Heart Rate Variability and Direct Current Measurement Characteristics in Professional Mixed Martial Arts Athletes


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Approach to the Problem
2.2. Subjects
2.3. Procedures
2.3.1. Test-Retest Reliability at the Same Location
2.3.2. Signal-To-Noise Ratio
2.3.3. Test-Retest Reliability at the Different Time-Points/Locations
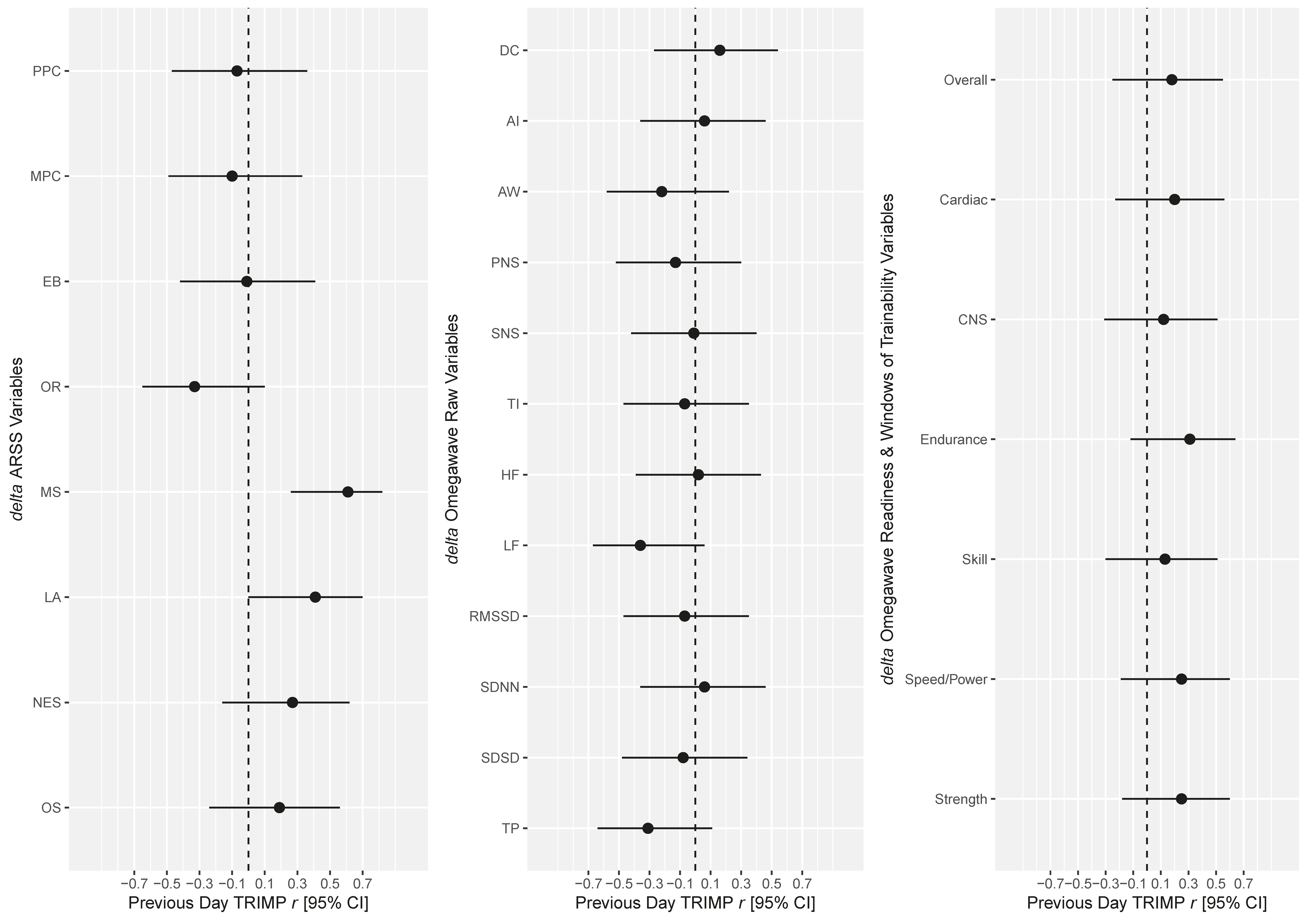
2.3.4. Correlations between Changes in HRV and DC Variables, ARSS Variables and the Previous Day’s TRIMP
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thorpe, R.T.; Atkinson, G.; Drust, B.; Gregson, W. Monitoring Fatigue Status in Elite Team-Sport Athletes: Implications for Practice. Int. J. Sports Physiol. Perform. 2017, 12 (Suppl. 2), 27–34. [Google Scholar] [CrossRef] [PubMed]
- Bourdon, P.C.; Cardinale, M.; Murray, A.; Gastin, P.; Kellmann, M.; Varley, M.C.; Gabbett, T.J.; Coutts, A.J.; Burgess, D.J.; Gregson, W.; et al. Monitoring Athlete Training Loads: Consensus Statement. Int. J. Sports Physiol. Perform. 2017, 12 (Suppl. 2), 161–170. [Google Scholar] [CrossRef] [PubMed]
- Robertson, S.; Kremer, P.; Aisbett, B.; Tran, J.; Cerin, E. Consensus on measurement properties and feasibility of performance tests for the exercise and sport sciences: A Delphi study. Sports Med. Open 2017, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Currell, K.; Jeukendrup, A.E. Validity, reliability and sensitivity of measures of sporting performance. Sports Med. 2008, 38, 297–316. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.; Batterham, A.M.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef]
- Ryan, S.; Kempton, T.; Pacecca, E.; Coutts, A.J. Measurement Properties of an Adductor Strength-Assessment System in Professional Australian Footballers. Int. J. Sports Physiol. Perform. 2019, 14, 256–259. [Google Scholar] [CrossRef]
- Crowcroft, S.; McCleave, E.; Slattery, K.; Coutts, A.J. Assessing the Measurement Sensitivity and Diagnostic Characteristics of Athlete-Monitoring Tools in National Swimmers. Int. J. Sports Physiol. Perform. 2017, 12 (Suppl. 2), 95–100. [Google Scholar] [CrossRef]
- Ryan, S.; Pacecca, E.; Tebble, J.; Hocking, J.; Kempton, T.; Coutts, A.J. Measurement Characteristics of Athlete Monitoring Tools in Professional Australian Football. Int. J. Sports Physiol. Perform. 2020, 15, 457–463. [Google Scholar] [CrossRef]
- Buchheit, M. Monitoring training status with HR measures: Do all roads lead to Rome? Front. Physiol. 2014, 5. [Google Scholar] [CrossRef]
- Malik, C.A.; Bigger, J.T., Jr.; Breithardt, G.; Cerutti, S.; Cohen, R.J.; Electrophysiology, Task Force of the European Society of Cardiology the North American Society of Pacing. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Dobbs, W.C.; Fedewa, M.V.; Macdonald, H.V.; Holmes, C.J.; Cicone, Z.S.; Plews, D.J.; Esco, M.R. The Accuracy of Acquiring Heart Rate Variability from Portable Devices: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 417–435. [Google Scholar] [CrossRef] [PubMed]
- Plews, D.J.; Laursen, P.B.; Kilding, A.E.; Buchheit, M. Evaluating training adaptation with heart-rate measures: A methodological comparison. Int. J. Sports Physiol. Perform. 2013, 8, 688–691. [Google Scholar] [CrossRef] [PubMed]
- Esco, M.R.; Flatt, A.A. Ultra-Short-Term Heart Rate Variability Indexes at Rest and Post-Exercise in Athletes: Evaluating the Agreement with Accepted Recommendations. J. Sports Sci. Med. 2014, 13, 535–541. [Google Scholar] [PubMed]
- Saboul, D.; Pialoux, V.; Hautier, C. The impact of breathing on HRV measurements: Implications for the longitudinal follow-up of athletes. Eur. J. Sport Sci. 2013, 13, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Heathers, J.; Quintana, D.; Angus, D.; Krygier, J.; Kemp, A.; de Rosnay, M. Water Consumption as a Source of Error in the Measurement of Heart Rate Variability; Open Science Framework: Charlottesville, VA, USA, 2018; pp. 1–40. [Google Scholar] [CrossRef]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.; Hanakam, F.; Wiewelhove, T.; Döweling, A.; Kellmann, M.; Meyer, T.; Pfeiffer, M.; Ferrauti, A. Heart Rate Monitoring in Team Sports—A Conceptual Framework for Contextualizing Heart Rate Measures for Training and Recovery Prescription. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef]
- Sherman, S.R. Comparison of Weekly HRV Measures Collected from Two Different Recording Times and Their Relation to Performance in Collegiate Female Rowers; Department of Kinesiology, The University of Alabama: Tuscaloosa, AL, USA, 2018. [Google Scholar]
- Aladjalova, N.A. Slow Electrical Processes in the Brain; Elsevier: Amsterdam, The Netherlands, 1964; Volume 7. [Google Scholar]
- Bechtereva, N.P. The Neurophysiological Aspects of Human Mental Activity; Oxford University Press: New York, NY, USA, 1978. [Google Scholar]
- Valenzuela, P.L.; Sánchez-Martínez, G.; Torrontegi, E.; Vázquez-Carrión, J.; Montalvo, Z.; Kara, O. Validity, Reliability, and Sensitivity to Exercise-Induced Fatigue of a Customer-Friendly Device for the Measurement of the Brain’s Direct Current Potential. J. Strength Cond. Res. 2020. [CrossRef]
- Morris, C.W. The Effect of Fluid Periodization on Athletic Performance Outcomes in American Football Players; Kinesiology and Health Promotion, Univeristy of Kentucky: Lexington, KY, USA, 2015. [Google Scholar]
- Ilyukhina, V.A.; Zabolotskikh, I. Physiological basis of differences in the body tolerance to submaximal physical load to capacity in healthy young individuals. Hum. Physiol. 2000, 26, 330–336. [Google Scholar] [CrossRef]
- Peterson, K. Recurrent Neural Network to Forecast Sprint Performance. Appl. Artif. Intell. 2018, 32, 692–706. [Google Scholar] [CrossRef]
- Coyne, J.O.C.; Haff, G.G.; Coutts, A.J.; Newton, R.U.; Nimphius, S. The Current State of Subjective Training Load Monitoring—A Practical Perspective and Call to Action. Sports Med. Open 2018, 4, 58. [Google Scholar] [CrossRef]
- Heishman, A.D.; Curtis, M.A.; Saliba, E.; Hornett, R.J.; Malin, S.K.; Weltman, A.L. Non-Invasive Assessment of Internal and External Player Load: Implications for Optimizing Athletic Performance. J. Strength Cond. Res. 2018, 32, 1280–1287. [Google Scholar] [CrossRef] [PubMed]
- Omegawave Coach User Guide. In: Espoo, Finland: Omegawave Oy. 2020. Available online: https://omegawave.blob.core.windows.net/sitematerials/default-document-library/ow-coach-user-guide.pdf (accessed on 10 June 2020).
- Saw, A.E.; Main, L.C.; Gastin, P.B. Monitoring the athlete training response: Subjective self-reported measures trump commonly used objective measures: A systematic review. Br. J. Sports Med. 2016, 50, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Weaving, D.; Jones, B.; Till, K.; Abt, G.; Beggs, C. The Case for Adopting a Multivariate Approach to Optimize Training Load Quantification in Team Sports. Front. Physiol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Kellmann, M.; Kölling, S. Recovery and Stress in Sport: A Manual for Testing and Assessment; Routledge: HAbingdon, UK, 2019. [Google Scholar]
- Russo, M.A.; Santarelli, D.M.; O’Rourke, D. The physiological effects of slow breathing in the healthy human. Breathe 2017, 13, 298–309. [Google Scholar] [CrossRef]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Lauri, A.; Simon Parker, H.; Doleshal, P.; Dodge, C. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar]
- Thorpe, R.T.; Strudwick, A.J.; Buchheit, M.; Atkinson, G.; Drust, B.; Gregson, W. The Influence of Changes in Acute Training Load on Daily Sensitivity of Morning-Measured Fatigue Variables in Elite Soccer Players. Int. J. Sports Physiol. Perform. 2017, 12, S2–S107. [Google Scholar] [CrossRef]
- Hopkins, W.G. A spreadsheet for deriving a confidence interval, mechanistic inference, and clinical inference from a p-value. Sports Sci. 2007, 11, 16–20. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hopkins, W.G. Spreadsheets for analysis of validity and reliability. Sportscience 2015, 19, 36–42. [Google Scholar]
- Hopkins, W.G. Measures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [PubMed]
- Atkinson, G.; Nevill, A. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Fazackerley, L.; Fell, J.; Kitic, C.M. The effect of an ultra-endurance running race on heart rate variability. Eur J. Appl Physiol 2019, 119, 2001–2009. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| +1REST (1) | +1EASY (2) | +1HARD (3) | p | g | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1–2 | 1–3 | 2–3 | 1–2 | 1–3 | 2–3 | ||||
| Raw Variables | |||||||||
| Aperiodic Influences (s) | 2.2 ± 0.8 | 2.1 ± 0.7 | 2.2 ± 0.9 | 0.43 | 0.57 | 0.91 | 0.17 | 0.12 | 0.02 |
| Aspirate Waves (AU) | 0.06 ± 0.04 | 0.06 ± 0.03 | 0.05 ± 0.03 | 0.51 | 0.10 | 0.27 | 0.14 | 0.35 | 0.24 |
| DC Potential (mV) | 14.9 ± 12.4 | 8.9 ± 9.6 | 15.3 ± 13.0 | 0.01 * | 0.86 | 0.01 ** | 0.54 | 0.04 | 0.56 |
| HF (ms2) | 396 ± 325 | 355 ± 327 | 438.9 ± 428.7 | 0.68 | 0.70 | 0.28 | 0.08 | 0.08 | 0.22 |
| LF (ms2) | 1588 ± 1675 | 1280 ± 1117 | 1185.6 ± 1100.5 | 0.91 | 0.67 | 0.61 | 0.02 | 0.10 | 0.10 |
| LF/HF | 6.2 ± 7.6 | 5.5 ± 4.7 | 5.0 ± 6.4 | 0.65 | 0.32 | 0.11 | 0.10 | 0.22 | 0.32 |
| MRI | 213.6 ± 73.8 | 221.7 ± 96.1 | 219.2 ± 71.2 | 0.69 | 0.46 | 0.88 | 0.08 | 0.16 | 0.04 |
| PNS (s) | 0.6 ± 0.2 | 0.6 ± 0.2 | 0.6 ± 0.2 | 0.28 | 0.35 | 0.95 | 0.24 | 0.20 | 0.01 |
| RMSSD (ms) | 77.4 ± 42.9 | 72.1 ± 31.3 | 73.7 ± 34.3 | 0.51 | 0.65 | 0.82 | 0.14 | 0.10 | 0.05 |
| SDNN (ms) | 98.1 ± 43.4 | 88.0 ± 34.2 | 91.3 ± 38.9 | 0.29 | 0.56 | 0.67 | 0.22 | 0.12 | 0.09 |
| SDSD (ms) | 97.1 ± 53.6 | 90.8 ± 38.4 | 92.5 ± 43.1 | 0.54 | 0.66 | 0.84 | 0.13 | 0.09 | 0.04 |
| SNS (%) | 0.4 ± 0.1 | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.07 | 0.09 | 0.97 | 0.39 | 0.18 | 0.00 |
| Tension (AU) | 78.1 ± 119.5 | 87.9 ± 180.6 | 156.9 ± 477.8 | 0.11 | 0.19 | 0.90 | 0.34 | 0.28 | 0.02 |
| Total Power (ms2) | 2099 ± 1823 | 1731 ± 1219 | 1758.4 ± 1236.5 | 0.65 | 0.70 | 0.99 | 0.10 | 0.08 | 0.00 |
| Scale Variables | |||||||||
| Overall Readiness (1–7) | 5.5 ± 1.5 | 5.6 ± 1.4 | 5.7 ± 1.6 | 0.84 | 0.49 | 0.27 | 0.04 | 0.14 | 0.22 |
| Cardiac Readiness (1–7) | 5.9 ± 1.6 | 6.3 ± 1.4 | 6.1 ± 1.7 | 0.14 | 0.30 | 0.66 | 0.32 | 0.22 | 0.10 |
| CNS Readiness (1–7) | 5.8 ± 1.1 | 5.3 ± 1.0 | 5.8 ± 0.9 | 0.02 * | 0.54 | 0.04 * | 0.52 | 0.12 | 0.45 |
| Endurance WOT (1–4) | 2.4 ± 0.8 | 2.5 ± 0.6 | 2.6 ± 0.8 | 0.90 | 0.11 | 0.08 | 0.02 | 0.35 | 0.37 |
| Skill WOT (1–4) | 2.2 ± 0.7 | 2.0 ± 0.9 | 2.1 ± 0.9 | 0.39 | 0.95 | 0.44 | 0.18 | 0.02 | 0.16 |
| Speed/Power WOT (1–4) | 1.6 ± 1.3 | 1.4 ± 1.3 | 1.9 ± 1.1 | 0.71 | 0.35 | 0.19 | 0.08 | 0.20 | 0.28 |
| Strength WOT (1–4) | 2.2 ± 0.9 | 2.2 ± 0.7 | 2.3 ± 0.9 | 0.81 | 0.65 | 0.41 | 0.06 | 0.10 | 0.18 |
| +1REST (1) | +1EASY (2) | +1HARD (3) | p | g | |||||
|---|---|---|---|---|---|---|---|---|---|
| 1–2 | 1–3 | 2–3 | 1–2 | 1–3 | 2–3 | ||||
| Total TRIMP (AU) | 0 ± 0 | 520 ± 244 | 890 ± 383 | 0.00 *** | 0.00 *** | 0.01 ** | 3.90 | 3.90 | 1.12 |
| ARSS Recovery | |||||||||
| PPC | 4.1 ± 1.4 | 4.3 ± 1.1 | 4.1 ± 1.2 | 0.69 | 0.92 | 0.74 | 0.16 | 0.04 | 0.13 |
| MPC | 4.4 ± 0.9 | 4.4 ± 0.9 | 4.3 ± 1.1 | 0.85 | 0.87 | 0.74 | 0.07 | 0.06 | 0.13 |
| EB | 4.5 ± 1.4 | 4.5 ± 1.0 | 4.5 ± 1.1 | 0.90 | 0.97 | 0.92 | 0.05 | 0.02 | 0.04 |
| OR | 3.5 ± 1.5 | 3.9 ± 1.1 | 3.2 ± 1.2 | 0.76 | 0.15 | 0.03 * | 0.12 | 0.61 | 0.87 |
| ARSS Stress | |||||||||
| MS | 2.3 ± 1.4 | 2.8 ± 1.0 | 3.2 ± 1.2 | 0.26 | 0.08 | 0.40 | 0.45 | 0.70 | 0.33 |
| LA | 1.6 ± 1.2 | 1.7 ± 1.4 | 2.2 ± 1.2 | 0.96 | 0.25 | 0.31 | 0.02 | 0.46 | 0.39 |
| NES | 1.3 ± 1.4 | 1.5 ± 1.3 | 1.5 ± 1.4 | 0.55 | 0.51 | 0.94 | 0.24 | 0.26 | 0.03 |
| OS | 2.4 ± 1.7 | 2.3 ± 1.3 | 2.4 ± 1.4 | 0.91 | 0.98 | 0.91 | 0.05 | 0.01 | 0.04 |
| +1REST | +1EASY | +1HARD | OVERALL | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Raw Variables | ||||||||||
| %CV | ICC | %CV | ICC | %CV | ICC | %CV (95% CI) | ICC (95% CI) | sTE (95% CI) | MDC95 | |
| Aperiodic Influences | 37.5 | 0.12 | 29.8 | 0.51 | 40.0 | 0.20 | 35.9 (26.2, 56.7) | 0.28 (−0.12, 0.67) | 0.86 (0.65, 1.26) | 99.4 |
| Aspirate Waves | 29.6 | 0.92 | 28.9 | 0.91 | 44.0 | 0.84 | 34.7 (25.4, 54.8) | 0.89 (0.73, 0.96) | 0.36 (0.28, 0.53) | 96.1 |
| DC Potential | 25.1 | 0.82 | 32.5 | 0.82 | 35.5 | 0.69 | 31.4 (23.0, 49.2) | 0.80 (0.54, 0.93) | 0.49 (0.37, 0.71) | 87.0 |
| HF | 79.8 | 0.78 | 53.5 | 0.85 | 81.2 | 0.80 | 71.7 (50.7, 121) | 0.81 (0.56, 0.93) | 0.48 (0.36, 0.70) | 199 |
| LF | 46.8 | 0.93 | 43.2 | 0.90 | 83.6 | 0.87 | 63.2 (45.0, 105) | 0.90 (0.74, 0.97) | 0.35 (0.27, 0.52) | 175 |
| LF/HF | 89.6 | 0.82 | 67.7 | 0.78 | 88.6 | 0.77 | 82.0 (57.5, 140) | 0.80 (0.54, 0.93) | 0.48 (0.37, 0.71) | 227 |
| MRI | 7.70 | 0.96 | 4.60 | 0.99 | 5.26 | 0.97 | 6.05 (4.56, 8.99) | 0.98 (0.93, 0.99) | 0.17 (0.13, 0.25) | 16.8 |
| PNS | 17.1 | 0.89 | 16.9 | 0.86 | 25.4 | 0.81 | 20.1 (14.9, 30.8) | 0.85 (0.64, 0.95) | 0.42 (0.32, 0.62) | 55.7 |
| RMSSD | 15.3 | 0.97 | 13.9 | 0.97 | 20.1 | 0.96 | 16.6 (12.4, 25.3) | 0.96 (0.90, 0.99) | 0.21 (0.16, 0.31) | 46.0 |
| SDNN | 14.4 | 0.95 | 15.0 | 0.94 | 21.1 | 0.93 | 17.1 (12.7, 26.0) | 0.94 (0.85, 0.98) | 0.27 (0.20, 0.40) | 47.4 |
| SDSD | 14.7 | 0.97 | 13.3 | 0.97 | 19.7 | 0.96 | 16.1 (12.0, 24.5) | 0.96 (0.91, 0.99) | 0.21 (0.16, 0.31) | 44.6 |
| SNS | 12.7 | 0.86 | 7.76 | 0.93 | 12.9 | 0.85 | 11.3 (8.5, 17.0) | 0.88 (0.70, 0.96) | 0.38 (0.29, 0.56) | 31.3 |
| Tension | 41.8 | 0.92 | 25.8 | 0.95 | 52.9 | 0.89 | 41.0 (29.8, 65.5) | 0.92 (0.79, 0.97) | 0.32 (0.24, 0.47) | 114 |
| Total Power | 47.5 | 0.92 | 34.0 | 0.92 | 67.1 | 0.86 | 50.5 (36.4, 82.1) | 0.90 (0.74, 0.96) | 0.35 (0.27, 0.52) | 140 |
| Scale Variables | ||||||||||
| TE | ICC | TE | ICC | TE | ICC | TE (95% CI) | ICC (95% CI) | sTE (95% CI) | MDC95 | |
| Overall Readiness (1–7) | 1.10 | 0.45 | 0.46 | 0.91 | 0.67 | 0.85 | 0.78 (0.59, 1.14) | 0.75 (0.46, 0.91) | 0.53 (0.40, 0.78) | 2.16 |
| Cardiac Readiness (1–7) | 1.10 | 0.52 | 0.46 | 0.92 | 0.44 | 0.94 | 0.72 (0.55, 1.06) | 0.81 (0.57, 0.93) | 0.47 (0.35, 0.68) | 1.99 |
| CNS Readiness (1–7) | 0.60 | 0.67 | 0.46 | 0.81 | 0.62 | 0.58 | 0.57 (0.43, 0.83) | 0.72 (0.41, 0.90) | 0.56 (0.43, 0.82) | 1.58 |
| Endurance WOT (1–4) | 0.75 | 0.07 | 0.32 | 0.75 | 0.36 | 0.82 | 0.51 (0.38, 0.74) | 0.55 (0.16, 0.82) | 0.70 (0.53, 1.02) | 1.41 |
| Skill WOT (1–4) | 0.52 | 0.40 | 0.35 | 0.86 | 0.49 | 0.70 | 0.46 (0.35, 0.67) | 0.71 (0.39, 0.89) | 0.57 (0.43, 0.83) | 1.27 |
| Speed and Power WOT (1–4) | 1.22 | 0.05 | 0.75 | 0.72 | 0.87 | 0.49 | 0.96 (0.73, 1.41) | 0.46 (0.05, 0.77) | 0.76 (0.58, 1.11) | 2.67 |
| Strength WOT (1–4) | 0.69 | 0.32 | 0.20 | 0.93 | 0.39 | 0.81 | 0.47 (0.35, 0.68) | 0.68 (0.34, 0.88) | 0.60 (0.46, 0.88) | 1.30 |
| Raw Variables | ||||
|---|---|---|---|---|
| Inter-Day %CV (95% CI) | Intra-Day %CV (95% CI) | SNR | Interpretation | |
| Aperiodic Influences | 36.5 (26.3, 59.2) | 35.9 (26.2, 56.7) | 1.02 | Acceptable |
| Aspirate Waves | 76.9 (53.5, 135) | 34.7 (25.4, 54.8) | 2.21 * | Good |
| DC Potential | 68.2 (47.8, 118) | 31.4 (23.0, 49.2) | 2.17 * | Good |
| HF | 91.4 (62.9, 164) | 71.7 (50.7, 121) | 1.28 | Acceptable |
| LF | 86.2 (59.5, 153) | 63.2 (45.0, 105) | 1.36 | Acceptable |
| LF/HF | 116 (78.2, 216) | 82.0 (57.5, 140) | 1.41 | Acceptable |
| MRI | 13.3 (9.84, 20.6) | 6.05 (4.56, 8.99) | 2.20 * | Good |
| PNS | 27.3 (19.9, 43.5) | 20.1 (14.9, 30.8) | 1.36 | Acceptable |
| RMSSD | 46.9 (33.5, 77.7) | 16.6 (12.4, 25.3) | 2.82 * | Good |
| SDNN | 38.9 (28.0, 63.4) | 17.1 (12.7, 26.0) | 2.27 * | Good |
| SDSD | 46.0 (32.9, 76.2) | 16.1 (12.0, 24.5) | 2.85 * | Good |
| SNS | 16.8 (12.4, 26.1) | 11.3 (8.5, 17.0) | 1.48 | Acceptable |
| Tension | 71.3 (49.8, 124) | 41.0 (29.8, 65.5) | 1.74 * | Good |
| Total Power | 71.0 (49.6, 123] | 50.5 (36.4, 82.1) | 1.41 | Acceptable |
| Scale Variables | ||||
| Inter-day TE (95% CI) | Intra-day TE(95% CI) | SNR | Interpretation | |
| Overall Readiness (1–7) | 1.25 (0.94, 1.86) | 0.78 (0.59, 1.14) | 1.60 * | Good |
| Cardiac Readiness (1–7) | 1.24 (0.93, 1.85) | 0.72 (0.55, 1.06) | 1.71 * | Good |
| CNS Readiness (1–7) | 0.90 (0.68, 1.34) | 0.57 (0.43, 0.83) | 1.59 * | Good |
| Endurance WOT (1–4) | 0.53 (0.40, 0.80) | 0.51 (0.38, 0.74) | 1.06 | Acceptable |
| Skill WOT (1–4) | 0.73 (0.55, 1.09) | 0.46 (0.35, 0.67) | 1.58 * | Good |
| Speed and Power WOT (1–4) | 1.13 (0.85, 1.69) | 0.96 (0.73, 1.41) | 1.18 | Acceptable |
| Strength WOT (1–4) | 0.70 (0.53, 1.05) | 0.47 (0.35, 0.68) | 1.51 * | Good |
| Raw Variables | ||||
|---|---|---|---|---|
| %CV (95% CI) | Difference %CV | ICC (95% CI) | sTE (95% CI) | |
| Aperiodic Influences | 43.2 (31.4, 69.0) | 7.4 | 0.18 (−0.13, 0.51) | 2.23 (1.70, 3.26) |
| Aspirate Waves | 49.9 (36.0, 80.6) | 15.1 | 0.85 (0.67, 0.94) | 0.44 (0.34, 0.65) |
| DC Potential | 129 (87.6, 235) | 97.2 | −0.06 (−0.29, 0.27] | >4.0 |
| HF | 93.7 (63.3, 163) | 22.0 | 0.79 (0.56, 0.91) | 0.55 (0.42, 0.80) |
| LF | 105 (72.3, 184) | 41.3 | 0.80 (0.57, 0.91) | 0.53 (0.40, 0.78) |
| LF/HF | 79.6 (56.1, 135) | −2.4 | 0.84 (0.65, 0.93) | 0.46 (0.35, 0.67) |
| MRI | 67.8 (48.3, 113) | 61.8 | 0.32 (−0.02, 0.63) | 1.51 (1.15, 2.21) |
| PNS | 21.3 (15.8, 32.6) | 1.2 | 0.82 (0.62, 0.92) | 0.49 (0.37, 0.71) |
| RMSSD | 27.4 (20.2, 42.4) | 10.8 | 0.91 (0.79, 0.96) | 0.34 (0.26, 0.49) |
| SDNN | 26.9 (19.8, 41.6) | 9.8 | 0.81 (0.60, 0.92) | 0.50 (0.38, 0.74) |
| SDSD | 25.5 (18.9, 39.4) | 9.4 | 0.92 (0.82, 0.97) | 0.31 (0.23, 0.45) |
| SNS | 13.9 (10.4, 21.0) | 2.6 | 0.80 (0.58, 0.91) | 0.52 (0.40, 0.76) |
| Tension | 51.0 (36.8, 82.5) | 10.0 | 0.87 (0.70, 0.94) | 0.42 (0.32, 0.61) |
| Total Power | 87.8 (61.5, 151) | 37.2 | 0.80 (0.58, 0.91) | 0.53 (0.40, 0.77) |
| Scale Variables | ||||
| TE (95% CI) | Difference TE | ICC (95% CI) | sTE (95% CI) | |
| Overall Readiness (1–7) | 0.94 (0.72, 1.38) | 0.16 | 0.73 (0.56, 0.92) | 0.65 (0.49, 0.94) |
| Cardiac Readiness (1–7) | 0.80 (0.61, 1.17] | 0.08 | 0.82 (0.71, 0.95) | 0.49 (0.37, 0.71) |
| CNS Readiness (1–7) | 1.10 (0.84, 1.61] | 0.54 | −0.12 (−0.58, 0.26) | >4.0 |
| Endurance WOT (1–4) | 0.35 (0.26, 0.51) | −0.16 | 0.78 (0.65, 0.93) | 0.56 (0.42, 0.81) |
| Skill WOT (1–4) | 0.74 (0.56, 1.08) | 0.28 | 0.32 (−0.03, 0.72) | 1.52 (1.16, 2.22) |
| Speed and Power WOT (1–4) | 0.98 (0.75, 1.43) | 0.02 | 0.37 (0.04, 0.75) | 1.25 (1.03, 1.98) |
| Strength WOT (1–4) | 0.57 (0.44, 0.84) | 0.11 | 0.63 (0.42, 0.88) | 0.80 (0.61, 1.17) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coyne, J.O.C.; Coutts, A.J.; Fomin, R.; French, D.N.; Newton, R.U.; Haff, G.G. Heart Rate Variability and Direct Current Measurement Characteristics in Professional Mixed Martial Arts Athletes. Sports 2020, 8, 109. https://doi.org/10.3390/sports8080109
Coyne JOC, Coutts AJ, Fomin R, French DN, Newton RU, Haff GG. Heart Rate Variability and Direct Current Measurement Characteristics in Professional Mixed Martial Arts Athletes. Sports. 2020; 8(8):109. https://doi.org/10.3390/sports8080109
Chicago/Turabian StyleCoyne, Joseph O. C., Aaron J. Coutts, Roman Fomin, Duncan N. French, Robert U. Newton, and G. Gregory Haff. 2020. "Heart Rate Variability and Direct Current Measurement Characteristics in Professional Mixed Martial Arts Athletes" Sports 8, no. 8: 109. https://doi.org/10.3390/sports8080109
APA StyleCoyne, J. O. C., Coutts, A. J., Fomin, R., French, D. N., Newton, R. U., & Haff, G. G. (2020). Heart Rate Variability and Direct Current Measurement Characteristics in Professional Mixed Martial Arts Athletes. Sports, 8(8), 109. https://doi.org/10.3390/sports8080109