerable people in medico-social buildings. Thermal comfort can take on multiple meanings, being associated with vulnerability, the indoor environment, and the provision of effective care. Thus, adapting the thermal environment of occupants in medico-social institutions is crucial to maintain a good quality of service and support a population that is particularly vulnerable to illness.
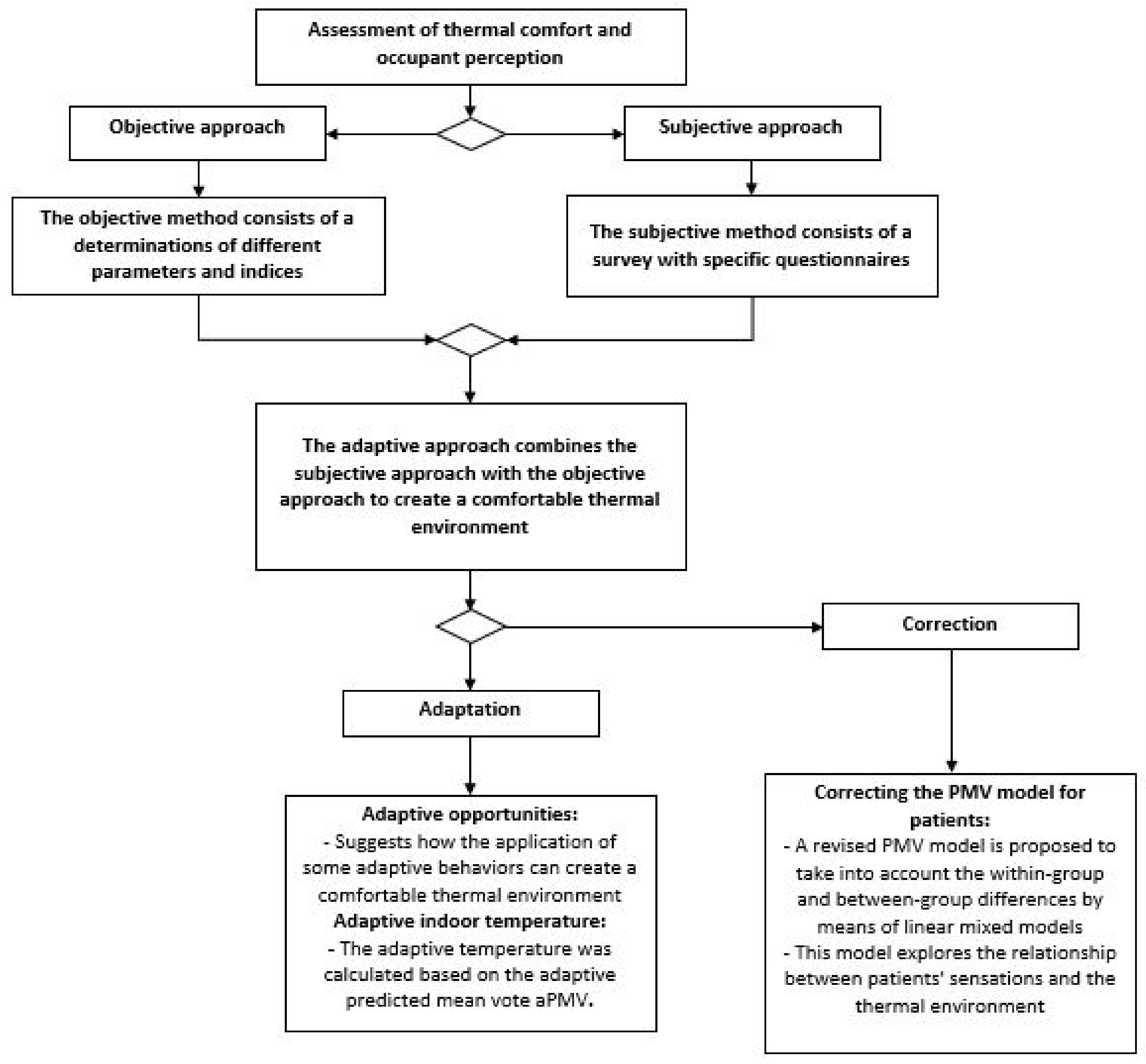
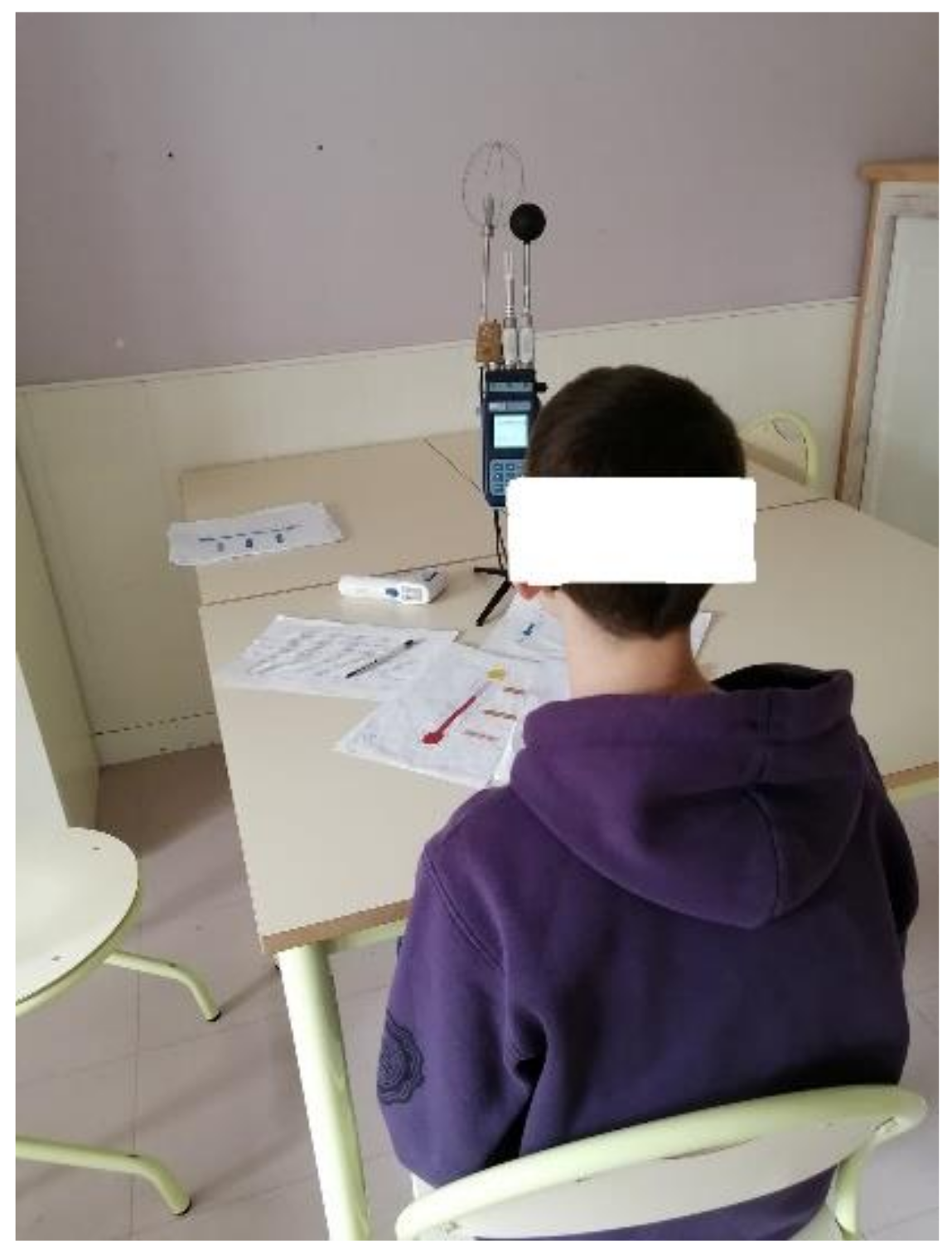
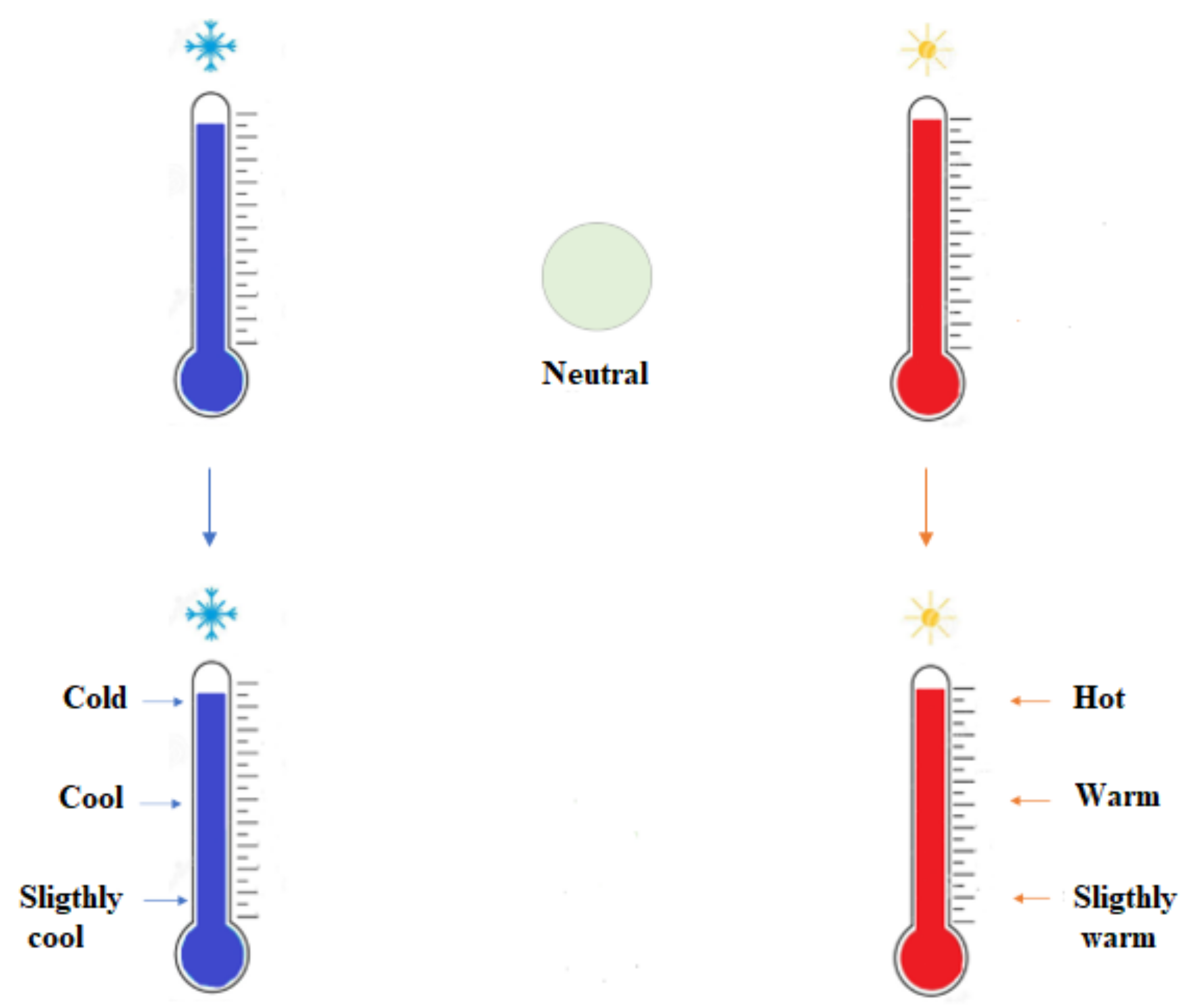
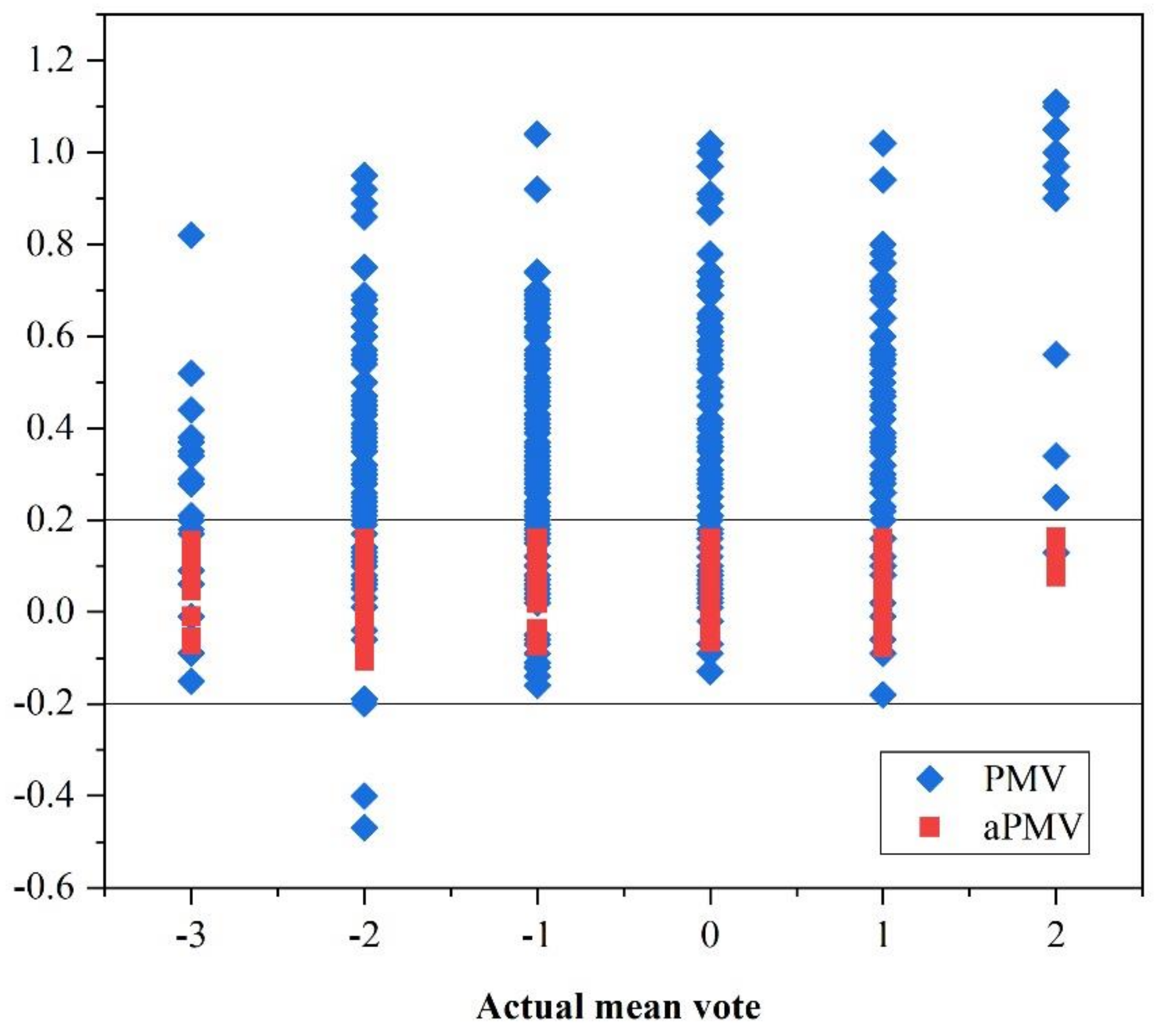
To achieve this goal, we correlate thermal sensation to the indoor environment. Indeed, the HVAC system can be set based on more appropriate metering in the future to reduce energy consumption while improving the indoor climate for patients. Therefore, this study investigates the effect of indoor thermal conditions on the satisfaction of occupants in healthcare facilities. This investigation consists of two parts. The first evaluates the indoor environmental parameters of the studied buildings in terms of air temperature, operative temperature, air velocity, and humidity, as well as the activity and clothing insulation of their occupants. The second part explores the perception of patients regarding their satisfaction with the indoor thermal environment in terms of the actual mean vote (AMV). The optimal temperature is calculated based on the adaptive thermal comfort approach to develop a new PMV model that provides a relationship between the indoor parameters and the thermal sensation of occupants.
4. Correcting the PMV Model for the Patients
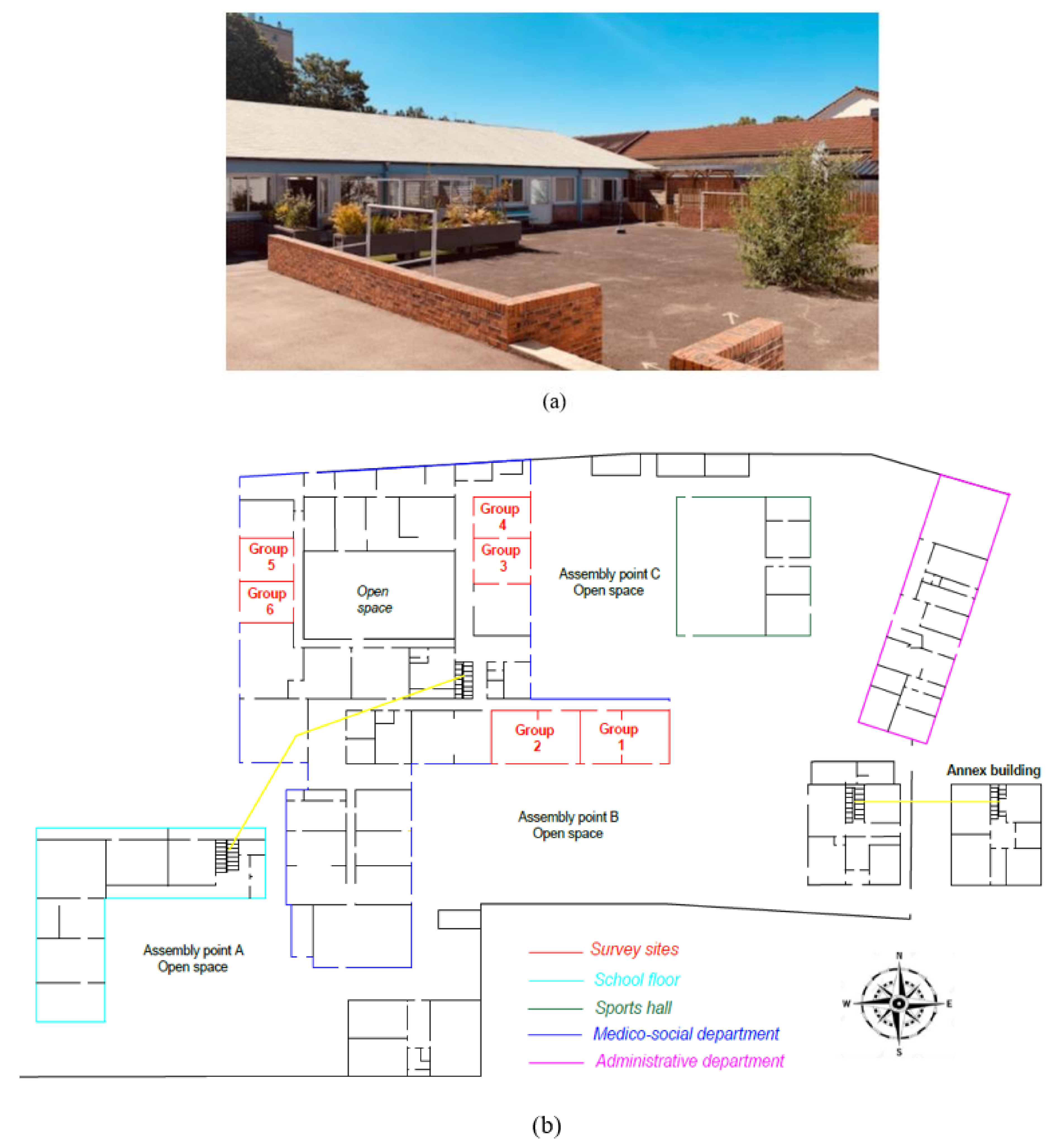
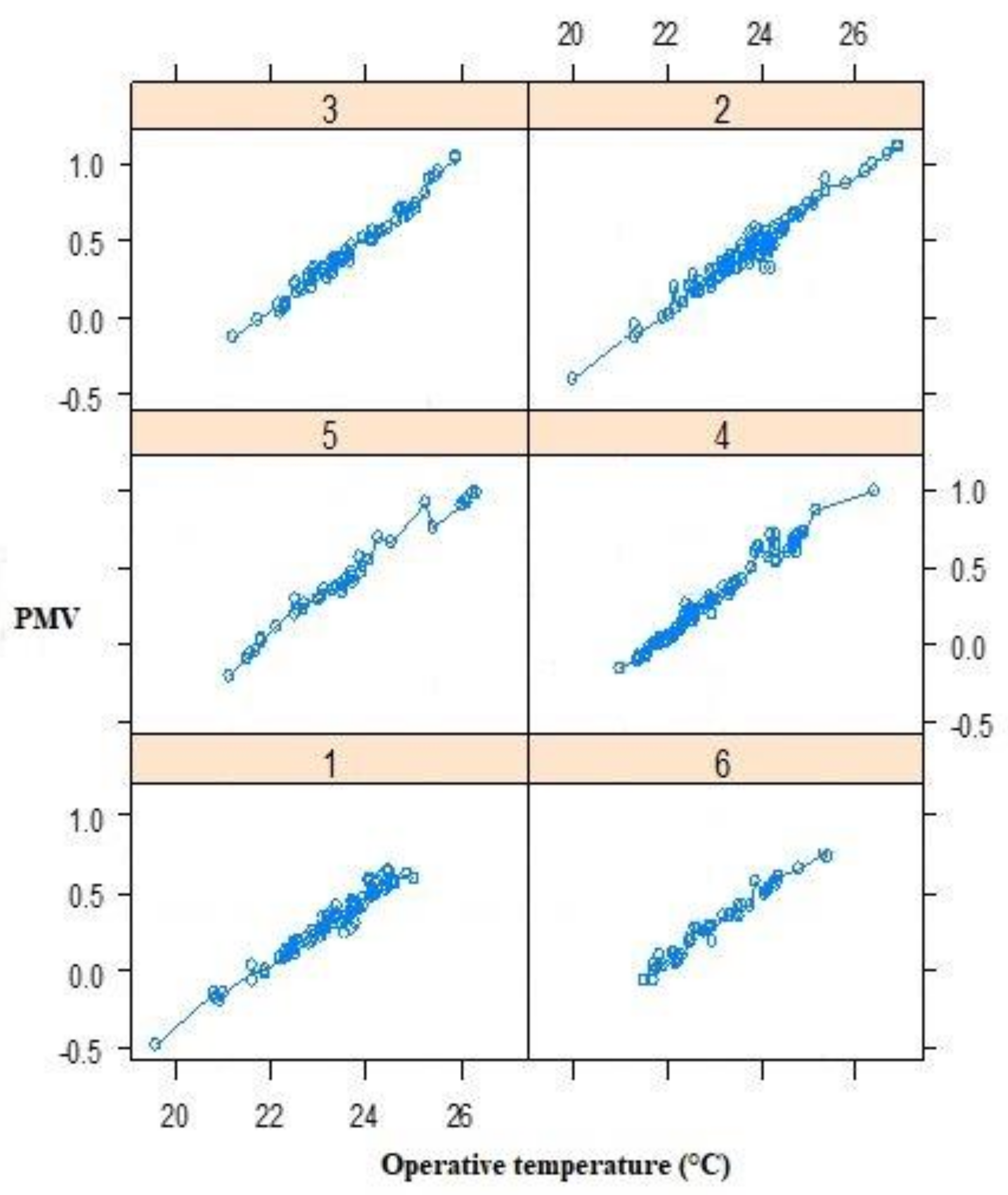
A new design of the PMV model takes into account within-group and between-group differences. For each response, we simultaneously measured the indoor environmental parameters. Therefore, a first-order correction to the PMV model for the patients was possible. Our data are longitudinal, while our data points might not be truly independent. We have six groups (
Figure 2) as well as different observations per group, while our survey study may be insufficient if we try to fit models with too many parameters. Therefore, a linear mixed-effect model was chosen to incorporate all the data, even in the case of many covariates.
Linear mixed-effect models are statistical models containing both fixed and random effects. These models are useful in a wide variety of disciplines but rarely used in the thermal comfort field [
38]. They are particularly useful in settings with repeated measurements. As many types of mixed-error models exist, we compared random intercept, random slope, intercept, and random slope models.
Figure 16 shows that the intercept changes from one group to another, while the slope remains mostly stable. To select the best model, the Bayesian information criterion (BIC) was used, and the model with the lowest BIC was preferred. Finally, a random intercept model was selected. BIC is defined as [
48]:
where
is the maximized value of the likelihood function of the model, n the sample size, and k the number of parameters estimated by the model.
For i = (1 … n) and j = (1 … m), linear mixed models were described as follows:
where
are the fixed effects,
) the random effects, n the number of groups, m the number of repetitions per group, X the independent variable,
the random intercept associated with each group,
the random slope associated with each group, and
the error term.
In this study, a random intercept model was selected:
We looked for a model in which the random intercept was the same for all groups. Equation (23) thus becomes:
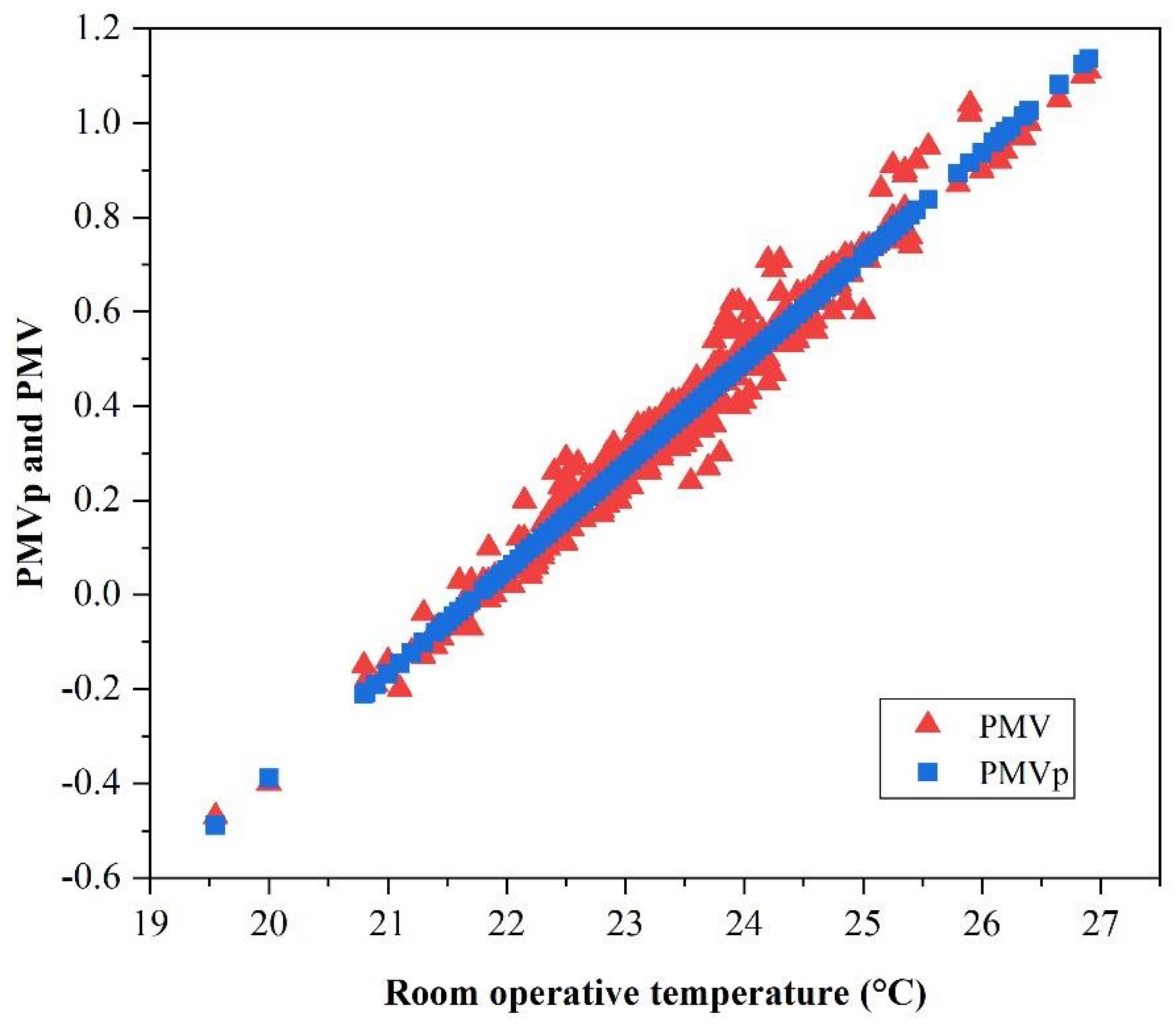
Using R programming language, we propose an AMV-corrected PMV model in which the independent variable is the operative temperature, and the output is the predicted mean vote for patients (PMVp).
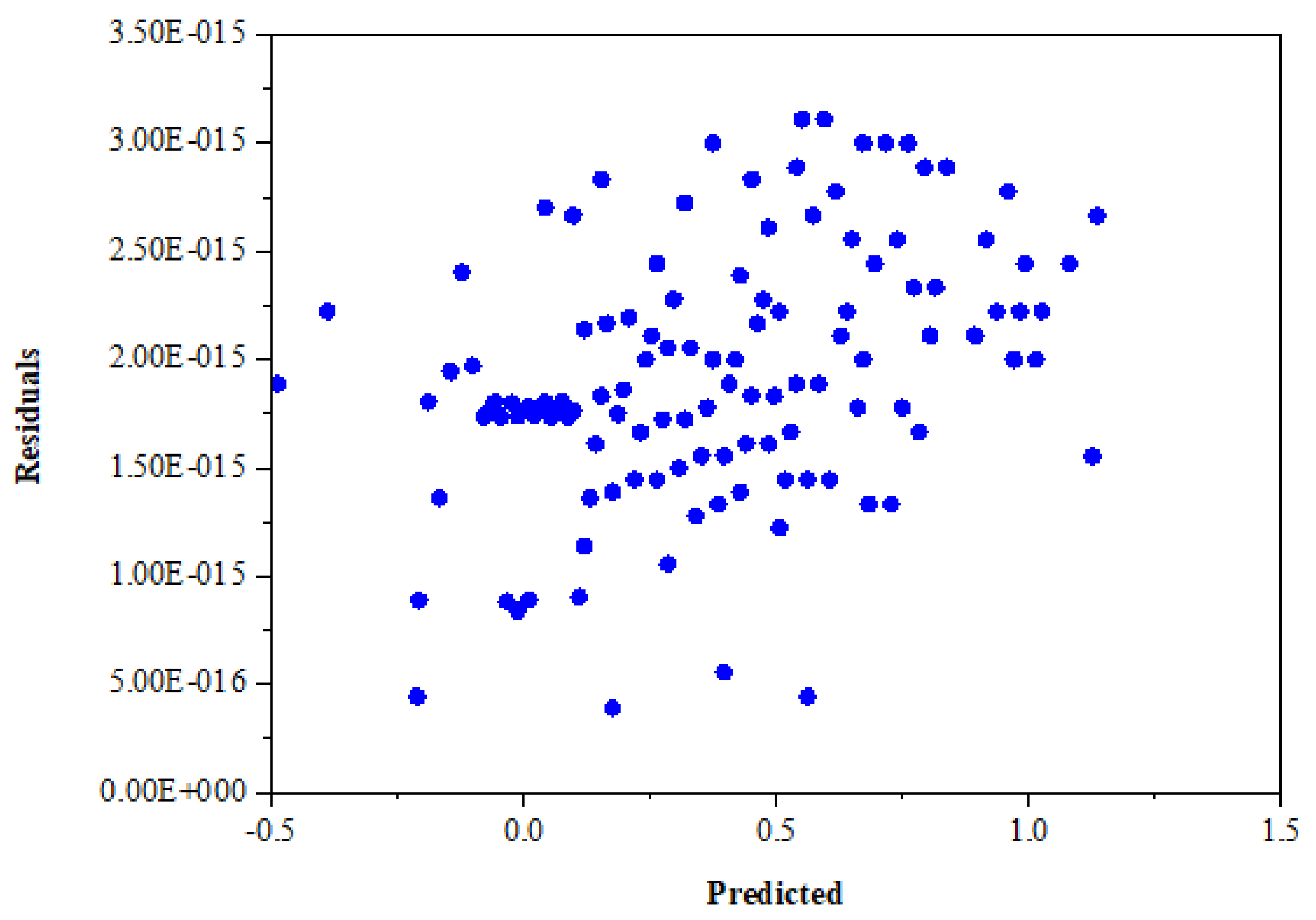
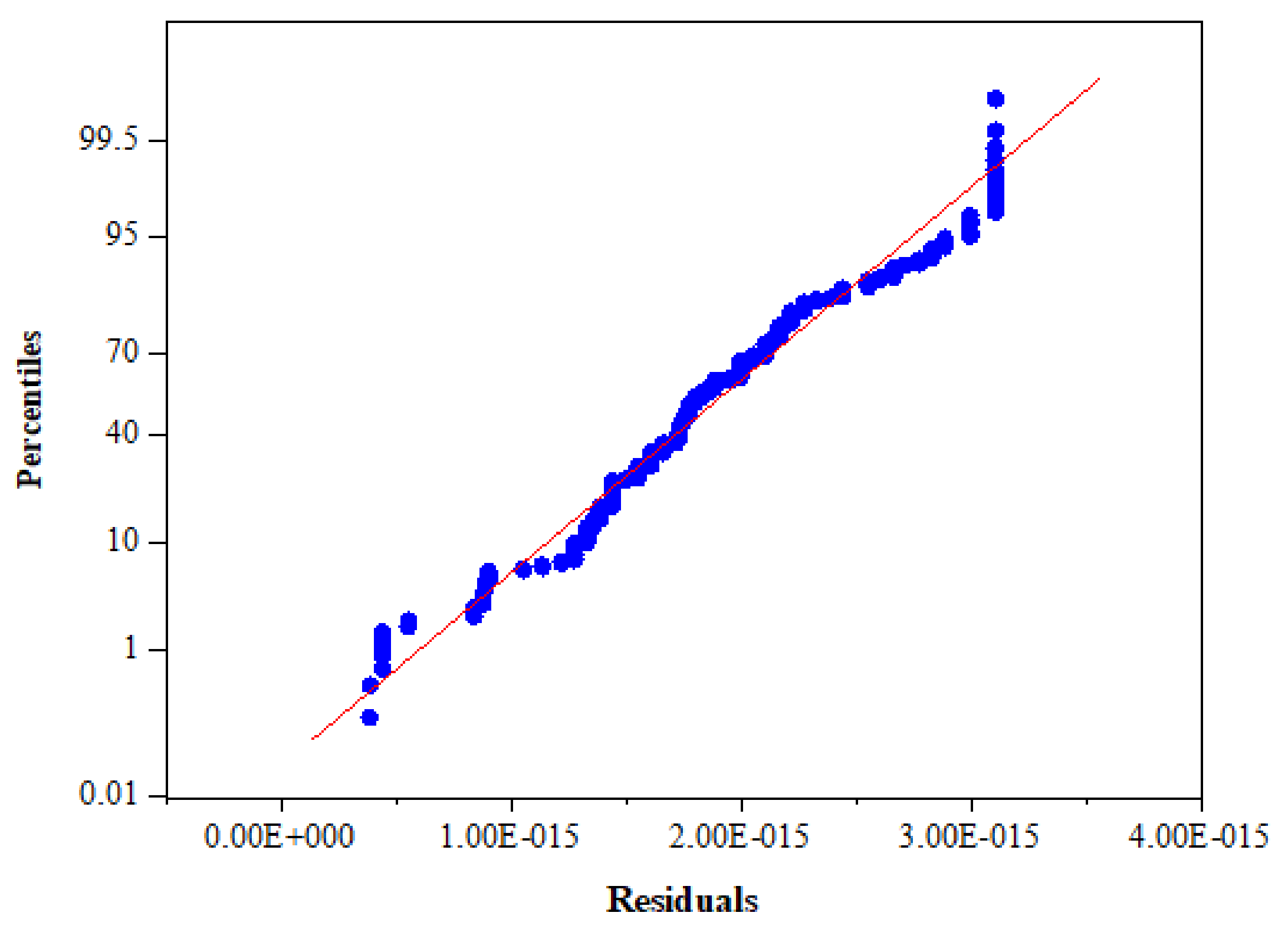
Figure 17 compares the evaluations of PMVp and PMV as a function of the operative temperature. The variation of PMV and PMVp in both cases is homoscedastic, so the linearity assumption is valid. The validity of the model can be verified using the coefficient of determination (
= 0.99), while the residual analysis is defined as the difference between the actual observation and the corresponding fitted value [
49]. The residuals versus predicted values were randomly distributed around zero (
Figure 18), with the normal probability plot of the residuals resembling a straight line (
Figure 19); therefore, the validity of the model is confirmed.
where
is the standard deviation and
the random intercept over the entire data set.


 ,
, 




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}